
Abstract
Background
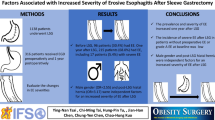
Laparoscopic sleeve gastrectomy (LSG) is one of the commonest bariatric procedures. However, it is associated with postoperative gastroesophageal reflux disease (GERD) and erosive esophagitis (EE). This study aims to assess the impact of various preoperative clinical and endoscopic characteristics on the development of postoperative GERD and EE.
Methods
This study is a single-institution retrospective cohort study involving all patients who underwent LSG. A univariate and multivariate analysis was performed to identify preoperative parameters that were significantly associated with the development of postoperative GERD and EE, at up to 1-year follow-up.
Results
At up to 1-year follow-up, out of 127 patients, only preoperative endoscopic presence of a hiatal hernia noted on axial length (p=0.024) and the Hill’s classification of the gastroesophageal junction (p<0.001) were significantly associated with the development of postoperative GERD. Similarly, at 1-year follow-up endoscopy, the presence of a hiatal hernia (p=0.041) and the Hill’s classification (p=0.001) were associated with postoperative EE. On the multivariate analysis, compared to patients with a Hill’s I flap valve, Hill’s II patients were more likely to develop postoperative GERD (OR 7.13, 95% CI: 1.69–29.98, p=0.007), and Hill’s III patients were more likely to develop postoperative GERD (OR 20.84, 95% CI: 3.98–109.13, p<0.001) and EE (OR 34.49, 95% CI: 1.08–1105.36, p=0.045). All patients with Hill’s IV developed postoperative GERD and EE in this study.
Conclusion
Postoperative GERD and EE remain an important limitation following LSG. Proper preoperative assessment using the Hill’s classification can help to accurately predict patients at risk of postoperative GERD and EE.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Laparoscopic sleeve gastrectomy (LSG) is one of the most common bariatric procedures performed worldwide, accounting for more than 50% of all bariatric procedures,1 and with respectable weight loss and metabolic benefits which are comparable to laparoscopic Roux-en-Y gastric bypass.2,3 However, one of the main disadvantages of LSG is its tendency to cause postoperative gastroesophageal reflux disease (GERD) or worsen underlying GERD.4 While it is widely accepted that the presence of a hiatal hernia predisposes to GERD,5 the presence of a hiatal hernia and its impact on patients who have undergone LSG is still controversial.6,7 Currently, the two commonly employed methods for endoscopic classification of a hiatal hernia are via its axial length,8 or by grading the laxity of the gastroesophageal junction and the presence or absence of a gastroesophageal flap valve, better known as the Hill’s classification system (see Supplementary Table 1).9
Interestingly, while the mechanisms involved in postoperative worsening of GERD or de novo GERD after LSG have been well documented,10,11,12 the factors predicting for postoperative GERD amongst patients undergoing LSG are not so evident.13 The aim of this study was to investigate the impact of preoperative demographic and endoscopic parameters, in particular the presence of a hiatal hernia, EE, and the preoperative Hill’s classification, in predicting for postoperative GERD and endoscopic evidence of EE amongst patients who have underwent LSG.
Materials and Methods
This is a single-institution retrospective cohort study of which all patients who have undergone LSG from 1st November 2018 to 31st July 2021 were reviewed. Demographic and preoperative endoscopy information was obtained. This study obtained institutional ethics board approval (2020/2482).
All patients who underwent LSG had undergone a prior multidisciplinary assessment to assess their medical fitness and indication and underwent lifestyle modifications with the help of a dedicated physiotherapist and dietician, as well as mental health assessment with a psychologist prior. They also underwent a routine preoperative endoscopic evaluation via an esophagogastroduodenoscopy to evaluate for the presence of any pathologies in the upper gastrointestinal tract, as well as to document the presence of any hiatal hernia, the preoperative Hill’s classification of the gastroesophageal junction, and the presence of any erosive esophagitis. The presence of a hiatus hernia was documented by the endoscopist performing the esophagogastroduodenoscopy. This was based on the position of the start of the gastric circular mucosal folds being proximal to the location of the diaphragmatic crural impression endoscopically. In cases where the endoscopist did not report the presence of a hiatus hernia on the endoscopy report, it was recorded as being absent. The Hill’s classification of the gastroesophageal junction was recorded by the endoscopist on retroflexion view of the gastroesophageal junction with the stomach fully distended.
