
Abstract
The current study assesses the evidence for the association between several neighborhood social processes (collective efficacy and social disorder) and two important individual-level quality of life indicators, which are avoidance behaviour and mental health. In addition to these neighborhood characteristics, the study also assesses the impact of an individual’s social support network on these two outcomes. Hypotheses are derived from a theoretical framework that integrates insights from social capital theory, collective efficacy theory and broken windows theory. Hypotheses about both neighborhood- and individual-level effects are tested by applying multilevel analyses to data from the ‘Social capital and Well-being In Neighborhoods in Ghent’ (SWING) survey of 2011, which consists of face-to-face interviews among the adult population in the second largest municipality of Belgium. Results suggest that individuals living in neighborhoods with lower levels of social trust and higher levels of disorder report more avoidance behaviour. Neighborhood effects on mental health are rather negligible. Individuals who experience more social support report both a better mental health and fewer avoidance behaviour.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Following the World Health Organization Quality of Life Assessment (WHOQOL), quality of life is a subjective, multi-dimensional concept that can include both positive and negative dimensions (Kuyken et al. 1995). The WHO defines it as ‘a broad ranging concept, incorporating in a complex way individuals’ physical health, psychological state, level of independence, social relationships, personal beliefs and their relationships to salient features of the environment’ (Kuyken et al. 1995, p. 1405). When studying the quality of life of individuals it is important to take into account this broad nature of the concept by clearly delineating the dimensions and approaches. In current quality of life studies, the idea of measuring human development from a more subjective point of view is becoming more important. As a consequence, the concept of subjective well-being can be considered as one of the most popular measures of quality of life. The book ‘Subjective Well-Being and Security’ (Webb and Herrera 2012) makes clear that subjective well-being ‘encompasses a subjective appraisal, including cognitive and affective dimensions’ and ‘is appraised as perceived and felt by an individual’.
This study focusses on this subjective approach of quality of life by examining two important indicators that refer to the psychological state of an individual, which are avoidance behaviour and mental health. In criminological literature, avoidance behaviour is perceived as one of the main dimensions of fear of crime. Fear of crime is a broad concept that can be divided into a cognitive, an emotional and a behavioral dimension (Farrall et al. 2009; Hale 1996). Ferraro’s definition (Ferraro 1995, p. 4) describes the content of fear of crime very well: ‘an emotional response of dread or anxiety to crime or symbols that a person associates with crime’. In other words, fear of crime is an emotion, fear of crime is a reaction, and in particular fear of crime refers to crime or symbols that can be associated with crime. A narrow interpretation of this definition points to the emotional affective component of fear of crime. Following some well-known classifications (Ferraro and Lagrange 1987; Gabriel and Greve 2003) a broad interpretation of the fear of crime concept also demonstrates the importance of a cognitive and a behavioural component. The cognitive component comes before the emotional affective component and refers to a process that converts signals and stimuli which have to do with threat and danger into a risk assessment of personally becoming a victim of crime. The behavioural component comes after the emotional affective component and refers to the behavioural reactions of fear, such as avoidance and defensive behaviour. As such, avoidance behaviour can be defined as the defensively reaction of an individual to an emotional state of fear (Ferraro and Lagrange 1987; Gabriel and Greve 2003). Within the context of the quality of a society, mental health problems are considered as one of the major social ills of modern societies (Layard and Layard 2011). Recent research suggest that positive and negative aspects of mental health are not necessary highly correlated (Bergsma et al. 2011). In this study, we focus on the negative aspects of mental ill-heath, which refers to the anxiety, depression, loss of behavioral or emotional control, and lack of psychological well-being of an individual (McKenzie and Harpham 2006; Ware and Sherbourne 1992).
The particular neighborhood in which an individual resides might have a significant impact on his quality of life. At the end of the nineteenth and the beginning of the twentieth century scholars of the classic Chicago School, which played a primary role in the development of urban sociology, already documented the uneven distribution of a multitude of social problems such as crime, mental disorders, physical abuse and alcoholism in the impoverished areas surrounding the city centre (Faris and Dunham 1939; Park 1915; Shaw and Mckay 1942; Wirth 1938). It was argued that structural characteristics of neighborhoods (population density, poverty, ethnic heterogeneity, and residential mobility) fostered the breakdown of traditional institutions of informal control, which in turn gave rise to concentrations of crime and health problems (Faris and Dunham 1939; Sampson and Groves 1989; Shaw and Mckay 1942). Partly following the footsteps of the early Chicago sociologists, scholars have developed new theoretical frameworks such as social capital theory (Coleman 1988; Putnam 1993), collective efficacy theory (Sampson et al. 1997) and broken windows theory (Kelling and Coles 1996) in which they further elaborated the specific social processes that are responsible for the link between structural characteristics of neighborhoods and concentrations of crime and health problems. In this study we apply some of their insights to increase our understanding of the association between neighborhood characteristics and an individual’s quality of life. More specifically, we focus on the impact of neighborhood social trust, informal social control and social disorder, which are central processes within collective efficacy and broken windows theory. In addition to these neighborhood characteristics and based on social capital theory the individual level of social support might have a clear link with one’s quality of life.
