
Abstract
Purpose
We evaluated the associations between gestational age (GA) and lung-to-liver signal intensity ratio (LLSIR) and fetal lung volume (FLV) using magnetic resonance imaging (MRI). Moreover, we evaluated the reproducibility of these measurements.
Materials and methods
LLSIR and FLV were measured using single-shot fast spin-echo MRI in 88 consecutive fetuses. The Spearman test was used to assess the relationships between (1) LLSIR and GA, and (2) FLV and GA in 81 fetuses without lung abnormalities. Intra- and inter-observer reliabilities were assessed using intra-class correlation coefficients (ICCs).
Results
Overall, GA and LLSIR were significantly correlated (r = 0.62, p < 0.001). However, GA and LLSIR were only significantly correlated during the third trimester (before third trimester: r = 0.39, p = 0.08; during third trimester: r = 0.46, p < 0.001). Overall, GA and FLV were significantly correlated (r = 0.72, p < 0.001). FLV was significantly correlated with GA before (r = 0.86, p < 0.001) and during the third trimester (r = 0.47, p < 0.001). All ICCs were above 0.90.
Conclusions
LLSIR and FLV are useful for the assessment of fetal lung maturity and are highly reproducible. Before the third trimester, FLV is more suitable than LLSIR for the evaluation of fetal lung maturity.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Fetal lung development is important for the perinatal prognosis [1], as the lungs must be able to adapt to the changing physiologic processes during pregnancy and after birth. Assessments of lung maturity are helpful in the planning of delivery and parental counseling. Fetal lung maturity is frequently assessed by the lecithin and surfactant levels in the amniotic fluid [2]; however, an invasive procedure is required. In contrast, echography and magnetic resonance imaging (MRI) can assess fetal lung development non-invasively. Although lung maturity assessments on echography, such as observed/expected lung to-head ratio and the quantitative lung index, are widely used by obstetricians, otherwise, the observation of fetal lung by echography is affected by operator experience. Compared to that achieved in echography, MRI offers a larger field of view, better tissue contrast, and the absence of bone shadowing [3]. Furthermore, MRI visualization of the fetus is not significantly limited by maternal obesity or fetal position. Moreover, MRI provides multiplanar imaging. MRI during the second or third trimester of pregnancy is considered safe for the fetus [4]. In addition, a recent study showed that exposure to MRI during the first trimester of pregnancy was not associated with an increased risk of harm to the fetus or adverse events in the early childhood [5]. Therefore, MRI is highly useful in detecting fetal lung abnormalities, such as lung hypoplasia, diaphragmatic hernia, and lung masses.
MRI assessments of lung maturity involve the measurement of the lung volume or signal intensity, as the lung signal intensity and fetal lung volume (FLV) increase with fetal lung development [6, 7]. In addition, low signal intensity indicates pulmonary hypoplasia [8]. However, it remains unclear which index is more suitable for determining lung maturity. Moreover, a few studies have evaluated the intra- and inter-observer reproducibility of these indexes [9]. Therefore, the purpose of the present study was to evaluate the associations between gestational age and FLV and lung signal intensity measurements of normal lungs. In addition, we examined the reproducibility of these indexes.
Materials and methods
Study population
This retrospective study was approved by the institutional review board of our university; the requirement for informed consent was waived. Ninety-three fetuses who underwent comprehensive MRI (1.5 T) examination between May 2009 and May 2017 were retrospectively reviewed. Those with defective image quality (n = 5) were excluded, and the remaining 88 fetuses were analyzed. Of these, seven fetuses had lung abnormalities [death (n = 1), congenital diaphragmatic hernia (n = 4), and congenital pulmonary airway malformation (CPAM) or tumor (n = 2)], while 81 fetuses had no lung abnormalities. Fetuses without lung abnormalities were divided into two groups, based on the gestational age: less than 28 weeks (before the third trimester) and more than 29 weeks (during the third trimester). Gestational periods were defined in accordance with Women’s Health at the US Department of Health and Human Services (first trimester, weeks 1–12; second trimester, weeks 13–28; and third trimester, weeks 29–40).
MRI protocol
All studies were performed using a whole-body 1.5-T MRI scanner (Achieva 1.5 T Nova; Philips Healthcare, Best, The Netherlands). A single-shot fast spin-echo sequence was performed in the transverse, sagittal, and coronal planes of the fetus. The parameters were as follows: TR/TE, 4000/120 ms; flip angle, 90°; section thickness, 5 mm; field of view, 380 mm; matrix, 288 × 192; and number of signals acquired, 1.