The laparoscopic sleeve gastrectomy was performed using a standard 4- or 5-port technique, with a 40Fr bougie. Entry was performed via optical entry in the left hypochondrial region, followed by pneumoperitoneum and a diagnostic laparoscopy. Two working ports were placed in the midline and the right hypochondrial region, followed by an assistant port in the left hypochondrial region. A Nathanson liver retractor may be employed in the xiphisternum to expose the hiatus and retract the left lobe of the liver. For all patients reviewed, no concomitant hiatal hernia repairs were performed. Transection line was started 5cm proximal to the pylorus, and no omentopexies were performed.
Postoperatively, patients were reviewed by their bariatric surgeon after discharge, and the presence of any de novo or worsening preoperative GERD was documented. For this study, GERD was defined clinically by the presence of classical symptoms including heartburn and acid reflux. Patients, up to 1-year follow-up, reporting presence of typical reflux symptoms, or needing long-term proton pump inhibitors for alleviation of their symptoms, were considered to have presence of postoperative GERD. At 1-year follow-up, all patients also underwent a surveillance esophagogastroduodenoscopy to document the presence of any EE. EE was graded based on the Los Angeles classification.14 Patients with Los Angeles grade A to D were all considered to have EE.
Primary outcome measures include postoperative GERD symptoms at up to 1-year follow-up, and postoperative EE documented on postoperative esophagogastroduodenoscopy at 1-year follow-up. Data for continuous variables were presented as the mean with its standard deviation for variables with a normal distribution and the median with its interquartile range for skewed variables, while categorical variables were presented as n (%). Statistical analyses were performed via SPSS 26.0 (SPSS, Inc., Chicago, IL). Univariate analysis was performed using a chi-squared test for dichotomous independent variables, while an analysis of variance (ANOVA) test was employed for variables with 3 or more outcomes. A multivariate analysis was conducted via binomial logistical regression of all parameters and represented via their odds ratios (OR) with their 95% confidence intervals (CI). A p value of <0.05 was taken to be statistically significant.
Results
Characteristic of the Cohort
Between 1st November 2018 and 31st July 2021, a total of 127 patients had undergone LSG from a single academic medical institution and district general hospital. The median age and body mass index (BMI) of the patients were 37 years old (interquartile range: 33 to 47 years old) and 41.7 kg/m2 (interquartile range: 37.7 to 47.8) respectively. The basic demographic and endoscopic parameters of the patients were summarized in Table 1. In addition, 4 patients were on therapeutic anticoagulation prior (3.1%), 1 patient was suffering from depression (0.8%), and 2 patients were previous cancer survivors (1.6%). One of them had ovarian cancer while the other had endometrial cancer. All patients had not undergone any prior bariatric procedures. Based on the American Society of Anesthesiologists (ASA) for physical status classification,15 most patients were ASA class III (74.8%, n=95), with the remainder being ASA class II (23.6%, n=30). Except for 1 patient (0.8%), all patients were functionally independent prior to surgery.
The average length of stay was 3 days (interquartile range: 3 to 4 days). The mean operating time was 80.2 min (± 29.9 min). In total, 8 (6.8%) patients suffered from postoperative complications. All except 1 of them were Clavien-Dindo grade 2 complications,16 which included postoperative wound infection (n=1), postoperative vomiting (n=4), and postoperative hypoxemia (n=2). One patient had a staple line leak which required a laparoscopic omental patch repair of the staple line leak, with subsequent conversion to a laparoscopic Roux-en-Y gastric bypass. There were 6 (5.1%) patients who were readmitted within 30 days of discharge. These were due to wound infection (n=1), postoperative vomiting (n=3), constipation (n=1), and non-specific abdominal pain (n=1).