This study adds to the empirical knowledge on the relationship between neighborhood conditions and quality of life outcomes in three particular ways: (1) Two important distinct dimensions of quality of life are included and compared – avoidance behaviour and perceived mental health; (2) a distinction is made between three specific neighborhood social processes – social trust, informal social control and social disorder; and (3) next to these neighborhood characteristics, we take into account the role of individual social capital, which is not necessarily tied to the neighborhood. Furthermore, a methodological surplus value is created by measuring neighborhood social processes using a community survey of professional key informants (Pauwels and Hardyns 2009). As further discussed in the method section, by measuring neighborhood social processes independently from the individual characteristics, independent measures are obtained.
Theoretical Background
This study is guided by an integrated theoretical framework, based on social disorganisation theory. Whereas the original social disorganisation theory only focused on structural characteristics, social capital dimensions such as the lack of social trust were unmeasured. Contemporary elaborations of social disorganisation theory further enriched the theory by linking neighborhood conditions and dimensions of social capital to disentangle the micro–macro links, or the micro foundations of macro-level theory.
In literature, a distinction can be observed between two different conceptualizations of social capital (Kawachi et al. 2004): on the one hand, a social cohesion school which tends to emphasize cohesive processes as the property of a group (e.g., social trust and informal social control in communities or neighborhoods) and, on the other hand, a network school which sees social capital as the resources that are embedded within an individual’s social networks (e.g., social support of individuals) (Kawachi et al. 2008; Lin 1999). However, this distinction in particular and the social capital debate in general are not without critiques.
Social capital is generally used to refer to a myriad of aspects of the social context, ranging from, but not limited to, levels of social support, frequency of social contact with others, social cohesion or generalized trust (Macinko and Starfield 2001). It entails both quantitative (e.g., frequency of informal social contacts) and qualitative (e.g., levels of trust) aspects of the social context, which are respectively labelled as structural and cognitive components of social capital (Baum and Ziersch 2003; Harpham 2008). Notwithstanding the way in which social capital is operationalised, the central idea behind the concept is that being connected to others can provide people access to resources (tangible and/or intangible) they do not own themselves (Macinko and Starfield 2001). However, a clear distinction between social capital at the individual and collective level is considered problematic (Kawachi et al. 2008) due to at least two reasons. Firstly, a mutual dependency between social capital at the individual and collective level is observed, in the form of an accumulation, compensation or differentiation of social capital at these different operational levels. For more information on these forms, we refer to (Kim et al. 2011; Möhnen et al. 2012; Poortinga 2006). Secondly, a positive association between quality of life and social capital at the neighborhood level might reflect both the clustering of inhabitants with specifically beneficial individual social capital in specific neighborhoods (‘compositional effect’) and/or a ‘true’ effect of neighborhood social capital (‘contextual effect’) (Lindstrom et al. 2002; Subramanian et al. 2003). Therefore, information on social capital at the individual level is needed to fully interpret the relationship between quality of life outcomes and social capital at the collective level.
The following paragraphs further elaborate on the different theoretical concepts in our framework and discuss in detail how they impact an individual’s quality of life.
Neighborhood Collective Efficacy
Collective efficacy theory underlines the importance of a neighborhood’s capacity to solve its commonly identified problems, such as concentrations of unhealthy living conditions, insecurity, and crime (Kawachi and Berkman 2003; Sampson 2003; Sampson 2012; Sampson et al. 1997). Collective efficacy is defined as ‘social cohesion among neighbors combined with their willingness to intervene on behalf of the common good’ (Sampson et al. 1997). This definition makes a clear link between two main dimensions of collective efficacy, which are social trust (or social cohesion) and informal social control. Communities have collective efficacy when the combination of both social trust and informal social control is present. Social trust in a neighborhood is an essential condition that fosters informal social control, and thus the willingness to intervene for the common good. Therefore, neighborhoods characterised by high levels of collective efficacy might be more resistant to high local concentrations of disorder and crime and, therefore, show beneficial effects on the quality of life of its residents (Sampson 2012). These effects of collective efficacy on quality of life can be understood as both direct, as indirect through the reduced neighborhood level of disorder and crime.
Neighborhood Disorder
Broken windows theory and Mirowsky and Ross’ condition-cognition-emotion theory emphasize the detrimental effects of social and physical disorder on several indicators of quality of life such as distress and fear of crime (Innes 2004; Kelling and Coles 1996; Ross and Mirowsky 2001, 2009; Skogan 1990; Wilson and Kelling 1982). Disorder may trigger a chain of negative events (or spiral of decline) that ultimately leads to higher crime rates in neighborhoods and reduced quality of life for its inhabitants. As a consequence, it might be expected that neighborhoods that lack collective efficacy have to cope with more social and physical disorder which, in turn, directly increases the risk of lower levels of quality of life among its residents (Sampson 2003; Sampson 2012).
