
Abstract
Housing quality, which includes structural and environmental risks, has been associated with multiple physical health outcomes including injury and asthma. Cockroach and mouse infestations can be prime manifestations of diminished housing quality. While the respiratory health effects of pest infestation are well documented, little is known about the association between infestation and mental health outcomes. To address this gap in knowledge and given the potential to intervene to reduce pest infestation, we assessed the association between household pest infestation and symptoms of depression among public housing residents. We conducted a cross-sectional study in 16 Boston Housing Authority (BHA) developments from 2012 to 2014 in Boston, Massachusetts. Household units were randomly selected and one adult (n = 461) from each unit was surveyed about depressive symptoms using the Center for Epidemiologic Study-Depression (CES-D) Scale, and about pest infestation and management practices. In addition, a home inspection for pests was performed. General linear models were used to model the association between pest infestation and high depressive symptoms. After adjusting for important covariates, individuals who lived in homes with current cockroach infestation had almost three times the odds of experiencing high depressive symptoms (adjusted OR = 2.9, 95% CI 1.9–4.4) than those without infestation. Dual infestation (cockroach and mouse) was associated with over five times the odds (adjusted odds = 5.1, 95% CI 3.0–8.5) of experiencing high depressive symptoms. Using a robust measure of cockroach and mouse infestation, and a validated depression screener, we identified associations between current infestation and depressive symptoms. Although the temporal directionality of this association remains uncertain, these findings suggest that the health impact of poor housing conditions extend beyond physical health to include mental health. The study adds important information to the growing body of evidence that housing contributes to population health and improvements in population health may not be possible without addressing deficiencies in the housing infrastructure.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Multi-factorial and evolving, the complex relationship between housing and health has emerged as one that cannot be ignored as the medical and public health communities strive to improve population health. Key aspects of housing known to influence health are stability, affordability, quality, and surrounding community, with each exerting its influence in multiple ways [1, 2]. Of particular interest, especially in the subsidized sector, is housing quality. Housing quality, which includes structural and environmental risks, has been associated with multiple health outcomes including injury and asthma [1,2,3,4].
Cockroach and rodent infestations can be prime manifestations of diminished housing quality prevalent in subsidized housing and are associated with poor health outcomes [1,2,3,4]. In a 2004 survey, over half of residents in public housing and Section 8 properties reported problems with rodents in the last year [5]. Another study found that 71% of public housing residents in a single development had infestation, but only 22% reported it [6]. Several studies have identified an association between roach and rodent exposure and asthma morbidity [7,8,9,10]. While the respiratory health effects of pest infestation are well documented, much less is known about mental health effects of pest infestation or the effects of mental health conditions on pest infestation. In addition, many studies have attempted to control pest infestation in low-income housing using integrated pest management (IPM), an environmentally sensitive approach that involves a series of pest management evaluations and decisions based on a four-tiered strategy of setting thresholds, monitoring, prevention, and control [11]. However, these efforts rarely identify mental health improvements as a potential benefit of infestation reductions or measure these outcomes [10, 12,13,14]. This may be due to limited evidence regarding the presence or directionality of any potential association between pest infestation and mental health conditions.
Several housing characteristics have been associated with mental health outcomes including housing type and indoor environmental quality [15,16,17,18]. In two reviews, multi-dwelling housing type was associated with poorer psychological health as compared to living in single unit homes and housing quality was positively correlated with well-being [15, 17]. In a 2007 study, dampness and mold were associated with depression, explained in part by a lack of perceived control for residents over their home environment [18].
The relationship between pest infestation and depressive symptoms may similarly be mediated through an individual’s sense of control. The presence of pests may be perceived as an uncontrollable stressor and result in feelings of loss of control over the home environment, the domain in which many exert maximal control. Individuals who experience limited control at home or at work have an increased risk of developing depression [19,20,21]. Building-level pest management strategies that rely on centralized decision-making may diminish an individual’s sense of control, given that decisions are outside of an individual’s locus of control. Conversely, pest management practices that rely on tenant engagement and participation could lead to a greater sense of control, and action could be equated with some level of control. In addition, response and sensitivity to stressful events plays an integral role in the development of depression [22]. Alternatively, depression, through its impact on motivation and concentration, may contribute to pest infestation if depressed persons find it difficult to limit pest promoting conditions in their home and engage with pest management staff.
