
Abstract
We analyze the impact of networks and stress on the general and mental health of men and women aged 25 to 59 using data from the Canadian 2008 General Social Survey on Social Networks. Controlling for demographic and other variables, we examine the effects on health of social network types (family vs. friends), size, strength (frequency of contact) and diversity, and the interaction of these network variables with stress. We largely find the expected health benefits of network size, strength and diversity. Nonetheless, we also find diminishing health returns at higher levels of the network measures. The general health of men and women, for example, benefits from increasing size of family network, but such benefit decreases after a certain size. Likewise, increases in friend and family network sizes have positive but diminishing returns on men’s mental health. As expected, stress negatively impacts the general and mental health of men and women but social networks can buffer some of the negative effects. The negative effect of stress on men’s mental health is lessened with a more diverse network. Similarly, the negative effect of stress on women’s mental health decreases with larger network of friends. However, in the case of general health, men with higher stress have worsening health if they are in more diverse networks.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Stress is a common feature of life. Research in health, sociology, and psychology has shown that individuals living in a stressful situation are more likely to develop behavioral and psychological problems (Garmezy and Rutter 1983; Lincoln et al. 2005). However, not all individuals experiencing stressful events have health issues. According to Antonovsky (1979, 1987), whether a stressed individual will have health problems depends on resources available to them, including financial resources and social support. As predicted by the stress process model, the buffering effect of social network on health has been widely documented in different societies (Barger 2013; Berkman and Glass 2000; Cohen 2004; Holt-Lunstad et al. 2010).
Social networks are at the core of social structure, linking individuals to society through connections among relatives, friends, neighbours, colleagues, and others (Murata 2010; Zhang 2010). Social network is one of the key elements in both Social-Resource Theory and Social-Capital Theory (Zhang 2010). Understanding how the structural properties of social networks facilitate or inhibit the provision of social support is critical to understanding the social context of health and well-being and has been the subject of substantial social science research over the past four decades (Berkman et al. 2000). Social networks have been found to be important to social well-being (Ryan et al. 2009; Dubow and Tisak 1989), participation in social or political movements (Ikeda and Richey 2005; Shemtov 2003; Passy and Giugni 2001; La Due Lake and Huckfeldt 1998), industrial and academic development (Kim and Rhee 2010; Walker et al. 1997), health care utilization (St. Clair et al. 1989), international relations (Hafner-Burton et al. 2009), and even animal behavior and organization (Krause et al. 2007; Sih et al. 2009). In general, it is widely accepted that social networks transmit resources among connected individuals and determine how each individual integrates to the society.
However, because of the complexity of the concept of social network and the various measurements and methods, there are remaining questions to address. In particular, little research has sought to compare the impact of social network on different measures of health status. Moreover, it is rare in previous research to use multiple indicators to include the various dimensions of the social network. Furthermore, most social network researchers have tended to focus on the positive side of social networks to health, and there is less attention to the mechanisms through which social networks may have negative impacts on health (Pescosolido and Levy 2002).
This study deals with part of the issues mentioned above by examining, firstly, the impact of the social network on self-reported general and mental health status. Secondly, this study uses diverse measures to quantify both family and friend social networks, including network size, strength, and diversity. Thirdly, by introducing a squared term, we examine the possible diminishing effects of social networks on health status. We also include an interaction term with level of stress in order to investigate possible buffering effects, and we investigate gender differences in the various relationships.
The Association between Social Networks and Health Status
Human beings need resources to survive which can be roughly classified into personal resources and environmental resources (Ehrhardt et al. 2007; Wayman 2002). Personal factors are internal attributes that can buffer the harmful effects of an adverse situation. Environmental resources are external elements that provide support and protect against negative factors threatening the person’s survival (Wang et al. 1997). Social networks are a crucial part of environmental resources and they provide access to other resources, such as instrumental, material, expressive and social support (Cohen and Syme 1985; House et al. 1988).