In total, there were 17 hiatal hernias that were reported in this study, with a mean axial length of 1.80cm (± 0.79 cm). All hiatal hernias recorded were type I sliding hernias determined based on the craniocaudal axial length on endoscopy. No patients with paraesophageal hernias were noted. Except for 2 patients with a 3-cm hiatal hernia, who also were graded as Hill’s grade IV, all the remaining patients have a hiatal hernia noted on axial length of 2cm or less.
Factors Contributing to Symptomatic GERD up to 1 Year After LSG
A total of 123 patients had available preoperative esophagogastroduodenoscopy information available for retrieval, of which 121 had documented the presence or absence of a hiatal hernia, and the Hill’s classification of the gastroesophageal junction. Most patients had no preoperative hiatal hernia based on axial length (86.0%, n=104). Most of them had a relatively tight gastroesophageal junction, with the majority being either Hill’s grade I or II (see Table 1). A total of 15 patients (11.8%) had preoperative documented EE on esophagogastroduodenoscopy. All of them were grade A (93.3%, 14/15), except for 1 patient with grade B EE. The incidence of preoperative symptomatic GERD was 10.2% (n=13).
At up to 1-year follow-up, 29.1% (37/127) patients had developed postoperative GERD symptoms. Out of this group, 33 of them (89.2%) denied any preoperative GERD symptoms, and hence had developed de novo GERD. A univariate analysis was performed to identify factors associated with postoperative symptomatic GERD (see Table 2). Only the presence of a preoperative hiatal hernia documented on axial length (p<0.024) and the preoperative Hill’s classification (p<0.001) were significantly associated with the development of postoperative symptomatic GERD at up to 1-year follow-up. On the multivariate analysis, compared to patients with Hill’s grade I, patients with Hill’s grade II (OR 7.13, 95% CI: 1.69–29.98, p=0.007) and III (OR 20.84, 95% CI: 3.98–109.13, p<0.001) were more likely to develop postoperative symptomatic GERD. All patients with Hill’s grade IV developed postoperative symptomatic GERD at up to 1-year follow-up (see Table 3).
Factors Contributing to EE at 1 Year After LSG
At the time of this study, a total of 64 patients had undergone postoperative esophagogastroduodenoscopy at 1-year follow-up. Of these, almost half (45.3%, 29/64) had developed EE on endoscopy. Majority of them were grade A (65.50%, 19/29), followed by grade B (24.1%, 7/29) and grade C (10.3%, 3/29).
A univariate analysis performed similarly identified only the presence of a preoperative hiatal hernia (p=0.041) and the preoperative Hill’s classification (p=0.001) to be significantly associated with the development of postoperative EE at 1-year follow-up (see Table 2). Interestingly, patients with symptomatic preoperative GERD appeared less likely to develop postoperative EE on the univariate analysis, though this did not reach statistical significance (p=0.081). A larger proportion of patients with preoperative EE on endoscopy had postoperative EE, although it also did not reach statistical significance (p=0.067).
A multivariate analysis was subsequently performed, which only identified the Hill’s classification as the only significant predictor for postoperative EE. Compared to patients with Hill’s grade I, patients with a Hill’s grade III gastroesophageal junction were more likely to develop postoperative EE (OR 34.49, 95% CI: 1.08–1105.36, p=0.045). All patients with Hill’s grade IV had postoperative EE (see Table 4).
