
Abstract
A rich tradition of research has addressed income inequality and health, but the issue has achieved a fresh currency with the reversals of economic fortunes wrought by the Great Recession. This paper analyses the degree to which changing inequality induced by the Great Recession impacted Europeans’ subjective health (self-rated health and satisfaction with health). To address this question, we analyse the multilevel European Quality of Life Survey conducted mainly in 2003, 2008, and 2012 which provides representative samples from 24 European countries at all three time points, as well as national-level data on inequality (Gini coefficient) and appropriate national-level and individual-level controls. We find that, net of GDP, inequality has no statistically significant impact before, during or after the Great Recession. Turning to determinants, our variance-components multi-level models controlling for known individual-level predictors show that inequality remains insignificant at all time points, while individual family income is strongly related to subjective health GDP per capita has little effect except indirectly through income. We also assessed impacts specifically for vulnerable, at-risk groups. Including GDP per capita, Gini coefficient, and individual level controls, our model explains about one quarter of the variance in health status (R-squared >.23). All in all, our results support a rational choice, materialist hypothesis: that absolute prosperity of the individual matters to subjective health, but income inequality does not, in Europe in this period. This supports a policy emphasis on increasing levels of pay, and on poverty relief, rather than on reducing inequality.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Apparently linked to social ills from violence to low social trust to obesity, alcoholism, decreased life expectancy and poor health outcomes, income inequality has been widely fingered as the culprit in many continuing problems in the developed world (e.g. Markus 2017; Wilkinson and Pickett, 2009, 2010). Politicians and the public have not lagged behind scholars in focusing on inequality, framing it alternately as a huge source of social woes or a galvanizing force encouraging innovation and effort. In the United States and across Europe, income inequality has become a fraught topic besieged by political and sociological disagreement. This political context makes it particularly important to seek clear empirical evidence of how much inequality actually impacts important social issues and to what extent these impacts differ across social groups.
In this contentious atmosphere, the “Great Recession” added particular urgency to the issue of income distribution (Moya and Fiske 2017), sparking widespread protests against the perceived power and abuses of the wealthiest elite -- including the now-defunct “Occupy Wall Street” movement which captured national attention in 2011 in the US. Indeed, it has been suggested that the Great Recession may have caused an “equilibrium rupture” sundering previously stable perceptions and attitudes about inequality (Esping-Andersen and Nedoluzhko 2017). Amid this renewed attention to inequality, arguments that incomes at the very top of society are bouncing back much faster than incomes in the lower quintiles abound (see Alvaredo et al. 2017), raising the issue of whether, towards the end of the Recession, the impacts of inequality might be even greater. In this context, it is key to understand the true relationship between recession, income inequality, and social outcomes.
When it comes to the impacts of inequality on health specifically, a similar lack of consensus emerges. While the determinants of population health have been strenuously debated with in the field, some influential theories centre income inequality as a key predictor of health outcomes (see Smith and Egger 1996). In the decade since Wilkinson and Pickett's (2009, 2010) influential research, there has been a vast surge of interest in the topic, with many scholars finding significant support for the link between inequality and poor objective and subjective health outcomes, while others argue that the observed relationship is a result of flawed methodology and differences in socioeconomic development (Beckfield, 2004 provides a thorough and insightful review of the early literature). One difficulty in obtaining a clear view of inequality’s impact on health is that national-level socio-economic development is a potentially important influence on health and it has a strong negative correlation with income inequality. That makes it essential to control GDP when analyzing income inequality. A critical review of the literature suggests that, using modern methodologies and accounting for the impact of GDP per capita (at parity purchasing power) on health outcomes, in general income inequality does not widely impact health outcomes (Lynch et al., 2004). Recent research is particularly inconclusive when it comes to the impact of inequality on subjective health (either self-rated health or health satisfaction), with some finding a statistically significant, although small, relationship in some European countries (Hildebrand and van Kerm, 2009), while others controlling properly for GDP find no relationship (Zagorski et al., 2014). Thus, there is substantial reason to doubt the conventional wisdom that inequality has an important negative effect on health, but the issue remains unresolved. By analogy, notice that recent research on the impact of income inequality on happiness/ subjective wellbeing/ life satisfaction found that the apparent relationship detected in earlier research was a methodological artefact: Correctly specified multilevel models using appropriate control variables find no net link between income inequality and individual subjective wellbeing in the advanced countries and a neutral to positive association in the developing countries (Esping-Andersen and Nedoluzhko 2017, Evans et al. 2017, Kelley and Evans 2017a, Kelley and Evans 2017b, Kenworthy 2017, Lin 2017; Ng and Diener 2018, Nielsen 2017, Rozer and Kraaykamp 2013).
The relationship between recession and health outcomes is equally poorly understood. It has been seen across the United States and Europe that recessions – including the Great Recession – tend to have a mixed impact on mortality rates, decreasing mortality rates in general but increasing suicides and perhaps also deaths from cardiac problems (Ruhm 2000; Stuckler et al. 2011; Stuckler et al., 2008). Yet, a trend of higher death rates in times of prosperity is also found across OECD nations (Gerdtham and Ruhm 2006). When it comes to the “Great Recession,” preliminary research suggests that, in some countries, infectious disease outbreaks rose (Karanikolos et al. 2013). This body of research, however, has two key limitations. First, many of these studies observe cross-national differences, but do not analyze contextual differences systematically in multilevel models. We remedy this gap by investigating nationally representative samples from 24 European nationsFootnote 1 descriptively and also analyzing the impact of inequality on individuals’ self-reported health, net of GDP per capita and net of individual-level characteristics. That strategy enables us to see the pure impact of the inequality context, net of the social composition of the population. Secondly, much of the prior research focused only on mortality statistics, reports of disease outbreaks and the like; by contrast, the data we analyze are rich in individual-level measures that enable us to examine differences among social groups in the impact of income inequality.
While these health statistics are certainly revealing they do not tell the whole story – it is also important to look at health through a broader lens. Did the stress of the recession decrease people’s self-rated health or satisfaction with their health? Did the Great Recession change the impact that inequality might have on subjective health? Did the changing levels of inequality or other aspects of the Great Recession have uniform impacts across individuals or were vulnerable subgroups more deeply affected (Bobak et al., 2000; Markus 2017, Rodriguez-Bailon et al. 2017; Willson and Shuey 2016)?