Social networks can buffer the negative effects of adverse social events and provide more opportunities for positive experience (Berkman and Glass 2000; Dubow and Tisak 1989; Gage 2013). For instance, expressive support can make an individual feel that he/she is valued by others, which leads to enhanced self-esteem and feelings of mastery over stressors. Informational support may help the individual to understand and cope more effectively with stressors (Dubow and Tisak 1989). The perceived availability of social support, especially emotional support, has direct effects on health and buffers the negative effects of stress (Cohen 2004; Holt-Lunstad et al. 2010). Patients can use social network to access health information or find a regular family doctor (Griffiths et al. 2012; Devlin and Rudolph-Zbarsky 2014). Moreover, studies show that support of immediate and extended family, and of friends, along with open communication amongst family members, are factors promoting resilience (Greeff and Van Der Merwe 2004). Conversely, socially isolated individuals are less able than others to buffer the impact of health stressors and consequently are at greater risk for negative health outcomes (Smith and Christakis 2008).
However, previous research has tended to emphasize the salubrious potential of social networks and ignore the possible negative effect of social networks on health. For instance, network interactions could be based on relations of power and conflict, leading to negative outcomes (House et al. 1988; Crimmins et al. 2011). Social networks can also constrain healthy behavior or encourage unhealthy behavior (Smith and Christakis 2008; Holt-Lunstad et al. 2010). While the support among network members is mostly based on interdependence, long-term asymmetric relations could also create dependency and undermine health (Antonucci and Jackson 1990; Howard 2006; van Dijk 1998; Kiecolt-Glaser et al. 1991; Schulz and Beach 1999). Therefore, a full understanding of the relationship between social network and health can only be reached when both positive and negative dimensions are examined (Sneed and Cohen 2014; Pescosolido and Levy 2002; Martire and Franks 2014).
Besides paying attention to both positive and negative relationships, we also check for both linear and curvilinear relationships. While larger social networks can offer stronger support, having too many ties may have negative consequences because of the higher demands of a larger network (Pescosolido and Levy 2002).
Since earlier analyses indicate that networks may operate differently for men and women, and there can be different dynamics in men and women’s health, all analyses were done separately by gender (Marquez et al. 2014; Sneed and Cohen 2014). Various research finds that women are more likely to provide support to both women and men. Umberson et al. (2014) propose that men and women enact gender in their daily lives in such a way that stress may strengthen women’s social ties but undermine men’s ties. Men and women have also been found to manage their social networks in substantially different ways, resulting in different network components affecting on their health (Szell and Thurner 2013). Crimmins et al. (2011) find social participation is a key factor in men’s health, while social network scores play a larger role for women. In a study of hypertension among older people, a larger network was associated with a lower risk for men, while network density increased women’s hypertension awareness (Baek et al. 2016).
In sum, it is important to examine the impact of the social network on alternate measures of health status for men and women, to pay attention to both positive and negative impact of social network measures on health, and to consider possible curvilinear relationships between social network measures and health status.
Dimensions or Characteristics of Social Networks
We adapt the conceptual model proposed by Berkman et al. (2000: 847) by seeking to measure the following characteristics of egocentric social networks: size, density, homogeneity and type.
Network size is the number of people involved in the given network. It is generally assumed that the network size determines access to resources and that larger networks offer more emotional and instrumental support (Falci and McNeely 2009). While a larger network may include more support donors, the duties and obligations associated with the network may increase with the expansion of the network size. The difficulty of maintaining large networks can become a source of stress or tension. For instance, Falci and McNeely (2009) find that both a too large and a too small network results in high levels of depressive symptoms among adolescents.
Network density measures the interconnectedness of a network, which is best determined by the extent to which network members are connected to each other (Berkman et al. 2000). Since we do not have a measure of density, we use the frequency of contact as a measure of the strength of the network. This frequency of contact may determine the probability of lending support, and the quantity, quality, and types of support (Murata 2010; García et al. 2005; van Dijk 1998). At the same time, a strong network could be a burden to both the support donors and recipients because of expected responsibilities, duties and obligations (Fingerman et al. 2004). In this study, we include the squared items of network size and strength to capture the possible curvilinear relationship with health status.
