
Abstract
Overcrowding in emergency departments (ED) jeopardizes quality and access to health care, which represents a major issue for service delivery. This study determined predictors of frequent ED utilization among 320 patients recruited from six hospital ED in Quebec (Canada). Data collection included patient interviews and administrative databanks. A hierarchical linear regression analysis was performed using the Andersen Behavioral Model as a framework, with variables organized into predisposing, enabling, and needs factors. Results showed that needs factors were most strongly associated with ED utilization, particularly schizophrenia and personality disorders. Predisposing and enabling factors each contributed one variable to the model: past hospitalization for Mental Health (MH) reasons, and having regular care from an outpatient psychiatrist over the 12 months prior to interview at the ED, respectively. Increasing integration of MH services in networks may reduce unnecessary ED utilization and overcrowding, while providing better accessibility and care continuity for patients who visit ED for MH reasons.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Recent studies have demonstrated that emergency department (ED) overcrowding may be attributed to high demand from patients seeking medical attention, not only for urgent treatment but often for treatment occasioned by the lack of availability or inadequacy of health services in the community.1, 2 For instance, the reduction of inpatient beds2 or limited access to healthcare resources in the community1 has resulted in the increased probability of ED use. This high influx of patients may leave ED with insufficient resources to provide urgent care services while compromising patient safety, comfort, and satisfaction.1, 2 Excessive ED use may also raise health care costs and ultimately result in reduced quality of health care.1, 2
The inadequacies in health care that stem from ED overcrowding may be partially explained by the prevalence of people visiting ED for mental health (MH) reasons.3, 4 In fact, research shows that mental disorder (MD) was the primary reason for 4–15% of all ED visits while 8–27% of those ED visits resulted in hospitalizations lasting 38% longer than those of ED patients without MD.5, 6 Moreover, according to studies conducted in various countries, small numbers of patients with MD make repeated use of ED services, accounting for a disproportionate number of total ED visits.7,8,9 High ED utilizers for MH reasons have usually been defined in the field as people who visit the ED three to four, or more, times per year.10,11,12 Examining the frequency of visits in a psychiatric ED, a Canadian study reported that 2% of these high utilizers who attended the psychiatric ED accounted for 21% of all ED visits over a 15-year period.11 Studies have also shown that high ED utilizers for MH reasons often have more than one MD, including substance use disorder (SUD), and are often high utilizers of other health services as well.13, 14 Thus, a vital research target has involved the identification of factors associated with frequent ED utilization in efforts to better manage high ED utilizers, reduce excessive health care expenses, and improve quality of health services.
To better discern factors predicting frequent ED utilization, the Anderson behavioral model may be used as a conceptual framework.15 This model is often applied in evaluative health care research to analyze risk factors, service utilization, and outcomes in vulnerable populations, including patients with MD.16,17,18 According to this framework, variables of interest are classified as predisposing, enabling, and needs factors.15 Predisposing factors refer to individual characteristics, such as age, sex, marital status, etc.; enabling factors are those that influence health service use, such as regular sources of care and satisfaction with health services etc.; and needs factors are clinical variables, particularly those referring to the number and types of disorders.17
Research has shown that needs factors tend to be the most strongly associated with frequent ED utilization, followed by predisposing and or enabling factors.19, 20 Needs found to be associated with frequent ED utilization include MD such as schizophrenia,11, 21 personality disorders,9, 10, 22 anxiety disorders,21, 23, 24 affective disorders,12, 23, 24 SUD,11, 24,25,26 as well as comorbid MD/SUD and or chronic physical illnesses.11, 27,28,29 While such clinical diagnoses are objective health measures, more subjective measures such as patient self-perceptions of physical and mental health may also be considered as needs factors, playing a role in help-seeking for medical care or support.30, 31 However, these types of measures have not been studied in the context of ED utilization.
