
Abstract
Purpose
Pulmonary complications are common causes of morbidity and mortality after orthotopic liver transplantation (OLT) and consist of atelectasis, pleural effusion, pulmonary oedema, adult respiratory distress syndrome (ARDS) and pneumonia. The aim of this paper is to describe the incidence of pulmonary complications after OLT during the first postoperative week and to evaluate the informative value of the chest X-ray (CXR) in clinical practice.
Materials and methods
Patients who underwent OLT at the Ancona Transplant Centre between August 2005 and August 2012 were included in this retrospective study. The CXR and, if performed, the thoracic computed tomography (TCT) scans performed during the first 7 postoperative days were reviewed, and the radiological findings for atelectasis, pleural effusion, pulmonary oedema, ARDS and pneumonia were independently assessed and quantified by two radiologists according to the Fleischner Society criteria. Cases of pneumothorax after thoracentesis were assessed. Development of pneumonia was defined as the simultaneous presence of positive CXR or TCT and positive serological or fluid samples and clinical symptoms; the prevalence of infectious agents was assessed. The radiological reports produced in the clinical setting were compared with the findings.
Results
Among 259 patients included, atelectasis was observed in 227 patients (87.6 %); pleural effusion in 250 (96.5 %); pulmonary oedema in 204 (78 %); ARDS in seven patients (2.6 %); and pneumothorax in 37 patients (14 %). Pneumonia occurred in 32 cases (12.3 %). Pulmonary oedema was underestimated in the radiological reports in 104 cases (40 %).
Conclusions
Knowledge about postoperative pulmonary complications and collaboration between the radiologist and clinician are essential for improving the management of OLT recipients.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Orthotopic liver transplantation (OLT) is a lifesaving therapy for patients with end-stage liver disease. Although advances in surgical techniques, organ preservation, immunosuppression and postoperative care have improved the survival over the last few decades, sepsis remains the leading cause of early postoperative mortality [1, 2], infections continue to be the cause of graft loss and morbidity [3]; and pneumonia is the most common postoperative infection [4] and a leading cause of morbidity and mortality [1] in OLT recipients.
Furthermore, severe, infectious or noninfectious, pulmonary complications are a major contributor to postoperative death in liver recipients more than in other solid organ transplanted patients [5], and occur in approximately 35–50 % of recipients [6]. These data highlight the importance of prevention, early diagnosis and therapy.
Commonly encountered noninfectious pulmonary complications are atelectasis, pleural effusion, pulmonary oedema, adult respiratory distress syndrome (ARDS), whereas the most common infectious pulmonary complication is pneumonia [6]. In addition, further complications can occur, such as pneumothorax after thoracentesis.
Among noninfectious pulmonary complications, pulmonary oedema is common after surgery and, in particular, after solid organ transplantation (Fig. 1). It has been demonstrated that immediate pulmonary oedema resolving within 24 h after liver transplantation had little clinical consequence, while persistent permeability-type pulmonary oedema led to a worse outcome [7]. Thus, the detection and the assessment of pulmonary oedema at radiological imaging, particularly during the early postoperative period, can be helpful for clinical management. Atelectasis is a common finding, particularly on the right pulmonary base, and is a risk factor for the development of pneumonia [8]. Pleural effusion is a common and expected consequence of OLT which contributed to parenchymal compression and atelectasis, and thus indirectly to pneumonia; furthermore, when pleural effusion is moderate/severe, it can cause respiratory impairment and requires thoracentesis. Therapeutic thoracentesis, however, can lead by itself to further complications, such as pneumothorax, haemorrhage and infections [9–11]. ARDS is due to capillary damage and loss of proteic fluid in the interstitial space and consequent diffuse alveolar damage. ARDS is often associated with sepsis from pulmonary infections, with a high mortality rate. In general, all noninfectious pulmonary abnormalities are significant risk factors for pneumonia [2, 8].

Antero–posterior supine chest X-ray (CXR) in mild (a) and severe (b) pulmonary oedema
Among early infectious complications, pneumonia is the most frequently encountered, with an incidence of 5–52 %, and a related mortality rate of 36.6–53 % [2, 6, 8, 12–18] (Figs. 2, 3). In these patients, immunosuppressive therapy is the critical risk factor for opportunistic respiratory infections (ORI). On the other hand, presentations of ORI may be atypical because of patient immunosuppression [3]; inflammatory responses are impaired by immunosuppressive therapy, with poor clinical and radiological findings.