Hypotheses About Inequality
Rational Choice Materialism (Supported Hypothesis)
Our preferred theory – dubbed “simple materialism” – posits that inequality does not actually impact health outcomes in developed nations. Correlations between country-level characteristics – in this case inequality – and individual outcomes are particularly prone to omitted variable bias (also known as confounding variables bias), so great care must be taken to untangle the true relationships between aggregate-level and individual-level variables. Simple materialism posits that inequality is not relevant to subjective health in Europe. Applied to our particular questions of the overall impact and whether this changed during the Great Recession, the hypotheses are:
-
H1: National-level income inequality does not reduce individuals’ overall subjective health in advanced societies or in poor European societies, on average, all else equal. This holds for both (a) self-rated health and (b) health satisfaction.
-
H2: This will hold before, during, and after the Great Recession, because the rational-choice materialist model posits a null effect of inequality under all economic conditions.
Note that H1 makes a general claim that, on average, income inequality does not reduce subjective health – this holds for the pooled data or the average effect across many time points. H2 makes more specific claims, that income inequality does not reduce subjective health at specific time points (rather on average).
Rejected Alternatives: Political-Influence Model & Relative Deprivation Theory
Theories addressing the issue of the impact of inequality on subjective health need to link the macro-level contextual influence, inequality, to the individual-level outcome subjective health (van Praag 2010), a process which has been contentious and fraught with methodological and practical issues. Although no consensus has been reached, scholars have posited a number of different pathways by which income inequality might make people less healthy. One of the most compelling of these theories proposes that in unequal societies, those at the top of the income distribution also have greater access to political power, which they exert to ensure that healthcare policies are implemented in ways that benefit them more and vulnerable populations less (Schwabish et al., 2006). In this view, access to valued goods and services in a society tends to be so structured that national income inequality signals poor health care for the middle and lower classes, even net of national socioeconomic development (Wilkinson and Pickett 2009). We might call this the political-influence or policy capture model of how inequality impacts health. This theory predicts a strong cross-national result: Since economic resources always matter to the political processFootnote 2 (in this view), inequality will lead to poor health outcomes for the less fortunate across societies. Thus:
-
H-1 Alt(Political-Influence): National-level income inequality will reduce individuals’ overall subjective health across advanced societies, all else equal. This will hold both for (a) self-rated health and (b) health satisfaction.
-
H-2 Alt(Political-Influence): This net effect of inequality on subjective health will be largely the same in all three times, since it reflects relatively static distribution of political influence. This will hold both for (a) self-rated health and (b) health satisfaction.
Thus, for the pooled data, the political influence hypothesis H-1 predicts a negative effect of inequality on subjective health, in contrast to the “simple materialism” H1 which predicts that inequality have no effect on individuals’ subjective health, all else equal. For the estimates from each time-point separately, the political influence hypothesis H-2 predicts that inequality will worsen subjective health by approximately equal amounts at each of the 3 time points in the study. This is in contrast to the simple materialism hypothesis H2 that inequality will not worsen subjective health at any of the three time points. All these hypotheses apply to both self-rated health and health satisfaction.
Another alternative locates the harms of inequality within the individual psyche. The implicit reigning theory in policy circles is a variant of relative deprivation theory (Merton and Kitt 1950; Runciman, 1966) holding that the majority of the population will always feel that inequality is unjust or evil and will hence feel oppressed by it (Sen 1973; Stiglitz 2012), with these feelings reducing their quality of life in all domains (Seidl et al., 2005), presumably including subjective health. Under this model, the impact of inequality on subjective health would rise with increasing public attention to and discontent with inequality (as was seen in the wake of the Great Recession), as people became more aware of their relative position. In this view:
-
H1-Alt (Relative Deprivation): All else equal, national-level income inequality should reduce individuals’ subjective health (self rating, satisfaction with health).
-
H2-Alt (Relative Deprivation): There should be a marked increase in the damage inequality does to subjective health in the 2012 surveys in the wake of the recession.
In terms of the pooled population, H1-Alt (relative deprivation) predicts that income inequality will reduce subjective health. Thus, it leads to the same prediction as H1-Alt (political influence). Both of them contrast with H1 claiming that income inequality will NOT reduce subjective health. H2-Alt (relative deprivation) posits that the impact of inequality on subjective health will differ across the 3 time points, specifically that inequality will worsen health in all three time points, but that the effect would be greater in 2012. This contrast both with H2-Alt (political influence) which predicts a negative impact uniform in magnitude across the 3 time points and also contrasts with H2 claiming that there will be no negative impact at any of the 3 time points. All these hypotheses are expected to hold both for self-rated health and for health satisfaction.
The hypotheses are summarized in Table 1.
These do not exhaust the list of potential hypotheses, but they include those most influential to date.
Hypotheses about the Recession Context Per Se
Besides the potential effects of inequality and incomes, the recession context might harm the health of at-risk groups in other ways. In short, the impacts of recession could be strongly differentiated among social groups, even net of income (Ahs and Westerling 2006; Burgard and Kalousova 2015; McDaniel 2013; Pearlin et al., 1981). Thus, the intersection of recession and vulnerability could produce especially negative outcomes.
To explore these possibilities, we will also examine models that assess whether the effects of membership in several vulnerable groups changed over the course of the Great Recession (net of income and other influences):
Data and Methods
Data
The individual cases are from representative samples of 24 European countries which participated in the European Quality of Life Surveys with central years of 2003, 2007, and 2012 (EuroFound, 2013). These surveys are conducted by EuroFound, a tripartite European Union Agency. Only the 24 (out of 28) countries which participated in all three surveys are included in this analysis.
The EQLS conducts personal interviews with a minimum of 1000 respondents per country and aims to select representative national samples from sampling frames that include at least 95% of the citizens of each participating country (EuroFound 2013). Where such a sampling frame is not available, the EQLS generates a listing of potential cases by a random route procedure (a starting address is randomly selected, and from there, the interviewer takes alternate left- and right-hand turns at intersections, selecting every nth address). Some small and unusual populations (for example, the homeless) are likely undersampled. In all it is plausible to consider these to be reasonably representative national samples.
The quality of interviewing, data processing, and documentation is unusually high. In all, these are among the best cross-national data yet available that include not only careful and detailed measurement of actual income but also standard measures of self-rated health and of health satisfaction together with a reasonable range of individual-level control variables.
Measurement
Focal Variables
Subjective health
We measure subjective health with a two-item scale (alpha reliability = 0.85). The EQLS addressed subjective health using a health satisfaction question and a health self-report (also known as self-rated health), two items that have good face validity, predictive validity, are well known, and are highly correlated. Hence it is reasonable to treat them both as tapping the same underlying variable, subjective health.
