
Abstract
The aim of this study is to investigate the correlates of self-reported health (SRH) among older adults in Malaysia and Singapore. The study uses data collected in the Global Ageing Study (GLAS) 2007, one of the largest surveys of its kind, specially designed to investigate attitudes towards later life, ageing and retirement. Data were collected from 1002 and 1004 respondents from Malaysia and Singapore respectively. The study found that Singaporeans report a healthier life than Malaysians. The two countries have consistent results with regard to the influences of selected covariates on individual health. Poorer health is more prevalent among people with lower education, among those widowed, divorced or separated, and those working in blue-collar occupations. Although social support is found to be an important determinant of SRH, the effects are partially confounded with other covariates. These findings enhance our knowledge about the health status of older people, and in turn will be useful for governments to ensure effective policy making.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
This paper examines factors associated with older people’s health status in two Asian economies: Singapore and Malaysia. Cross comparative research in the Asian region is worthwhile as, according to a recent report of ADB (2007) there is a huge disparity in real per capita GDP in the developing Asia-Pacific region. Singapore ranks among the top five regional economies while Malaysia is considered middle-ranking. Socio-economic and demographic forces are key correlates of health status in old age (see for example, Smith and Kington 1997; Cai and Kalb 2006; Alam and Karim 2006; Cutler et al. 2008; Kalwij and Vermeulen 2008; Kagamimori et al. 2009; Khan and Raeside 2014). The elderly in poorer countries will suffer more due to the decline in social and familial support (Rahman et al. 2004; Khan and Leeson 2006; Khan 2014). The family has been the main provider of support for older people in many parts of Asia but changing norms, migration, and smaller family sizes have perhaps contributed to the decreasing social support provided to older parents (Chan et al. 2006; Alam and Karim 2006; Khan 2014).
Populations are ageing both in Singapore and Malaysia. However, the speed of ageing populations is faster in the former (UN 2013) due to swift improvements in education, housing and health (WHO 2007a, b). In Singapore about 80 % of primary health care services are provided by private practitioners while the rest is provided by the state. At the government polyclinics, Singapore citizens aged 65 and above are given special subsidies of up to 75 % on their consultation and treatment fees. Healthcare in Singapore is predominantly a user pays system, with people who can afford to pay more for better healthcare from the private sector. Healthcare is financed through a national savings scheme known as Medisave, which is strongly regulated by the government, with limits on the amount of money which can be withdrawn at any one time.
In Malaysia, there have been gradual improvements in morbidity and mortality, and life expectancy has increased dramatically over the last 20 years. Despite positive change in demographic and socioeconomics, both communicable and non-communicable diseases remain a burden in Malaysia (WHO 2007b). Health care is currently provided by the public and private sectors, as well as by nongovernmental organizations in Malaysia.
Despite increased access to primary health in recent years, there are large health inequalities amongst older Malaysians particularly with regard to social class, ethnicity and rural–urban place of residence. Wu and Rudkin (2000) found that low socioeconomic status is associated with poorer health for all three ethnic groups – Malay, Chinese, and Indian, and family, household structure and kinship patterns vary across the three main ethnic groups. The Malay kinship system is generally bilateral, with some areas adhering to a matrilineal system in patterns of post-marital residence and inheritance. In contrast, the Chinese adhere to a patrilineal system in which, similar to Indian families, extended families are the ideal. Social contact is also important for positive health outcomes. Co-residence with any family member matters to the wellbeing of elderly (Wu and Rudkin 2000; Al-Kandari and Crews 2014). Children who co-reside with or live near ageing parents are able to provide a range of supportive services, including transfers of money and material goods, assistance with household chores, personal care, and companionship (Wu and Rudkin 2000; Khan 2014). Social support and health are found to be closely related and become an increasing important area of research in gerontology and social policy (Thanakwang and Soonthorndhada 2011; Khan 2014). Su and Ferraro (1997) reported that social integration with family and friends have direct positive effects on the subjective health assessments of older Malaysians, even after controlling for the negative effects of diminished functional health.
There is a fair amount of literature on health inequalities that deal with socioeconomic status and these inequalities are expressed in a variety of health outcomes, including subjective measure of self-reported health, and the extent of chronic disease morbidity and mortality (e.g., Jarallah and Al-Shammari 1999; Wu and Rudkin 2000; Rahman et al. 2004; Chan et al. 2006; Fong et al. 2007). Other studies in Asia highlight the subject of physical, mental, social and environmental health status within the population and individuals’ self-reported health perception (see for example, Jarallah and Al-Shammari 1999; Chan et al. 2006).