Signal intensity measurement
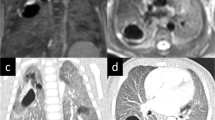
The lung-to-liver signal intensity ratio (LLSIR) was measured independently by two radiologists using the Osirix software. The signal intensities of the lung and liver were measured in the same slice. The selected areas had homogeneous signal intensity and were free of vascular and tracheal structures (Fig. 1a). For cases of CPAM or tumor, the hyperintense lesion of the lung was selected. The LLSIR was measured three times per lung, with each measurement taken from a different image and/or section, and when possible, from a different orientation plane, as previously reported [10]. The average of the three ratios was adopted. To determine intra-observer variability, the LLSIR was measured 2 weeks after the initial evaluation for all 88 fetuses.

Coronal single-shot fast spin-echo magnetic resonance image in a fetus as 32 weeks of gestational age. a Signal intensity measurement. Regions of interest in the liver and lung. b Lung volume measurement
Lung volume measurement
Two radiologists independently evaluated the FLV using Osirix software, which calculates the volume by multiplying the surface area and slice thickness to determine the slice volume and automatically adding up the slice volumes [11]. For both abnormal and normal lungs, the lung parenchyma was included, while the pulmonary hilum was excluded, as in a previous report (Fig. 1b) [12]. Lung volume was measured in the plane (transverse, sagittal, or coronal) with the best image quality, in which the whole lung could be observed. The previous studies have shown that FLV measurements are independent of section thickness and imaging plane [12]. To determine intra-observer variability, FLV measurements were repeated at 2 weeks after the initial evaluation for all 88 fetuses.
Statistical analyses
Continuous data are expressed as the mean ± standard deviation or median (first quartile and third quartile), in accordance with the distribution. The intra- and inter-observer agreements were assessed using the intra-class correlation coefficient (ICC). For fetuses without lung abnormalities, the Spearman test was used to assess the relationships between (1) signal intensity and gestational age, and (2) FLV and gestational age. A p value < 0.05 was considered statistically significant. All statistical analyses were performed using the JMP software (version 11.2; SAS Institute, Inc., Cary, NC, USA), and SPSS version 19 (SPSS, Chicago, IL, USA).
Results
Characteristics of the fetuses without lung abnormalities (n = 81)
The reasons for the MRI examinations of the fetuses without lung abnormalities (n = 81) are provided in Table 1. A total of 22 fetuses were scanned before the third trimester, and 59 fetuses were scanned during the third trimester. The median gestational age was 32 [interquartile range (IQR) 28–34.5] weeks in all fetuses without lung abnormalities, 25.5 (IQR 16.8–27) weeks in those scanned before the third trimester, and 33 (IQR 31–35) weeks in those scanned during the third trimester.
Reproducibility of LLSIR and FLV measurements
The intra- and inter-observer ICCs were, respectively, 0.96 [95% confidence interval (CI) 0.94–0.97, p < 0.001] and 0.93 (95% CI 0.83–0.97, p < 0.001) for the LLSIR, and were 0.94 (95% CI 0.90–0.96, p < 0.001) and 0.91 (95% CI 0.68–0.96, p < 0.001) for the FLV.
Relationship between gestational age and the LLSIR in fetuses without lung abnormalities (n = 81)
The median LLSIR was 2.6 (IQR 2.2–3.3). Overall, the LLSIR was significantly correlated with gestational age (r = 0.62, p < 0.001) (Table 2). The overall association between gestational age and the LLSIR was represented by the following equation: LLSIR = 0.07 × g + 0.67, where g is the gestational age (Fig. 2). In terms of gestational age groups, the LLSIR and gestational age were not significantly correlated before the third trimester(r = 0.39, p = 0.08), but were significantly correlated during the third trimester (r = 0.46, p < 0.001).

Relationship between the lung-to-liver signal intensity ratio (LLSIR) and gestational age. Filled circle indicates normal lung, open circle indicates congenital diaphragmatic hernia, open triangle indicates congenital pulmonary airway malformation or tumor, and times symbol indicates death
Relationship between gestational age and FLV in fetuses without lung abnormalities (n = 81)
The median selected slice number for the FLV measurement was 7 (IQR 5–10) and the median FLV was 43.3 (IQR 30.2–57.7) ml. Overall, gestational age and FLV were significantly correlated (r = 0.72, p < 0.001) (Table 2). The association between gestational age and FLV was represented by the following equation: FLV = 0.6727e0.1311g, where g is the gestational age (Fig. 3). In terms of gestational age groups, FLV and gestational age were significantly correlated before (r = 0.86, p < 0.001) and during the third trimester (r = 0.47, p < 0.001).