Research identifying associations between predisposing and enabling factors, with frequent ED utilization has been less consistent, however. Concerning predisposing factors, some studies have identified associations between frequent ED utilization and being male, or being in the young adult to early middle-age range.25, 27, 32 These high ED utilizers are more likely to be unemployed, to have low income, and little family support as compared with other ED utilizers.33, 34 Therefore, they may lack opportunities for gaining knowledge about MH resources. Moreover, past hospitalization for MH reasons has also been shown to be a strong indicator of an individual’s predisposition to make subsequent use of ED and other health services.35 Patient perceptions of the attitudes held by MH professionals toward them may also be an important predisposing factor for ED use, due to widespread stigmatizing attitudes toward mental illness even among trained MH professionals.36 Yet no previous study has examined this factor with respect to predictors of ED utilization.
In terms of enabling factors, while some studies have associated frequent ED utilization with frequent use of other health services,20, 37 others have found the contrary: that lower use of community-based MH services may be linked to frequent ED utilization.38, 39 Perhaps this discrepancy may be due to differences in patient satisfaction with respect to the quality of health services (i.e., accessibility, continuity, intensity of care, etc.). However, few studies have explored whether ED use is influenced by patient satisfaction with ED and community health services. In fact, research on the influence of community-based service utilization in relation to frequent ED utilization is lacking. While studies such as Huynh et al.19 found that a regular source of care (i.e., having a family physician) has been associated with higher ED use, this association needs further investigation.
Since profiles of high ED utilizers are heterogenous, factors predicting frequent ED utilization for MH reasons require further examination. Previous research that examined different subgroups of ED utilizers have mostly used administrative databanks, and were conducted in a single ED setting. This study combines information from both administrative databanks and patient surveys conducted at multiple ED settings. In an effort to address the inconsistencies in the literature concerning predisposing and enabling factors, the survey for this study included several health service utilization variables, as well as other variables that have never or rarely been tested with ED utilizers (e.g., self-rated knowledge about MH resources, service satisfaction, perceived physical and mental health, etc.) Moreover, this study is one of few using the Andersen behavioral model as a conceptual framework to analyze the contribution of predisposing, enabling, and needs factors in ED utilization. In this context, the purpose of this study was to determine predictors of frequent ED utilization for MH reasons in a sample of 320 patients from six hospital ED in Quebec. Based on the literature, it was hypothesized that needs factors would be the strongest predictors of frequent ED utilization, but it was also expected to find associated predisposing and enabling factors in the model.
Methods
Setting and data collection
The six ED sites chosen for this study operated in three different Quebec regional health networks. Two ED were situated in Montreal, three in Quebec City, and one in a suburban area. Four were psychiatric ED integrated into general ED; another was a general ED with a psychiatric department, and, finally, a psychiatric ED within a MH university institute.
Participants who presented at ED with mental health concerns as the primary reason for their visits were recruited between January and June 2017. Inclusion in the study was based on the ability of potential participants to provide informed consent, as evaluated by ED staff. Participants also had to provide consent for research team members to access their medical records for 2016–2017, which would cover the 12-month period prior to information collected from the questionnaire during the interview. Data were collected for study participants on previous diagnoses, hospitalizations, ED, and other health service utilization.
Participant interviews were conducted on-site at ED but in separate offices, and at various times and days of the week, especially when ED were operating at peak capacity. In cases where the conditions of participants prevented them from following through with interviews at the time of recruitment, interviews were postponed until the patients had stabilized, whether during or after hospitalization. A structured patient questionnaire was administered, requiring about 30 min to complete. Questions were adapted from the Canadian Community Health Survey-MH,40 and included sociodemographic and socioeconomic characteristics, patient health beliefs (e.g., self-rated knowledge about MH resources), utilization and satisfaction with health services (e.g., family physician), as well as perceived physical and mental health. SUD was also assessed in the questionnaire using two standardized scales: the Alcohol Use Disorders Identification Test (AUDIT),41 measuring consequences of alcohol use (ten items) with a score of ≥ 8 indicating an alcohol use disorder; and the Drug Abuse Screening Test-20 (DAST-20),42 measuring consequences of drug use (ten items) with a score of ≥ 6 indicating a drug use disorder. The Cronbach’s alpha in the original validation was 0.88 for the AUDIT43 and 0.74 for the DAST-20.42
Data were also obtained from two provincial health administrative databanks: (1) the Quebec Health Insurance Regime (RAMQ), which includes information on ED and other health service utilization, medical diagnoses, and MD; and (2) the hospitalization databank (MED-ECHO) for hospitalization and discharge records. RAMQ and MED-ECHO data were retrieved from these databanks for the years 2016–2017 to provide a more comprehensive medical and service use history for participants. These data were merged with the questionnaire responses of each participant. The study was approved by a MH university institute research ethics board.