In the conceptual model proposed by Berkman et al. (2000: 847), social network homogeneity refers to the similarity among members in a network. However, in most social network research, it is measured by its converse, the network diversity. While it may be easier to establish a network among individuals who have similar social, economic, and cultural backgrounds (Ehrhardt et al. 2007; Li and Zhang 2015), more diverse networks may have access to more resources. In this study, network diversity refers to the respondent knowing people from a variety of occupations. We hypothesize that people who know others from more varied occupations will have access to more support.
We use the concept of network type to include the aspects of group structure based on kin, work, or neighborhood (Berkman et al., 2000: 847). In particular, we include networks based on family and those based on friendship. Social relationships among family members may be more durable over time, and be able to accommodate for lack of mutuality at a given point in time (van Dijk 1998). On the other hand, friends are based on individual choices, providing a different type of network (Ehrhardt et al. 2007; Dubow and Tisak 1989). Thus the size and strength of networks based on families and relatives is considered separately from networks based on friendship.
In sum, this study uses five indicators to measure the characteristics of social networks: the size of the family network, the size of the friend network, the strength of the family network, the strength of the friend network, and the diversity of people’s network. We propose that the role of social networks in health depends on the nature of the relationship (family or friends), the network’s size and strength (frequency of contact), and diversity.
Data, Measures and Methods
This study is based on data from the 2008 Canadian General Social Survey (GSS)Footnote 1 which focused on social networks. The GSS is based on randomly chosen individuals, and thus the measures refer to egocentric social networks rather than measures taken from each member of the network. The target population of the 2008 GSS included persons 15 years and over living in private households in Canada, excluding residents of the Yukon, Northwest Territories and Nunavut; and full-time residents of institutions (Statistics Canada 2009). The total sample size of the survey is 20,401.
The present study focuses on respondents aged between 25 and 59 who numbered 12,257. Respondents aged 25–59 are selected in order to exclude younger and older persons who would have different dynamics with regard to health status and social networks. The sample size is further reduced to 11,539 due to non-response on given measures.Footnote 2
Dependent Variables
The outcome variables are general health status and mental health status which are commonly used in previous research:
-
1.
The general health status is based on question, “In general, would you say your health is: 1 = poor? 2 = fair? 3 = good? 4 = very good? 5 = excellent?”
-
2.
The mental health status is based on question, “In general, would you say your mental health is: 1 = poor? 2 = fair? 3 = good? 4 = very good? 5 = excellent?”
The mental health is controlled in the analysis of the general health and the general health is controlled in the analysis of the mental health. Moreover, to simplify the analysis, the outcome variables are treated as interval-ratio measures.Footnote 3
Independent Variables
The stress level of a respondent is measured by the survey question, “Thinking of the amount of stress in your life, would you say that most days are: 1 = not at all stressful? 2 = not very stressful? 3 = a bit stressful? 4 = quite a bit stressful? 5 = extremely stressful?”
The structure of social network is measured by five components covering the type, size, strength and diversity. The size of the family network is measured by “number of relatives you feel close to”. The size of the friend network is measured by “How many close friends do you have?” where “close” friend is defined as “people who are not your relatives, but who you feel at ease with, can talk to about what is on your mind, or call on for help.” Since the questions refer to people who are “close” to the respondent, it should be noted that weak ties are not included in the size of these ego networks. Given that the measures of network size are highly skewed, the measures are capped at values that are some three standard deviations above the mean.Footnote 4
The strength of networks is measured through frequency of contact. This is obtained by a summation of answers to two questions, “In the past month, how often did you see any of your relatives/friends?” and “In the past month, how often did you communicate with any of your relatives/friends by telephone (outside of people you live with)?” There are six possible answers for each question (5 = Everyday, 4 = A few times a week, 3 = Once a week, 2 = 2 or 3 times a month, 1 = Once a month, 0 = Not in the past month) which result a range of 0 to 10 as values for each of family and friend network strength.