Individual Social Support
Besides the neighborhood social climate, it is important to focus on the individual’s social network in relation to quality of life. Social networks are linked to quality of life because of the support they provide (Berkman et al. 2000; Colvin et al. 2002). Individual social support does not solely refer to local social ties that are embedded in the neighborhood, but also to the support of social networks that are not bounded by the neighborhood. Researchers have found that one’s social support is beneficial for mental and physical health, e.g., general well-being and the absence of the symptoms of diseases, and reduces the risk of feeling unsafe, depressive or oppressive (Coyne and Downey 1991; Sacco 1993; Thoits 1985; Thoits 1995, 2011; Wright and Cullen 2001). Social support directly enhances an individual’s quality of life by providing opportunities for interaction, help with practical tasks, and relieving feelings of loneliness (Ganster and Victor 1988; Makarios and Livelsberger 2013).
Conceptual Model and Hypotheses
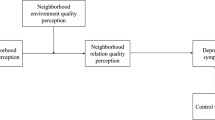
The research hypotheses tested in this study were constructed stepwise according to the structure of the contextual model (see Fig. 1):
-
H1: Significant variation in avoidance behaviour and mental health can be attributed to the neighborhood level.
-
H2: The neighborhood variation in avoidance behaviour and mental health exists independently of the neighborhood composition (i.e., socio-demographic characteristics of individuals).
-
H3: Neighborhood social trust and informal social control are associated with lower levels of avoidance behaviour and higher levels of mental health, independent of the neighborhood’s demographic composition.
-
H4: Neighborhood disorder is associated with higher levels of avoidance behaviour and lower levels of mental health, independent of the neighborhood’s demographic composition, and reduces the effects of neighborhood social trust and informal social control.
-
H5: An individual’s social support is associated with lower levels of avoidance behaviour and higher levels of mental health, independent of the individual’s socio-demographic background and neighborhood processes.

Hypothesized effects on quality of life
Data and Methods
Design and Context
This study draws upon data from the Social capital and Well-being In Neighborhoods in Ghent (SWING) survey of 2011. This survey consists of face-to-face interviews with 1025 neighborhood inhabitants and 638 key informants in 50 neighborhoods in Ghent. Ghent is the third largest city in Belgium, 158 km2 in size, with approximately 250.000 inhabitants (1.506/km2). The city is divided into 201 statistical sectors. A statistical sector (henceforth referred to as ‘neighborhood’) comprises the smallest administrative unit of analysis at which demographic and socio-economic information is systematically gathered in Belgium and can be compared to the US census tract level (on average 1.319 inhabitants/neighborhood). The survey provides information on social processes, quality of life indicators and socio-demographic characteristics at both the individual and neighborhood level.
Sampling and Data Collection
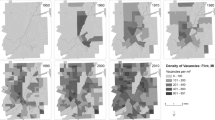
First, a stratified sample of 50 neighborhoods was selected from the 142 neighborhoods in Ghent with a minimum population size of 200 inhabitants (see figure 2). Neighborhoods were randomly selected following a stratified selection procedure based on population density and the level of deprivation (deprived versus non-deprived), resulting in a representative set of neighborhoods. The inclusion of adjacent neighborhoods was avoided in order to keep the impact of spatial proximity to a minimum.

Selected neighborhoods. The selected non-deprived neighborhoods are indicated in gray, and the selected deprived neighborhoods are indicated with diagonal lines
Second, in each of the 50 selected neighborhoods, two independent surveys were administered: a survey of inhabitants to collect data about individual characteristics and a survey of key informants to collect data about neighborhood social processes. Using the municipal registry, we randomly selected inhabitants from each neighborhood through a stratified sampling design (stratification by age, sex and nationality). In total, 1025 inhabitants took part in the survey (response rate of 52 %). The survey was administered face-to-face, except for the measurement of mental health, which was administered in a short self-administered questionnaire to avoid response bias. Additionally, we selected a sample of so-called key informants in each neighborhood to collect data about the neighborhood social processes. Key informants are defined as ‘persons who are in a ‘privileged’ position to provide detailed information on local area processes’ (Pauwels and Hardyns 2009, p. 404).Footnote 1 In this study, key informants are people who work professionally (or voluntarily) in one of the selected neighborhoods, and, therefore, can observe and experience what is happening in these neighborhoods. Key informants like family doctors, policemen, local community workers, postmen, café/pub owners or staff of other local catering industry, often have more accurate knowledge about the social processes under study than the ‘average’ inhabitant who lives in neighborhood x but works in neighborhood y, and provide more accurate and less biased information. Another important advantage of using carefully selected professional key informants to measure neighborhood processes is that neighborhood level data is totally independent of the individual level inhabitants’ data. Finally, due to the increased accuracy, few respondents are necessary per neighborhood to obtain reliable and valid measures of social processes. Previous studies have demonstrated that key informant surveys are able to generate ecologically reliable and valid measures of neighborhood social processes (Pauwels and Hardyns 2009). In total, 638 key informants were reached across 50 neighborhoods. More detailed information can be found online in the technical report of the SWING study 2011 (https://biblio.ugent.be/publication/4164887).