Conceptual framework and study variables
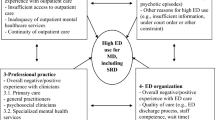
Based on the Andersen Behavioral Model15 and literature on ED and other service use for MH reasons, independent variables were identified, and organized into predisposing, enabling, and needs factors for analysis with the dependent variable: number of ED visits for MH reasons over the 12 months prior to interview at the ED (Fig. 1). The dependent variable was collected from the questionnaire. Predisposing factors included age, sex, education level, employment status, household income, having social support from family or friends, self-rated knowledge about MH resources, and patient perceptions on attitudes held by MH professionals (outside the ED) toward them—collected by the questionnaire; while data on past hospitalization for MH reasons (frequency and number of days) came from the databanks. Enabling factors included having a regular source of care (outside the ED or hospitalization) over the 12 months prior to interview at the ED and satisfaction with regular care received from a family physician, an outpatient psychiatrist, and or a case manager—collected from the questionnaire; while data on frequency of family physician and outpatient psychiatrist consultations for MH reasons (outside the ED or hospitalization) came from the databanks. Needs factors included perceived physical and mental health, and SUD (AUDIT score ≥ 8; DAST-20 score ≥ 6)—collected by the questionnaire; and clinical diagnoses (anxiety, depression, schizophrenia, bipolar disorder, personality disorders, and number of chronic physical illnesses), came from the databanks.

Conceptual framework based on the Andersen Behavioral Model
Data analyses
Univariate, bivariate, and multivariate analyses were carried out. Univariate analyses were comprised of frequency distribution for categorical variables (number and percentages), mean values, and corresponding standard deviations for continuous variables. The dependent variable, number of visits to ED for MH reasons over the 12 months prior to interview at the ED, was assessed with regard to normality assumptions (skewness and kurtosis). Bivariate analyses were comprised of simple linear regression analyses, to assess associations (with the alpha value set at p < 0.10) between each independent variable and the dependent variable, separately. Multivariate analyses were performed for significantly associated variables introduced by blocks into the hierarchical linear regression model, using Backward elimination method. Following the hypothesis, variables in the needs block were entered into the model first, followed by variables in the predisposing and enabling blocks. For each block of predictors, the total variance explained, and the model fit were generated.
Results
The participant response rate was 88%, with 328 participants accepted into the study and 43 individuals who declined to participate in the study of a total of 371 initially invited. Eight participants were later removed from the study due to missing data, resulting in a final sample of 320 participants for the analyses. Participant characteristics (N = 320) are reported in Table 1. Mean age was 39 years old and 52% of participants were female. About 56% of participants had more than a secondary education level, and 33% were currently employed. Regarding household income, 44% earned less than CAN$21,000/year. Over 90% of participants reported having social support from family or friends. About 40% rated their knowledge about MH resources as poor, while more than 75% had positive perceptions of MH professionals (outside the ED) or viewed themselves as treated fairly by them. Regarding past hospitalization for MH reasons, average frequency was about one hospitalization within a year, with the average number of days at 16.71. Approximately 40% of participants reported having a regular source of care (outside the ED or hospitalization) during the previous 12 months; with 65% receiving care from a family physician, 45% from an outpatient psychiatrist, and 39% from a case manager. Around 33% were satisfied or totally satisfied with regular care received from an outpatient psychiatrist or from a case manager. The mean frequency of visits to a family physician was 1.07, and to an outpatient psychiatrist was 8.06. More than 40% of participants rated their physical and mental health as poor or fair. The three most prevalent MD were depression (46%), anxiety (31%), and schizophrenia (30%). The dependent variable, number of ED visits for MH reasons over the 12 months prior to interview at the ED, ranged from 0 to 40, with a mean of 2 (SD = 4). Within this distribution, 14% of participants qualified as high ED utilizers (≥ 4 ED visits or more during the year). The dependent variable was normally distributed, with a skewness of 0.845, and a kurtosis of 0.298.
