
Abstract
Background
Primary care providers (PCPs) often take the lead role in caring for patients with overweight and obesity; however, few PCPs counsel patients about weight loss. Online weight management programs that are integrated within primary care may help address this gap in care.
Objective
To identify perceptions of and experience with online weight management programs in general and with a proposed online program, to identify barriers to use, and to improve the design and content of our intervention, which included an online program plus population health management (PHM) support from primary care practices.
Design
A mixed qualitative methods study including three patient focus groups and seven semi-structured interviews with healthcare providers.
Participants
A total of 13 adult patients (age range, 20–70) with body mass index (BMI) 27–35 kg/m2 attended the focus groups. In-person semi-structured interviews were conducted with seven healthcare providers (three PCPs, two population health managers, one primary care nurse, and one registered dietitian).
Main Measures
We developed and used semi-structured focus groups and interview guides. The focus group and interviews were recorded and transcribed. Using grounded theory, we analyzed the transcripts to identify and extract common concepts and themes.
Key Results
Although patients and healthcare providers expressed positive opinions about online weight management programs, few patients had experience with them, and providers stated that such programs are not being widely implemented in primary care settings. Some participants highlighted the flexibility and low cost as strengths of online weight management tools compared with in-person programs. All participants had favorable opinions about our proposed intervention and were overwhelmingly positive about the combination of an online program and PHM support.
Conclusions
This study highlights the potential value of online weight management programs and PHM support in primary care.
Clinical Trials Registration
NCT02656693.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
INTRODUCTION
Over two thirds of US adults have overweight or obesity, defined as body mass index (BMI) ≥ 25 kg/m2.1 Overweight and obesity are associated with many serious health conditions, including type 2 diabetes, cardiovascular disease, and some cancers.2,3,4,5 Even small amounts of weight loss can lead to significant health benefits, and a variety of weight loss strategies have been shown to be effective.6,7,8,9,10 Primary care providers (PCPs) can play an important role in helping patients with weight management.11,12,13 Clinical practice guidelines recommend that PCPs offer or refer their patients to an intensive, multi-component behavioral intervention if they would benefit from weight loss.10 However, PCPs often do not have sufficient time or training to counsel patients about weight, and other services may be difficult for patients to access due to convenience and cost.14,15,16,17,18,19,20
Advances in patient-facing health information technology (HIT) have changed the landscape of self-management.21 Although data increasingly support the role of these tools in improving health services’ efficiency and health outcomes,22,23,24 several studies to date have shown mixed results on the effect of these technologies on quality of care.25 Currently, health centers perceive patient-facing HIT as an ideal tool to engage their patient populations in chronic disease management.26
Evidence from a number of studies, including several within the primary care setting, indicates that online (i.e., Internet-based) weight management programs can help people achieve and maintain clinically meaningful weight loss,27,28,29,30,31,32,33,34,35,36,37,38,39 However, these programs are not being widely implemented in primary care, and it is unclear whether they are effective or scalable in real clinical practice.39 To address this, we conducted the Partnerships for Reducing Overweight and Obesity with Patient-Centered Strategies (PROPS) Study. The overall goal of the PROPS Study was to adapt an evidence-based online weight management program, integrate it with population health management (PHM) support from primary care practices, and conduct a cluster-randomized trial to compare the effectiveness of the combined intervention (including the online program and PHM support) with the online weight management program alone and with usual care. The study design and methods for the trial are described elsewhere (Baer et al., 2019; in preparation.)
This paper describes the methods and results of the qualitative work conducted during the first phase of the study, namely focus groups with patients and semi-structured interviews with healthcare providers, to obtain feedback about the proposed intervention before the main trial began. We aimed to identify perceptions of and experience with online weight management programs in general and with our proposed online program, identify barriers to use, and iteratively improve the design and content of the intervention.
METHODS
BMIQ is a cloud-based, HIPAA-compliant platform designed for healthcare providers to deliver weight management programs to patients in a variety of settings.40,41,42 For the PROPS Study, we made several enhancements to the existing BMIQ application; these are described in detail elsewhere (Baer et al., 2019; in preparation). Currently, BMIQ offers patients 33 educational sessions, delivered over a period of 12 months; these sessions are available in written and video formats and cover a variety of topics, including healthy eating, physical activity, and goal setting. To complement these sessions, the program also includes structured exchange-based meal plans; tools for tracking food, physical activity, and weight; and tailored feedback via email and text messages (see Fig. 1 for key BMIQ features).40 A professional interface in BMIQ allows providers to monitor patients’ engagement with the program, including their logins, sessions viewed, and tracking data.40 In our study, population health managers (PHMs), who are non-clinical staff working closely with the primary care practices, and research staff used the professional interface to monitor patients’ progress, conduct outreach, and provide periodic updates to PCPs. BMIQ is available in both English and Spanish and can be accessed via a computer, tablet, or smartphone.