In addition to the psychological pathways through which pest infestation might influence and be influenced by mental health, the neurotoxicological pathway needs consideration. High levels of pesticide exposure are strongly associated with high levels of anxiety and depressive symptoms in the context of occupational use [23, 24]. Although pesticides are regulated, inappropriate use can result in exposure to high concentrations, and studies have shown off-market pesticides or off-label use in public housing developments with high rates of infestation [25].
In Boston (Massachusetts), previous studies have shown that public housing residents have a higher prevalence of symptoms of persistent sadness than their non-public housing counterparts [26]. The higher prevalence of certain chronic conditions among public housing residents has been attributed to a variety of causes including substandard housing, poverty, and isolation [27]. Given the high prevalence of both depressive symptoms and pest infestation among the public housing population, and given the potential to intervene to reduce pest infestation, there was great interest among many stakeholders, including the Boston Housing Authority (BHA) and a community-based tenant organization, regarding whether pest infestation and depressive symptoms were associated. Additionally, stakeholders were interested in whether development-level pest management activities, given their potential to influence an individual’s sense of control, would be either directly associated with depressive symptoms or could modify any potential association between pest infestation and depressive symptoms. While studies have focused on the associations between housing quality and depressive symptoms, few assess the relationships between the presence of pests, specifically cockroaches and mice, and depressive symptoms [16, 18, 28, 29]. To address this gap in our understanding of pest infestation and depressive symptoms, although not the temporal directionality of any potential association, we conducted a cross-sectional study to determine whether pest infestation was associated with symptoms of depression among adult residents in Boston public housing, and whether methods to reduce pest infestation, such as IPM, were associated with depression or modified any identified associations between pest infestation and depression.
Methods
The Integrated Pest Management Intensity Impact Study (IPMIIS) was a cross-sectional study conducted in 16 BHA developments from January 2012 to January 2014 in Boston, Massachusetts. To assess the association between pest factors and depressive symptoms, one adult from each enrolled household was surveyed, and a home inspection for evidence of pest infestation was performed. This study was reviewed and approved by the Boston Medical Center Institutional Review Board, and informed consent was obtained from all participants.
Setting and Participants
Housing units were randomly selected from eligible developments. To be included in the study, a development needed to have at least 75 units and could not be receiving HOPE VI funding, privately managed, or considered a condominium. Of the 63 developments in BHA’s portfolio, 36 were eligible.
Given differences in pest management practices across developments and to ensure developments across the spectrum of pest infestation and management strategies were included, we used pest management data to categorize developments into pest management intensity levels. While BHA development managers use IPM principles, the implementation of these practices varied with some developments employing fewer strategies than others, resulting in program heterogeneity across our study sites.
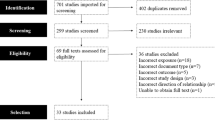
Seven criteria, aligned with IPM principles and informed by our experiences with IPM, were included in the pest management classification scheme (Fig. 1). Existing BHA data systems were the primary data sources. Based on the distribution of these criteria, we identified three intensity levels: high intensity IPM, low intensity IPM, and traditional pest management practices (Fig. 1). A development was assigned to a pest management intensity level if it met three or more criteria. Of the 36 eligible developments, 12 were classified as high IPM intensity, 12 as low IPM intensity, and 12 as traditional pest management.