Prior research unanimously shows that subjective health has strong predictive validity of health and mortality (e.g. Schnittker and Bacak 2014; DeSalvo et al., 2006), although there is some concern that this link varies slightly among social groups (Altman et al., 2016).
Each question was read out aloud by the interviewer and also shown to respondent on a written card. Respondents saw only the text, not the material shown in italics below. The verbatim items from the 2003 survey are:
[Question 41: Health satisfaction, wording for all three Waves with equal interval scoring ranging from 0 to 100]
Could you please tell me on a scale of 1 to 10 how satisfied you are with each of the following items, where 1 means you are very dissatisfied and 10 means you are very satisfied?
...
f. Your health _____
[scoring:
-
1
-- very dissatisfied 0
-
2
-- 11.11
-
3
-- 22.22
-
4
-- 22.22
-
5
-- 44.44
-
6
-- 55.56
-
7
-- 66.66
-
8
-- 77.78
-
9
-- 88.89
-
10
-- very satisfied 100
...
[Q43A: Health self-report, 2003 wording]
In general, would you say your health is …..
-
1
Excellent [ scored 94.0 ]
-
2
Very good [ scored 86.4 ]
-
3
Good [ scored 74.4 ]
-
4
Fair [ scored 53.1 ]
-
5
Poor [ scored 23.0 ]
[Q43B: Health self-report, 2008 and 2011-2012 wording]
In general, would you say your health is …..
-
1
Very good [ scored 90.8 ]
-
2
Good [ scored 77.6 ]
-
3
Fair [ scored 56.4 ]
-
4
Bad [ scored 28.8 ]
-
5
Very bad [ scored 12.47 ]
Technical complication: Ordinal probit scoring. There is an annoying complication. Unfortunately, the answer “Excellent” was inexplicably dropped from the “Health self-report” question (Q43 in 2003) in later years, so “Very good” becomes the top answer. Moreover, the bottom was expanded and re-worded from one category, “Poor” to two: “Bad” and “Very Bad”. Fortunately, the answers to the “Health satisfaction” question (Q41 in 2003) were maintained across all the surveys and, fortunately, the correlation of the two items remains strong in each year.
We harmonized Q43A from 2003 and Q43B from 2008 and 2011–2012 using methods of (Evans and Kelley 2004, Appendix B) with life satisfaction as the criterion. To harmonize 43a and 43b, we need to map them into a common scoring. The answer categories are ordinal, but not identical. For many purposes the conventional procedure would be to score them in equal intervals, for example 1, 2, 3, 4, and 5 (Likert scoring) or equivalently and more intuitively as points out of 100, specifically 0, 25, 50, 75, and 100. However, the equal interval assumption is problematic, at least in theory: it could be that (for example) the gap between “Very good” and “good” is larger when “excellent” is also included than when it is not.
To cater for such possibilities, we assign the intervals empirically on the basis of ordinal probit analyses (one for 2003, one for 2008 and 2011–2012 combined as they had the same answer categories). These analyses make no assumption about intervals. These posit an underlying continuous linear variable, y*, that reflects respondents’ unobserved true health self-report, plus an error term:
where the Xj are j observed structural variables described above, the bj are weights for them, individual subscripts are suppressed for simplicity, and e is a normally distributed random error term. Respondents are assumed to answer the survey question by choosing the answer category closest to their underlying position, y*:
where i subscripts the response categories labeled by their endpoints (“cutting points”). The coefficients bj and the cutting points Cuti are estimated simultaneously by maximum likelihood. We used the routines in Stata 8.
The cutting points imply a suitable scoring for the categories of the dependent variable, essentially an effect-proportional score using y* as the criterion. The gap between categories – the distance of each cutting point from the one above – is allowed to vary freely.
Any linear transformation of the scores leads to mathematically identical standardized coefficients and to metric coefficients and predicted values that differ only by a little algebra. Thus, there is no strong empirical basis for preferring one to another. For convenience, and without loss of generality, we therefore score them from a low of 0 to a high of 100. The only empirical question is then the size of the intervals between 0 and 100. These scores are shown in text boxes above.
These items are conceptually similar, are correlated at 0.76 and have similar correlations with criterion variables, both individual-level criterion variables and national characteristics (Table 2). According to the classical measurement model (Bollen 1989, Treiman 2009), these measurement properties justify combining them into a two-item scale to reduce random measurement error. Accordingly, we make them into a simple additive scale, averaging the two items. However, because the health self-report question wording for 2003 (Q43A) is not directly comparable with the wording in later years (Q43B), for greater certainty in examining the Great Recession’s effects, for the models estimated separately by year, we estimated the models with the two subjective health measures separately as well as with the combined scale.
Because of the change in answer categories of the “Health self-report” item, it is more prudent to run the analysis separately for each year, 2003, 2008, and 2011–2012.
Changes over time can be reliably ascertained only from the “Health satisfaction” item (Q41 in 2003).
Inequality: Gini
To measure inequality, we use Gini coefficients, as is conventional e.g. OECD 2006; World Bank, 2014). The versions we use were provided by EuroFound in the EQLS survey files. The Gini coefficient is a widely used measure of inequality at the country level which is very highly correlated with other measures of income inequality, for example with the share of national income going to individuals in the top 20% of households. The Gini ranges between a hypothetical low of 0 for exactly equal incomes to a hypothetical high of 1 for a solitary income recipient (and all others receiving no income). It is sometimes expressed in a 0 to 100 metric. Unfortunately, the Gini is strongly affected by cultural lifestyles such as the propensity for living alone (Firebaugh 1999), but it remains widely used as a convenient summary number. It is (by a large margin) the most widely used measure of income inequality (Gastwirth 2017).
Controlling for other changes (including earnings and GDP per capita), the Gini coefficient rises around 10% on average from our 2003 baseline to 2012, possibly reflecting the effects of the Great Recession.
Control Variables
Country Level
GDP per capita at parity purchasing power (e.g. IMF 2012) is an important control variable at the national level. GDP measures the dollar value of goods and services produced for the market (and also includes some governmental services) inside a country in a year. If investors own a factory abroad, the value of the goods the factory produces do not count in that country’s GDP. However, production inside the country for export is counted in GDP.
In the analysis, the GDP control is essential because inequality as measured by the Gini is strongly correlated with GDP (r = −.39), so omitting GDP from models of subjective health risks incorrectly attributing to Gini effects that properly belong to GDP. So an analysis of inequality’s effect on health without a GDP control could be seriously misleading, attributing to inequality the poor health outcomes actually flowing from low levels of socioeconomic development.