Measures
Dependent Variables
We studied two important individual-level indicators of quality of life, which are avoidance behaviour and perceived mental health. Avoidance behaviour was measured by asking the respondents to indicate (on a 5-point scale ranging from ‘never’ to ‘very often’) on three items how many times they exhibited avoidance behaviour, such as ‘avoiding certain areas in the neighborhood because they are not safe’. Item responses were summed to create a single measure with higher scores indicating higher levels of avoidance behaviour (α = 0.77). Mental health refers to the perceived anxiety, depression, loss of behavioral or emotional control, and psychological well-being of an individual (Ware and Sherbourne 1992). The construct was measured with the 5-item scale on symptoms of depression and nervousness from the SF-36 mental health scale. Higher scores refer to better mental health (α = 0.79). The respondents were asked to answer five questions (on a 6-point scale ranging from ‘always’ to ‘never’) that measure their well-being during the past 4 weeks, such as ‘have you been a very nervous person?’. Previous international research supports the construct validity of the SF-36 mental health scale (Hamano et al. 2010; Hays et al. 1995).
Explanatory Variables – Individual Level Measures
Individual background characteristics are used as statistical controls to distinguish contextual effects from neighborhood compositional effects. Two types of background variables are included in the analyses. First, the socio-demographic variables age (in years) and gender (0 = male, 1 = female). Second, the socioeconomic variables education (0 = primary, 1 = secondary, 2 = higher) and home ownership (0 = owner, 1 = tenant). To measure individual social support respondents were asked to indicate for 4 items (on an 8-point scale ranging from “0” to “more than 11”) how many friends, family members or acquaintances would give practical support, such as “take you to the doctor/hospital when you are too ill to get there by yourself”. Responses were summed to create a measure with higher scores indicating higher levels of individual social support (α = 0.87). This scale is a short version of the social support questionnaire in the MOS Social Support Survey (Sherbourne and Stewart 1991).
Explanatory Variables – Neighborhood Level Measures
Neighborhood social processes were measured through the key informant technique as discussed earlier. The construction of the corresponding variables proceeded in two steps (Oberwittler and Wikström 2009). First, scales were used to measure perceived neighborhood social trust, informal social control and disorder at the individual (key-informant) level. Second, and after checking the ecological reliability, summed scores on these scales were aggregated to the neighborhood level, according to the neighborhood in which key informants resided. The measures of social trust and informal social control, as the two key dimensions of collective efficacy, are based on the influential work of (Sampson et al. 1997). Social trust, a summated scale (α = 0.81) with higher scores indicating higher levels of social trust, consists of five items, such as ‘people around here are willing to help their neighbors’. Key informants were asked to indicate (on a 5-point scale ranging from “totally disagree” to “totally agree”) how strongly they agreed with each of these items. To measure informal social control key informants were asked (on a 5-point scale ranging from “very likely” to “very unlikely”) about the likelihood that their neighbors could be counted on to intervene in various ways if problem situations appear, such as ‘children were skipping school and hanging out on a street corner’. Higher scores on this 5-item measure (α = 0.82) indicate higher levels of informal social control. Neighborhood disorder was assessed by asking key informants (on a 5-point scale ranging from “never” to “very often”) how often they have observed six occurrences in their neighborhood, such as “adolescents hanging around on street corners”. Responses were combined into a single measure with high scores indicating higher levels of disorder (α = 0.85).
Analytic Strategy
The MLwiN software (version 2.25) was used to perform a two-level hierarchical linear regression model with individuals at level 1 and neighborhoods at level 2. Restricted maximum likelihood estimates for the model parameters are obtained through the restricted iterative generalized least squares algorithm (Goldstein 2003). Listwise deletion is used to exclude cases with missing values. Only 15 cases for avoidance behaviour (1.5 %) and 17 cases for mental health (1.7 %) had to be excluded from the analysis due to missing values. Independent continuous variables are centered around their grand-mean to make the intercept more easily interpretable.
For each dependent variable, a series of five models (corresponding to our five research hypotheses) is tested in a blockwise analysis. First, an intercept only-model is fitted, without any level 1 or level 2 predictors. This model serves as a benchmark against which other models can be compared and partitions the variance in between neighborhood and within neighborhood variance. Model 1 includes the individual background variables to control for the neighborhood composition. In model 2 neighborhood social trust and informal social control are entered as independent constructs. Neighborhood disorder is added in model 3 in order to verify whether this variable is associated with quality of life outcomes, independent of neighborhood composition, and to evaluate the strength of the association of collective efficacy with quality of life. In the final model, individual social support is included at the individual level to test whether this variable is associated with lower levels of quality of life, independent of the individual’s background and neighborhood collective efficacy and disorder. A likelihood ratio test (based on the deviances) was used to evaluate the improvement of fit for each model.Footnote 2
Results
Descriptives and Bivariate Correlation Coefficients Between Neighborhood-Level Measures
Univariate statistics for all individual-level and neighborhood-level variables can be found in Table 1. Respondents (N = 1025) are between 18 and 88 years old (average age = 47). Men and women are more or less equally distributed in the overall sample. Less than half of the respondents have higher education (43.6 %), and about one third are house tenants (31.6 %). At the neighborhood level, we can observe high variation in neighborhood disorder.