Illustration of the BMIQ Program.
To obtain patient and provider feedback about weight management programs and tools before starting the trial, we conducted three patient focus groups and seven semi-structured interviews with healthcare providers during March and April of 2016, several months prior to the start of recruitment for the main trial. The study took place at Brigham and Women’s Hospital (BWH) in Boston, MA, and was reviewed and approved by the Partners HealthCare Human Research Institutional Review Board (protocol # 2015P002372). The PROPS trial was also registered on clinicaltrials.gov (ID: NCT02656693). All of the patients and healthcare providers who participated in the focus groups and interviews provided verbal informed consent.
Focus Groups with Patients
Study Design, Aims, and Focus Group Guides
Two focus group guides were developed based on current literature and expert opinion: one guide for the first two focus groups (Appendix 1, online) and a second guide for the third group (Appendix 2, online). We piloted both of these guides with several patient and stakeholder advisors, who have provided advice throughout the course of the study, and refined them based on their feedback. The aim of the first two focus groups was to solicit general feedback from patients about weight management programs and about our proposed intervention. The aim of the third focus group, which was comprised of a subset of patients who had already participated in one of the first two focus groups, was to obtain more specific feedback about BMIQ after patients had used it on their own.
Participants
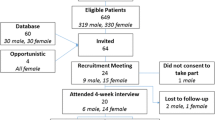
Eligibility criteria for the focus groups were similar to those for the PROPS main trial. Patients were between 20 and 70 years old, had BMI between 27 and 35 kg/m2, were English-speaking, had access to the Internet, and were interested in weight management and/or motivated to lose weight. We identified patients using data from the electronic health record and recommendations from PCPs.
We identified 112 eligible patients for the focus groups. We contacted 47 of these patients following the PCPs’ approval; we screened 34, and 23 of these patients were determined to be eligible. In total, 13 participated in the focus groups; five participated in one of the two initial focus groups as well as the third, which was designed to collect more specific feedback after patients had used the BMIQ program on their own. Table 1 summarizes the characteristics of the focus group participants.
Semi-structured Interviews with Providers
Study Design, Aims, and Interview Guide
We conducted semi-structured interviews with healthcare providers to gather their perspectives about weight management programs and tools available to patients and their opinions about our proposed intervention. To do so, we created a semi-structured interview guide (Appendix 3, online) that was developed based on a literature review and expert opinion.
Participants
We identified seven BWH healthcare providers who are considered key stakeholders. We conducted in-person interviews with three PCPs, two PHMs, one primary care registered nurse, and one registered dietitian.
Data Collection and Analysis
The focus groups and interviews were recorded and transcribed with the consent of the participants. Using grounded theory,43 we analyzed the transcripts to identify and extract common concepts and themes.
RESULTS
Focus Groups with Patients
Perceptions of and Previous Experience with Weight Management Programs
While most focus group participants had tried to lose weight in the past, only a few had used formal weight management programs, including online weight management tools. The participants who had previous experience with formal weight loss programs had tried Weight Watchers and/or used online tools like LoseIt!, MyFitnessPal, and SparkPeople. Most participants who had used these programs reported positive opinions about them and felt that they had helped them to lose weight. Specifically, they mentioned that programs enhanced their awareness and motivation to lose weight and taught them how to change their eating habits and lifestyle. For example, one person stated that:
I don’t even really like to call it [Weight Watchers] a diet as much as it’s just a change in your lifestyle... and it really taught me to be more careful about portion control.
Participants highlighted the barriers and limitations of these programs. They emphasized that it can be hard to stick with the programs (e.g., to keep tracking points/calories and change their daily routine and eating habits). They also noted that weight loss is a long and difficult process. Finally, one informant stated that he had stopped using a program because the recommended meals were too expensive. Below are representative comments from the participants:
I think for me,... what’s not as successful is I don’t keep up with the exercise, and,…I snack too much. I’m snacking and I know that would be too many points if I were actually keeping track of the points, but I don’t keep track of the points anymore, and so... it’s, it’s hard, because you have to continually work at the program.