Discussion
LSG has emerged as a desired bariatric procedure as it avoids an intestinal bypass,12 with robust weight loss outcomes,2,3 and it does not have a steep learning curve.17 However, with its increased adoption and increased long-term data made available, studies reported an increased rate of postoperative GERD and EE after LSG.4,12 Despite knowing the pathophysiologic mechanisms involved in causing de novo GERD, including the increase in intraluminal pressure, removal of the fundus, presence of a hiatal hernia, or disruption of the angle of His intraoperatively,12 there are reports that LSG may seem to improve pre-existing GERD as well.12 These relate to a decrease in intra-abdominal pressure from weight loss, loss of the stomach fundus and hence reduction in acid production, increased gastric emptying, and reduction in volume due to the tubularization of the stomach.12 As such, while the First International Consensus Conference recommended higher degrees of EE and Barrett’s esophagus to be contraindications for LSG,7 there was no consensus on the type of surgery for patients with pre-existing GERD symptoms, as well as patients with an underlying hiatal hernia.7 Furthermore, the factors predisposing to GERD and EE after LSG were not well elucidated.13
In this study, the prevalence of postoperative symptomatic GERD after LSG was 29.1%, with 26.0% of patients suffering from de novo GERD. This was comparable to that reported by Himpens et al., in their randomized controlled trial comparing LSG and gastric banding, where they reported a de novo GERD at 1-year of 21.8%.18 A total of 45.3% of patients suffered from postoperative EE, which was slightly lower than the 51.4% reported by Navarini et al., in their randomized controlled trial comparing LSG and laparoscopic Roux-en-Y gastric bypass on its impact on postoperative GERD.19 The authors postulate that this could be due to the smaller sample size of patients who had undergone their esophagogastroduodenoscopy at their 1-year follow-up, and it is expected that the incidence of postoperative EE will increase with subsequent follow-up. Interestingly, the prevalence of preoperative symptomatic GERD in this study population is relatively low, at just 10.2%. The authors postulate that this could be due to a lower prevalence of GERD in Asia,20,21,22 as well as possible under-reporting of symptoms amongst patients with un-investigated GERD.23
To our knowledge, this study was the first study to evaluate the Hill’s classification of the gastroesophageal junction on the likelihood of developing de novo or aggravating postoperative GERD or EE after LSG. In the univariate analysis, only the presence of a hiatal hernia and the Hill’s classification were significantly associated with postoperative symptomatic GERD and EE. Based on the multivariate analysis, only the preoperative Hill’s classification remained predictive for postoperative symptomatic GERD and EE (see Tables 3 and 4). Also, the magnitude of the association appeared to correlate with a higher Hill’s grading. All patients with a Hill’s grade IV developed postoperative symptomatic GERD and EE. Patients with a Hill’s grade III had significantly higher odds of developing postoperative symptomatic GERD (OR 20.84, 95% CI: 3.98–109.13, p<0.001) and EE (OR 34.49, 95% CI: 1.08–1105.36, p=0.045) compared to patients with Hill’s grade I flap valve. For patients with Hill’s grade II, there were significantly more patients with postoperative symptomatic GERD (OR 7.13, 95% CI: 1.69–29.98, p=0.007), but not EE (OR 3.76, 95% CI: 0.21–66.30, p=0.366). This study thus demonstrated that the Hill’s classification system of the laxity of the gastroesophageal junction, even after adjusting for other preoperative factors, appeared to be better than preoperative GERD symptoms, preoperative presence of a hiatal hernia, or preoperative EE in predicting for postoperative symptomatic GERD and EE.