Table 2 presents the bivariate correlations between neighborhood-level variables. Not unsurprisingly, many of these variables are highly correlated. Socioeconomic disadvantage and disorder correlate nearly perfectly (R = 0.79). For reasons of multicollinearity, socioeconomic disadvantage is excluded from the multilevel analyses. One other notable observation, which comprises a marked difference with the US collective efficacy studies, is that the two subcomponents of collective efficacy, social trust and informal social control, are not connected to each other (R = 0.06 with p > 0.05). Although neighborhood studies in the US have shown that local settings with a high degree of social trust generally also have a high degree of informal social control (R = 0.80 with p < 0.001 in Sampson et al. 1997), this is not the case in this study. This finding could indicate that collective efficacy results from a specific international context cannot simply be transferred and applied to other countries and settings.
Multilevel Models
Tables 3 and 4 present the results of five successive multilevel models for avoidance behaviour and mental health, respectively. Model 0 shows that 7.7 % of the variance in avoidance behaviour and 1.7 % of the variance in mental health is situated at the neighborhood level. The grand-mean (represented by the intercept) for the avoidance behaviour scale (5.75, range 3–15) and the mental health scale (74.25, range 12–100) indicates that people with high levels of avoidance behaviour are in the minority in our sample, while people with high levels of mental health are in the majority.
Model 1 shows the impact of individual background characteristics. Women, tenants, lower educated, and older respondents report significantly higher levels of avoidance behaviour. Women and tenants also report significantly lower levels of mental health. Age and education are not significantly associated with self-reported levels of mental health. The small amount of variation in mental health found at the neighborhood level is almost entirely determined by the compositional effect of gender and homeownership. However, a considerable amount of neighborhood level variation remains in case of avoidance behaviour, even after controlling for neighborhood composition.
In model 2 we evaluate the impact of the two dimensions of neighborhood collective efficacy (social trust and informal social control), independent from the neighborhood’s demographic composition. Higher levels of neighborhood social trust are associated with lower levels of avoidance behaviour and better mental health.Footnote 3 Informal control has no significant association with either avoidance behaviour or mental health. If we look at the ICC we can see that social trust substantially reduced the between-neighborhood variance in avoidance behaviour, while the between-neighborhood variance in mental health is now entirely gone.
Model 3 shows the extent to which neighborhood disorder is associated with avoidance behaviour and mental health, independent from the neighborhood’s demographic composition and neighborhood collective efficacy. With respect to avoidance behaviour this seems to be the case indeed. The net-effect of social trust becomes non-significant once neighborhood disorder is introduced in the model. Furthermore, our hypothesis concerning the effect of disorder is corroborated: higher levels of neighborhood disorder are associated with higher levels of avoidance behaviour. In the mental health model, none of the neighborhood characteristics has a significant effect. Moreover, adding neighborhood disorder does not lead to a better model fit. This is not so surprising because of the small amount of variation between neighborhoods in mental health and the fact that the confidence interval of the only significant association (social trust) was already close to zero in the previous model.
In the final model, individual social support is included at the individual level. We can observe that social support matters. Those who report higher levels of individual social support also report fewer avoidance behaviour. Given the very small association, however, it is not unexpected that - with the notable exception of the effect of home ownership (which becomes non-significant) - the values for the other parameters in the model do not substantially change. Also, in the mental health model, individual social support has a significant effect, and including the variable renders home-ownership insignificant. Higher levels of individual social support are associated with higher levels of mental health.
Conclusion and Discussion
This study has shown noticeable differences when studying different dimensions of quality of life. With regard to mental health, the neighborhood impact is limited to a minimum, while with regard to avoidance behaviour we could observe that neighborhood characteristics, however relatively small, does significantly matter. More specifically we found significant associations of neighborhood social distrust and social disorder with avoidance behaviour. People living in those neighborhoods tend to report more avoidance behaviour, independent of their demographic background. In this regard, we want to stress that the direct association of social disorder is stronger than the association of social trust with avoidance behaviour. From a policy point of view, this could indicate that diminishing the visual triggers of disorder could be more effective to reduce inhabitants’ avoidance behaviour. Besides neighborhood aspects of the social climate, it is important to mention the role of individual social support. The social support an individual can count on does make a difference for both components of quality of life in this study.