It’s hard to follow plans with Weight Watchers, anyway, I mean, it’s like... you know, there’s so much food out there that... it’s bad for ya? But it’s still so good that you want to eat it anyway, regardless!
I participated in Weight Watchers. Initially it was great. I lost the weight I wanted to lose and maintained that for quite some time...and then I kind of fell off the wagon and, then I lost weight again, on Weight Watchers, and then I fell off the wagon again, and... that’s where I am now.
Participants also noted that most tools are cumbersome and often require a lot of work to track items, limiting regular use. For example, one person stated that:
I got one...it does a lot of tracking of your activity. So, that’s good. And it gives you a calorie count – just how much you’re burning. But you can also go online and enter your food in there, too, but I haven’t... it’s just an added thing.
Attitudes Towards Proposed Intervention
General Feedback About the Program
We received general feedback about our proposed intervention in the first two focus groups and more specific feedback from the five participants who participated in the third focus group after using and testing the online program on their own. Overall, the participants (in all focus groups) seemed to like BMIQ; they felt it looked simple and easy to follow and found all of the features important for weight management.
The majority of participants felt that the tracking tools were the most important to use. Participants stated that using BMIQ made them think more about their diet and health. They thought they would use all of the features at first, but as soon as they figured out which ones were the most useful for them, they might use just a few of them. The opinions of participants on how often they would use BMIQ ranged from two to five times per week.
While most participants who tested BMIQ on their own used a desktop computer to access the website, some also used laptops, tablets, and smartphones. Several participants accessed BMIQ in more than one way. Surprisingly, very few participants used smartphones to access BMIQ. This could be because most of the participants were in their 50s and 60s; in addition, the program was not designed as a mobile application. See below for some representative comments from the participants.
The phone is too small for me to do it.
Well, I thought maybe that I’d try to use my mobile phone ... because that’s quicker for me, and then I have it with me all the time,… whenever I’m sitting’ down, whatever I’m doing’, I could just... even when I’m out, I can just go through,….and check it out. But… it didn’t work for me, though.
Finally, the majority of participants felt that the integration of BMIQ with PHM support could significantly help study participants manage their weight. Specifically, they liked the idea that a PHM would be reaching out to patients at certain times to provide feedback and support. Most participants also stated that they feel comfortable talking about weight management with someone other than their primary care doctor (e.g., a PHM or dietitian).
Feedback About Specific Features Within the Program
The following findings (Table 2) are related to specific features within BMIQ. This feedback is based on specific tasks that the participants were asked to do when they tested the program on their own (Appendix 2, online).
Semi-structured Interviews with Providers
Feedback About Weight Management Programs in Primary Care
When asked about available weight management programs, the majority mentioned several BWH weight management programs, such as the “surgical management program” and the “medical weight management program,” but none in their primary care practices. They stated that if needed, they refer their patients to other programs at BWH and/or to their registered dietitian.
The registered dietitian we interviewed stated that her department’s activities in the ambulatory care setting are not as comprehensive as in the inpatient setting. Their main ambulatory activity is a referral service for patients; the department also teaches primary care physicians about nutrition and weight management. She stated that one of her main goals is to better engage primary care physicians in weight management programs and initiatives.
With the exception of the registered dietitian, none of the healthcare providers who participated were actively engaged in weight management programs for patients, including research initiatives. The providers had mixed opinions about the extent to which these weight management programs were useful. Most agreed that the success of these programs really depends on the patients themselves, with the most likely benefit among those who are extremely motivated and have resources.
According to the providers, one of the barriers to engaging patients in the current hospital programs is the fact that weight management programs are typically not covered by insurance. Thus, for many patients, these programs are very expensive. All of the providers stated that they were aware of other weight management programs that their patients were using outside their practices, especially Weight Watchers. Overall, they had a positive attitude towards these outside programs. They believed that if these programs promote physical activity, healthy eating, and gradual weight loss, then they are useful initiatives. A few providers worried that some of these programs were a “quick fix” and not sustainable. Most of the providers do not actively refer their patients to other weight management programs outside their practices but support the patients if they use such programs. For example, one PCP said, “I encourage my patients to do whatever works for them.”
In general, most providers had positive attitudes towards online weight management tools and programs because of routine access to smartphones, which enable people with limited resources to have access to these programs. Specifically, they mentioned LoseIt! and MyFitnessPal as programs their patients had used successfully. Below are some representative comments from the providers:
My attitudes (towards the online weight management tools/programs) are pretty pragmatic. If it works for you, then it’s great.