Perceptions of healthcare are complex and subjective and can be affected by several social, cultural, psychological and economic factors (Jarallah and Al-Shammari 1999). Self-perception of an individual about her/his health has been found to be a major component in life satisfaction among older persons (Zautra and Hempel 1984; Benyamini et al. 2003). People who rated their health higher were more likely to assign high ratings as an indication of good physical and psychological health (Benyamini et al. 2003). An SRH indicator, whereby respondents are asked to classify their current health status on a hierarchical scale e.g., excellent, good, fair, poor, has proven valuable measure (Kuhn et al. 2004). Multiple studies have demonstrated that SRH is a good predictor of mortality and functional ability even after some variables controlled for (Appels et al. 1996; Idler and Benyamini 1997). Very few SRH studies have been undertaken in developing countries (Zimmer et al. 2000), and none between two tiger economies. In many settings the ‘fair health’ category in all likelihood is comprised of a substantial proportion of people in good health. Kuhn et al. (2004) combined the ‘fair’ and ‘good’ categories for data in Bangladesh to make a sharp distinction with poor health (Kuhn et al. 2004). Wu and Rudkin (2000) considered a similar health category. A few exceptions on the selection of health category can be seen in the literature where ‘fair’ and ‘good’ are combined and eventually considered to be the good health category because of socio-cultural beliefs and practices (see for example, Wu and Rudkin 2000; Rahman and Barsky 2003).
Marital status may be associated with longer duration of survival in old age, however, the effect of marital status on SRH was found to be insignificant in a British study (Arber and Cooper 1999). It is possible that the situation in the developing world might be different. Given the context of poor countries, there are few alternatives to family support for older people, and kin ties might have a substantial impact on health and survival in old age (Rahman 1999; Wu and Rudkin 2000). For Malaysia, Wu and Rudkin (2000) showed that the impacts of marital status on health varied by ethnicity - from no impact at all in the case of Indians, to a consistent impact among the Chinese, regardless of the frequency or presence of daily contact with children. On the other hand, a substantial effect is seen to be among Malays whereby spouses were associated with improved health only in the absence of daily contacts with children. This implies that it is not marital status per se that has a positive effect on wellbeing, but regular contact with loved ones.
The purpose of this study is twofold: first, to give an overview of current health status in Malaysia and Singapore within a global perspective; and second, to identify the important factors associated with SRH among older adults in both countries.
Data and Methods
The Data Set
The study utilizes data collected in the study of “The Global Ageing Survey” (GLAS), a global cross-sectional ageing survey conducted in 21 countries and territories in 2007 under the auspices of the Oxford Institute of Population Ageing, the University of Oxford and the HSBC Bank Ltd, UK. One of the principal objectives of the survey has been to investigate people’s attitudes towards health and retirement and to draw general conclusions for the wellbeing of elderly. In Singapore, 1004 responses of people 40 to 79 were gathered, and in Malaysia, the total was 1002. The interviews were mostly conducted by telephone and on some occasions by face-to-face. Individuals were drawn from various social classes with proportional representation of age and sex. The questionnaires contained a wide range of questions about their attitudes and perceptions to employment and retirement in addition to health questions and activities of daily living (ADL) where it indicates the ability to perform various physical, personal and cognitive activities.
Statistical Methods
The data have been compiled and analysed using software IBM SPSS. Descriptive data analysis was carried out to understand the selected characteristics of respondents in addition to the frequency analysis of variables for the selected subcategories. Bivariate analysis was performed to compare the difference in the perception of health for the subgroups of selected variables and the significance of difference was measured by the Chi-square tests. In addition, correlation analysis was undertaken to examine the strength of relationship between variables and a t-test used to check the statistical significance. Finally, a multivariate logistic regression model was used to explore the factors affecting SRH status among older adults in both Malaysia and Singapore after controlling for various predictors.