Relationship between fetal lung volume (FLV) and gestational age. Filled circle indicates normal lung, open circle indicates congenital diaphragmatic hernia, open triangle indicates congenital pulmonary airway malformation or tumor, and times symbol indicates death
Characteristics of the fetuses with lung abnormalities (n = 7)
The LLSIR and FLV of the lung abnormalities are shown in Table 3. To compare with normal lungs, the LLSIRs of lung abnormalities are also provided in Fig. 2. The LLSIR in cases of CPAM or tumor exceeded the upper prediction intervals. The FLVs of lung abnormalities are also provided in Fig. 3.
Discussion
In contrast to a previous report [8], the present study focused on whether the LLSIR or FLV was more suitable for determining normal lung maturation and on the reproducibility of these indexes. The main findings are as follows: (1) FLV and LLSIR measurements are highly reproducible, (2) both FLV and the LLSIR are correlated with gestational age, and (3) FLV is more suitable than the LLSIR before the third trimester.
Reproducibility of LLSIR and FLV measurements
In the present study, the intra- and inter-observer agreements for the LLSIR were beyond 0.7. This high reproducibility might be due to the careful selection of an area with homogeneous signal intensity, free of vascular and tracheal structures, and the use of the average ratio from three measurements. The intra- and inter-observer agreements for the FLV were also beyond 0.7, regardless of whether manual tracing of the contour was performed. Choosing the plane with the best image quality, and in which the whole lung could be observed, is thought to have contributed to the high reproducibility in the FLV measurement. This high reproducibility should be considered an advantage of MR assessments of lung maturity.
Relationship between gestational age and the LLSIR in fetuses without lung abnormalities
Signal intensity values have high variance in the fetal lung. Therefore, the signal intensity should be compared to that of another structure [13]. Some studies have used the cerebrospinal fluid [14], fetal muscle, or the spleen [15]. However, the liver was used in the present study, as the liver touches the lungs and can be measured on the same slice.
Fetal lung fluid increases with growth and is necessary for lung maturation. Fetal lung development can be categorized as follows: the embryonal (conception—6 weeks), pseudoglandular (6–16 weeks), canalicular (16–28 weeks), saccular (28–36 weeks), and alveolar (36 weeks—term) phases [16]. At the beginning of the pregnancy, the fetal lungs are not filled with fluid. Therefore, an increase in signal intensity is scarce before the third trimester, consistent with the present results. With maturation, the fetal lungs become filled with fluid, as lung fluid is secreted from the epithelial cells, with production starting in the late canalicular stage [1]. Moreover, with fetal lung development, the alveoli and bronchioles become thinner, and the lungs become filled with even more amniotic fluid [17]. In the present study, the LLSIR and gestational age were not correlated before the third trimester, but were correlated during the third trimester. This result is thought to reflect the progression in fetal lung maturity.
In addition, the LLSIR exceeded the upper prediction intervals in cases of CPAM or tumor in this study (Fig. 2). Thus, the LLSIR may have the potential to detect abnormal lungs.
Relationship between gestational age and the FLV in fetuses without lung abnormalities
In the present study, the association between gestational age and FLV was represented by the equation: FLV = 0.6727e0.1311g, where g is the gestational age. In the estimation of the final lung volume, it is important to consider this exponential development. A previous study similarly represented normal FLV development exponentially [18]. However, other studies have reported variations in the representation of normal FLV development [19]. These inconsistent results may be related to differences in the methods for volume assessment and differences in the proportion of fetuses across trimesters.
In the present study, the FLV had a higher correlation with gestational age before the third trimester compared to that during the third trimester. This result is related to the large amount of individual variation in the FLV during late pregnancy [19, 20]. Thus, the FLV is a useful index for fetal lung maturity, especially before the third trimester. Actually, the FLV tended to be lower in cases of congenital diaphragmatic hernia compared to that in normal fetuses (Fig. 3).
Limitations
The present study has several limitations. Although FLV data for fetuses of younger gestational age are important, as it is related to the indication of abortion, the present study had little data on fetuses before the third trimester. The previous studies have similarly had little data on fetuses of younger age [3]. Therefore, more data on younger fetuses are needed. Second, the same fetuses were not examined at different times to evaluate changes in the LLSIR and FLV. Third, we did not examine the relationships between outcomes and these indexes (LLSIR and FLV). Because various factors can affect the outcomes, an accurate correlation between the pregnancy outcomes and these indexes is difficult to examine. As a reference, a previous study reported that a cut-off value of 2.00 for the LLSIR is optimal in predicting the neonatal occurrence of respiratory distress [1].
Conclusions
LLSIR and FLV measurements are associated with gestational age, and these indexes are highly reproducible. The FLV is more correlated with gestational age before third trimester than during the third trimester, and is a more suitable index of lung maturity than the LLSIR during the early pregnancy.