Individual-level controls are not of substantive interest here; rather their purpose is to avoid omitted variables bias and hence to contribute to good estimation of the effects of interest. They were chosen in light of prior research finding that they impact aspects of subjective health: Age (e.g. Franz et al. 2016), measured in single years; Gender (e.g. Reiker et al., 2010), measured with female as the reference category scored 0 and male as the deviation category scored 1; Education (e.g. Clouston et al., 2015; Ross and Mirowsky 2010), scored in single years; Marital status (e.g. Lawrence et al., 2018) scored as 2 dummy variables: (a) never married = 1 and all others =0 and (b) formerly married = 1 and all others =0, so the omitted/reference category is currently married). Attendance at worship services (e.g. Doane and Elliott 2016; Zhang 2017; Green and Elliott 2010), scored in the natural log of the number of days per year -- the natural log has been shown to be more strongly related than is the raw metric to happiness and health.
Finally, family income (e.g. Read et al., 2016), translated to a common metric (Euros) across countries by the EQLS. For clarity and easier comparability with past research, we have converted it to US dollars per year without (contrary to much recent European practice) any family size adjustment into equivalent incomes.
Descriptive Results and Changes Over Time
Across the span of the Great Recession, satisfaction with health shows little change in the samples as a whole. The average European rated their satisfaction with their health between 68 and 71 points out of 100 over this time span. (Fig. 1). There is a very slight downward bow shape – a dip of about 1 point out of 100 followed by a rise of about 2 points. (We just show health satisfaction, because of the issue with splicing the answer categories for self-rated health.) Thus, it seems that the Great Recession has caused at most a slight and temporary decrease in subjective health across Europe in the general population.

Satisfaction with health, 2003–2012
Of course, even with a confidence band as narrow as that shown in Fig. 1, there could be substantial country-to-country variation in the impact of the recession. To examine that issue, we turn now to health satisfaction and self-rated health ratings in individual countries. As described in the measurement section, the multivariate analysis will be working with a subjective-health index combining these items, but it will facilitate intuitions to explore them separately first. The average health satisfaction rating across these countries in 2003 was 69 points out of 100. Nonetheless, health satisfaction ratings varied greatly among European countries, with the least satisfiedFootnote 3 Europeans, the Latvians, rating their health satisfaction at a mere 53 points out of 100 and the most satisfied, the Irish, rating theirs an average of 80 points of 100, about 27 points higher than the Latvians in 2003 (Table 3, left panel). The standard deviation among the countries was 7.5. The gap between top and bottom remains substantial, albeit slightly reduced to around 20–23 points across the course of the Great Recession. The picture is broadly similar for self-reported health (Table 3, right panel). The means are shown for all the countries, but the change calculations are only made for the countries that conducted all 3 surveys.
There is no obvious pattern of change over time (Table 3). In the health satisfaction ratings, during the onset of the Great Recession, most changes between 2003 and 2008 were under 3 points out of 100 (less than half the standard deviation among countries in 2003). When we control for changes in individual-level demographic and SES variables, only 5 of the countries had statistically significant declines in health satisfaction: Austria, Belgium, Denmark, Italy and Turkey. These are geographically, and linguistically diverse and had diverse level of income inequality. Only 2 had statistically significant increases: France and Slovakia. These two, also, are diverse in many ways, with no obvious special similarity connecting them. The only really large change in this period was the decline in Austria, 8.9 points out of 100 after the OLS adjustment for individual-level demographic and SES changes (but it had bounced back to 2003 level by 2011–2012, so one is not inclined to make too much of it). Moreover, neither the country with the highest mean health satisfaction in 2003 (Ireland, 80) nor the country beginning the period with the lowest health satisfaction (Latvia, 53) experienced a significant change during the slide into the depths of the recession. Changes between 2008 and 2011–2012 were also highly varied. Moreover, the picture is also highly diverse over both time periods for health self-report (although the changes 2003 to 2008 changes need to be taken with a grain of salt, because of the answer category change).
Thus, the bivariate results do not support the view that the Great Recession impaired subjective health in Europe, on average. There are some small falls and some small rises in health satisfaction and in self-reported health across this period, but no strong pattern. This is preliminary evidence against the hypothesis that the Great Recession induced feelings of vulnerability and loss of control that in turn impaired subjective health in the general population. Of course, that leaves open the possibility that there were substantial gains and losses that balanced each other out. To address this possibility several of the analyses below focus specifically on at-risk subgroups.
Analytic Results on Inequality and Health
Income Inequality
Our key question for this section is to what degree societal income inequality accounts for variation in individuals’ subjective health. To find the answer, we turn to the multilevel regression analysis described in the Methods section above, with all variables standardized to a mean of 0 and standard deviation of 1 for ease of comparison of their relative importance in predicting subjective health.Footnote 4
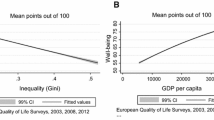
First, consider the gross effect of inequality. In a model where the Gini coefficient is the only predictor of subjective health, it has a modest negative association with subjective health rating – a statistically significant standardized effect of −0.09 for the pooled file, putting it at the bottom edge of the moderately-important range or the top edge of the weak-but-probably real - range. For the 3 years separately, the size of the effect is very close to that, but is statistically significant only in 2008 (Table 4, Panel 1; power for N = 28, s = 1, and effect size of −0.10 = .91).
Of course, that does not take into account the effects of social influences which happen to be correlated with (or potentially causes of) inequality, and hence is subject to omitted variables bias (also called confounding variables bias). Socioeconomic development, as represented by GDP, has a substantial negative association with inequality, so, to get a more nearly unique effect of income inequality, socioeconomic development should be controlled. Accordingly, Panel 2 augments the gross effect model of Panel 1 by adding GDP per capita as a contextual predictor. In Panel 2, the effect of inequality is nonsignificant for all the years combined and for each year separately and the absolute value of the coefficient estimate is substantially reduced from around .10 in Panel 1 to under .05 (Table 4, Panel 2). By contrast, the effect of per capita GDP is much larger and statistically significant. The R-squared for all three years in Panel 2 is increased by the inclusion of per capita GDP, but remains small.