Bivariate analyses are presented in Table 2, including variables significantly associated with the dependent variable based on a 90% confidence interval. These variables were used to build the hierarchical linear regression model (Table 3), on the basis of needs factors, followed by predisposing, and enabling factors. Among needs factors, the first block, five predictors were retained: anxiety, depression, schizophrenia, bipolar disorder, and personality disorders. With the addition of the second block, predisposing factors, only one variable was retained: frequency of past hospitalization for MH reasons (2015–2016). Likewise, only one variable was retained after the introduction of the third block, enabling factors: having regular care from an outpatient psychiatrist (outside the ED) over the 12 months prior to interview at the ED. All the predictors retained remained positively and significantly associated in the regression model with introduction of the three blocks, and with a 95% confidence level. The total variance explained by variables in the model was 56%, with 47% attributed to needs factors, 8% to predisposing factors, and 1% to enabling factors. The model fit, as determined by the ANOVA F test, was acceptable.
Discussion
This study examined predictors of frequent ED utilization for MH reasons, in relation to predisposing, enabling and needs factors, for a sample of 320 participants recruited from six ED in Quebec. Participants reported an average of two ED visits per year, and the number of high ED utilizers (14% at ≥ 4 visits per year) was comparable to frequencies reported in the literature, which vary from less than 1% to 18%.44 Results of the study confirmed the hypothesis that needs factors were most strongly associated with ED utilization (47%), followed by predisposing and enabling factors.
The result that needs factors were the strongest predictors confirms findings from previous studies that identified MD as highly associated with frequent ED utilization.19, 20 Among the MD tested in this study, personality disorders and schizophrenia were found to be the strongest predictors of frequent ED utilization. Previous studies have found that patients with these chronic and severe MD account for a large proportion of patients considered high ED utilizers.11, 21, 24 Moreover, individuals with anxiety or affective disorders may also experience severe symptoms that compromise their health and lead them to seek care at the ED.12, 19 These MD may also produce unpleasant physical symptoms (e.g., gastrointestinal symptoms, headache, sleep disturbance, pain, etc.) or mimic serious medical conditions like heart attack.45, 46 Many patients with MD, especially those with severe MD, have also reported life-threatening behaviors or conditions such as self-harm, suicidal ideation, or attempt,33 which are highly associated with ED visits for MH reasons.47
Among the predisposing factors, past hospitalization for MH reasons was identified as the only predictor of frequent ED utilization in this study. This finding is supported by previous studies that have reported frequent ED utilization as highly associated with past hospitalization,25, 48 and also subsequent hospitalization for MH reasons.17 A recent study conducted in Montreal, Canada showed that one-third of patients with MD visiting the ED, or hospitalized following an ED visit, made return visits to the ED within 30 days of discharge,49 suggesting a persistence of high unmet needs due to inadequate care. Furthermore, since treating severe MD, comorbid MD/SUD, or MD/chronic physical illnesses in a single ED visit is difficult, patients with these conditions and whose MH needs tend to remain unmet, particularly those who have been previously hospitalized, may continue to seek help at ED on a frequent basis.17, 50, 51
Regarding enabling factors, having regular care from an outpatient psychiatrist over the 12 months prior to interview at the ED was the only predictor of frequent ED utilization. Few patients were followed by a psychiatrist regularly, and they usually presented with more severe MD or complex profiles, which may explain their frequent use of ED. These types of patients may also exhibit serious needs in other areas such as housing or food adequacy.52 However, the accessibility and intensity of care provided by outpatient psychiatrists may be insufficient, and thereby lead patients to seek help from ED for their unmet needs or relief in crisis situations during the intervals between scheduled psychiatric appointments. Studies have also shown that frequent ED utilization is associated with inadequate primary care or services in the community,38, 39 as well as poor integration or coordination within and across MH service networks.44, 53
It was surprising that some factors known to be strongly associated with frequent ED utilization did not emerge as significant predictors of ED utilization in this study. For example, there was a high prevalence of SUD in the study sample with about one-third scoring above the cut-offs for AUDIT and DAST-scores; yet neither alcohol or drug consumption were found to be strongly associated with frequent ED utilization in the hierarchical analyses. While studies on high ED utilizers have identified SUD as a strong indicator of ED utilization,24, 44 the results may be explained by the possibility that participants visiting the ED for MH reasons may have denied or underreported their alcohol and or drug consumption. This often occurs among patients with SUD, according to previous research.19, 54
Concerning predisposing factors, this sample represented a highly deprived group in terms of sociodemographic indicators, with two-thirds unemployed and about half with a household income below CAN$21,000/year. Although poor socioeconomic conditions are known to act as stressors to physical and mental health that may lead people to seek ED services,55 the socioeconomic differences among participants in this study may not have been sufficient to predict differences in their frequency of ED utilization, whether single or multiple ED visits.