This figure presents the criteria used to determine the three levels of pest management identified in this study: traditional pest management (PM), low integrated pest management (IPM), and high IPM. The six criteria were % of apartments receiving annual inspection, % of apartments with pests, % units with pests not followed up, 3-year average work order prevalence, pest contract lapse, and a combination of development participation in previous IPM pilot and presence of tenant coordinator. Of the 36 eligible developments, 12 developments were categorized into each intensity level, and from these 12, 6 were selected from each intensity level for inclusion in the study. Within each intensity level, 480 units were randomly selected. In the traditional PM, low IPM, and high IPM intensity levels, 161, 179, and 122 participants were enrolled, respectively. 1 A development with 3 or more criteria in one pest management intensity level was assigned to that level, 2 Fewer developments in the low IPM level were visited because the sample size was achieved prior to visiting 2 developments
The 36 eligible developments were assessed on two additional criteria: ease with which study staff could access the development via public transportation and whether there was ongoing major construction work. A total of 18 developments were selected with 6 in each intensity level, which included 3 developments that primarily housed elderly and disabled residents and 3 that primarily housed families. The developments were built between 1950 and 1983. Each intensity level included walk-up, town house, and high-rise building structure types. The number of units across the developments ranged from 76 to 1016. Within each intensity level, 4 eligible developments were visited initially, to accommodate the study team logistics, with additional selected developments visited only if the rate of enrollment was not adequate. Participants were enrolled from 16 of the 18 developments (Fig. 1).
Residential units were randomly selected from each development. The desired sample size was 480 units with 160 units in each intensity level. Based on previous experiences, we assumed one third of units visited by study staff would be enrolled. Therefore, we randomly selected 1440 units from a total of 4784 available units using simple random sampling without replacement from an enumerated census of units provided by BHA. Proportionate sampling was used to determine the number of units selected from each study development. Study staff visited randomly selected units and recruited one adult per unit. Staff visited 1440 units, 480 units in each pest management level. One participant was enrolled from 32.1% (n = 462) of units visited, with enrollment rates of 25.4, 37.2, and 33.5% in high IPM, low IPM, and traditional pest management levels, respectively. Overall, 30.9% of residents from units visited declined to participate (n = 445) and 37.0% (n = 533) of units visited did not respond to door knocks. Participants had to be 18 years or older, speak either English or Spanish, and able to provide informed consent. Each participant who completed the survey was given a $20 gift card.
Data Collection
Once enrolled, study teams administered surveys to participants in either Spanish or English. Data obtained from the surveys included sociodemographic characteristics, symptoms of depression, pest infestation, and pest management activities. Study teams also performed a visual inspection of each unit to assess for signs of pest infestation, promoting conditions, and management practices. Measurement of pest infestation was limited to cockroach and mouse problems only. Data were collected using Prontoforms® software on 3S iPhones®.
Measures
The primary outcome of this study was depressive symptoms. Depressive symptoms were assessed with the validated and widely used Centers for Epidemiological Study-Depression (CES-D) Scale. The CES-D is a 20-item scale with a possible range 0–60 [30]. A dichotomous variable was created to represent high depressive symptoms (HDS) based on validated cut points for CES-D score which maximizes the sensitivity and specificity for predicting major depressive disorder. For adults, the cut point is 16 [30, 31].
The main predictors of interest were the presence of cockroaches and mice in the housing unit. Participants were asked whether or not they had a current problem with cockroaches or mice. In addition, study teams were trained to identify four common signs of cockroach infestation (live roaches, dead roaches, roach skins, roach frass) and six common signs of rodent infestation (live rodents, dead rodents, rodent dropping, and evidence of gnawing, nesting, and rub marks). The identification of one or more signs of either pest was classified as having observed evidence of that pest. Given that self-reported infestation may be biased and staff ability to identify markers of infestation may be limited, a housing unit was identified as having a current cockroach or mouse infestation only if study staff identified evidence of cockroaches and/or mice during the inspection and the participant self-reported a problem with the same pest in survey responses. The decision to require both self-reported and staff observed pests may have resulted in an underestimation of pest infestation but increased the likelihood that units identified as infested had pests present in the unit.
Participant-reported frequency of cockroach and mouse sightings in the last year (never, few times a year or month, few times a week, or daily) was an additional predictor modeled separately from infestation.