The fact that the regression effect of the Gini coefficient on subjective health is not statistically significant for the pooled file supports H1 which posited that national-level income inequality does not reduce individuals’ overall subjective health in advanced societies or in poor European societies, on average, all else equal. and is contrary to H-1 Alt(Political-Influence) and H1-Alt (Relative Deprivation), both of which posited that all else equal, national-level income inequality should reduce individuals’ subjective health.
Moreover, the finding that the regression effect of the Gini coefficient is not statistically significant for any of the 3 years separately, supports H2 which posited that national-level income inequality does not reduce individuals’ overall subjective health in advanced societies or in poor European societies, on average, all else equal before, during, and after the Great Recession. This is contrary to the claim of H-2 Alt (Political Influence) that the effects would be negative and of approximately the same size in all 3 years. It is also contrary to the claim of H-2 Alt (Relative Deprivation) that not only will national-level income inequality always reduce individuals’ subjective health (self-rating, satisfaction with health), but that there will also be a marked increase in the damage inequality does to subjective health in the 2011–2012 surveys in the wake of the Great Recession.
The finding of the irrelevance of inequality to subjective health -- that inequality as measured by the Gini does not affect subjective health, net of GDP in Europe -- is robust to the inclusion of individual level controls; income and GDP do somewhat benefit health outcomes. There is an interesting switch over the course of the recession, with the importance of family income rising and GDP falling, although both are significant across the period. Future research should further explore this serendipitous finding.
Thus, income inequality does not reduce individuals’ subjective health, net of socioeconomic development in Europe in the general population before, during, or after the Great Recession of 2008. Nevertheless, the perennially pressing issue of “how the other half lives” raises the question of whether these population-wide effects mask more deleterious effects among those in the bottom half of the income distribution. What if inequality damages only the bottom half of society? Could the advantages gained by the top half be masking the disadvantages suffered by the less fortunate half? In other words, it is a question of intersectionality (interaction) – whether inequality has deleterious effects on people with lower incomes, but not on more prosperous folk. To address this question, many approaches are possible, but we have chosen the simple one of re-estimating the model from Table 4, Panel 3, separately for respondents whose family incomes were in the bottom half of their country’s income distribution and for those in the top half (Table 5).
The results show that national income inequality fails to have a statistically significant impact on subjective health, even on people in the bottom half of society’s income distribution, who presumably suffer more of the ill effects of unequal distribution of resources. Moreover, inequality’s effects, even if they were statistically significant, are in the “too weak to matter” zone (absolute value under 0.05), except the positive effect in 2013 (the sign change may simply reflect which nations were pulling out if the recession first). The other effects are broadly the same for the two groups, although the effects of GDP and income are a little stronger for people in the bottom half. Thus, we find no special relationship between inequality and poor subjective health among the bottom half of society (nor indeed among the bottom 10%, as we will see shortly). This further supports our materialist hypothesis that absolute resources matter to health, but the distribution within society does not, even during or after the Great Recession.
Vulnerable segments of society
Even after this, the possibility remains that the Great Recession per se (rather than the inequality aspect of it), had especially deleterious effects on the subjective health of people in vulnerable segments of society: The very poor whose hold on a decent life and hence on health access and activities is precarious at the best of times; young adults whose job security is likely to be less than for prime age adults and whose future outlook may be strongly shaped by present circumstances; the elderly whose subjective health tends to be in decline and who may feel especially vulnerable; and perhaps most importantly the unemployed whose prospects may be deeply darkened by recession. To examine these possibilities, we re-estimate the model from Panel 3 of Table 4, but this time including dichotomous variables representing these special groups (Table 6). This table shows the metric regression coefficients in order to clarify the magnitudes of the effects.
Net of other influences, being very poor – having a family income in the bottom 10% of the distribution – reduces subjective health by about 6 or 7 points out of 100 (Table 6, row 1). This is a statistically significant reduction. But this disadvantage did not change over the course of the recession. In good times and bad, there is a deficit of 6 or 7 points out of 100 associated with being very poor.
By contrast to poverty’s subjective health deficit, young adults enjoy especially good subjective health, a statistically significant bonus of about 12 points out of 100, all else equal. This same bonus (compared to the middle aged) holds good over the period, the Great Recession neither helping nor hurting.
Not surprisingly, seniors over age 65 have lower subjective health by 10 to 12 points than the middle aged throughout the period.
Before the recession, unemployment had no net effect on subjective health (Table 6, row 4). But the alarming economic context of the recession changed the individual-level impact of unemployment so that it had a statistically significant negative impact on subjective health in the depths of the recession, a deficit of about 2 points out of 100 for “simple” unemployment (short term and spouse not unemployed) reaching 4.6 points out of 100 for those most deeply mired in unemployment (long term unemployed with unemployed spouse). By 2011–2012, the subjective health cost of unemployment shrank but remained significantly higher than the null effect of pre-recession times, a deficit of about 1.8 points for those recently out of work stretching up to 2.7 points for the long term unemployed with an unemployed spouse.
Thus, all in all, the Great Recession did not substantially change the subjective-health vulnerability of most of these at-risk groups, except that it mildly ameliorated the subjective health deficit of seniors while generating a subjective health deficit for the unemployed which had not existed in pre-Recession times.
Discussion
Summary
Prior research revealed that income inequality did not reduce subjective health in advanced societies prior to the Great Recession (Zagorski et al., 2010). But the Great Recession’s profound economic and social dislocation led to a resurgence in inequality and many scholars have argued that it amplified the negative effects of inequality on many aspects of social life (Markus 2017, Moya and Fiske 2017). To find out, this paper has used powerful and robust multilevel (variance-components GLS) models to analyse the European Quality of Life Surveys across a time span from the prosperous days of 2003, to the depths of the Great Recession (2008), to the moderate recovery time of 2011–2012. Our aim was to discover whether the conventional wisdom that inequality harms Europeans’ quality of life, specifically their subjective health (health satisfaction and health self-report), holds true. The simple bivariate correlations of societal inequality with individuals’ subjective health are negative, albeit small. But the apparent negative effect is misleading because of the confounding effect of a key omitted variable, national socioeconomic development (GDP per capita): Unequal societies are, on average, much poorer (r = −.46) and so are disadvantaged because of that. Our variance-components multilevel models estimating the impact of Gini controlling for national per capita GDP, demonstrate that national levels of income inequality, have no statistically significant effects on subjective health in Europe in 2003 to 2011–2012: Before, during, and after the Great Recession, inequality has no impact on subjective health in Europe.