The Hill’s classification, first introduced by Hill et al. in 1996, was derived from an observational study of 13 cadavers to determine the presence of an anti-reflux valve and hiatal hernia.9 In the absence of a hiatal hernia, the angle of His, defined as the acute angulation along the greater curve of the stomach where the esophagus enters the stomach,24 creates a flap valve mechanism.9,25 The laxity of this flap valve varies and can be objectively graded based on the Hill’s classification.9 This classification has been shown to be superior to the axial measurement of a hiatal hernia in the endoscopic assessment of the gastroesophageal junction and its association with GERD.8 This observation was similarly demonstrated in this study for patients who have undergone LSG as well. The authors believe that the predictive value of the Hill’s classification may be due to its ability to grade the mechanical laxity of the gastroesophageal junction. As previously demonstrated by Hill et al. in their cadaveric studies,9 despite the absence of an active lower esophageal sphincter in a cadaver, a mechanical pressure gradient still existed in patients without a hiatal hernia, with lower Hill’s grade classifications. This mechanical gradient can be recreated in cadavers with a hiatal hernia by suturing the gastroesophageal junction to the preaortic fascia to recreate the angle of His and the gastroesophageal flap valve.9 Various mechanisms are thought to be responsible in maintaining the normal gastroesophageal junction, including the physiologic lower esophageal sphincter pressure,24 the diaphragmatic crura,24 length of the intra-abdominal esophagus,24 and the angle of His24 with its associated gastroesophageal flap valve.9,24,25 Our current study findings suggest that the integrity of the gastroesophageal flap valve and the laxity of the gastroesophageal junction graded by the Hill’s classification may play a bigger role than previously thought, in determining the risk of GERD and EE after LSG.
Unlike measurement of the axial length of a hiatal hernia which is only useful to detect large hiatal hernias, the Hill’s classification system may potentially avoid missing patients with a lax gastroesophageal junction without a frank hiatal hernia. The use of axial length to grade a hiatal hernia can be subjective, with variations due to inspiration,3 as well as the physiologic shortening of the esophagus from either peristalsis, instrumentation, or distension.26 Thus, measurement of the axial length of a hiatal hernia is only useful to detect large sliding hiatal hernias. In this study, all patients diagnosed with a hiatal hernia on axial length had a type 1 sliding hiatal hernia, with a mean length of only 1.80cm (± 0.79cm). Given that a separation of the squamocolumnar junction from the crural impression of 2cm or less may still be considered physiological,26 this might explain the discrepancy in the number of patients with a hiatal hernia diagnosed on axial length on endoscopy (n=17), in contrast to the number of patients with a Hill’s grade IV (n=2). This finding was not unexpected given the retrospective nature of the study as patients with a large hiatal hernia noted on axial length would have been counseled for a laparoscopic Roux-en-Y gastric bypass instead of a LSG. Hence, this may explain why the presence of a hiatal hernia does not appear to significantly impact postoperative symptomatic GERD and EE on the multivariate analysis. This explained why none of the patients in this study population with a preoperative hiatal hernia had undergone a concomitant hiatal hernia repair, as most of these hernias were small. However, given that both patients with Hill’s grade IV have a true anatomical hiatal hernia on axial length (both were 3cm in length), the study finding further strengthened the reproducibility and correlation between the Hill’s classification system with the axial length measurement system on clinically significant hiatus hernias. Furthermore, the study findings also support the Hill’s classification system as a predictive tool to stratify patients, who may not have a frank hiatal hernia, on their risk of postoperative symptomatic GERD and EE. In this context, the Hill’s classification in grading the laxity of the gastroesophageal junction and its impact on postoperative symptomatic GERD and EE may play a more important role than previously thought, as most patients undergoing LSG were likely those without any large hiatal hernias that can be detected on axial length.
It is hoped that these study findings can help in creating a standardized reporting system for preoperative esophagogastroduodenoscopy findings for patients undergoing LSG. On top of preoperative symptom evaluation of GERD, the axial length of any hiatal hernia, and the presence of EE, the Hill’s classification of the gastroesophageal junction should also be documented. Based on the current study findings, at up to 1-year follow-up, less than one quarter and half of patients with Hill’s grade I or Hill’s grade II developed symptomatic GERD and EE after LSG respectively. In contrast, more than 50% of patients with Hill’s grade III had postoperative symptomatic GERD at up to 1-year follow-up, with a majority developing postoperative EE at 1-year follow-up. Lastly, all patients with Hill’s grade IV had symptomatic GERD and postoperative EE by 1 year. Thus, the authors believe that while LSG may be acceptable for patients with Hill’s grades I and II, patients with Hill’s grades III and IV might be better served with an alternative bariatric procedure instead, such as a laparoscopic Roux-en-Y gastric bypass, or a LSG with a hiatal hernia repair. In this study, patients with preoperative GERD, EE, or hiatal hernia were offered laparoscopic Roux-en-Y gastric bypass, with LSG as an alternative. Patients included in this study had decided to proceed with LSG after an informed decision-making process.