Additional predictors included sociodemographic characteristics known to be associated with depression (age, sex, race/ethnicity, educational attainment, marital status, and employment status) and the following pest management characteristics: pest management intensity levels, presence of cockroach or mouse management practices identified by staff during inspection, participant-reported pest technician visit in the previous 12 months, and participant-reported pest product use by residents (e.g., fogs, traps, sprays) in the previous 12 months [31, 32].
Study teams were also trained to identify 19 common pest-promoting conditions during the inspection based on BHA management and pest contractor experience. Common pest-promoting conditions included those that allowed access to food (e.g., crumbs on surfaces, open food containers), water (e.g., dripping faucets, pet water bowls with water), and shelter (e.g., cardboard boxes, cracks, and crevices in walls). A unit was identified as having high pest-promoting conditions if staff identified more than 11 pest-promoting factors. This cut point approximated the median number of conditions among enrolled units.
Finally, three housing-related conditions associated with poor mental health in previous studies were measured: the presence of mold, residence in a high-rise building, and number of individuals in the unit [15,16,17].
Statistical Analysis
Preliminary descriptive analyses were conducted to summarize the demographic composition of study participants, unit-level pest infestation, and pest management practices, as well as the distribution of mental health outcomes. In this study, because housing developments were identified and then individual units were randomly sampled from within selected developments, there existed potential for a clustering effect where household level responses could be correlated within each housing development. To account for this, marginal regression models were fit using generalized estimating equations (GEE) with a robust empirical variance estimator to account for clustering and the lack of independence of observations at the level of housing development. General linear models were constructed and used to model the association between both pest infestation and pest management practices and high depressive symptoms.
Predictor and control variables found to be significant (p ≤ 0.05) in each individual model were included. Irrespective of p value, however, models controlled for age, race/ethnicity, and sex, as these variables are independent risk factors for depressive symptoms [32, 33]. Odds ratios are reported for the binary depression variable, representing an increased likelihood of having experienced depressive symptoms compared to the reference category of each pest and pest management predictor variable. Confidence intervals at the 95% level are also reported for all estimates. All analyses were conducted using SAS Enterprise Guide, version 7.1 (SAS Institute, 2012, Cary NC).
Results
We enrolled one adult from each of 462 housing units across 16 BHA developments. Table 1 presents the demographic characteristics of all study participants with complete exposure and outcome data (n = 435). The demographic characteristics and presence of depressive symptoms did not differ between those with complete records (n = 435) and those with missing data (n = 27) (data not shown). Of those with complete data, the majority of participants (75%) were female and 45% were between the ages of 40–64 years. The proportion of non-Latino Black (26%) and Latino (54%) study participants was similar to that of non-Latino Black (32%) and Latino (47%) residents residing in the 16 BHA study developments (BHA data not shown). Approximately 53% completed high school and 22% were employed.
Depressive symptoms were reported by 38% of participants. The prevalence of current cockroach and current mouse infestation was 15 and 14%, respectively. While prevalence of cockroach and mouse infestation was similar, the frequency of sightings differed. Among those who self-reported cockroach infestation, 25% reported sighting roaches daily or few times a week, while 15% of those who self-reported mouse infestation reported sighting mice daily or few times a week (Table 1). Additionally, among those who had current cockroach infestation, 87% reported sighting roaches daily or few times a week while 57% of those who had current mouse infestation reported sighting mice daily or a few times a week (data not shown).
Pest Infestation and Depressive Symptoms
Table 1 also presents the unadjusted odds ratios for high depressive symptoms in association with participant characteristics, housing conditions, and pest management practices. Individuals who live in homes with current roach infestation had 2.8 (95% CI 1.9–4.0) times the odds of experiencing high depressive symptoms when compared to individuals who lived in homes without roach infestation. While current mouse infestation was not associated with our outcome, dual infestation with cockroach and mouse was associated with over four times the odds (4.2, 95% CI 2.5–6.9) of experiencing high depressive symptoms. In addition, participants who reported seeing cockroaches daily or a few times a week in the last year had almost twice the odds of high depressive symptoms (1.9, 95% CI 1.4–2.6).