The network diversity is measured by the extent to which the respondent knows people from a variety of occupations. In the 2008 GSS, respondents were asked whether they knew people in each of the following categories: social workers, police officers or fire-fighters, food or beverage servers, labourers in landscaping or grounds maintenance, managers in sales, marketing or advertising, computer programmers, instructors or leaders in recreation and sport, security guards, engineers, farmers, nurses, janitors or caretakers, accountants or auditors, graphic designers or illustrators, delivery or courier drivers, early childhood educators or assistants, sewing machine operators, carpenters. The summation of answers to all these questions, which ranges from 0 to 18. It should be noted that this knowledge of people from various occupations does not necessarily relate to the same ego network as the measures of size and strength. In particular, size and strength relates to people to whom one is close, while knowledge would include people with whom one had weak ties.
In our analysis, a squared term of each of the five network measures was added to capture possible curvilinear relationships between the network measures and the dependent variables. Furthermore, to reduce the correlations between given variables and their squared items, and between given variables and associated interaction terms, stress level is measured as deviation from the mean and network measures are standardized (see Table 1).
For citeris paribus reasons, several control factors are introduced (see Table 1): age group (five year age group from 25 to 59), gender (female 50.3% and male 49.7%), marital status (single 16. 2%, married/common-law 75.3%, and others (divorced, separated, and widowed) 8.4%), work status (not working 22.8% and working 77.8%), education level (ten categories, used as a ratio level variable), religion (no religion 24.6%, Catholic 39.6%, Protestant 29.3%, and others 14.5%), place of birth (Canada 79.8% and outside Canada 20.2%), province (Quebec 24.9% and other than Quebec 75.1%), residence (urban (CMA/CA) 81.5% and rural (rural/small town) 18.5%), and number of children in the household (0 = none to 4 = four or more children).
Method
After examining the first-order correlations between the two health status measures and five components of social network, the analysis consists of six sets of regressions to examine the incremental contributions of various sets of variables in predicting general and mental health status. Model 1 introduces only the control variables. In Model 2, stress level is included to test its main effect on the dependent variables. Model 3 includes the network measures. In Model 4, the squared network measures are added. Model 5 has the interactions between the stress level and original social network measures, keeping only significant squared social network measures in the model. In the Final Model, only the significant interaction terms are included. The same sets of regressions are run for men and women respectively to examine whether the variables in the model affect their health statuses differently. All analyses results are weighted.Footnote 5
Results
As expected, the health measures are negatively related to the level of stress (Table 2). The bivariate associations also indicate that the network measures have positive relationships with all measures of health status.
Looking first at the total explained variance, the models associated with the two alternate measures of health are broadly similar (Table 3). The total explained variance on general health and mental health is in the order of 35.3 to 38.5% with the stress variable playing the largest role and the network variables and associated interactions adding a lesser amount to the explained variance. Stress plays a larger role in mental health than in general health, and this is especially the case for women. The network measures and their interactions with stress add 0.2% to male’s and 0.4% female’s explained variance for general health, and 1.5% and 0.9% to male and female explained variance for mental health.
The detailed impact of the variables are summarized in Tables 4 and 5, showing the final model for each of the two health status measures. Each table shows regression coefficients separately for men and women.
General Health Status
For general health, the only significant network predictor is that of friend network size which is positively related to women’s health (Table 4). All other network measures do not have a significant linear relationship with general health for either gender when all other variables in models are controlled. In particular, the frequency of contact with family and friends (strength) does not have a statistically significant relationship with either men or women’s general health status.
The coefficients of the squared network indicators are negative and significant for the indicator of family network size of both genders, and also for women’s friend network size, indicating curvilinear relationships with general health status. These relationships are displayed in Fig. 1a showing that the general health improves with size of family network until it reaches a point where greater size has a negative effect. For men, the turning point is around 0.3 SD above the mean or 9 family members while for women it is 0.5 SD below the mean or 4 family members. For women, the friend network size also has a turning point showing lower benefits on health after reaching 8 or 9 friends (Fig. 1b).