Currently, opinions remain divided for patients with GERD symptoms undergoing bariatric surgery. Results from the First International Consensus Conference reported that slightly more than half of the surgeons surveyed will still recommend a LSG or a LSG with an anti-reflux procedure for patients with GERD symptoms.7 In the presence of an asymptomatic hiatal hernia, most surgeons will opt for a repair and closure of the hiatus during surgery.7 More studies are needed to determine the ideal surgical technique for such patients predisposed to GERD and EE after LSG. Initial results for concomitant LSG-fundoplication were associated with increased complication rates.27 The authors also eagerly await the results of the RELIEF trial, which investigated the role of LINXTM magnetic sphincter augmentation in patients with postoperative GERD after LSG that has recently finished recruitment (ClinicalTrials.gov identifier: NCT02429830).
This study has several limitations. Firstly, it is a single-institution retrospective cohort study, hence prone to information and recall bias. Also, the follow-up period is short at only 1 year, and only a subgroup of patients (n=64) had undergone esophagogastroduodenoscopy at the end of 1 year. However, this subgroup of patients had similar outcomes as the entire cohort and hence was likely a representative sample for the analysis. In addition, GERD symptoms exist as a spectrum with varying degrees of severity, which may not be well represented in this study, which was reported as either present or absent. It is also unclear if the presence of a Los Angeles grade A esophagitis, which is itself subject to potential interobserver and intraobserver differences,28 would correlate with any clinically meaningful GERD. Also, the proportion of patients requiring preoperative proton pump inhibitors was unavailable. However, given that more than half of patients with postoperative symptomatic GERD had postoperative EE (51.7%), as well as the similar preoperative correlations between both GERD and EE outcomes, these outcome measures were likely clinically relevant. In addition, the presence of preoperative EE appeared to correlate with postoperative EE on the univariate analysis, though it did not reach statistical significance (p=0.067). The lack of such an association seen on the multivariate analysis might be related to the limited sample size in this study. Lastly, the study population is a heterogeneous multi-ethnic Asian population, which may not be applicable to other regions. However, even with these limitations, the authors believe that the study findings are important, as it is the first study to document the importance of the laxity of the gastroesophageal junction, graded by the Hill’s classification system on predicting postoperative GERD and EE after LSG. Furthermore, the authors believe the study findings may potentially help shed light on the clinical importance of the gastroesophageal flap valve in maintaining the integrity of the gastroesophageal junction, both in physiologic and diseased states, as well as in cases where the stomach is tubularized such as after an LSG.
Conclusion
In conclusion, the study findings demonstrated that the Hill’s classification system is paramount in predicting the development of postoperative GERD and postoperative EE after LSG in bariatric surgery patients.
References
Berger ER, Huffman KM, Fraker T, Petrick AT, Brethauer SA, Hall BL, Ko CY, Morton JM. Prevalence and Risk Factors for Bariatric Surgery Readmissions: Findings From 130,007 Admissions in the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program. Ann Surg. 2018 Jan;267(1):122-131.
Peterli R, Wölnerhanssen BK, Peters T, Vetter D, Kröll D, Borbély Y, Schultes B, Beglinger C, Drewe J, Schiesser M, Nett P, Bueter M. Effect of Laparoscopic Sleeve Gastrectomy vs Laparoscopic Roux-en-Y Gastric Bypass on Weight Loss in Patients With Morbid Obesity: The SM-BOSS Randomized Clinical Trial. JAMA. 2018 Jan 16;319(3):255-265.