I think generally it’s a great idea. You have your coach in your pocket.
Specific Feedback About Our Proposed Intervention
In general, providers felt that there was great value in having a reliable online program that providers can recommend to their patients. Specifically, they appreciated the various features of the online program. All providers were overwhelmingly positive about our proposed intervention. They believed that the integration of an online program with PHM support could be a powerful and effective weight management strategy. There was a consensus about the importance of the PHM role in this type of intervention—“The human touch,” as one of the providers said. According to them, patients need this support to overcome problems and to feel that someone cares about them. For example, one provider stated that
You might feel accountable to your smartphone; but you might feel more accountable to your smartphone plus the population health managers that call you on Tuesday. I think it’s great!
All providers also saw great value in receiving information about their patients from this program. Some providers wanted to receive information about all their patients who engaged in the program and some only about ones who had issues (e.g., lost a lot of weight in a short time period). Most providers (especially the physicians) stated that they would like to receive a concise report about their patients. They wanted the report to include a list of their patients, how much weight they had lost, and if there were any important issues that they should know about (red flags). All providers thought that eventually they would like the information incorporated and viewable in the electronic health record (EHR); other options for receiving information were via email and/or meeting with the PHMs. Some thought that once per month is a reasonable time period for updates, and others preferred a time period of once every two to three months.
When asked if they were interested in having direct access to the patient online weight management program, the providers reported that they would not have the time to use it. The providers had mixed opinions about communicating with their patients via the online weight management program. Some stated that they encouraged patients to communicate with them via the patient portal within the EHR. Nevertheless, communicating with patients via a separate website (outside of the electronic health record) did not seem realistic to them.
DISCUSSION
We assessed perceptions among both patients and providers of experience with online weight management programs in general and with our proposed intervention (BMIQ online program integrated with PHM support). Our goal was also to identify strategies to overcome barriers to use and to iteratively improve the design and content of our intervention.
One key theme was that while most focus group participants had tried to lose weight previously, few had actually used formal weight management tools, even though most had positive impressions of them if they had previously used one. Interestingly, a few participants highlighted some strengths of the online weight management tools compared with in-person programs, stating that it is hard to follow through with the in-person programs, which could also be very expensive. Consistent with this notion, previous studies have shown that online weight management programs can help people achieve and maintain clinically meaningful weight loss,27,28,29,30,31,32,33,34,35,36 and that online programs may increase convenience and decrease the cost of lifestyle interventions.30, 38
Our findings from the semi-structured interviews with healthcare providers confirm and extend the findings from the patient focus groups, as well as from previous studies that have examined the current state of weight management in primary care.44 The majority of providers stated that while hospitals have weight management programs, primary care settings do not widely implement such programs. Moreover, providers had mixed opinions regarding the extent to which in-person weight management programs were useful.
In addition, most of the providers in this study had positive attitudes towards online weight management tools and programs because of their accessibility. Consistently, several studies indicate that even though PCPs perceived having important roles in patients’ successful weight management, they are not currently engaged in this process.14,15,16,17,18,19,20, 45 Other studies have shown that online weight management programs can help patients achieve weight loss in the primary care setting30, 39, 46 and be cost-effective.47
Finally, both patients and providers seemed to like our proposed intervention. They saw great value in having a reliable online program such as BMIQ and found its features important for weight management. All participants in this study (i.e., patients and providers) were overwhelmingly positive about the combination of the online program with PHM support. They believed that the integration of BMIQ and PHM support could be a very powerful and effective weight management strategy. Thus, there was consensus about the importance of the PHM in this type of intervention.
Our study was limited to patients and providers who were associated with BWH or one of its affiliated primary care clinics, which limits the generalizability of our results. In addition, the patients and providers who chose to participate may not be representative of all patients and providers at BWH. Future studies examining perspectives in a broader group of patients and healthcare providers, both at BWH and at other institutions, would be helpful.
Our patient focus groups and semi-structured interviews with healthcare providers highlight the potential value of online weight management programs and PHM support in primary care settings. While patients and healthcare providers expressed positive opinions about online weight management programs, few patients had tried them, representing an opportunity for a well-designed intervention. Providers confirmed that such programs are not being widely implemented in primary care settings. Thus, primary care clinics should consider developing and incorporating this type of program into their offerings and engage providers and patients in these important initiatives.