One limitation to the generalizability of these findings is that the database for the analysis does not include any countries outside Europe. This means that extremely poor countries are not included and means that we cannot safely generalize from these results to the newly developed rich nations of Asia, for example (Link 2008). In short, this is a starting point rather than a terminus: Assessment of the relationship between income inequality and subjective health in the rest of the world should be a goal for future research. Moreover, this database has only one datapoint from an economic “boom” period (2003), so another priority should be studying the potential impact of inequality on subjective health over longer periods that include both boom and bust.
In addition to our primary focus on inequality, we also examined some other income and labor-market related vulnerabilities. We found that, although inequality had no impact, all income groups suffered subjective health declines during the Great Recession. Then experiences diverged by income level. The subjective health of the prosperous sprang back by 2011–2012, in contrast to the situation for those on middling and low incomes whose subjective health remained depressed in 2011–2012. Thus, the subjective health of middle-income and poor people was less resilient than that of their more prosperous peers in this recession and the cause was something other than income or income inequality.
Note also that unemployment did not appear to impact subjective health in the pre-recession period, but significantly reduced subjective health in 2008, an effect which shrank, but remained significant into 2011–2012.
Reflection on the Literature
This paper replicates and extends recent analyses finding that societal-level income inequality does not reduce subjective health in Europe. The replication is important because Zagorski et al.'s (2014) multilevel model comes to a similar finding in a methodologically sound way, but it only includes data from a single year, 2003, so the possibility remained that their result was context-dependent on a particular time. Discovering that the same result holds for 2003–2012 and through a dramatic economic recession, allows us now to be much more confident that the prior finding that national-level income inequality does not impair subjective health is sound, replicable science which holds under a wider range of economic conditions than the earlier research was able to test.
Moreover, our results extend this prior research by expanding the array of aspects of quality of life. Thus, we have found solid support for the key hypotheses we set out to test:
-
H1: National-level income inequality does not reduce individuals’ subjective health and
-
H2: this result is robust across time and in poor (European) societies as well as rich.
Hence, the findings do not support the political-influence hypothesis (also called the policy capture hypothesis) which posits that inequality is detrimental because it allows the elite to divert public resources for their own benefit. The findings also fail to support the relative deprivation hypothesis which posits that societal inequality impairs quality of life for middle income and poor people. Thus, the working hypothesis for future research is that, when it comes to individuals’ subjective health, national income inequality is unimportant in Europe and an important question is whether this holds more widely around the world.
From the standpoint of the relative deprivation hypothesis (although not the political influence hypothesis), one might wonder if this comes about because people do not perceive income inequality correctly. For the political influence hypothesis, people’s perceptions are not necessarily relevant (Schwabish et al., 2006; Wilkinson and Pickett 2009), because the process or resource diversion would probably be most effective and sustainable if it were not perceived. However, perceptions are key to the relative deprivation hypothesis: If people do not perceive others as above them in the hierarchy, they will not be offended and hurt by the others’ success (e.g. (Merton and Kitt 1950; Runciman, 1966; Seidl et al., 2005) People may underestimate the magnitude of inequality, but they perceive the shape of the income distribution veridically: Indeed perceptions correlate with the Gini at around 0.8 (Evans and Kelley 2017, 2018). This makes it seem unlikely that inequality does not matter because people are unaware of it.
Our findings support the materialist claim that what matters is not inequality but prosperity: The observed relationship many scholars have found between inequality and health seems likely to be a manifestation of the fact that the richer nations of Europe are also generally more equal. Across time periods, the results show a small-to-moderately-important positive link between GDP per capita and health satisfaction, net of inequality (Gini). It is possible that this largely reflects the legal, political, and social enhancements that modernization brings (rather than the economic ones). Another aspect of prosperity also matters and, indeed, it may account for the apparent GDP effect: Net of GDP, family income has a substantial impact on individuals’ subjective health, which rules out a post-materialist interpretation. Indeed, the family income effects are in the “strong” range (standardized effects in the 0.2–0.3 range), and appear largely to account for the GDP effect. This result emphasizes the great importance of having both income and subjective health measured as precisely as possible in the same survey in order to obtain a good estimate of their connection. Although family income is only a control variable in our analysis, these substantial effects illustrate the continued relationship between income and subjective health outcomes, even in advanced societies. The poor have lower subjective health than their more prosperous peers at all 3 time points, net of national-level inequality and affluence and net of socio-demographic characteristics.
In short, it is poverty, not inequality, that is unhealthy. This evidence suggests that goals of supporting and enhancing population wellbeing are best served by social and economic policy emphases on enhancing prosperity and alleviating poverty, rather than on suppressing income inequality.
Notes
28 European countries took part in the study in at least one time point. For the analysis comparing the time points we restrict the sample to the 24 countries that participated in all 3 waves. This keeps the samples for the different time points comparable. Data collection was centered on the years we indicate, but in some instances stretched into adjacent years.
At least in the kinds of political structures found in the European countries analyzed.
Based on health satisfaction in 2003.
The data are z-scored using the sample mean and standard deviation for all the countries pooled for all three years combined.
References
Ahs, A., & Westerling, R. (2006). Self-rated health in relation to employment status during periods of high and of low levels of unemployment. European Journal of Public Health, 16(3), 294–304.
Altman, C. E., Van Hook, J., & Hillemeier, M. (2016). What Does Self-Rated Health Mean? Changes and Variations in the Association of Obesity with Objective and Subjective Components of Self-rated Health. Journal of Health and Social Behavior, 57(1), 39–58.
Alvaredo, F., Chancel, L., Piketty, T., Saez, E., Zucman, G., (2017). Global Inequality Dynamics: New Findings from WID.world. NBER Working Paper No. 23119.
Beckfield, J. (2004). Does Income Inequality Harm Health? New Cross-National Evidence. Journal of Health and Social Behavior, 45(3), 231–248.
Bollen, K. A. (1989). Structural Equations with Latent Variables. New York: Wiley.
Bobak, M., Pikhart, H., Rose, R., Hertzman, C., & Marmot, M. (2000). Socioeconomic factors, material inequalities, and perceived control in self-rated health: cross-sectional data from seven post-Communist countries. Social Science & Medicine, 51(9), 1343–1350. https://doi.org/10.1016/S0277-9536(00)00096-4.
Burgard, S. A., & Kalousova, L. (2015). Effects of the Great Recession: Health and Well-Being. Annual Review of Sociology, 41, 181–201. https://doi.org/10.1146/annurev-soc-073014-112204.
Clouston, S. A. P., Richards, M., Cadar, D., & Hofer, S. M. (2015). Educational Inequalities in Health Behaviors at Midlife. Journal of Health and Social Behavior, 56(3), 323–340.