Finally, it was surprising that having either a family physician or a case manager did not emerge as a significant protective factor against frequent ED utilization. In the case of family physicians, there is currently a shortage in Quebec where only 55% of patients with MD have been reported to have a family physician.49, 56 Moreover, family physicians are considered to have limited ability to treat MD, making the ED a more logical choice for patients seeking MH care.57, 58 With respect to case managers, while they provide follow-up that may act as a protective measure against repeated ED visits, in crisis situations for instance, these professionals may also encourage patients to seek help from ED services.59, 60 Overall, follow-up by case managers in Quebec such as in assertive community treatment and intensive case management programs61, 62 also tends to focus on patients with severe MD, who are known to be high utilizers of ED and other health services.
This study has some limitations. First, as the research was conducted exclusively in urban areas, the findings may not be generalizable to semi-urban or rural areas. Second, the study settings were all located in Quebec, which has a specific configuration of MH care services integrated within a universal health care system. Therefore, the study findings may not apply in countries that have very different MH care systems, especially those, such as the USA, with more privatized health care arrangements. Third, data on patient health, perceived physical/mental health, and satisfaction with health services were self-reported, and therefore may have presented a risk of bias. Finally, patterns of service use related to physical health were not considered in this study.
Implications for behavioral health
This is the first study to identify predictors of frequent ED utilization for MH reasons using the Andersen Behavioral Model, merged data from a questionnaire and databanks, and a hierarchical regression analysis. The hypothesis that needs factors would explain most variation in frequency of ED utilization was confirmed, with schizophrenia and personality disorders as the strongest predictors. Two other variables among the predisposing and enabling factors, also emerged contributing to the model: having a history of hospitalization for MH reasons, and regular care from an outpatient psychiatrist over the 12 months prior to interview at the ED.
These findings suggest that frequent ED utilization may be reduced by addressing unmet needs for MH care among ED utilizers, especially patients with severe MD like schizophrenia and personality disorders and those more likely to have a history of hospitalization or to see a psychiatrist as part of regular care. Strategies that may reduce frequent ED use for MH reasons include assertive community treatment, home treatment teams, and intensive case management. These practices enhance access to care and follow-up for MH needs, thereby reducing ED use. These strategies also have benefits for patients with other severe or complex MH profiles and unmet needs. Other measures aimed at minimizing ED utilization for MH reasons include post-ED care planning, shared-care, case management, and improved coordination between ED and primary care (e.g., crisis centers). Increasing integration of MH service networks around ED should also improve accessibility and continuity of care for high ED utilizers, thereby reducing unnecessary ED utilization and overcrowding.
References
Burns TR. Contributing factors of frequent use of the emergency department: a synthesis. International Emergency Nursing. 2017;35:51–55.
Rasouli HR, Aliakbar Esfahani A, Abbasi Farajzadeh M. Challenges, consequences, and lessons for way-outs to emergencies at hospitals: a systematic review study. BMC Emergency Medicine. 2019;19(1):62.
Doupe MB, Palatnick W, Day S, et al. Frequent users of emergency departments: developing standard definitions and defining prominent risk factors. Annals of Emergency Medicine. 2012;60(1):24–32.
Larkin GL, Beautrais AL, Spirito A, Kirrane BM, Lippmann MJ, Milzman DP. Mental health and emergency medicine: a research agenda. Academic Emergency Medicine. 2009;16(11):1110–1119.