Salminen P, Helmiö M, Ovaska J, Juuti A, Leivonen M, Peromaa-Haavisto P, Hurme S, Soinio M, Nuutila P, Victorzon M. Effect of Laparoscopic Sleeve Gastrectomy vs Laparoscopic Roux-en-Y Gastric Bypass on Weight Loss at 5 Years Among Patients With Morbid Obesity: The SLEEVEPASS Randomized Clinical Trial. JAMA. 2018 Jan 16;319(3):241-254.
Yeung KTD, Penney N, Ashrafian L, Darzi A, Ashrafian H. Does Sleeve Gastrectomy Expose the Distal Esophagus to Severe Reflux?: A Systematic Review and Meta-analysis. Ann Surg. 2020 Feb;271(2):257-265.
Sgouros SN, Mpakos D, Rodias M, Vassiliades K, Karakoidas C, Andrikopoulos E, Stefanidis G, Mantides A. Prevalence and axial length of hiatus hernia in patients, with nonerosive reflux disease: a prospective study. J Clin Gastroenterol. 2007 Oct;41(9):814-8. doi: https://doi.org/10.1097/01.mcg.0000225678.99346.65.
Lye TJY, Ng KR, Tan AWE, Syn N, Woo SM, Lim EKW, Eng AKH, Chan WH, Tan JTH, Lim CH. Small hiatal hernia and postprandial reflux after vertical sleeve gastrectomy: A multiethnic Asian cohort. PLoS One. 2020 Nov 6;15(11):e0241847.
Assalia A, Gagner M, Nedelcu M, Ramos AC, Nocca D. Gastroesophageal Reflux and Laparoscopic Sleeve Gastrectomy: Results of the First International Consensus Conference. Obes Surg. 2020 Oct;30(10):3695-3705.
Hansdotter I, Björ O, Andreasson A, Agreus L, Hellström P, Forsberg A, Talley NJ, Vieth M, Wallner B. Hill classification is superior to the axial length of a hiatal hernia for assessment of the mechanical anti-reflux barrier at the gastroesophageal junction. Endosc Int Open. 2016 Mar;4(3):E311-7.
Hill LD, Kozarek RA, Kraemer SJ, Aye RW, Mercer CD, Low DE, Pope CE 2nd. The gastroesophageal flap valve: in vitro and in vivo observations. Gastrointest Endosc. 1996 Nov;44(5):541-7.
Sharma A, Aggarwal S, Ahuja V, Bal C. Evaluation of gastroesophageal reflux before and after sleeve gastrectomy using symptom scoring, scintigraphy, and endoscopy. Surg Obes Relat Dis. 2014 Jul-Aug;10(4):600-5.
Rebecchi F, Allaix ME, Giaccone C, Ugliono E, Scozzari G, Morino M. Gastroesophageal reflux disease and laparoscopic sleeve gastrectomy: a physiopathologic evaluation. Ann Surg. 2014 Nov;260(5):909-14; discussion 914-5.
Stenard F, Iannelli A. Laparoscopic sleeve gastrectomy and gastroesophageal reflux. World J Gastroenterol. 2015 ;21(36):10348-57.
Althuwaini S, Bamehriz F, Aldohayan A, Alshammari W, Alhaidar S, Alotaibi M, Alanazi A, Alsahabi H, Almadi MA. Prevalence and Predictors of Gastroesophageal Reflux Disease After Laparoscopic Sleeve Gastrectomy. Obes Surg. 2018 Apr;28(4):916-922.
Lundell LR, Dent J, Bennett JR, Blum AL, Armstrong D, Galmiche JP, Johnson F, Hongo M, Richter JE, Spechler SJ, Tytgat GN, Wallin L. Endoscopic assessment of oesophagitis: clinical and functional correlates and further validation of the Los Angeles classification. Gut. 1999 Aug;45(2):172-80.