The general form of a logistic regression is:
Where p = Prob(Y = 1) is the probability that an individual reports poor health condition, β 0 is the intercept parameter, β i is the regression coefficients of the ith variable in the model. The fundamental equation for logistic regression tells us that with all other variables held constant, there is a constant increase of slope in logit(p) for every 1-unit increase in independent variable, and so on. They are the maximum likelihood estimates after transforming the dependent into a logit variable (the natural log of the odds of the dependent occurring or not) and can be tested by the Wald statistic which follows χ 2 distribution with 1° of freedom. It permits one to test the null hypothesis in the logistic regression that a particular coefficient is zero. The main interpretation of logistic regression results is to find the significant predictors of dependent variable. The odds ratios (OR) are computed by \( \exp \left(\widehat{\beta}\right) \) which explains the effect of a particular variable compared to their corresponding reference group. The significance of covariates is indicated by the odds ratios (OR) as well as its 95 % confidence intervals (95 %CI). The odds ratios are usually used to quantify the effect of significant independent variables on the dependent variable. The overall fitness of the logistic regression model was assessed by examining the distribution of log-likelihood ratio (−2logL) and χ 2 test of significance. A detailed discussion on logistic regression and its application can be found elsewhere (see for example, Hosmer and Lemeshow 2000; Khan and Raeside 1997; Khan 2014).
Variables Used in the Analysis
The description of the selected variables that used for the study is depicted in Table 1. The self-reported health (SRH) of respondent being used as a dependent variable in this study. During the interview, respondents were asked about their perception of health status and a question was How is your health in general? In order to record and compare the health situation of older adults across selected countries, responses are categorised in a five point ordered categorical scale as very good, good, fair, poor, and very poor. The higher the numerical value, the poorer is the respondent’s overall health situation. For the purpose of analysis we then consider dichotomous groups by merging ‘very good’ and ‘good’ into one group and all remaining responses into another group on the assumption that each group behaves more or less similar fashion and is considered to be homogeneous. Furthermore, categories ‘fair’, ‘poor’, and ‘very poor’ were merged as having poor health. The causes of the poor health will be explored in the present paper. Benyamini et al. (1999, 2003) also considered same groups for their studies.
Based on the above literature review, we selected various independent variables: age, gender, marital status, household size, education, employment status, received financial support, provided financial support, received help and care, provided help and care, geographical region, difficulties with movement or a set of physical difficulties (ADL-1), a set of personal difficulties (ADL-2), and memory problem or cognitive dysfunction (ADL-3). Respondents are regarded as disabled if they responded positively to having difficulties of one or more Activities of Daily Living (ADL). Individuals who scored a 0 were considered to have ADL limitations.
The selected independent variables outline above will be examined to understand how they are related to the SRH. We have performed some systematic analysis: first by exploratory data analysis, then by bivariate, and finally by multivariate analysis. These analyses will help to isolate the influence of selected variables on SRH among older adults in both countries.
Results and Discussion
Exploratory Data Analysis
The definition, measurement and classification of selected variables are illustrated in Table 1. An exploratory statistical analysis has been performed and some are briefly discussed here (results are not shown in Table 1). In both countries the mean age of respondents is estimated to be around 59 years. The ratios of males to females are almost half and equal in both the countries. A higher proportion of larger household size is found in Malaysia than in Singapore. In Singapore, the average educational level of attainment is much higher than Malaysia. In Malaysia, relatively more people received financial as well as help and care supports. On the contrary, in Singapore more people provide financial help and care supports to relatives, friends and neighbours. Higher proportions of older adults have contact with their children in Malaysia than in Singapore. Compared to Singapore, in Malaysia, more people face difficulties with ADLs such as getting up from chair or walking. SRH was analysed in the present study in which a basic statistical analysis was performed for four age cohorts 40–49 years, 50–59 years, 60–69 years and 70–79 years. Across-cohort comparison of self-reported health has then been made between Malaysia and Singapore. It was found that more Malaysians reported being in poor health than Singaporeans (39.5 % versus 30.5 %, p < 0.000). These results are expected. Moreover, they are also consistent to earlier findings.
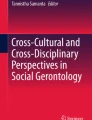
The distribution of SRH outcomes among elderly in both Singapore and Malaysia are displayed in Fig. 1. As might be expected, the younger the respondent the better their overall self-reported heath. The coefficient of correlation is found to be much higher for Malaysians (r = 0.511, p < 0.001) than for Singaporeans (r = 0.319, p < 0.001), and they are statistically significant. (The result is not shown as a tabular form and may be made available from authors upon request). The significance of association may reflect the inherent picture of health care delivery systems of the two countries. From Fig. 1, we also see a similar pattern of correlation when SRH is divided by age cohort. It has been revealed that irrespective of the country, the proportion of respondents reporting very good health is declining with age. On the other hand, the proportion of respondents reporting fair or worse health is increasing steadily (Results illustrated before merging). This general trend helps us to confirm an existing hypothesis that an individual’s health situation is closely related with chronological age. This study also finds that that the response varies across the selected age cohorts. As can be seen from Fig. 1, for the younger cohorts, 40–59 years, a large proportion of respondents reported having good health followed by very good health. On the other hand, while considering the oldest cohort (70–79 years) we see the completely opposite picture. From this result, one can conclude that Singaporean elderly are generally healthier than those of Malaysians. This is an expected finding which helps to understand the overall health situation in Singapore and Malaysia. In turn, this depends on necessary improvement of socio-economic and demographic factors, primary health care and service delivery, cultural context and the political paradigm of the country. Thus, it would be ideal to explore some of these factors to understand their influence on SRH of an individual.