Barratt H, Rojas-Garcia A, Clarke K, et al. Epidemiology of mental health attendances at emergency departments: systematic review and meta-analysis. PLoS One. 2016;11(4):e0154449.
Clarke D, Usick R, Sanderson A, Giles-Smith L, Baker J. Emergency department staff attitudes towards mental health consumers: a literature review and thematic content analysis. International Journal of Mental Health Nursing. 2014;23(3):273–284.
Mandelberg JH, Kuhn RE, Kohn MA. Epidemiologic analysis of an urban, public emergency department's frequent users. Academic Emergency Medicine. 2000;7(6):637–646.
Hansagi H, Olsson M, Sjoberg S, Tomson Y, Goransson S. Frequent use of the hospital emergency department is indicative of high use of other health care services. Annals of Emergency Medicine. 2001;37(6):561–567.
Poremski D, Kunjithapatham G, Koh D, Lim XY, Alexander M, Lee C. Lost keys: understanding service providers' impressions of frequent visitors to psychiatric emergency services in Singapore. Psychiatric Services. 2017;68(4):390–395.
Althaus F, Paroz S, Hugli O, et al. Effectiveness of interventions targeting frequent users of emergency departments: a systematic review. Annals of Emergency Medicine. 2011;58(1):41–52 e42.
Chaput YJ, Lebel MJ. Demographic and clinical profiles of patients who make multiple visits to psychiatric emergency services. Psychiatric Services. 2007;58(3):335–341.
Sirotich F, Durbin A, Durbin J. Examining the need profiles of patients with multiple emergency department visits for mental health reasons: a cross-sectional study. Social Psychiatry and Psychiatric Epidemiology. 2016;51(5):777–786.
Fahimi J, Aurrecoechea, A., Anderson, E., Herring, A., Alter, H. Substance abuse and mental health visits among adolescents presenting to US emergency departments. Pediatric Emergency Care. 2015;31:331–338.
Pines JM, Asplin BR, Kaji AH, et al. Frequent users of emergency department services: gaps in knowledge and a proposed research agenda. Academic Emergency Medicine. 2011;18:e64–e69.
Andersen RM. Revisiting the behavioral model and access to medical care: does it matter? Journal of Health and Social Behavior. 1995;36(1):1–10.
Doran KM, Shumway M, Hoff RA, Blackstock OJ, Dilworth SE, Riley ED. Correlates of hospital use in homeless and unstably housed women: the role of physical health and pain. Women's Health Issues. 2014;24(5):535–541.
Hamilton JE, Desai PV, Hoot NR, et al. Factors associated with the likelihood of hospitalization following emergency department visits for behavioral health conditions. Academic Emergency Medicine. 2016;23(11):1257–1266.
Gasperini B, Cherubini A, Pierri F, Barbadoro P, Fedecostante M, Prospero E. Potentially preventable visits to the emergency department in older adults: results from a national survey in Italy. PLoS One. 2017;12(12):e0189925.
Huynh C, Ferland F, Blanchette-Martin N, Menard JM, Fleury MJ. Factors influencing the frequency of emergency department utilization by individuals with substance use disorders. Psychiatric Quarterly. 2016;87(4):713–728.
Richard-Lepouriel H, Weber K, Baertschi M, DiGiorgio S, Sarasin F, Canuto A. Predictors of recurrent use of psychiatric emergency services. Psychiatric Services. 2015;66(5):521–526.
Wooden MD, Air TM, Schrader GD, Wieland B, Goldney RD. Frequent attenders with mental disorders at a general hospital emergency department. Emergency Medicine Australasia. 2009;21(3):191–195.
Chang G, Weiss AP, Orav EJ, Rauch SL. Predictors of frequent emergency department use among patients with psychiatric illness. General Hospital Psychiatry. 2014;36(6):716–720.
Brunero S, Fairbrother G, Lee S, Davis M. Clinical characteristics of people with mental health problems who frequently attend an australian emergency department. Australian Health Review. 2007;31(3):462–470.