One remarkable result in this study is that social trust and informal social control do not correlate at the neighborhood level of analysis. In line with previous findings of Carpiano (2006), (Hardyns 2012; Pauwels and Hardyns 2010), this is a new indication that, dependent on the specific setting, the collective efficacy concept, as measured by key informants, should be split into both dimensions when studying contextual effects. Other researchers have emphasized that collective efficacy results from a specific international context cannot simply be transferred and applied to other countries and settings (Reisig and Cancino 2004; Zhang et al. 2009). One major criticism made by the authors is that the questions used to measure informal social control are excessively geared to the big-city context and are not suited to regional cities or a more rural context.
Two other methodological findings need to be noticed. Firstly, neighborhoods were operationalized by using administrative units in this study. It is not clear to what extent these units coincide with what the respondents perceive as their neighborhood (Stafford et al. 2008). Although we followed the advice ‘smaller is better’ (Oberwittler and Wikström 2009) by selecting the lowest level administrative units available in Belgium, the possibility remains that neighborhood-effects are underestimated due to heterogeneity in the environmental conditions within these geographical areas. For that reason, it could be interesting to execute similar studies in other promising output areas which are even smaller, such as street segments or street-blocks (Weisburd et al. 2009). Secondly, we must bear in mind the problem of strong multicollinearity between socioeconomic disadvantage and disorder. To avoid too much inflation of the standard errors, we had to exclude the socioeconomic disadvantage index from the multilevel models. Nevertheless, additional exploratory analyses revealed that the effect of socioeconomic advantage on avoidance behaviour remained strong, even after controlling for collective efficacy and disorder. This indicates that we have not yet identified all the individual and/or neighborhood-level processes that can explain why people living in disadvantaged neighborhoods report more avoidance behaviour.
To conclude we want to draw special attention to some recommendations for future studies on the relation between social capital and quality of life. Firstly, it seems reasonable to accept that neighborhood effects on someone’s quality of life is dependent on individual characteristics such as the length of residence of an individual in the neighborhood. For that reason the study of interaction effects could give a more detailed picture in the constellation of someone’s quality of life. Secondly, collective efficacy could also be measured by asking neighborhood inhabitants, instead of key informants, on their perceived social trust and their perceived informal social control of their neighborhood. It can be argued that key informants have less accurate knowledge on the informal social control within a neighborhood than neighborhood inhabitants themselves. Future research could focus on the external validity of these measures. Last, the combination of neighborhood and individual measures of social capital needs to be stimulated in future studies. In a society where geographic mobility is constantly growing, it can be expected that individual dimensions of social capital become more important than neighborhood dimensions of social capital, or at least intensively interact with each other.
Notes
The point of departure is that the privileged witness represents an important additional source of information to supplement the more established resident surveys. The importance of this principle has been noted by (Campbell 1955), who wrote: ‘if the use of informants as a social science research tool is to be developed, it seems likely that principles of optimal selection will have to be developed.’ The principle of optimal selection should ensure that the knowledge of professional key informants exceeds the knowledge of ordinary residents.
This likelihood ratio test statistic follows a chi-square distribution with degrees of freedom equal to the difference in the number of parameters estimated in the two models (Hox 2010).
Nevertheless, additional analyses reveal that the confidence interval associated with the effect of neighborhood social trust on mental health is very close to zero [CI: 0.09–1.73], which indicates uncertainty about the magnitude of its effect in the population.
References
Baum, F., & Ziersch, A. M. (2003). Social capital. Journal of Epidemiology and Community Health, 57(5), 320–323.
Bergsma, A., Ten Have, M., Veenhoven, R., & De Graaf, R. (2011). Mental disorders and happiness; a 3-year follow-up in the Dutch general population. The Journal of Positive Psychology, 6(4), 253–259.
Berkman, L. F., Glass, T., Brissette, I., & Seeman, T. E. (2000). From social integration to health: Durkheim in the new millennium. Social Science and Medicine, 51(6), 843–857.
Campbell, D. T. (1955). The informant in quantitative research. American Journal of Sociology, 60(4), 339–342.
Carpiano, R. M. (2006). Toward a neighborhood resource-based theory of social capital for health: can Bourdieu and sociology help? Social Science and Medicine, 62(1), 165–175.
Coleman, J. S. (1988). Social capital in the creation of human-capital. American Journal of Sociology, 94, S95–S120.
Colvin, M., Cullen, F. T., & Vander Ven, T. (2002). Coercion, social support, and crime: an emerging theoretical consensus. Criminology, 40(1), 19–42.
Coyne, J. C., & Downey, G. (1991). Social-factors and psychopathology - stress, social support, and coping processes. Annual Review of Psychology, 42, 401–425.
Faris, R. E., & Dunham, H. W. (1939). Mental disorders in urban areas: an ecological study of schizophrenia and other psychoses. Chicago: The University of Chicago Press.
Farrall, S. D., Jackson, J., & Gray, E. (2009). Social order and the fear of crime in contemporary times. Oxford: Oxford University Press.