Distribution of self-reported health conditions among older adults in Malaysia and Singapore
Bivariate Analysis
The bivariate relationships between the characteristics of the older adults and incidence of poorer health outcome are shown in Tables 2 to 3. Table 2 shows a picture of how health reporting varies with regard to various characteristics of respondents in both countries. A conventional statistical method, chi-square is used to test the significant difference among various subgroups of variables. It can be seen from Table 2 that the overall health situation decreases with the increase of age and a significant difference exists among the selected age cohorts. This is not only a consistent finding for Malaysia and Singapore but also at the regional and global levels. This finding confirms the theoretical notion of physical decline in human health as individual’s age.
There is no significant gender difference between the two countries in terms of possessing poorer health. In contrast, however, gender differences in health were found to be significant for regional as well as global level data. This will be investigated further in multivariate analysis.
Marital status is found to be an important factor for determining health condition. A higher proportion of older widowed, divorced and separated individuals reported to have poor health not only in Malaysia and Singapore but across the globe. In other words, poor health is more prevalent among elderly who are widowed, divorced or separated irrespective of geographical location. In Malaysia the lowest proportion of people reported to have poor health is amongst those who are married and have a long term partner, whereas in Singapore those who have never married comprise the smallest proportion of those reporting poor health.
While exploring the effect of education, we see that there is a significant variation in reporting poor health across the selected hierarchical occupational groups. Our analysis shows that the lowest proportion of respondents reporting poor health were among white collar occupations. The highest proportion of individuals reporting poor health was unemployed. This can be explained by the fact that unemployed people are often considered to be less educated and therefore are socially depressed.
Our analysis reveals that a higher proportion of people who suffer from poor health received financial help from friends or relatives and a lower proportion of older adults reporting poor health provide financial support. These findings help us to confirm the fact that by and large the intergenerational contact with respect to financial flow is associated with poor health of older persons.
Physical inactivity has been associated with lower socioeconomic status (Fong et al. 2007). Older adults are likely to report that disability is a barrier to improving their healthiness and wellbeing (Rowe and Kahn 1987; Newsom et al. 2004). As expected, our analysis shows that poor health is associated with receiving more help and care supports from friends or relatives. In Malaysia, the positive response rate is found to be 55.5 % against 31.4 % of individuals who have never received such assistance, whilst in Singapore, the response rate was 38.5 % against 28.8 % of people who never received any help or care. On the other hand, a lower proportion of respondents with poor health outcomes have provided help and care to friends or relatives. For example, in Malaysia about 27.0 % respondents have ever provided support compared with 41.7 % who have never done so, and in Singapore it was 21.4 % ever provided versus 33.7 % never provided support. This tendency to provide support is also supported by findings from Asia and global dataset (see Table 2).
This study also examined various selected activities of daily life and how they are related to the poor health of older adults both in Malaysia and Singapore. The findings are then compared with the evidence available at the regional and global levels. As can be seen from Table 3, a vast majority of older Malaysians than Singaporeans reported to have poor health as having difficulties with daily living activities such as getting up from a chair, walking 100 m, climbing stairs, lifting heavy objects, dressing, bathing, eating, getting in or out of bed, preparing a meal, doing work around the house/yard/garden and, remembering things. These finding are concomitant with the findings at the regional and global levels. In Singapore, some of the values of chi-square that are seen insignificant for dressing, bathing and eating may be attributable to the non-response. Therefore, one can conclude that poor SRH may be associated with what difficulties one would usually face in daily living.