As expected, sex, age, and race/ethnicity were associated with depressive symptoms. Housing conditions associated with depression in previous studies including presence of mold, living in a high-rise building, and overcrowding were not associated in this study.
The adjusted associations are presented in Table 2. The association between cockroach infestation and high depressive symptoms persisted after adjusting for age, race/ethnicity, and sex (2.9, 95% CI 1.9–4.4). While there remained no association between mouse infestation and depressive symptoms in the adjusted models (1.1, 95% CI 0.7–1.8), the combination of roach and rodent infestation was associated with over five times the odds of depressive symptoms (5.1, 95% CI 3.0–8.5) when compared to those without dual infestation after adjustment.
Pest Management
While the bivariate analysis (Table 1) demonstrates a lower odds of depressive symptoms among participants living in developments with low intensity IPM (0.6, 95% CI 0.5–0.8) and traditional IPM (0.6, 95% CI 0.5–0.8) when compared to high intensity IPM, these associations were attenuated and no longer significant in the adjusted models (Table 3). Reported pest control product use by residents in the last 12 months was associated with higher odds of depressive symptoms when compared to no use of pest control products in unadjusted (1.7, 95% CI 1.2–2.3) and adjusted models (1.7, 95% CI 1.1–2.5). There was no association between evidence of pest management practices in a housing unit or reported pest technician visits and depressive symptoms.
Pest Infestation and Pest Management
To assess whether pest management practices attenuated the association between roach infestation and high depressive symptoms, we generated the odds ratios for the association between roach infestation and depressive symptoms after adjusting for the four pest management practices (Table 4). Odds ratios for roach infestation increased slightly for three of the pest management variables, and there was minor attenuation (OR from 2.9 (95% CI 1.9–4.4) to 2.8 (95% CI 1.8–4.3)) after adjusting for pest control product use by residents.
Given the relationship between pest infestation and pest management, estimates of association between pest infestation and depression were stratified by pest management variables to assess for possible effect modification. Stratified odds ratios were generated for each pest management variable. The magnitude and direction of the crude and stratified odds ratios were generally similar (data not shown). In addition, interaction terms for each pest management variable were individually included in adjusted models. None of the interaction terms were significant (data not shown).
Discussion
Our study found a strong association between depressive symptoms and pest infestation among public housing residents in Boston. Specifically, individuals who lived in housing units with cockroach infestation were 2.9 times more likely to have high depressive symptoms than those without infestation in the adjusted analysis (OR = 2.9, 95% CI 1.9–4.4). The odds of depressive symptoms increased to fivefold (OR = 5.1, 95% CI 3.0–8.5) when both cockroach and mouse infestations were present. While cockroach and mouse infestations have been associated with respiratory health outcomes such as asthma, this cross-sectional study of public housing residents is among the first to assess the association between cockroach and mouse infestations and depressive symptoms using a robust measure of active pest infestation and a validated depression screening tool.
Although the study did not identify an association between depressive symptoms and development-level pest management practices, unit-level evidence of pest management practices, or pest technician visit, it did identify a significant association between self-reported pest control product use and depressive symptoms. The directionality of the association is unclear, as there are multiple mechanisms by which individual pest control use could influence depressive symptoms (e.g., the stress related to individuals needing to take action beyond development-level pest management), or the result could be interpreted as residents who are depressed continuing to take action to control pests. The analysis did not demonstrate a significant attenuation of the association between pest infestation and depressive symptoms when adjusting for these pest management practices. Self-reported pest control product use in the home, such as fogs, sprays, and bait traps, modestly attenuated the association of roach infestation with depression, with a reduction in the odds ratio from 2.9 to 2.8. Use of pest control products may be a means through which one may exercise control over one’s home environment. Although modest in magnitude, the attenuation of the relationship between pest infestation and depression by self-reported product use qualitatively supports “loss of control” as a plausible pathway between pest infestation and depression symptoms [18].