CXR and thoracic computed tomography (TCT) in a case of early-onset pneumonia caused by Escherichia coli

CXR and TCT in a case of late-onset fatal pneumonia caused by Pseudomonas aeruginosa
The radiological diagnosis of pneumonia is defined as the simultaneous presence of a positive radiological examination (chest X-ray, CXR or thoracic computed tomography, TCT) for a new or increasing consolidation opacity (at CXR) or parenchymal consolidation (at TCT) in association with positive serological samples or fluid specimens (sputum or bronchoalveolar lavage or pleural fluid or bronchoscopy aspirates), and clinical symptoms such as fever, and dyspnoea, or desaturation if the patient is on mechanical ventilation [8, 23].
In this setting, an early diagnosis is difficult, but essential to improve patient survival [19]. Both the clinician and the radiologist, therefore, need to be familiar with the spectrum of pathogens, such as cytomegalovirus and fungi, and the presentations of the most common opportunistic respiratory infections. Furthermore, detecting and describing all noninfectious complications is helpful in the management of a critical, intensive care patient, such as the OLT recipient. In the first postoperative week, in particular, the differential diagnosis between pulmonary oedema, pneumonia and ARDS in a dyspnoic patient is very important because therapeutic management is quite different. The aim of this paper is to describe the prevalence of noninfectious and infectious pulmonary complications during the first week of follow-up of OLT.
Materials and methods
This was a retrospective study on CXR and TCT performed during the first 7 postoperative days in patients who underwent OLT at the Surgical Department and Transplant Centre of the University of Ancona between August 2005 and August 2012, selected according to the database of the Ancona Surgical Department and Transplant Centre.
We included patients who underwent OLT at the Surgical Department and Transplant Centre of the University of Ancona between August 2005 and August 2012. Exclusion criteria were patients with no postoperative CXR or TCT due to death occurring on the first postoperative day.
In all patients, CXR were performed as a supine film every day during the first 7 postoperative days, in accordance with the Centre’s protocol. The radiological examinations performed in the first 7 postoperative days (CXR and, if performed, TCT) were independently reviewed by two radiologists (PE and GA), and the presence or absence of atelectasis, pleural effusion, pulmonary oedema, ARDS and pneumonia were assessed according to Fleischner Society Glossary of Terms for Thoracic Imaging [20].
Atelectasis, pleural effusion and pulmonary oedema were quantified: atelectasis was classified as mild (involvement of less than one segment), moderate (involving one or more segments of a lobe) or severe (involving more lobes). Pleural effusion was scored as mild (loss of the sharpness of costophrenic or diaphragmatic sulci), moderate (effusion involving less than a quarter of a hemithorax) or severe (involving more than a quarter of a hemithorax). Pulmonary oedema was scored as mild (interstitial oedema) and severe (alveolar oedema).
ARDS was defined as the acute development of a diffuse patchy alveolar oedema without vascular pedicle thickening and without cardiac enlargement, with the simultaneous presence of reduced pulmonary compliance needing assisted ventilation with PaO2/FIO2 ≤200 mmHg [21]. If TCT was performed, ARDS was defined as symmetric ground-glass or airspace opacity with gravity-dependent atelectasis [22].
Then, the radiological reports produced in the clinical context were compared with the findings detected in the retrospective assessment performed by the two radiologists.
In order to identify lung infections, the medical records and the laboratory values of each patient were reviewed: to exclude simple contaminations, the onset of pneumonia was defined as the simultaneous presence of a radiological examination (CXR or TCT) positive for a new or increasing consolidation opacity (at CXR) or parenchymal consolidation (at TCT) in association with positive serological samples or fluid specimens (sputum or bronchoalveolar lavage or pleural fluid or bronchoscopy aspirates), and clinical symptoms such as fever, and dyspnoea, or desaturation if the patient was on mechanical ventilation [8, 23]. The prevalence of infectious agents in our population was also assessed.