Multivariate Logistic Regression Analysis
To identify the net effect of selected variables we also performed multivariate logistic regression analysis controlling for various characteristics such as age, gender, employment status and activities of daily living and the results of logistic regression for Malaysia and Singapore are presented in Table 4. Two models were developed for each country’s data. Age is found to be the single most important factor influencing SRH of individual in both countries after controlling for all the other selected variables in the analysis. This provides strong evidence of a biological functional decline as we age. It can be seen from Table 4 that the adjusted odds ratios (OR) for 50–59 years compared to 60–69 years Malaysian cohort ranged from 1.487 (95 %CI 0.868–2.547) to 2.668 (95 %CI 1.515–4.700). The effect is found to be the highest among the oldest age group 70–79 in Malaysia in which the risk of reporting poor health is seen to be almost five times higher compared to youngest cohort 40–49 (adjusted OR = 4.739, 95 %CI 2.518–8.921). Although Singapore follows a similar pattern, its age effect is much lower than that of Malaysia. For example, for age cohort 70–79 years, the risk of reporting poor health is observed to be 2.5 times in Singapore, while it is 4.7 times in Malaysia. What this indicates is that older Singaporean adults are perceived healthier than their Malaysian counterparts. This finding is consistent with what one would expect given the socioeconomic development of the two countries.
The effect of gender on SRH status is examined after controlling for all remaining variables. Although females are found to have a lower chance of reporting poor health, the effect appears to be insignificant for either country. Thus, it can be concluded that there is no significant gender difference in reporting poor health status in Malaysia and Singapore. Past literature shows that marital status is very important for health and longevity. This study also examined marital status and whether or not it has any causality with SRH. Our analysis reveals that those who are married and maintaining a long term relationship are found to be less likely to report poor health in Malaysia than those never married, controlling for all other variables in the model. On the other hand, marital status has no significant impact on SRH among older adults in Singapore. Further investigation is required to explain this finding.
Household size appeared to have no significant influence on reporting poor health status while controlling for other factors in multivariate models. On the other hand, education has an inverse effect on poor health reporting in both Malaysia and Singapore i.e., in general the higher the level of educational attainment, the lower is the reporting of poor health status of individuals. It can be seen from Table 4 that in Malaysia reporting of poor health was found to be 0.840 times (16.0 %) lower for secondary educated and 0.236 times (76.4 %) lower for tertiary or higher levels of educated older adults compared to those educated to primary school level primary. Table 4 also indicates that the odds of reporting poor health decrease by 76.4 % for one unit increase in tertiary and higher education, and are found to be statistically significant. This implies that Malaysians who possess tertiary or higher education have a lower chance of reporting poor health. A similar pattern can also be seen in our analysis for Singapore; however, the hierarchy in educational effect is found to be statistically insignificant.
In the paper, unemployment is found to be an important factor for both the countries as compared to other occupational categories. In other words, those who are unemployed have a 2.495 times (95 %CI, 1.148–5.422) and 1.755 times (95 %CI, 1.006–3.061) higher chance of reporting poor health condition than those who belong to white collar occupations in Malaysia and Singapore respectively. This indicates a common message that a poorer health outcome is associated with lower occupational status. This can be explained further by the fact that higher educated people usually engage in white collar jobs and report better health. This is not an unexpected finding and may not necessarily be contradict with the previous finding.
It can be seen from Table 4 that receiving financial support from friends or relatives has influence with opposite direction for Malaysia and Singapore. However, some of these effects are seen to be statistically significant. On the other hand, in both Malaysia and Singapore, those who provided financial support are less likely to report poorer health status. This is expected as healthier people across the countries can able to extend financial support to others. In other words, wealthier people are relatively more healthy and financially well-off and therefore be able to provide financial support to others.
Our analysis shows that in Malaysia, those who received help and care supports are seen to report poor health status than those who do not. On the other hand, in Singapore, those who provided help and care support to others (friends or relatives) are found to be 43.7 % less likely to report poorer health (adjusted OR = 0.563, 95 %CI: 0.370–0.856). This is an expected finding and is concomitant with what we see in the literature for developed countries. Although Malaysia has a similar tendency, results are only found to be significant for Singapore. Perhaps this provides a strong message that helping others may keep individuals in better health by many ways physically, mentally and socially.