References
Flegal KM, Carroll MD, Kit BK, et al. Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999-2010. JAMA 2012;307:491–7.
Overweight, obesity, and health risk. National Task Force on the Prevention and Treatment of Obesity. Arch Intern Med 2000;160:898–904.
Flegal KM, Graubard BI, Williamson DF, et al. Excess deaths associated with underweight, overweight, and obesity. JAMA 2005;293:1861–7.
Ogden CL, Carroll MD, McDowell MA, et al. Obesity among adults in the United States no change since 2003-2004. Hyattsville: National Center for Health Statistics; 2007.
Ogden CL, Yanovski SZ, Carroll MD, et al. The epidemiology of obesity. Gastroenterology 2007;132:2087–102.
National Institutes of Health. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults--the evidence report Obes Res 1998;6 Suppl 2:51S–209S.
The prevention or delay of type 2 diabetes. Diabetes Care 2002;25:742–9.
Anderson JW, Konz EC. Obesity and disease management: effects of weight loss on comorbid conditions. Obes Res 2001;9 Suppl 4:326S–34S.
Franz MJ, VanWormer JJ, Crain AL, et al. Weight-loss outcomes: a systematic review and meta-analysis of weight-loss clinical trials with a minimum 1-year follow-up. J Am Diet Assoc 2007;107:1755–67.
Jensen MD, Ryan DH, Apovian CM, et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. Circulation 2013.
Hunt JR, Kristal AR, White E, et al. Physician recommendations for dietary change: their prevalence and impact in a population-based sample. Am J Public Health 1995;85(5):722–6.
Campbell MK, DeVellis BM, Strecher VJ, et al. Improving dietary behavior: the effectiveness of tailored messages in primary care settings. Am J Public Health 1994;84(5):783–7.
Nawaz H, Adams ML, Katz DL. Weight loss counseling by health care providers. Am J Public Health 1999;89(5):764–7.
Foster GD, Wadden TA, Makris AP, et al. Primary care physicians’ attitudes about obesity and its treatment. Obes Res 2003;11:1168–77.
Lyznicki JM, Young DC, Riggs JA, et al. Obesity: assessment and management in primary care. Am Fam Physician 2001;63:2185–96.
Shay LE, Shobert JL, Seibert D, et al. Adult weight management: translating research and guidelines into practice. J Am Acad Nurse Pract 2009;21:197–206.
Frank E, Kunovich-Frieze T. Physicians’ prevention counseling behaviors: current status and future directions. Prev Med 1995;24:543–5.
Huang J, Yu H, Marin E, et al. Physicians’ weight loss counseling in two public hospital primary care clinics. Acad Med 2004;79:156–61.
Logue EE, Smucker WD. Obesity management in primary care: changing the status quo. J Fam Pract 2001;50:520.
Wadden TA, Didie E. What’s in a name? Patients’ preferred terms for describing obesity. Obes Res 2003;11:1140–6.
Pew Research Center. 2014. Cell phone and smartphone ownership demographics URL: http://www.pewinternet.org/data-trend/mobile/cell-phone-and-smartphone-ownership-demographics [accessed 2019-03-20]
Greene J, Hibbard JH, Sacks R, et al. When patient activation levels change, health outcomes and costs change, too. Health Aff (Millwood) 2015;34(3):431–437.
Grando MA, Rozenblum R, Bates DW, editors. Information technology for patient empowerment in healthcare. 1st ed. Berlin: Walter de Gruyter Inc; 2015.
Hibbard JH, Greene J, Overton V. Patients with lower activation associated with higher costs; delivery systems should know their patients’ ‘scores’. Health Aff (Millwood) 2013 Feb;32(2):216–222.
Rozenblum R, Donzé J, Hockey PM, et al. The impact of medical informatics on patient satisfaction: a USA-based literature review. Int J Med Inform 2013;82(3):141–58.
Broderick A, Haque F. Mobile health and patient engagement in the safety net: a survey of community health centers and clinics. Issue Brief (Commonw Fund) 2015;9:1–9.
Coons MJ, Demott A, Buscemi J, et al. Technology interventions to curb obesity: a systematic review of the current literature. Curr Cardiovasc Risk Rep 2012;6:120–34.
Harvey-Berino J, Pintauro S, Buzzell P, et al. Does using the Internet facilitate the maintenance of weight loss? Int J Obes Relat Metab Disord 2002;26:1254–60.