a The variation of the general health status with family network size within the range of two SD from the mean by gender. b The variation of female’s general health status with the friend network size within two SD from the mean. c The change of the impact of stress on male’s general health status with the network diversity within two SD from the mean
Stress has a stronger negative effect on general health for women (−0.101) than for men (−0.048) (Table 4). In addition, there are significant interactions between stress and network diversity in the case of men. As the interaction term is negative, this means that the negative effect of stress on the general health status is stronger with more network diversity for men (see Fig. 1c). That is, stress has a more negative effect on general health for men who know people from a more diverse set of occupations (more diverse network).
Mental Health Status
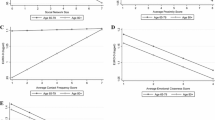
Turning to the impact of social network components on the mental health status, the results show better health for women and men with larger family network size and larger friend network size (Table 5). Both the friend network strength and network diversity have significant positive relationships with men’s mental health. In addition, only for men, the coefficients of the squared family and friend network size are significant. The negative signs for the squared terms of network sizes indicate a curvilinear relationship with mental health: that is, increases in network sizes have diminishing returns on mental health improvements (see Fig. 2a). However, the squared term is negative for men’s and positive for women’s family network strength. For men, this indicates that both low and high frequency of family contacts show lower mental health, while an intermediate frequency of contacts are related to better mental health. For women, it is those with intermediate contacts who have the poorest mental health (Fig. 2b).

a The variation of male’s mental health status with family and friend network size within two SD from the mean. b The variation of mental health status with family network strength within two SD from the mean by gender. c The variation of the impact of stress on male’s mental health status with the network diversity within two SD from the mean. d The variation of the impact of stress on female’s mental health status with the friend network size within two SD from the mean
There are also significant positive interaction terms between stress and (1) men’s network diversity and (2) women’s friend network size (see Table 5). This means that the negative effect of stress on mental health status is not as pronounced when men have more network diversity (Fig. 2c). Similarly, the negative effect of stress is lessoned when women have a larger network of friends (Fig. 2d).
Summary and Discussion
People interact and connect with each other through social networking and establishing social relationships. These social connections and the quality of these relationships are clearly important to health. This paper has sought to measure the impact of networks, their types (family vs friends), size (number of relatives and friends with whom one feels close), strength (frequency of seeing or communicating with relatives and friends) and diversity (number of occupations in which one knows people), on alternate measures of health. We have paid particular attention to the potential curvilinear nature of the relationships between the network measures and health in order to observe possible diminishing returns (significant negative coefficients in the squared terms measuring the network variables). We have also paid attention to stress as a factor in health, and especially to the interaction of network measures with the level of stress, in order to observe possible differential impacts of network considerations at various levels of stress.
As other studies have shown, social networks are more strongly associated with mental health than to physical health (Crimmins et al. 2011). Except in one case, we find the expected positive relationships between health and network size, strength and diversity. The exception involves men’s indicating worsening general health when they know people from a more diverse set of occupations. We also find that the network size is more important to both general and mental health than the frequency of contact (network strength). In particular, neither family nor friend network strength is associated with the general health, while the friend network strength is only associated with men’s mental health.
While many of the squared values of the network variables do not have statistically significant relationships with the health measures, in all but two cases the significant relationships have negative coefficients, indicating diminishing health returns at higher levels of the network measures. It may be that larger family networks can make strong demands and consequently bring deteriorating health. Pescosolido and Levy (2002) also find that larger networks may bring not only more care and concern, but also more regulation or oversight.
The interaction terms between stress and the various network measures are only occasionally statistically significant. Except in one case, the signs on these interaction terms are positive, indicating that the negative effect of stress on health is weakened with larger networks and more frequent contact. However, in the case of general health, men with higher stress have worsening health if they are in more diverse networks. It may be that, in the context of high stress, the more numerous comparisons associated with diverse networks can make people feel that their health is deteriorating.
This study confirms the buffering effect of social networks on the negative impact of stress on health, as found in previous research (Ryan et al. 2009; Greeff and Van Der Merwe 2004; Dubow and Tisak 1989). The curvilinear relationship between the social network measures and the health measures suggests that networks need to be considered as both support donors and support receivers. Each member of the social network changes between these two roles. Support receivers would mostly benefit from a large and strong network, but these could be a burden to support donors (Falci and McNeely 2009; Fingerman et al. 2004).