Evidence suggests that many older persons are seen to be inactive despite efforts to promote the benefits of regular physical activity (Centre for Disease Control 2007). The presence of difficulties (physical disability or ADL-I) is an important risk factor for explaining health conditions both in Malaysia and Singapore. This means that the higher the frailty the higher is their chance of an individual reporting poor health. This is an expected finding. On the other hand, the presence of personal disability or ADL-II renders older adults 1.737 times (with 95 %CI: 0.954–3.162) more likely to report poor health in Malaysia whereas the risk seen to be 1.884 times (95 %CI: 1.164–3.051) higher than reference group in Singapore. These findings carry a consistent but important message that disability is the major threat to the older adult’s health situation even after controlling for other factors in the models. Memory lapse is used as a crude measure of cognitive disorder among older adults and it can be seen from Table 4 that presence of difficulties with remembering has a strong influence on reporting poor health and the odds ratios are significant for Singapore (adjusted OR = 1.497, 95 %CI: 1.024–2.190). This indicates that cognitive impairment directly affects health of older persons. Thus to enhance the quality of life we need better understanding of the factors that increase the risk of developing cognitive impairment.
Conclusion
The principal aim of this study has been to identify key determinants of SRH among older adults in both Malaysia and Singapore and to make a cross country comparison. This study uses data collected in the Global Ageing Survey 2007 which is as yet, the world’s biggest global ageing survey of its kind. This study has benefited from using some of the most important variables from such a recent global ageing survey. We then performed a variety of analytical techniques, exploratory, bivariate and multivariate statistical analyses, to tease out key determinants of reporting poor health in old age between the two countries. The present study generally elucidates health inequality among older adults primarily with regard to the reporting of subjective health (self- reported) is mainly dependent on numerous characteristics of individuals. Our analysis provides interesting findings on SRH which have practical implications for public health policy formulation.
Biological age is found to have a positive influence on reporting poor health in both countries which means that the higher the age the higher proportion of reporting poor health. However, social support would make a difference in the SRH of older people and the presence of a spouse and family members could also mean more social support. Better financial preparedness and access to better health care services may have improved the health status of older adults and this is supported in our analysis by the fact that Singaporeans are less likely to report poor health compared to Malaysians.
Poor health was assumed to be higher among socially disadvantaged elderly groups. such as people with poor reading and numeracy skills, or those who are economically inactive due to disabilities, − an assumption supported by the findings of this study. For example, poor health is reported to be the highest among elderly who are widowed, divorced and separated. Education has a huge impact on health perception and it is found in our study that the possession of poor health is associated with lower education. Therefore, the lower (than Malaysia) reporting of poor health among older Singaporean adults was attributed to their higher level of education. On the other hand, unemployment increases the risk of reporting poor health in both countries. Thus, it may be concluded that lower levels of education and unemployment are associated with a higher risk of reporting poor health among older adults in Malaysia and Singapore. It can also be seen from earlier studies that education is negatively related to the risk of the onset of functional limitations (Zimmer et al. 1998), and mortality (Liu et al. 1998).
This study has examined the association between intergenerational support and health status of older adults. It suggests that in Singapore and Malaysia those who received financial support from friends or relatives were highly likely to report poor health. On the other hand, those who provide financial supports to others are less likely to report poor health. Moreover, in Singapore those who provide help and care reported being healthier than their counterparts in Malaysia. These are all expected findings and are consistent with results of Khan (2014).
Our analyses help us to understand certain intergenerational issues of these two countries. First, there exists an intergenerational solidarity between generations despite rapid changes in social transformation. Secondly, intergenerational support is gradually weakening with the passage of time. In Singapore, this has been recognised by the government – hence the Maintenance of Parents Act, and incentives for HDB housing (public housing in Singapore is managed by the Housing and Development Board) given to those who live with/close to parents etc. Finally, both countries are sharing almost similar cultural as well as Asian values.
Disability in old age is an important topic in an ageing society. As mentioned earlier,poor health across the globe may be associated with reduction in the physical as well as psychological condition in old age. Investigation of selected activities of daily life reveals how they are associated with poor health reporting in Singapore and Malaysia. Our analysis shows that a vast majority of older Malaysians than Singaporeans reported poor health as having difficulties with daily living activities. This study suggests that cognitive impairment directly influences SRH in both Singapore and Malaysia. Therefore, governments should improve health care facilities for older adults particularly with regard to social care including personal help and domiciliary care provisions. Social workers have been doing numerous activities for elderly care in both countries, for example, a voluntary welfare organisation (VWO) in Singapore and NGOs and charitable organisations in Malaysia. Improving social care services can in turn help build confidence in the health of older adults. Non-governmental organisations, civil society and community based voluntary organisations can also play important role by enhancing awareness and implementing new projects in collaboration with the government.