In addition to the loss of control mechanism, previous research has identified at least two other plausible mechanisms for the association between cockroach infestation and depression identified in this study. Psychosocial stress, induced by the presence of cockroaches, can lead to depression. Research demonstrates a linear relationship between frequency and severity of stress and episodes of depression. If perceived as a stressor, cockroach infestation could contribute to depressive symptoms [22]. Additionally, cockroach infestation could lead to social isolation because individuals may be reluctant to invite others into their home or guests may be unwilling to visit. Either way, the infestation could undermine social bonds and limit social support known to protect against poor mental health [28].
Our findings are consistent with the limited literature assessing the specific association between roach and rodent infestation and depressive symptoms. A previous study examined self-reported cockroach and rodent infestation and several measures of well-being [30]. While the study identified a relationship between rat infestation and somatization, it was restricted to women of color and limited by its use of self-reported infestation measures, which could be influenced by depressive symptoms. In a 2015 case series, Reider et al. described several patients who suffered the psychiatric consequences of bed bug infestation. The case reports described a range of psychiatric conditions associated with bed bug infestation including major depressive episodes and anxiety-spectrum disorders as well as social isolation [34]. While informative, these case reports are not generalizable.
Beyond the association between pest infestation and depressive symptoms, our study reinforced the high prevalence of depressive symptoms among public housing residents. Our finding that 38% of participants reported depressive symptoms is consistent with 2015 population survey data from Boston which indicated that 20.7% (95% CI 15.8–25.6) of BHA residents reported ≥ 15 days of sadness, significantly above general population estimates [26]. The difference in magnitude may be attributed to a difference in methods. The use of a validated tool and the random selection of units reduce the likelihood of a biased estimate of depressive symptoms in our study.
This study is limited by several factors. The cross-sectional design does not allow us to specify the directionality of the relationship between infestation and depressive symptoms. However, a key finding suggests pest infestation contributes to depressive symptoms. There was no significant difference in the presence of pest-promoting conditions among those with depressive symptoms compared to those without depressive symptoms. If depression preceded pest infestation, one might expect homes of depressed participants to have a higher prevalence of conditions that promote pest infestation such as open food containers, but no such differences were observed in this study. It is likely, however, that the relationship between pest infestation and depressive symptoms is bi-directional, each exerting its influence on the other in multiple ways. Further research is needed to understand the temporal relationship between cockroach infestation and depression, and to identify potential mediating factors such as control, stress, and isolation. Finally, the study is limited by our inability to address unmeasured confounders such as stress, income, and other health conditions.
While the study focused on public housing residents, a considerable strength in understanding pest management practices and structural characteristics of buildings, this may limit its generalizability. However, the random selection procedure used to select housing units maximized the representativeness of the BHA sample, which enhances our ability to generalize to other urban public housing settings, and possibly other affordable multi-unit housing situations. In addition, the relative economic homogeneity of this population may have limited the potential influence of unmeasured economic factors such as poverty, which are known risk factors for depression, on the associations identified in this study. While the percentage of units with current cockroach and mouse infestations was similar, the lower prevalence of daily or weekly mouse sightings suggests the study may have been underpowered to identify an association between mouse infestation and depressive symptoms. Finally, methods to measure pest management practices may have been limited in their ability to adequately capture pest management activities and their potential association with depressive symptoms.
Our study has several public health implications. First, this study demonstrates that the impact of cockroach infestation extends beyond respiratory health to include emotional well-being and mental health. And while not directly demonstrated in our study, activities to prevent and reduce pest infestation may have broader health benefits than those previously identified.
This study also provides further evidence in support of the movement to screen for mental health conditions among those who report pest infestation in the health care setting. In addition to providing the necessary treatment for any conditions identified, this type of screening may provide an opportunity to help an individual advocate for his or her rights as a tenant and enlist the help of appropriate government agencies to ensure building managers are adhering to standard codes.
Finally, this study adds important information to the growing body of evidence that housing contributes to population health and improvements in population health may not be possible without addressing deficiencies in the housing infrastructure. It raises questions and exposes the need for additional research to understand whether addressing housing quality should be part of a larger, national mental health strategy.