When ARDS was associated with superimposed pneumonia, pneumonia could not be directly identified by CXR, and the diagnosis was assessed on the basis of positive biological fluids. When TCT was performed, ARDS with superimposed pneumonia could be slightly asymmetric, reflecting areas of infection, compared to the symmetric pattern of ARDS without evidence of pneumonia [22]. The diagnosis of pneumonia was in any case assessed on the basis of positive biological fluids.
Results
The results are summarised in Table 1. Among the patients who underwent OLT at the Surgical Department and Transplant Centre of the University of Ancona between August 2005 and August 2012, 10 patients were excluded because death occurred on the first postoperative day and no postoperative CXR or TCT was available. A total of 259 patients were, therefore, included in this retrospective study. The mean age of the patient population was 53.4 years (SD 8.7 years), with 54 females and 205 males. Out of 259 OLT recipients, 198 are still living (76.3 %); Among the 259 patients included, 245 received only a single graft, and 14 cases were retransplanted.
Among the 259 patients included, the CXR obtained during the first postoperative week revealed atelectasis in 227 (87.6 %); this was mild in 164 (63.3 %), moderate in 57 (22 %) and severe in 6 (2.3 %); pleural effusion was detected in 250 (96.5 %) patients and was mild in 121 (22.8 %), moderate in 91 (35.1 %) and severe in 38 (14.6 %); pulmonary oedema was observed in 163 (62 %) patients and was mild in 108 (41 %) and severe in 55 (21 %); ARDS developed in seven patients (2.6 %) and was fatal in five cases (1.8 %).
Thirty-seven patients (14 %) developed pneumothorax following thoracentesis, performed in clinically relevant pleural effusions. Review of the radiological reports revealed that mild pulmonary oedema had been underestimated in clinical practice in 59 cases (42 %) (Table 2).
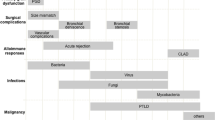
Infectious pneumonia was observed in 32 patients (12.3 %), and was fatal in five (15 % of infectious pneumonias, 1.9 % of the total population). The aetiological distribution of infectious pneumonia is shown in Fig. 4. Twelve out of 32 (37.5 %) cases of early pneumonia were due to Candida spp: 11 (34.4 %) to Candida albicans and one (3.1 %) to Candida glabrata. Five cases (15.6 %) of early pneumonia were due to Enterobacteriaceae; two (6.2 %) were due to Escherichia coli, one (3.1 %) case to extended-spectrum beta-lactamase (ESBL)-producing E. coli; two (6.2 %) were due to Enterococcus faecium and one (3.1 %) to a co-infection of E. coli and E. faecium. Two cases (6.2 %) were due to Klebsiella pneumoniae, one of which (3.1 %) to multiresistant K. pneumoniae. Two cases (6.2 %) were due to Pseudomonas aeruginosa. Two cases (6.2 %) were due to Staphylococcus aureus, one of them (3.1 %) to methycillin-resistant S. aureus, and two cases (6.2 %) were due to a co-infection of S. aureus and P. aeruginosa. Three cases (9.3 %) were due to coagulase-negative Staphylococcus; in one case (3.1 %) to multiresistant beta-haemolytic Staphylococcus and in one case (3.1 %) to S. epidermidis. One case (3.1 %) of early pneumonia was due to Streptoccocus pneumoniae.

Aetiological distribution and onset of cases of pneumonia during the first postoperative week
In addition, in the evaluation of fatal pneumonia, we considered the data from the complete follow-up of patients until the first postoperative month; during this period, pneumonia was fatal in 12 patients (4.6 % of the total population). The aetiological distribution of fatal infectious pneumonias is shown in Fig. 5. Six cases (50 % of fatal pneumonias) developed during the first postoperative week; among them, five cases (41.7 %) of fatal pneumonia were due to Candida [C. albicans in four cases (33.3 %) and C. glabrata in one case (8.3 %)]; all Candida-related fatal pneumonias had onset during the first postoperative week. One case was due to E. faecium (8.3 %). Among the remaining six cases (50 % of fatal pneumonias) with onset after the first postoperative week, three cases (25 %) were due to E. coli, one of which to extended-spectrum beta-lactamase producing E. coli); two cases (16.6 %) were due to P. aeruginosa; and one (8.3 %) case to S. epidermidis.