Coleman, J. S. (1990). Foundations of Social Theory. New York: Belknap Press.
Crimmins, E. M. (2004). Trends in the health of the elderly. Annual Review of Public Health, 25, 79–98.
DeSalvo, K., Bloser, N., Reynolds, K., He, J., & Muntner, P. (2006). Mortality prediction with a single general self-rated health question. Journal of General Internal Medicine, 21, 267–275.
Doane, M. J., & Elliott, M. (2016). Religiosity and Self-Rated Health. Journal of Religion and Health, 55(3), 844–855.
Esping-Andersen, G., & Nedoluzhko, L. (2017). Inequality Equilibria and Individual Well-Being. Social Science Research, 62(February), 24–28.
Evans, M. D. R., & Kelley, J. (2004). Effect of Family Structure on Life Satisfaction: Australian Evidence. Social Indicators Research, 69(3), 303–353.
Evans, M. D. R., & Kelley, J. (2017). Communism, Capitalism, and Images of Class: Effects of Reference Groups, Reality, and Regime in 43 Nations and 110,000 Individuals, 1987-2009. Cross-Cultural Research, 51(4), 315–359. https://doi.org/10.1177/1069397116677963.
Evans, M. D. R., & Kelley, J. (2018). Strong welfare states do not intensify public support for income redistribution, but even reduce it among the prosperous: A multilevel analysis of public opinion in 30 countries. Societies, 8(4.105), 1–53. https://doi.org/10.3390/soc8040105 Url: https://www.mdpi.com/2075-4698/8/4/105/htm. Access: June 15, 2019
Evans, M. D. R., Kelley, J., Kelley, S. M. C., Kelley, C. G. E., (2019) Rising Income Inequality During the Great Recession Had No Impact on Subjective Wellbeing in Europe, 2003-2012. Journal of Happiness Studies, 20(1), 203-228. EuroFound 2012. European Quality of Life Surveys (EQLS): First EQLS in 2003. Brussels: http://www.eurofound.europa.eu/surveys/eqls/index.htm. Access: June 15, 2019
EuroFound. (2013). EuroFound survey methodology. Brussels http://www.eurofound.europa.eu/surveys/methodology/index.htm Access: June 15, 2019
Firebaugh, G. (1999). Empirics of World Income Inequality. American Journal of Sociology, 104(6), 1597–1630.
Franz, C. E., Finkel, D., Panizzon, M. S., Spoon, K., Christensen, K., Gatz, M., Kremen, W. S., Krueger, R., Neiderhiser, J., Reynolds, C., Pedersen, N. L., & IGEMS consortium. (2016). Facets of Subjective Health from Early Adulthood to Old Age. Journal of Aging and Health, 29(1), 149–171.
Gastwirth, J. L. (2017). Is the Gini Index of Inequality Overly Sensitive to Changes in the Middle of the Income Distribution? Statistics and Public Policy, 4(1), 1–11. https://doi.org/10.1080/2330443X.2017.1360813.
Gerdtham, U. G., & Ruhm, C. J. (2006). Deaths rise in good economic times: evidence from the OECD. Economics and Human Biology, 4(3), 298–316. https://doi.org/10.1016/j.ehb.2006.04.001.
Green, M., & Elliott, M. (2010). Religion, Health, and Psychological Well-Being. Journal of Religion and Health, 49(2), 149–163.
Hildebrand, V., & van Kerm, P. (2009). Income Inequality and Self-Rated Health Status: Evidence from the European Community Household Panel. Demography, 46(4), 805–825. https://doi.org/10.1353/dem.0.0071.
IMF (International Monetary Fund). (2012). "Gross Domestic Product." Finance & Development. http://www.imf.org/external/pubs/ft/fandd/basics/gdp.htm. Accessed January 5, 2014.
Kelley, J. and Evans, M. D. R., (2017a). Societal Income Inequality and Individual Subjective Well-Being: Results from 68 Societies and over 200,000 Individuals, 1981–2008. Social Science Research 62(February):1–23. https://doi.org/10.1016/j.ssresearch.2016.04.020.
Kelley, J., & Evans, M. D. R. (2017b). The New Income Inequality and Well-Being Paradigm. Social Science Research, 62(February), 39–74.
Kenworthy, L. (2017). Income Inequality Probably Has Had Little or No Effect on Subjective Well-Being. Social Science Research, 62(February), 36–38.
Karanikolos, Marina, Philipa Mladovsky, Jonathan Cylus, Sarah Thomson, Sanjay Basu, David Stuckler, Johan Makenbach, and Martin McKee. (2013). Financial Crisis, Austerity and Health in Europe. The Lancet 381(April 13/ 9874): 1323–1331. doi: https://doi.org/10.1016/S0140-6736(13)60102-6.
Lawrence, E. M., Rogers, R. G., Zajacova, A., Wadsworth, T., (2018). Marital Happiness, Marital Status, Health, and Longevity. J Happiness Stud online before print: Doi:https://doi.org/10.1007/s10902-018-0009-9.
Lin, E,. (2017). Does income inequality reduce the quality of life in the post-Great-Recession era? A multi-level analysis of 87 countries with over 150,000 individuals. Pacific Association for Public Opinion Research, Annual Conference. Friday, December 15, 2017, Panel 3. San Francisco.
Link, B. G. (2008). Epidemiological Sociology and the Social Shaping of Population Health. Journal of Health and Social Behavior, 49(4), 367–384.
Lynch, J., Smith, G., Harper, S., Hillemeier, M., Ross, N., Kaplan, G., & Wolfson, M. (2004). Is Income Inequality a Determinant of Population Health? Part 1. A Systematic Review. The Milbank Quarterly, 82(1), 5–99.
Markus, H. R. (2017). In This Together: Doing and Undoing Inequality and Social Class Divides. Journal of Social Issues, 73(1), 211–221. https://doi.org/10.1111/josi.12212.
McDaniel, S. A. (2013). Understanding health sociologically. Current Sociology, 61(5–6), 826–841.
Moya, M., & Fiske, S. T. (2017). The Social Psychology of the Great Recession and Social Class Divides. Journal of Social Issues, 73(1), 8–22. https://doi.org/10.1111/josi.12201.
Ng, Weiting and Ed Diener. 2018. "Affluence and Subjective Well-Being: Does Income Inequality Moderate Their Associations?. Applied Research in Quality of Life Online before print(3 January 2018):1–26. doi: https://doi.org/10.1007/s11482-017-9585-9.