References
Gibson M, Petticrew M, Bambra C, Sowden AJ, Wright KE, Whitehead M. Housing and health inequalities: a synthesis of systematic reviews of interventions aimed at different pathways linking housing and health. Health Place. 2011;17(1):175–84.
Thomson H, Thomas S, Sellstrom E, Petticrew M. The health impacts of housing improvement: a systematic review of intervention studies from 1887 to 2007. Am J Public Health. 2009;99(Suppl 3):S681–92.
Bashir SA. Home is where the harm is: inadequate housing as a public health crisis. Am J Public Health. 2002;92(5):733–8.
Bonnefoy X. Inadequate housing and health: an overview. Int J Environ Pollut. 2007;30(4):411–29.
Pests Persist in Federally Subsidized Housing. (2008). Integrated Pest Management Interventions for Healthier Homes Case Series. [online] Washington, DC: National Center for Healthy Homes and Environmental Protection Agency’s Office of Pesticide Programs, pp.1-2. Available at: http://nchh.org/resource-library/Case_Study_Conditions_10-14-07.pdf. Accessed 5 Feb. 2017.
Wang C, Abou El-Nour MM, Bennett GW. Survey of pest infestation, asthma, and allergy in low-income housing. J Community Health. 2008;33(1):31–9.
Sheehan WJ, Rangsithienchai PA, Wood RA, Rivard D, Chinratanapisit S, Perzanowski MS, et al. Pest and allergen exposure and abatement in inner-city asthma: a work group report of the American Academy of Allergy, Asthma & Immunology Indoor Allergy/Air Pollution Committee. J Allergy Clin Immunol. 2010;125(3):575–81.
Clougherty JE, Levy JI, Hynes HP, Spengler JD. A longitudinal analysis of the efficacy of environmental interventions on asthma-related quality of life and symptoms among children in urban public housing. J Asthma. 2006;43(5):335–43.
Gruchalla RS, Pongracic J, Plaut M, Evans R 3rd, Visness CM, Walter M, et al. Inner city asthma study: relationships among sensitivity, allergen exposure, and asthma morbidity. J Allergy Clin Immunol. 2005;115(3):478–85.
Levy JI, Brugge D, Peters JL, Clougherty JE, Saddler SS. A community-based participatory research study of multifaceted in-home environmental interventions for pediatric asthmatics in public housing. Soc Sci Med. 2006;63(8):2191–203.
United States Environmental Protection Agency Introduction to Integrated Pest Management [Internet].: United States Environmental Protection Agency; 2017 [updated January 19,2017; cited April 4, 2017]. Available from: https://www.epa.gov/managing-pests-schools/introduction-integrated-pest-management.
Kass D, McKelvey W, Carlton E, Hernandez M, Chew G, Nagle S, et al. Effectiveness of an integrated pest management intervention in controlling cockroaches, mice, and allergens in New York City public housing. Environ Health Perspect. 2009;117(8):1219–25.
Wang C, Bennett GW. Comparative study of integrated pest management and baiting for German cockroach management in public housing. J Econ Entomol. 2006;99(3):879–85.
Brenner B, Markowitz S, Rivera M, Romero H, Weeks M, Sanchez E, et al. Integrated pest management in an urban community: a successful partnership for prevention. Environ Health Perspect. 2003;111(3):1649–53.
Evans GW, Wells NM, Chan HY, Saltzman H. Housing quality and mental health. J Consult Clin Psychol. 2000;68(3):526–30.
Evans GW, Kantrowitz E, Eshelman P. Housing quality and psychological well-being among the elderly population. J Gerontol B Psychol Sci Soc Sci. 2002;57(4):P381–3.
Evans G, Wells N, Moch A. Housing and mental health: a review of the evidence and a methodological and conceptual critique. J Soc Issues. 2003;59(3):475–500.
Shenassa ED, Daskalakis C, Liebhaber A, Braubach M, Brown M. Dampness and mold in the home and depression: an examination of mold-related illness and perceived control of one's home as possible depression pathways. Am J Public Health. 2007;97(10):1893–9.