While the validity and reliability have been checked, no significance bias or inconsistencies have been found in the dataset. However, one cannot rule out that no limitation exists as to how to collate the data and particularly on the accuracy of self-reported health data. Despite limitations, we claim that our results will help the governments in understanding the general health aspiration of their older adults and will benefit for taking proper policy implications. It is evident that neither governments well prepared at the policy level to meet the challenges in an ageing society. Therefore, more research is required to understand health aspiration particularly on preventive and social medicine rather than curative side. Special emphasis is needed to explore the prevalence of communicable as well as non-communicable diseases, as well as providing services for disability and long term care. The government social support system is required to address the need of older adults and perhaps the NGOs can also play an important role in providing support for elderly in the community.
According to Rowe and Kahn (1987), societies need a long term research-based strategies either to delay or to prevent common diseases in old age. Therefore, health strategy and planning are essential for governments in which other organisations, particularly the non-governmental organisations, have a role to play in helping to improve the health and well-being of the older population and reducing health inequalities. Thus, one can argue that more research is needed on health awareness, individual’s health management and health related quality of life.
Finally, this study describes a comparative health situation between two neighbouring South-East Asian countries - Malaysia and Singapore - and our findings elucidate how the selected variables influence the SRH among their older adults. Since both countries share a similar culture and gain practical lessons from each other, it is anticipated that the finding of the study will help policy-makers not only in understanding health situations but also to predict the future health of older adults of these countries as a whole.
One of the main limitations of the study is that the survey considers population aged between 40 and 79 years. Given that Singapore’s life expectancy is currently 82 years the study is unable to capture a fuller picture of an ageing population who are 60 years and above.
References
ADB. (2007). Purchasing power parities and real expenditures. Manila: Economics and Research Department, Asian Development Bank.
Alam, M., & Karim, M. (2006). Changing demographics, emerging risks of economic-demographic mismatch and vulnerabilities faced by older persons in south Asia: situation review in India and Pakistan. Asia-Pacific Population Journal, 21(3), 63–92.
Al-Kandari, Y., & Crews, D. (2014). Social support and health among elderly Kuwaitis. Journal of Biosocial Science, 46, 518–530.
Appels, A., Bosma, H., Grabauskas, V., Gostautas, A., & Sturmans, F. (1996). Self-rated health and mortality in a Lithuanian and a Dutch population. Social Science and Medicine, 42(5), 681–690.
Arber, S., & Cooper, H. (1999). Gender differences in health in later life: the new paradox? Social Science and Medicine, 48(1), 61–76.
Benyamini, Y., Leventhal, H., & Leventhal, E. A. (1999). Self-assessments of health: what do people know that predicts their mortality? Research on Ageing, 21(3), 477–500.
Benyamini, Y., Leventhal, E. A., & Leventhal, H. (2003). Elderly people’s ratings of the importance of health-related factors to their self-assessments of health. Social Science and Medicine, 56(8), 1661–1667.
Cai, L., & Kalb, G. (2006). Health status and labour force participation: evidence from Australia. Health Economics, 15(3), 241–261.
Centre for Disease Control (2007). The State of Aging and Health in America 2007.Available athttp://www.cdc.gov/aging/pdf/saha_2007.pdf. Accessed on 23 January 2015.
Chan, A., Pin, N. T., & Niti, M. (2006). The determinants of self-rated mental health among older adults in Singapore. Hallym International Journal of Ageing, 8(1), 65–81.
Cutler, D. M., Lleras-Muney, A. & Vogl, T. (2008). Socioeconomic Status and Health: Dimensions and Mechanisms. NBER Working Paper No. 14333 Issued in September, Washington DC: National Bureau of Economic Research.
Fong, C. W., Bhalla, V., Heng, D., Chua, A. V., Chan, M. L., & Chew, S. K. (2007). Educational inequalities associated with health-related behaviours in the adult population of Singapore. Singapore Medical Journal, 48(12), 1091–99.
Hosmer, D. W., & Lemeshow, S. (2000). Applied logistic regression (2nd ed.). New York: Wiley.
Idler, E. L., & Benyamini, Y. (1997). Self-rated health and mortality: a review of twenty-seven community studies. Journal of Health and Social Behaviour, 38(1), 21–37.
Jarallah, J. S., & Al-Shammari, S. (1999). Factors associated with health perception of Saudi elderly. Journal of Cross-Cultural Gerontology, 14(4), 323–334.
Kagamimori, S., Gaina, A., & Nasermoaddeli, A. (2009). Socioeconomic status and health in the Japanese population. Social Science and Medicine, 68(12), 2152–2160.
Kalwij, A., & Vermeulen, F. (2008). Health and labour force participation of older people in Europe: what do objective health indicators add to the analysis? Health Economics, 17(4), 619–638.