Dripps RD. New classification of physical status. Anesthesiol. 1963;24:111
Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD, de Santibañes E, Pekolj J, Slankamenac K, Bassi C, Graf R, Vonlanthen R, Padbury R, Cameron JL, Makuuchi M. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009 Aug;250(2):187-96.
Zacharoulis D, Sioka E, Papamargaritis D, Lazoura O, Rountas C, Zachari E, Tzovaras G. Influence of the learning curve on safety and efficiency of laparoscopic sleeve gastrectomy. Obes Surg. 2012 Mar;22(3):411-5.
Himpens J, Dapri G, Cadière GB. A prospective randomized study between laparoscopic gastric banding and laparoscopic isolated sleeve gastrectomy: results after 1 and 3 years. Obes Surg. 2006 Nov;16(11):1450-6.
Navarini D, Madalosso CAS, Tognon AP, Fornari F, Barão FR, Gurski RR. Predictive Factors of Gastroesophageal Reflux Disease in Bariatric Surgery: a Controlled Trial Comparing Sleeve Gastrectomy with Gastric Bypass. Obes Surg. 2020 Apr;30(4):1360-1367.
Ho KY. Gastroesophageal reflux disease is uncommon in Asia: evidence and possible explanations. World J Gastroenterol. 1999 Feb;5(1):4-6.
Wu JC. Gastroesophageal reflux disease: an Asian perspective. J Gastroenterol Hepatol. 2008 Dec;23(12):1785-93.
Richter JE, Rubenstein JH. Presentation and Epidemiology of Gastroesophageal Reflux Disease. Gastroenterology. 2018 Jan;154(2):267-276.
Hojo M, Nagahara A, Hahm KB, Iwakiri R, Watanabe T, Rani AA, Zhu Q, Chan FKL, Sollano JD, Kamiya T, Yamaguchi S, Motoya S, Fock KM, Fukudo S, Kachintorn U, Suzuki H, Murakami K; The International Gastroenterology Consensus Symposium Study Group. Management of Gastroesophageal Reflux Disease in Asian Countries: Results of a Questionnaire Survey. Digestion. 2020;101(1):66-79.
Holloway RH. The anti-reflux barrier and mechanisms of gastro-oesophageal reflux. Baillieres Best Pract Res Clin Gastroenterol. 2000 Oct;14(5):681-99.
Thor KB, Hill LD, Mercer DD, Kozarek RD. Reappraisal of the flap valve mechanism in the gastroesophageal junction. A study of a new valvuloplasty procedure in cadavers. Acta Chir Scand. 1987 Jan;153(1):25-8.
Kahrilas PJ, Kim HC, Pandolfino JE. Approaches to the diagnosis and grading of hiatal hernia. Best Pract Res Clin Gastroenterol. 2008;22(4):601-16.
Aiolfi A, Micheletto G, Marin J, Rausa E, Bonitta G, Bona D. Laparoscopic Sleeve-Fundoplication for Morbidly Obese Patients with Gastroesophageal Reflux: Systematic Review and Meta-analysis. Obes Surg. 2021 Apr;31(4):1714-1721.
Kusano M, Ino K, Yamada T, Kawamura O, Toki M, Ohwada T, Kikuchi K, Shirota T, Kimura M, Miyazaki M, Nakamura K, Igarashi S, Tomizawa M, Tamura T, Sekiguchi T, Mori M. Interobserver and intraobserver variation in endoscopic assessment of GERD using the “Los Angeles” classification. Gastrointest Endosc. 1999 Jun; 49(6): 700-4.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information

Rights and permissions
About this article

{kind=link}
Cite this article
Chue, K.M., Goh, D.W.X., Chua, C.M.E. et al. The Hill’s Classification Is Useful to Predict the Development of Postoperative Gastroesophageal Reflux Disease and Erosive Esophagitis After Laparoscopic Sleeve Gastrectomy. J Gastrointest Surg 26, 1162–1170 (2022). https://doi.org/10.1007/s11605-022-05324-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-022-05324-x