Ferraro, K. (1995). Fear of crime: interpreting victimization risk. Albany: State University of New York Press.
Ferraro, K. F., & Lagrange, R. (1987). The measurement of fear of crime. Sociological Inquiry, 57(1), 70–101.
Gabriel, U., & Greve, W. (2003). The psychology of fear of crime - Conceptual and methodological perspectives. British Journal of Criminology, 43(3), 600–614.
Ganster, D. C., & Victor, B. (1988). The impact of social support on mental and physical health. British Journal of Medical Psychology, 61, 17–36.
Goldstein, H. (2003). Multilevel statistical models (3rd ed.). London: Edward Arnold.
Hale, C. (1996). Fear of crime: a review of the literature. International Review of Victimology, 4(2), 79–150.
Hamano, T., Fujisawa, Y., Ishida, Y., Subramanian, S. V., Kawachi, I., & Shiwaku, K. (2010). Social capital and mental health in Japan: a multilevel analysis. Plos One, 5(10).
Hardyns, W. (2012). Social cohesion and fear of crime in the Flemish region. Looking back on the results and a preview of additional research. In P. Ponsaers (Ed.), Social analysis of security. Financial, economic and ecological crime, crime (in)security and (dis)trust, public and private policing (pp. 167–202). The Hague: Eleven International Publishing.
Harpham, T. (2008). The measurement of community social capital through surveys. In I. Kawachi, S. V. Subramanian, & D. Kim (Eds.), Social capital and health (pp. 51–62). New York: Springer.
Hays, R. D., Sherbourne, C. D., & Mazel, R. M. (1995). User’s manual for the Medical Outcomes Study (MOS) core measures of health-related quality of life. Santa Monica: RAND.
Hox, J. J. (2010). Multilevel analysis: techniques and applications. New York: Routlegde.
Innes, M. (2004). Signal crimes and signal disorders: notes on deviance as communicative action. British Journal of Sociology, 55(3), 335–355.
Kawachi, I., & Berkman, L. F. (Eds.). (2003). Neighborhoods and health. New York: Oxford University Press.
Kawachi, I., Kim, D., Coutts, A., & Subramanian, S. V. (2004). Health by association? Social capital, social theory, and the political economy of public health - commentary: reconciling the three accounts of social capital. International Journal of Epidemiology, 33(4), 682–690.
Kawachi, I., Subramanian, S. V., & Kim, D. (2008). Social capital and health: a decade of progress and beyond. In I. Kawachi, S. V. Subramanian, & D. Kim (Eds.), Social capital and health (pp. 1–26). New York: Springer Science.
Kelling, G. L., & Coles, C. M. (1996). Fixing broken windows. Restoring order and reducing crime in our communities. New York: Free Press.
Kim, D., Baum, C. F., Ganz, M. L., Subramanian, S. V., & Kawachi, I. (2011). The contextual effects of social capital on health: a cross-national instrumental variable analysis. Social Science and Medicine, 73(12), 1689–1697.
Kuyken, W., Orley, J., Power, M., Herrman, H., Schofield, H., Murphy, B., & Vandam, F. (1995). The World-Health-Organization Quality-of-Life Assessment (Whoqol) - Position paper from the World-Health-Organization. Social Science and Medicine, 41(10), 1403–1409.
Layard, P. R. G., & Layard, R. (2011). Happiness: lessons from a new science. UK: Penguin.
Lin, N. (1999). Building a network theory of social capital. Connection, 22, 28–51.
Lindstrom, M., Merlo, J., & Ostergren, P. O. (2002). Individual and neighbourhood determinants of social participation and social capital: a multilevel analysis of the city of Malmo, Sweden. Social Science and Medicine, 54(12), 1779–1791.
Macinko, J., & Starfield, B. (2001). The utility of social capital in research on health determinants. The Milbank Quarterly, 79(3), 387–427.
Makarios, M. D., & Livelsberger, T. (2013). Social Support and Crime. In F. T. Cullen & P. Wilcox (Eds.), The Oxford Handbook on Criminological Theory. Oxford:Oxford University Press.
McKenzie, K., & Harpham, T. (2006). Social capital and mental health. London:J. K. Publishers Ed.
Möhnen, S. M., Völker, B., Flap, H., Subramanian, S. V., & Groenewegen, P. (2012). The influence of social capital on individual health - a consequense of neighborhood social capital or neighbor networks? In S. M. Möhnen (Ed.), Neighborhood context and health: how neighborhood social capital affects individual health. Utrecht: Utrecht University.
Oberwittler, D., & Wikström, P.-O. H. (2009). Why small is better. Advancing the study of the role of behavioral contexts in crime causation. In G. N. J. Bruinsma, D. Weisburd, & W. Bernasco (Eds.), Putting crime in its place. Units of analysis in geographic criminology (pp. 33–58). New York: Springer.
Park, R. E. (1915). The city: suggestions for the investigation of behavior in the city environment. American Journal of Sociology, 20, 579–583.