Brown GW, Moran PM. Single mothers, poverty and depression. Psychol Med. 1997;27(1):21–33.
Maier SF, Watkins LR. Stressor controllability and learned helplessness: the roles of the dorsal raphe nucleus, serotonin, and corticotropin-releasing factor. Neurosci Biobehav Rev. 2005;29(4–5):829–41.
Griffin JM, Fuhrer R, Stansfeld SA, Marmot M. The importance of low control at work and home on depression and anxiety: do these effects vary by gender and social class? Soc Sci Med. 2002;54(5):783–98.
Bogdan R, Nikolova YS, Pizzagalli DA. Neurogenetics of depression: a focus on reward processing and stress sensitivity. Neurobiol Dis. 2013;52:12–23.
Beseler CL, Stallones L. A cohort study of pesticide poisoning and depression in Colorado farm residents. Ann Epidemiol. 2008;18(10):768–74.
Malekirad AA, Faghih M, Mirabdollahi M, Kiani M, Fathi A, Abdollahi M. Neurocognitive, mental health, and glucose disorders in farmers exposed to organophosphorus pesticides. Arh Hig Rada Toksikol. 2013;64(1):1–8.
Julien R, Adamkiewicz G, Levy JI, Bennett D, Nishioka M, Spengler JD. Pesticide loadings of select organophosphate and pyrethroid pesticides in urban public housing. J Expo Sci Environ Epidemiol. 2008;18(2):167–74.
Shah S, Dooley D, et al. Health of Boston 2016–2017. Public Health Surveillance. Boston: Boston Public Health Commission; 2018.
Ruel E, Oakley D, Wilson GE, Maddox R. Is public housing the cause of poor health or a safety net for the unhealthy poor? J Urban Health. 2010;87(5):827–38.
Burdette AM, Hill TD, Hale L. Household disrepair and the mental health of low-income urban women. J Urban Health. 2011;88(1):142–53.
Zahner GE, Kasl SV, White M, Will JC. Psychological consequences of infestation of the dwelling unit. Am J Public Health. 1985;75(11):1303–7.
Radloff L. The CES-S Scale: a self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1(3):385–401.
Nguyen HT, Kitner-Triolo M, Evans MK, Zonderman AB. Factorial invariance of the CES-D in low socioeconomic status African Americans compared with a nationally representative sample. Psychiatry Res. 2004;126(2):177–87.
Riolo SA, Nguyen TA, Greden JF, King CA. Prevalence of depression by race/ethnicity: findings from the National Health and Nutrition Examination Survey III. Am J Public Health. 2005;95(6):998–1000.
Pedersen CB, Mors O, Bertelsen A, Waltoft BL, Agerbo E, McGrath JJ, et al. A comprehensive nationwide study of the incidence rate and lifetime risk for treated mental disorders. JAMA Psychiatry. 2014;71(5):573–81.
Rieder E, Hamalian G, Maloy K, Streicker E, Sjulson L, Ying P. Psychiatric consequences of actual versus feared and perceived bed bug infestations: a case series examining a current epidemic. Psychosomatics. 2012;53(1):85–91.
Acknowledgments
This article is based on work funded by United States Department of Housing and Urban Development under Award No. HUD MALHH0193-09. Its contents are solely the responsibility of the authors and do not represent the official views of the U.S. Department of Housing and Urban Development. We would like to thank all the Boston Housing Authority residents who participated in this study. In addition, we thank Peter J. Ashley, Director of the Policy and Standards Division of HUD’s Office of Lead Hazard Control and Healthy Homes, for his support of this work.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
The study was reviewed and approved by the Boston University Medical Campus Institutional Review Board. Informed consent was obtained from all participants in the original data collection stages.
Rights and permissions
About this article

Cite this article
Shah, S.N., Fossa, A., Steiner, A.S. et al. Housing Quality and Mental Health: the Association between Pest Infestation and Depressive Symptoms among Public Housing Residents. J Urban Health 95, 691–702 (2018). https://doi.org/10.1007/s11524-018-0298-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11524-018-0298-7