Aetiological distribution and onset of fatal pneumonia cases
Discussion
Pulmonary complications have great importance in the clinical management of the OLT recipient, particularly in the early management in the intensive care unit.
Among noninfectious pulmonary complications, atelectasis, particularly of the right pulmonary base, is a common finding, and can be due to postoperative diaphragmatic hypomotility, to compression from perioperative pleural effusion, to the increase of intravascular volume and retained secretions, and also to pre-existent conditions, such as right diaphragmatic hypomotility due to hepatomegalia and ascites [11, 24, 25]. Atelectasis is a risk factor for the development of pneumonia [8]; in fact, infection establishes on the parenchymal portion involved in impaired ventilation and atelectasis [26], and thus prevention consists of early extubation, mobilisation and early postoperative kinetic therapy with continuous positive airway pressure (CPAP) ventilation. Kinetic therapy, in fact, has been reported to prevent and treat respiratory complications in selected critically ill patients [5] and also noninvasive ventilation was shown to improve the outcome of these patients [27]. In our population, pneumonia developed on atelectatic parenchyma in all cases, and in some cases with permanent fibrosis.
Pleural effusion is a common and expected consequence of OLT; usually unilateral and right-sided, it derives from a direct movement of fluid from the peritoneal cavity into the pleural space through diaphragmatic defects, and is due to residual ascites but also, in some cases, to preoperative conditions such as hepatic hydrothorax [10, 11, 28]. Pleural effusion is important because it contributes to parenchymal compression and atelectasis, and thus indirectly to pneumonia; furthermore, when pleural effusion is moderate/severe, it can cause respiratory impairment and a need for thoracentesis. Therapeutic thoracentesis can, however, lead to further complications, such as pneumothorax, haemorrhage and infections [9]; moreover, in patients with hepatic hydrothorax as an underlying condition, the risk of pneumothorax arises because of the presence of fibrosis. In our cases, pneumothorax occurred in 37 patients (14 % of the total population) after thoracentesis, performed in clinically relevant pleural effusions; this finding should lead to consideration of the therapeutic rationale of thoracentesis and the appropriateness of the procedure depending on the effective amount of pleural effusion [29]; thus, it is important to quantify the amount of pleural effusion and provide an opinion on the need for a possible thoracentesis.
Pulmonary oedema (Fig. 1) is a common noninfectious complication of surgery and, in particular, of solid organ transplant. Pulmonary oedema in OLT has been demonstrated to depend mainly on a flow volume-dependent mechanism, due to overhydration from fluid infusion, blood transfusion during surgery, and to fluid retention related to preoperative renal dysfunction or to renal failure [7]. Treatment of pulmonary oedema is crucial in postoperative management, particularly in the early postoperative period [30]. The importance of maintaining fluid balance during the perioperative period of OLT has been demonstrated [31]: if the haemodynamics are stable, the appropriate negative fluid balance in the early postoperative period apparently decreases the incidence of early pulmonary complications and results in a better postoperative recovery. OLT recipients often have a pre-existent diastolic dysfunction: even a mild pulmonary oedema can result in a conspicuous diastolic deficiency and in clinically relevant symptoms. Furthermore, it has been demonstrated that immediate pulmonary oedema resolving within 24 h after liver transplantation had little clinical consequence, while persistent permeability-type pulmonary oedema led to a worse outcome [7]. Thus, the detection and the assessment of pulmonary oedema at radiological imaging, particularly in the early postoperative period, can be helpful for clinical management. In our population, the comparison between our review and the radiological reports in clinical practice revealed that early pulmonary oedema, particularly when mild, had been underestimated in 104 cases (40 % of cases), and was not mentioned in the radiological reports: this could lead to an erroneous clinical management and a worse outcome.
ARDS is due to capillary damage and loss of proteic fluid in the interstitial space and consequent diffuse alveolar damage, and is often associated with sepsis from pulmonary infections, with a high mortality rate. In our population, ARDS occurred in seven patients (2.6 %) and was fatal in five cases (1.8 %), with a mortality rate of 67 %.