This study suffers from two important limitations. First, the causal order between networks and health probably goes in both directions (Brandt and Deindl 2017). Being based on cross-sectional data, this study cannot properly establish the causal relationships between the social network measures and health status (House et al. 1988). A second limitation is that the data set has only allowed us to capture some of the aspects of social networks. Size was only measured for “close” relatives and friends, thus weak ties were not captured. Strength was only measured through frequency of contact, while measures of density (network members knowing each other) would be more appropriate. Also, diversity was based on knowing people from various occupations. Besides being a limited way to capture diversity, this measure does not necessarily relate to the same network as the measures of size and strength since it would also capture diversity across weak ties.
Given the significance of networks to health, we need to look for adaptations that are important in the evolving society, or that would be appropriate in a given context. For instance, as more people live alone, to what extent can social media create supportive social networks? As immigration brings people from a diversity of origins, how can their networks be maintained or established? As geographic mobility and family dissolutions separate people, to what extent can formal structures fill the gap? The further study of social networks and their significance in various life domains will help in addressing these questions and in making the necessary adaptations.
Notes
Data analysis was done at the Research Data Center of Western University by using the detailed 2008 GSS data set.
This reduction in sample size is due to non-response on general state of health (0.66%), general state of mental health (0.71%), marital status (0.11%), religion of respondent (2.63%), working status (0.70%), country of birth (1.54%), education attainment (0.85%), stress level (0.96%), family network size (1.13%), friend network size (0.94%), family network strength (0.17%), and friend network strength (0.20%). The total non-response represents only 5.86% of persons aged 25–59 in the sample.
Ordinal regression was found to produce very similar results in terms of coefficients and significant levels.
The maximum value of family and friend network size is 200, with means of 7.42 and 5.96, and SD of 10.18 and 8.91respectively. Thus the family and friend network sizes are capped at 38 (7.42 + 10.18*3) and 33 (5.96 + 8.91*3).
Fractional weights are used so that the sample size after weighting is the same as the size of the sample under analysis.
References
Antonovsky, A. (1979). Health, stress and coping. San Francisco: Jossey Bass Publishers.
Antonovsky, A. (1987). Unraveling the mystery of health: How people manage stress and stay well. San Francisco: Jossey Bass Publishers.
Antonucci, T. C., & Jackson, J. S. (1990). The role of reciprocity in social support. In B. R. Sarason, I. G. Sarason, & G. R. Pierce (Eds.), Social support: An interactional view (pp. 173–198). New York: Wiley.
Baek, J., Hur, N. W., Kim, H. C., & Youm, Y. (2016). Sex-specific effects of social networks on the prevalence, awareness, and control of hypertension among older Korean adults. Journal Geriatric Cardiology, 13(7), 580–586.
Barger, D. S. (2013). Social integration, social support and mortality in the US National Health Interview Survey. Psychosomatic Medicine, 75, 510–517.
Berkman, F. L., & Glass, T. (2000). Social integration, social networks, social support, and health. In L. F. Berkman & I. Kawachi (Eds.), Social Epidemiology (pp. 137–173). New York: Oxford University Press.
Berkman, F. L., Glass, T., Brissette, I., & Seeman, T. E. (2000). From social integration to health: Durkheim in the new millennium. Social Science & Medicine, 51, 843–857.
Brandt, M., & Deindl, C. (2017). Causal links between social networks and health. Innovation in Aging, 1(1), 631.
Cohen, S. (2004). Social relationships and health. American Psychologist, 59(8), 676–684.
Cohen, S., & Syme, S. L. (1985). “Issues in the study and application of social support” in Social support and health edited by Sheldon Cohen and S. Leonard Syme. San Francisco: Academic Press.
Crimmins, Eileen M, Samuel H. Preston, and Barney Cohen. 2011. “Chapter 6 The Role of Social Networks and Social Integration.” In Explaining Divergent Levels of Longevity in High-Income Countries. National Research Council (US) Panel on Understanding Divergent Trends in Longevity in High-Income Countries, Washington (DC): National Academies Press.