References
Oka Y, Rahman M, Sasakura C, Waseda T, Watanabe Y, Fujii R, et al. Prenatal diagnosis of fetal respiratory function: evaluation of fetal lung maturity using lung-to-liver signal intensity ratio at magnetic resonance imaging. Prenat Diagn. 2014;34:1289–94.
O’Brien WF, Cefalo RC. Clinical applicability of amniotic fluid tests for fetal pulmonic maturity. Am J Obstet Gynecol. 1980;136:135–44.
Rubesova E. Why do we need more data on MR volumetric measurements of the fetal lung? Pediatr Radiol. 2016;46:167–71.
Jaffe TA, Miller CM, Merkle EM. Practice patterns in imaging of the pregnant patient with abdominal pain: a survey of academic centers. AJR Am J Roentgenol. 2007;189:1128–34.
Ray JG, Vermeulen MJ, Bharatha A, Montanera WJ, Park AL. Association between MRI exposure during pregnancy and fetal and childhood outcomes. JAMA. 2016;316:952–61.
Moshiri M, Mannelli L, Richardson ML, Bhargava P, Dubinsky TJ. Fetal lung maturity assessment with MRI fetal lung-to-liver signal-intensity ratio. AJR Am J Roentgenol. 2013;201:1386–90.
Kasprian G, Balassy C, Brugger PC, Prayer D. MRI of normal and pathological fetal lung development. Eur J Radiol. 2006;57:261–70.
Kuwashima S, Nishimura G, Iimura F, Kohno T, Watanabe H, Kohno A, et al. Low-intensity fetal lungs on MRI may suggest the diagnosis of pulmonary hypoplasia. Pediatr Radiol. 2001;31:669–72.
Paek BW, Coakley FV, Lu Y, Filly RA, Lopoo JB, Qayyum A. Congenital diaphragmatic hernia: prenatal evaluation with MR lung volumetry—preliminary experience. Radiology. 2001;220:63–7.
Brewerton LJ, Chari RS, Liang Y, Bhargava R. Fetal lung-to-liver signal intensity ratio at MR imaging: development of a normal scale and possible role in predicting pulmonary hypoplasia in utero. Radiology. 2005;235:1005–10.
van der Vorst JR, van Dam RM, van Stiphout RS, van den Broek MA, Hollander IH, Kessels AG, et al. Virtual liver resection and volumetric analysis of the future liver remnant using open source image processing software. World J Surg. 2010;34:2426–33.
Ward VL, Nishino M, Hatabu H, Estroff JA, Barnewolt CE, Feldman HA, et al. Fetal lung volume measurements: determination with MR imaging—effect of various factors. Radiology. 2006;240:187–93.
Keller TM, Rake A, Michel SC, Seifert B, Wisser J, Marincek B, et al. MR assessment of fetal lung development using lung volumes and signal intensities. Eur Radiol. 2004;14:984–9.
Osada H, Kaku K, Masuda K, Iitsuka Y, Seki K, Sekiya S. Quantitative and qualitative evaluations of fetal lung with MR imaging. Radiology. 2004;231:887–92.
Mills M, Winter TC, Kennedy AM, Woodward PJ. Determination of fetal lung maturity using magnetic resonance imaging signal intensity measurements. Ultrasound Q. 2014;30:61–7.
Laudy JA, Wladimiroff JW. The fetal lung. 1: developmental aspects. Ultrasound Obstet Gynecol. 2000;16:284–90.
Dubinsky TJ, Moshiri M, Adams Waldorf K, Wilson G, Maki JH, Hippe DS. Increased fetal lung T2 signal is not due to increasing surfactant concentration: an in vitro T2 mapping analysis. Prenat Diagn. 2017;37:211–4.
Duncan KR, Gowland PA, Moore RJ, Baker PN, Johnson IR. Assessment of fetal lung growth in utero with echo-planar MR imaging. Radiology. 1999;210:197–200.
Deshmukh S, Rubesova E, Barth R. MR assessment of normal fetal lung volumes: a literature review. AJR Am J Roentgenol. 2010;194:W212–7.
Rypens F, Metens T, Rocourt N, Sonigo P, Brunelle F, Quere MP. Fetal lung volume: estimation at MR imaging-initial results. Radiology. 2001;219:236–41.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that there is no conflict of interest.
Ethical approval
The study design was approved by the appropriate ethics review boards.
About this article

Cite this article
Ogawa, R., Kido, T., Nakamura, M. et al. Magnetic resonance assessment of fetal lung maturity: comparison between signal intensity and volume measurement. Jpn J Radiol 36, 444–449 (2018). https://doi.org/10.1007/s11604-018-0745-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11604-018-0745-0