Khan, H. T. A. (2014). Factors associated with intergenerational social support across the world. Aging International, 39(4), 289–326.
Khan, H. T. A., & Leeson, G. W. (2006). The demography of ageing in Bangladesh: a scenario analysis of the consequences. Hallym International Journal of Ageing, 8(4), 1–22.
Khan, H. T. A., & Raeside, R. (1997). Factors affecting the most recent fertility rates in urban–rural Bangladesh. Social Science and Medicine, 44(3), 279–289.
Khan, H. T. A., & Raeside, R. (2014). Between country variations in self-rated-health and associations with the quality of life of older people: evidence from the global ageing survey. Applied Research in Quality of Life, 9, 923–949.
Kuhn, R., Rahman, M. O., & Menken, J. (2004). Relating self-reported and objective health indicators to adult mortality in Bangladesh.. Boston: Population Association of America. IBS working paper p AC2004–0004.
Liu, X., Hermalin, A. I., & Chuang, Y. L. (1998). The effect of education on mortality among older Taiwanese and its pathways. Journal of Gerontology: Social Sciences, 53B(2), S71–S82.
Newsom, J. T., Kaplan, M. S., Huguet, N., & McFarland, B. H. (2004). Health behaviours in a representative sample of older Canadians: prevalence, reported change, motivation to change, and perceived barriers. Gerontologist, 44(2), 193–205.
Rahman, M. O. (1999). Family matters: the impact of kin on the mortality of the elderly in rural Bangladesh. Population Studies, 53(2), 227–235.
Rahman, M. O., & Barsky, A. J. (2003). Self-reported health among older Bangladeshis: how good is health indicator is it? The Gerontologist, 43(6), 856–863.
Rahman, M. O., Menken, J., & Kuhn, R. (2004). The impact of family members on the self-reported health of older men and women in a rural area of Bangladesh. Ageing and Society, 24(6), 903–920.
Rowe, J. W., & Kahn, R. L. (1987). Human ageing: usual and successful. Science, 237, 143–149.
Smith, J. P., & Kington, R. (1997). Demographic and economic correlates of health in old age. Demography, 34(1), 159–170.
Su, Y., & Ferraro, K. F. (1997). Social relations and health assessments among older people: do the effects of integration and social contributions vary cross-culturally? Journal of Gerontology: Social Sciences, 52B(1), S27–S36.
Thanakwang, K., & Soonthorndhada, K. (2011). Mechanisms by which social support networks influence healthy ageing among Thai community-dwelling elderly. Journal of Ageing and Health, 23, 1352–1378.
UN. (2013). World population prospects: the 2010 revision population database. New York: UN.
WHO (2007a). Malaysia: Health Situation. Regional office for the Western Pacific, World Health Organization. Available online at: http://www.who.int/nha/country/mys/en/. Accessed on 23 January 2015.
WHO (2007b). Singapore: Health Situation. Regional office for the Western Pacific, WorldHealth Organization. Available online at: http://www.who.int/nha/country/sgp/en/. Accessed on 23 January 2015.
Wu, Z. H., & Rudkin, L. (2000). Social contact, socioeconomic status, and the health status of older Malaysians. The Gerontologist, 40(2), 228–234.
Zautra, A., & Hempel, A. (1984). Subjective well-being and physical health: a narrative literature review with suggestions for future research. International Journal of Ageing and Human Development, 19(2), 95–110.
Zimmer, Z., Liu, X., Hermalin, A., & Chuang, Y. L. (1998). Educational attainment and transitions in functional status among older Taiwanese. Demography, 35(3), 361–75.
Zimmer, Z., Natividad, J., Lin, H., & Chayovan, N. (2000). A cross-national examination of the determinants of self-assessed health. Journal of Health and Social Behavior, 41(4), 465–481.
Acknowledgments
This research arises as a part of the strategic alliance between the Oxford Institute of Population Ageing and the HSBC Bank Plc for promoting the understanding of ageing issues across the globe. Authors gratefully acknowledge the help and research support were received from Dr. George Leeson at the Oxford Institute of Population Ageing, the University of Oxford in the UK.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Khan, H.T.A., Flynn, M. Self-Reported Health Status of Older Adults in Malaysia and Singapore: Evidence from the 2007 Global Ageing Survey. Applied Research Quality Life 11, 687–705 (2016). https://doi.org/10.1007/s11482-015-9390-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11482-015-9390-2