Devlin, R. A., & Rudolph-Zbarsky, J. (2014). Social networks and the probability of having a regular fami1ly doctor. Social Science & Medicine, 115, 21–28.
Dubow, F. E., & Tisak, J. (1989). The relation between stressful life events and adjustment in elementary school children: The role of social support and social problem solving skills. Child Development, 60, 1412–1423.
Ehrhardt, G., Marsili, M., & Vega-Redondo, F. (2007). Emergence and resilience of social networks: A general theoretical framework. Annals of Economics and Statistics / Annales d'Économie et de Statistique, 86(Apr. - Jun., 2007), 1–13.
Falci, C., & McNeely, C. (2009). Too many friends: Social integration, network cohesion and adolescent depressive symptoms. Social Forces, 87(4), 2031–2061.
Fingerman, L. K., Hay, E. L., & Birditt, K. S. (2004). The best of ties, the worst of ties: close, problematic, and ambivalent social relationships. Journal of Marriage and Family, 66(3), 792–808.
Gage, A. E. (2013). Social networks of experientially similar others: Formation, activation, and consequences of network ties on the health care experience. Social Science & Medicine, 95, 43–51.
García, E., López, J., Banegas, R., Pérez-Regadera, G. A., Cabrera, H. R., & Rodríguez-Artalejo, F. (2005). Social network and health-related quality of life in older adults: A population-based study in Spain. Quality of Life Research, 14(2), 511–520.
Garmezy, N., & Rutter, M. (Eds.). (1983). Stress, Coping and Development in Children. New York: McGraw- Hill. Times New Roman.
Greeff, A. P., & Van Der Merwe, S. (2004). Variables Associated with Resilience in Divorced Families. Social Indicators Research, 68, 59–75.
Griffiths, F., Cave, J., Boardman, F., Ren, J., Pawlikowska, T., Ball, R., Clarke, A., & Cohen, A. (2012). Social networks - The future for health care delivery. Social Science & Medicine, 75, 2233–2241.
Hafner-Burton, E. M., Kahler, M., & Montgomery, A. H. (2009). Network Analysis for International Relations. International Organization, 63(3), 559–592.
Holt-Lunstad, J., Smith, T. B., & Layton, B. J. (2010). Social relationships and mortality risk: A meta-analytic review. PLoS Medicine, 7(7), 1–20.
House, J. S., Landi, K. R., & Umberson, D. (1988). Social Relationships and Health. Science, 241(4865), 540–545.
Howard, E. (2006). The informal social support, well-being, and employment pathways of low-income mothers. In H. Yoshikawa, T. S. Weisner, & E. Lowe (Eds.), Making it work: Low-wage employment, family life, and child development (pp. 256–272). New York: Russell Sage Foundation.
Ikeda, K.'i., & Richey, S. E. (2005). Japanese Network Capital: The Impact of Social Networks on Japanese Political Participation. Political Behavior, 27(3), 239–260.
Kiecolt-Glaser, J. K., Dura, J. R., Speicher, C. E., Trask, O. J., & Glaser, R. (1991). Spousal caregivers of dementia victims: Longitudinal changes in immunity and health. Psychosomatic Medicine, 53, 345–362.
Kim, Y. C., & Rhee, M. (2010). The contingent effect of social networks on organizational commitment: A comparison of instrumental and expressive ties in a multinational high technology company. Sociological Perspectives, 53, 479–502.
Krause, J., Croft, D. P., & James, R. (2007). Social network theory in the behavioural sciences: Potential applications. Behavioral Ecology and Sociobiology, 62(1), 15–27.
La Due Lake, R., & Huckfeldt, R. (1998). Social capital, social networks, and political participation. Political Psychology Special Issue: Psychological Approaches to Social Capital, 19(3), 567–584.
Li, T., & Zhang, Y. (2015). Social network types and the health of older adults: Exploring reciprocal associations. Social Science & Medicine, 130, 59–68.
Lincoln, D. K., Chatters, L. M., & Taylor, R. J. (2005). Social support, traumatic events, and depressive symptoms among African Americans. Journal of Marriage and Family, 67(3), 754–766.