The risk of infection in the organ-transplant patient is due to many factors: the invasive procedure the patient has undergone, in particular the duration of mechanical ventilation [8]; the epidemiologic exposure the patient encounters, which can vary and depends on the “microbiological ecology” of the intensive care unit [6]; and the “net state of immunosuppression”, a complex interaction of factors such as the presence of underlying diseases, postoperative metabolic factors, concurrent infection with immunomodulatory viruses, and, more importantly, the characteristics of immunosuppressive therapy required to prevent and treat graft rejection [32]. Improvements in infection rates are related to more selective immunosuppressive agents, resulting in a decreased incidence of cytomegalovirus infections and invasive candidiasis, and in a late occurrence of invasive aspergillosis [33]. Bacterial infections are less frequent, but it is important to keep in mind that antimicrobial resistance has become more common [3].
The most important principles of patient treatment are prevention, early diagnosis and specific therapy, which should be tailored on the basis of local epidemiological data [2, 34, 35].
An adequate interpretation of pulmonary imaging can have a role both in prevention and in early diagnosis; in prevention, the detection of risk factors for pneumonia, such as atelectasis, can help to prevent pulmonary infections; a radiological assessment of pulmonary oedema can lead to adequate clinical management; a proper evaluation of the amount of pleural effusion can spare patients invasive procedures such as thoracentesis, which, in turn, can expose the patient to further risks that are relevant to clinical management, such as massive pneumothorax.
As regards early diagnosis, it is necessary to have precise knowledge of the probability of the different opportunistic agents of pneumonia, which could superimpose on noninfectious pulmonary abnormalities. This knowledge also includes information about the distribution of causative pathogens and the local “microbiological ecology”, which may vary among intensive care units [2]. In addition, knowledge of the risk factors for infection is also of great assistance in the accurate interpretation of CXR and TCT in OLT recipients. Thus, a correct interpretation and communication of radiological findings in early pulmonary imaging of OLT recipients can lead to a better outcome.
Conclusions
OLT Pulmonary complications, whether infectious or not, are important causes of morbidity and mortality. The radiologist should direct particular attention to the detection and quantification of atelectasis, pleural effusion and pulmonary oedema, so as to allow a better clinical management and positively impact the outcome of these patients.
References
Bonatti H, Pruett TL, Brandacher G et al (2009) Pneumonia in solid organ recipients: spectrum of pathogens in 217 episodes. Transplant Proc 41:371–374
Weiss E, Dahmani S, Bert F et al (2010) Early-onset pneumonia after liver transplantation: microbiological findings and therapeutic consequences. Liver Transpl 16:1178–1185
Patel G, Huprikar S (2012) Infectious complications after orthotopic liver transplantation. Semin Respir Crit Care Med 33:111–124
Küpeli E, Eyüboğlu FÖ, Haberal M (2012) Pulmonary infections in transplant recipients. Curr Opin Pulm Med 18:202–212
Kleine M, Joahnning K, Kousoulas L et al (2011) Observations with impact on the indication for kinetic therapy in critically ill liver transplant patients. Ann Transplant 16:25–31
Levesque E, Hoti E, Azoulay D et al (2012) Pulmonary complications after elective liver transplantation-incidence, risk factors, and outcome. Transplantation 94:532–538
Aduen JF, Stapelfeldt WH, Johnson MM et al (2003) Clinical relevance of time of onset, duration, and type of pulmonary edema after liver transplantation. Liver Transpl 9:764–771
Golfieri R, Giampalma E, Morselli Labate AM et al (2000) Pulmonary complications of liver transplantation: radiological appearance and statistical evaluation of risk factors in 300 cases. Eur Radiol 10:1169–1183
Soubani AO, Valdivieso M (2009) Complications of thoracentesis. Intern Med J 39:628
Alonso JC (2010) Pleural effusion in liver disease. Semin Respir Crit Care Med 31:698–705
Huffmyer JL, Nemergut EC (2007) Respiratory dysfunction and pulmonary disease in cirrhosis and other hepatic disorders. Resp Care 52:1030–1036