Harvey-Berino J, Pintauro S, Buzzell P, et al. Effect of internet support on the long-term maintenance of weight loss. Obes Res 2004;12:320–9.
McTigue KM, Conroy MB. Use of the internet in the treatment of obesity and prevention of type 2 diabetes in primary care. Proc Nutr Soc 2013;72:98–108.
Neve M, Morgan PJ, Jones PR, et al. Effectiveness of web-based interventions in achieving weight loss and weight loss maintenance in overweight and obese adults: a systematic review with meta-analysis. Obes Rev 2009.
Norman GJ, Zabinski MF, Adams MA, et al. A review of eHealth interventions for physical activity and dietary behavior change. Am J Prev Med 2007;33:336–45.
Saperstein SL, Atkinson NL, Gold RS. The impact of Internet use for weight loss. Obes Rev 2007;8:459–65.
Svetkey LP, Stevens VJ, Brantley PJ, et al. Comparison of strategies for sustaining weight loss: the weight loss maintenance randomized controlled trial. JAMA 2008;299:1139–48.
Weinstein PK. A review of weight loss programs delivered via the Internet. J Cardiovasc Nurs 2006;21:251–8;259-60.
Wing RR, Tate DF, Gorin AA, et al. A self-regulation program for maintenance of weight loss. N Engl J Med 2006;355:1563–71.
Bennett GG, Herring SJ, Puleo E, et al. Web-based weight loss in primary care: a randomized controlled trial. Obesity (Silver Spring) 2009.
Ahern DK, Phalen JM, Mockenhaupt RE. Science and the advancement of eHealth: a call to action. Am J Prev Med 2003;24:108–9.
Levine DM, Savarimuthu S, Squires A, et al. Technology-assisted weight loss interventions in primary care: a systematic review. J Gen Intern Med 2014.
BMIQ professional program. https://www.bmiq.com/. Accessed 20 March 2019.
Wolf A, Knox L, Meeks K, et al. Efficacy to effectiveness: translating the ICAN lifestyle intervention to the real world. Paper presented at: The 33rd Annual Meeting of The Obesity Society, Obesity Week2015; Los Angeles, California.
Kornhauser N, Welch R, Cigler T, et al. Feasibility and effectiveness of BMIQ: a novel web-based weight loss program in overweight/obese breast cancer survivors. Paper presented at: The 33rd Annual Meeting of The Obesity Sociey, Obesity Week2015; Los Angeles, California.
Strauss A, Corbin J. Basics of qualitative research: techniques and procedures for developing grounded theory. 2nd ed. Thousand Oaks: Sage; 1998.
Tsai AG, Remmert JE, Butryn ML, Wadden TA. Treatment of obesity in primary care. Med Clin North Am 2018;102(1):35–47.
Bennett WL, Gudzune KA, Appel LJ, et al. Insights from the POWER practice-based weight loss trial: a focus group study on the PCP's role in weight management. J Gen Intern Med 2014;29(1):50–8.
Appel LJ, Clark JM, Yeh HC, et al. Comparative effectiveness of weight-loss interventions in clinical practice. N Engl J Med. 2011;365(21):1959–1968.
Little P, Stuart B, Hobbs FR, et al. An internet-based intervention with brief nurse support to manage obesity in primary care (POWeR+): a pragmatic, parallel-group, randomised controlled trial. Lancet Diabetes Endocrinol 2016;4(10):821–828.
Acknowledgments
Research reported in this presentation was funded through a Patient-Centered Outcomes Research Institute (PCORI) Award (14-092-1758). All statements in this report, including its findings and conclusions, are solely those of the authors and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute (PCORI), its Board of Governors, or its Methodology Committee.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This study is compliant with Ethical Standards.
Conflict of Interest
The authors declare that they do not have a conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendices
Appendix 1. Focus Group Guide (Focus Groups 1 and 2)
Focus Groups: Focus Group Guide





Appendix 2. Focus Group Guide (Focus Group 3)
Guide for the Third Focus Group





Appendix 3. Healthcare Providers’ Interview Guide
Healthcare Providers’ Interview Guide


Rights and permissions
About this article

Cite this article
Rozenblum, R., De La Cruz, B.A., Nolido, N.V. et al. Primary Care Patients’ and Providers’ Perspectives about an Online Weight Management Program: a Qualitative Study. J GEN INTERN MED 34, 1503–1521 (2019). https://doi.org/10.1007/s11606-019-05022-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-019-05022-6