Nielsen, F., (2017). Inequality and Inequity. Social Science Research 62(February):29–35.
Merton, R. K. and Kitt, A. S. (1950). Contributions to the Theory of Reference Group Behavior. Pp 40–105 in Continuities in Social Research, edited by Robert K. Merton and Paul F. Lazarsfeld. Glencoe, IL: Free Press.
OECD. (2006). "Gini Index" in Glossary of Statistical Terms. http://stats.oecd.org/glossary/detail.asp?ID=4842. Accessed January 2, 2014.
Pearlin, L. I., Menaghan, E. G., Lieberman, M. A., & Mullan, J. T. (1981). The Stress Process. Journal of Health and Social Behavior, 22, 337–335.
Phelan, J. C., Link, B. G., & Tehranifar, P. (2010). Social Conditions as Fundamental Causes of Health Inequalities. Journal of Health and Social Behavior, 51(1_suppl., S28–S40.
Read, S., Grundy, E., & Foverskov, E. (2016). Socio-economic position and subjective health and well-being among older people in Europe. Aging & Mental Health, 20(5), 529–542.
Reiker, P. P., Bird, C. E., Lang, M., (2010). Understanding Gender and Health. Pp. 52–74 in Handbook of Medical Sociology, Sixth Edition. Cloe E. Bird and Peter Conrad (eds.) Nashville, TN: Vanderbilt University Press.
Rodriguez-Bailon, R., Bratanova, B., Willis, G. B., Lopez-Rodriguez, L., Sturrock, A., & Loughnan, S. (2017). Social Class and Ideologies of Inequality: How They Uphold Unequal Societies. Journal of Social Issues, 73(1), 99–116. https://doi.org/10.1111/josi.12206.
Ross, C. E. and Mirowsky, J., (2010). Why Education is the Key to Socioeconomic Differentials in Health. Pp. 33–51.n Handbook of Medical Sociology, Sixth Edition. Cloe E. Bird and Peter Conrad (eds.) Nashville, TN: Vanderbilt University Press.
Rozer, J., & Kraaykamp, G. (2013). Income Inequality and Subjective Well-Being: A Cross-National Study on the Conditional Effects of Individual and National Characteristics. Social Indicators Research, 113(3), 1009–1023.
Ruhm, C. J. (2000). Are Recessions Good for Your Health? The Quarterly Journal of Economics, 115(2), 617–650.
Runciman, W. G. (1966). Relative Deprivation and Social Justice. Harmondsworth, England: Penguin.
Seidl, C., Traub, S., Morone, A., (2005). Relative Deprivation, Personal Income Satisfaction and Average Well-being under Different Income Distributions. Research Paper No. 2005/04, UN University and World Institute for Development Economics Research.
Sen, A. (1973). On Economic Inequality. Oxford: Clarendon.
Schnittker, J. and Bacak, V., (2014). The Increasing Predictive Validity of Self-Rated Health. PLoS One 9(1): e84933 (online only, no page numbers): https://doi.org/10.1371/journal.pone.0084933.
Schwabish, J., Smeeding, T., Osberg, L., (2006). Income Distribution and Social Expenditures: A Cross-National Perspective. Pp. 247–88 in The Distributional Effects of Government Spending and Taxation, edited by D.B. Papadimitriou. Northampton, MA: Edward Elgar Publishing.
Smith, G. D., & Egger, M. (1996). Commentary: Understanding It All-Health, Meta-Theories, and Mortality Trends. British Medical Journal, 313(Dec. 21), 1584–1585.
Stiglitz, J. E. (2012). The Price of Inequality: How Today's Divided Society Endangers our Future. New York: W.W. Norton and Company.
Strandh, M., Winefield, A., Nilsson, K., & Hammarström, A. (2014). Unemployment and mental health scarring during the life course. European Journal of Public Health, 24(3), 440–445.
Stuckler, D., Basu, S., Suhrcke, M., Coutts, A., & McKee, M. (2011). Effects of the 2008 recession on health: a first look at European data. The Lancet, 378(July 9/9786), 124–125. https://doi.org/10.1016/S0140-6736(11)61079-9.
Stuckler, D., Meissner, C., King, L., (2008). Can a Bank Crisis Break Your Heart? Globalization and Health 4(1): online only, no page numbers; doi: https://doi.org/10.1186/1744-8603-4-1.
Treiman, D. J., (2009). Scale Construction. Pp. 241–62 in Quantitative Data Analysis. San Francisco: Jossey-Bass.
Turner, J. B. (1995). Economic Context and the Health Effects of Unemployment. Journal of Health and Social Behavior, 36(3), 213–229.
van Praag, B. M. S. (2010). Well-being inequality and reference groups. Journal of Economic Inequality, 9, 111–127.
Wilkinson, R. G., & Pickett, K. E. (2009). Income Inequality and Social Dysfunction. Annual Review of Sociology, 35, 493–511.
Wilkinson, R. G., & Pickett, K. E. (2010). The Spirit Level: Why Equality is Better for Everyone. London: Penguin Books.
Willson, A. E., & Shuey, K. M. (2016). Life Course Pathways of Economic Hardship and Mobility and Midlife Trajectories of Health. Journal of Health and Social Behavior, 57(3), 407–422.
World Bank. (2014). Gini Index" in Data . http://data.worldbank.org/indicator/SI.POV.GINI. Accessed January 5, 2014.
Zagorski, K. (2011). Income and Happiness in Time of Post-Communist Modernization. Social Indicators Research, 104, 331–349.
Zagorski, K., Kelley, J., & Evans, M. D. R. (2010). Economic Development and Happiness: Evidence from 32 Nations. Pol Sociol Rev, 2010(1), 3–20.
Zagorski, K., Evans, M. D. R., Kelley, J., & Piotrowska, K. (2014). Does National Income Inequality Affect Individuals' Quality of Life in Europe? Inequality, Happiness, Finances, and Health. Social Indicators Research, 117(3), 1089–1110.
Zhang, L. (2017). An Age–Period–Cohort Analysis of Religious Involvement and Adult Self-Rated Health. Journal of Religion and Health, 56(3), 916–945.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Evans, M.D.R., Kelley, J., Kelley, C.G.E. et al. Income Inequality in the Great Recession did not Harm Subjective Health in Europe, 2003–2012. Applied Research Quality Life 15, 1451–1473 (2020). https://doi.org/10.1007/s11482-019-09741-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11482-019-09741-0