Singh N, Gayowski T, Wagener M et al (1996) Pulmonary infections in liver transplant recipients receiving tacrolimus. Changing pattern of microbial etiologies. Transplantation 61:396–401
Aduen JF, Hellinger WC, Kramer DJ et al (2005) Spectrum of pneumonia in the current era of liver transplantation and its effect on survival. Mayo Clin Proc 80:1303–1306
Saner FH, Olde Damink SW, Pavlakovic G et al (2008) Pulmonary and blood stream infections in adult living donor and cadaveric liver transplant patients. Transplantation 85:1564–1568
Xia D, Yan LN, Xu L et al (2006) Postoperative severe pneumonia in adult liver transplant recipients. Transplant Proc 38:2974–2978
Bozbas SS, Eyuboglu FO, Ozturk Ergur F et al (2008) Pulmonary complications and mortality after liver transplant. Exp Clin Transplant 6:264–270
Colonna JO II, Winston DJ, Brill JE et al (1988) Infectious complications in liver transplantation. Arch Surg 123:360–364
Torres A, Ewig S, Insausti J et al (2000) Etiology and microbial patterns of pulmonary infiltrates in patients with orthotopic liver transplantation. Chest 117:494–502
Fishman JA (2011) Infections in immunocompromised hosts and organ transplant recipients: essentials. Liver Transpl 17(Suppl 3):S34–S37
Hansell DM, Bankier AA, MacMahon H et al (2008) Fleischner Society: glossary of terms for thoracic imaging. Radiology 246:697–722
Villar J, Pérez-Méndez L, Blanco J et al (2013) A universal definition of ARDS: the PaO(2)/FiO(2) ratio under a standard ventilatory setting-a prospective, multicenter validation study. Intensive Care Med 39:583–592
Goodman LR, Fumagalli R, Tagliabue P et al (1999) Adult respiratory distress syndrome due to pulmonary and extrapulmonary causes: CT, clinical, and functional correlations. Radiology 213:545–552
Thompson AB, Rickard KA, Shaw BW et al (1988) Pulmonary complications and disease severity in adult liver transplant recipients. Transplant Proc 20:646–649
Martel S, Carré PC (1996) Pathologies pulmonaires dans la transplantation cardiaque, hépatique et rénale chez l’adulte. Rev Mal Respir 13(Suppl 5):57–70
Ettinger NA, Trulock EP (1991) State of the art: pulmonary considerations of organ transplantation. Am Rev Respir Dis 143:1386–1405
Squadrone V, Coha M, Cerutti E et al (2005) Continuous positive airway pressure for treatment of postoperative hypoxemia. A randomized controlled trial. JAMA 293:589–595
Narita M, Tanizawa K, Chin K et al (2010) Noninvasive ventilation improves the outcome of pulmonary complications after liver resection. Intern Med 49:1501–1507
Von Bierbrauer A, Dilger M, Weissenbach P et al (2008) Hepatic hydrothorax—a rare cause of pleural effusion that is difficult to manage. Pneumologie 62:40–43
Daniels CE, Ryu JH (2011) Improving the safety of thoracentesis. Curr Opin Pulm Med 17:232–236
Snowden CP, Hughes T, Rose J et al (2000) Pulmonary edema in patients after liver transplantation. Liver Transpl 6:466–470
Jiang GQ, Peng MH, Yang DH (2008) Effect of perioperative fluid therapy on early phase prognosis after liver transplantation. Hepatobiliary Pancreat Dis Int 7:367–372
Simon DM, Levin S (2001) Infectious complications of solid organ transplantations. Infect Dis Clin North Am 15:521–549
Shi SH, Lu AW (2008) Spectrum and risk factors for invasive Candidiasis and non-Candida fungal infections after liver transplantation. Chin Med J 121:625–630
Rubin RH, Schaffner A (2001) Introduction to the Immunocompromised Host Society consensus conference on epidemiology, prevention, diagnosis, and management of infections in solid-organ transplant patients. Clin Infect Dis 33(Suppl 1):1–4
Fishman JA, Rubin RH (1998) Infection in organ-transplant recipients. N Engl J Med 338:1741–1751
Conflict of interest
Panfili E., Nicolini D., Polverini V., Agostini A., Vivarelli M., Giovagnoni A., declare that they have no conflict of interest.
Compliance with ethics guidelines
All patients gave their informed consent to the treatment of their clinical data at the admission to the University Hospital; data were treated in conformity to the Declaration of Helsinki.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Panfili, E., Nicolini, D., Polverini, V. et al. Importance of radiological detection of early pulmonary acute complications of liver transplantation: analysis of 259 cases. Radiol med 120, 413–420 (2015). https://doi.org/10.1007/s11547-014-0472-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11547-014-0472-2