Pauwels, L., & Hardyns, W. (2009). Measuring community (Dis)organizational processes through key informant analysis. European Journal of Criminology, 6(5), 401–417.
Pauwels, L., & Hardyns, W. (2010). Does it really have to be ‘an urban village’? A multilevel analysis of fear of crime. In L. Pauwels, W. Hardyns, & M. Van de Velde (Eds.), Social disorganisation, offending, fear and victimisation. Findings from Belgian studies on the urban context of crime (pp. 177–197). Den Haag: Boom Juridische Uitgevers.
Poortinga, W. (2006). Social capital: an individual or collective resource for health? Social Science and Medicine, 62(2), 292–302.
Putnam, R. D. (1993). Making democracy work: civic traditions in modern Italy. Princeton: Princeton University Press.
Reisig, M. D., & Cancino, J. M. (2004). Incivilities in nonmetropolitan communities: the effects of structural constraints, social conditions, and crime. Journal of Criminal Justice, 32(1), 15–29.
Ross, C. E., & Mirowsky, J. (2001). Neighborhood disadvantage, disorder, and health. Journal of Health and Social Behavior, 42(3), 258–276.
Ross, C. E., & Mirowsky, J. (2009). Neighborhood disorder, subjective alienation, and distress. Journal of Health and Social Behavior, 50(1), 49–64.
Sacco, V. F. (1993). Social support and the fear of crime. Canadian Journal of Criminology, 35(2), 187–196.
Sampson, R. J. (2003). The neighborhood context of well-being. Perspectives in Biology and Medicine, 46(3), S53–S64.
Sampson, R. J. (2012). Great American city. Chicago and the enduring neighborhood effect. Chicago: University of Chicago Press.
Sampson, R. J., & Groves, W. B. (1989). Community structure and crime - testing social-disorganization theory. American Journal of Sociology, 94(4), 774–802.
Sampson, R. J., Raudenbush, S. W., & Earls, F. (1997). Neighborhoods and violent crime: a multilevel study of collective efficacy. Science, 277(5328), 918–924.
Shaw, C., & Mckay, H. (1942). Juvenile delinquency and urban areas. Chicago: University of Chicago Press.
Sherbourne, C. D., & Stewart, A. L. (1991). The mos social support survey. Social Science and Medicine, 32(6), 705–714.
Skogan, W. G. (1990). Disorder and decline. New York: The Free Press.
Stafford, M., Duke-Williams, O., & Shelton, N. (2008). Small area inequalities in health: are we underestimating them? Social Science and Medicine, 67(6), 891–899.
Subramanian, S. V., Lochner, K. A., & Kawachi, I. (2003). Neighborhood differences in social capital: a compositional artifact or a contextual construct? Health & Place, 9(1), 33–44. doi:10.1016/S1353-8292(02)00028-X.
Thoits, P. A. (1985). Social support processes and psychological wellbeing theoretical possibilities. In I. G. Sarason & B. R. Sarason (Eds.), Social support theory, research and applications (pp. 51–72). The Hague: Martinus Nijhof.
Thoits, P. A. (1995). Stress, Coping, and Social Support Processes - Where Are We - What Next. Journal of Health and Social Behavior, 35, 53–79.
Thoits, P. A. (2011). Mechanisms linking social ties and support to physical and mental health. Journal of Health and Social Behavior, 52(2), 145–161.
Ware, J. E., & Sherbourne, C. D. (1992). The mos 36-item short-form health survey (Sf-36).1. Conceptual-framework and item selection. Medical Care, 30(6), 473–483.
Webb, D., & Herrera, E. W. (2012). Subjective well-being and security (Vol. 46). New York:Springer.
Weisburd, D., Bernasco, W., & Bruinsma, G. (2009). Putting crime in its place: units of analysis in geographic criminology. New York: Springer.
Wilson, J. Q., & Kelling, G. L. (1982). Broken windows: the police and neighborhood safety. Atlantic Monthly, 249, 29–38.
Wirth, L. (1938). Urbanism as a way of life. The American Journal of Sociology, 44(1), 1–24.
Wright, J. P., & Cullen, F. T. (2001). Parental efficacy and delinquent behavior: do control and support matter? Criminology, 39(3), 677–705.
Zhang, L. N., Messner, S. F., Liu, J. H., & Zhuo, Y. A. (2009). Guanxi and fear of crime in contemporary urban China. British Journal of Criminology, 49(4), 472–490.
Acknowledgments
The entire research team wishes to express its sincere gratitude for the financial support provided by the Research Foundation - Flanders (FWO). Furthermore the research team wishes to thank the city of Ghent for their help in facilitating this research project.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Hardyns, W., Vyncke, V., De Boeck, A. et al. Are Collective Efficacy, Disorder and Social Support Associated with One’s Quality of Life? Evidence from the Multilevel SWING Study in Belgium. Applied Research Quality Life 11, 739–756 (2016). https://doi.org/10.1007/s11482-015-9393-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11482-015-9393-z