Marquez, B., Elder, J. P., Arrendondo, E. M., Madanat, H., Ji, M., & Ayala, G. X. (2014). Social network characteristics associated with health promoting behaviors among Latinos. Health Psychology, 33(6), 544–553.
Martire, M. L., & Franks, M. M. (2014). The role of social networks in adult health: Introduction to the special issue. Health Psychology, 33(6), 501–504.
Murata, T. (2010). “Chapter 12 Detecting Communities in Social Networks” In Handbook of social network technologies and applications, B. Furht (ed.), Springer Science+Business Media, LLC, Boston, MA.
Passy, F., & Giugni, M. (2001). Social networks and individual perceptions: Explaining differential participation in social movements. Sociological Forum, 16(1), 123–153.
Pescosolido, B. A., & Levy, J. A. (2002). The role of social networks in health, illness, disease and healing: The accepting present, the forgotten past, and the dangerous potential for a complacent future. Social Networks and Health, 8, 3–25.
Ryan, R. M., Kalil, A., & Leininger, L. (2009). Low-income mothers’ private safety nets and children’s socio-emotional well-being. Journal of Marriage and Family, 71, 278–297.
Schulz, R., & Beach, S. R. (1999). Caregiving as a risk factor for mortality: The caregiver health effects study. The Journal of the American Medical Association, 282(23), 2215–2219.
Shemtov, R. (2003). Social networks and sustained activism in local NIMBY campaigns. Sociological Forum, 18(2), 215–244.
Sih, A., Hanser, S. F., & McHugh, K. A. (2009). Social network theory: New insights and issues for behavioral ecologists. Behavioral Ecology and Sociobiology (Social Networks: New Perspectives), 63(7), 975–988.
Smith, P. K., & Christakis, N. A. (2008). Social networks and health. Annual Review of Sociology, 34, 405–429.
Sneed, R. S., & Cohen, S. (2014). Negative social interactions and incident hypertension among older adults. Health Psychology, 33(6), 554–565.
St. Clair, P. A., Smeriglio, V. L., Alexander, C. S., & Celentano, D. D. (1989). Social network structure and prenatal care utilization. Medical Care, 27(8), 823–832.
Statistics Canada. 2009. 2008 General Social Survey: Selected Tables on Social Engagement. Statistics Canada, Social and Aboriginal Statistics Division. Ottawa. Catalogue no. 89-640-X.
Szell, M., & Thurner, S. (2013). How women organize social networks different from men. Scientific Reports, 3(1214), 1–6.
Umberson, D., Williams, K., Thomas, P. A., Liu, H., & Thomeer, M. B. (2014). Race, gender, and chains of disadvantage: Childhood adversity, social relationships, and health. Journal of Health and Social Behavior, 55(1), 20–38.
van Dijk, F. (1998). Private support and social security. Journal of Population Economics, 11(3), 345–371.
Walker, G., Kogut, B., & Shan, W. (1997). Social capital, structural holes and the formation of an industry network. Organization Science, 8(2), 109–125.
Wang, M. C., Haertel, G. D., & Walberg, H. J. (1997). Fostering educational resilience in inner-city schools. In M. C. Wang, G. D. Haertel, & H. J. Walberg (Eds.), Children and youth (pp. 119–140). Newbury Park: Sage.
Wayman, J. C. (2002). The utility of educational resilience for studying degree attainment in school dropouts. The Journal of Educational Research, 95, 167–178.
Zhang, M. (2010). Chapter 1 social network analysis: History, concepts, and research. In B. Furht (Ed.), Handbook of social network technologies and applications. Boston, MA: Springer Science+Business Media, LLC.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
No Conflict of interest/Ethical statement.
Rights and permissions
About this article

Cite this article
Liu, J., Beaujot, R. & Ravanera, Z. Measuring the Effects of Stress and Social Networks on the Health of Canadians. Applied Research Quality Life 13, 891–908 (2018). https://doi.org/10.1007/s11482-017-9565-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11482-017-9565-0