Vu F, Daeppen JB, Hugli O, et al. Screening of mental health and substance users in frequent users of a general Swiss emergency department. BMC Emergency Medicine. 2015;15:27.
Ledoux Y, Minner P. Occasional and frequent repeaters in a psychiatric emergency room. Social Psychiatry and Psychiatric Epidemiology. 2006;41(2):115–121.
Aagaard J, Aagaard A, Buus N. Predictors of frequent visits to a psychiatric emergency room: a large-scale register study combined with a small-scale interview study. International Journal of Nursing Studies. 2014;51(7):1003–1013.
Brennan JJ, Chan TC, Hsia RY, Wilson MP, Castillo EM. Emergency department utilization among frequent users with psychiatric visits. Academic Emergency Medicine. 2014;21(9):1015–1022.
Curran GM, Sullivan G, Williams K, et al. Emergency department use of persons with comorbid psychiatric and substance abuse disorders. Annals of Emergency Medicine. 2003;41(5):659–667.
Curran GM, Sullivan G, Williams K, Han X, Allee E, Kotrla KJ. The association of psychiatric comorbidity and use of the emergency department among persons with substance use disorders: an observational cohort study. BMC Emergency Medicine. 2008;8:17.
Briner D, Jäger M, Kawohl W, Baumgartner-Nietlisbach G. [Mental disorder and self-rated health among homeless people in Zurich—first epidemiological data from Switzerland]. Psychiatrische Praxis. 2017;44(6):339–347.
Jang Y, Yoon H, Chiriboga DA, Molinari V, Powers DA. Bridging the gap between common mental disorders and service use: the role of self-rated mental health among African Americans. American Journal of Geriatric Psychiatry. 2015;23(7):658–665.
Young AS, Chinman MJ, Cradock-O'Leary JA, et al. Characteristics of individuals with severe mental illness who use emergency services. American Journal of Geriatric Psychiatry. 2005;41(2):159–168.
Olsson M, Hansagi H. Repeated use of the emergency department: qualitative study of the patient's perspective. Emergency Medicine Journal. 2001;18(6):430–434.
Wise-Harris D, Pauly D, Kahan D, Tan de Bibiana J, Hwang SW, Stergiopoulos V. Hospital was the only option: experiences of frequent emergency department users in mental health. Administration and Policy in Mental Health. 2017;44(3):405–412.
Kahan D, Poremski D, Wise-Harris D, et al. Perceived case management needs and service preferences of frequent emergency department users: lessons learned in a large urban centre. PLoS One. 2016;11(12):e0168782.
Ngamini-Ngui A, Fleury MJ, Moisan J, Gregoire JP, Lesage A, Vanasse A. High users of emergency departments in Quebec among patients with both schizophrenia and a substance use disorder. Psychiatric Services. 2014;65(11):1389–1391.
Doran KM, Raven MC, Rosenheck RA. What drives frequent emergency department use in an integrated health system? National data from the veterans health administration. Annals of Emergency Medicine. 2013;62(2):151–159.
Ayangbayi T, Okunade A, Karakus M, Nianogo T. Characteristics of hospital emergency room visits for mental and substance use disorders. Psychiatric Services. 2017;68(4):408–410.
Nesper AC, Morris BA, Scher LM, Holmes JF. Effect of decreasing county mental health services on the emergency department. Annals of Emergency Medicine. 2016;67(4):525–530.
Statistics Canada. Canadian community health survey—mental health and well-being - cycle 1.2. http://www23.statcan.gc.ca/imdb-bmdi/document/3226_DLI_D1_T22_V2-eng.pdf 2003.
Bohn MJ, Babor TF, Kranzler HR. The alcohol use disorders identification test (AUDIT): validation of a screening instrument for use in medical settings. Journal of Studies on Alcohol. 1995;56(4):423–432.
Carey KB, Carey MP, Chandra PS. Psychometric evaluation of the alcohol use disorders identification test and short drug abuse screening test with psychiatric patients in India. Journal of Clinical Psychiatry. 2003;64(7):767–774.
Accietto C. La Validation d'une Version Française du Questionnaire A.U.D.I.T. "Alcohol Use Identification Test". Genève, Université de Genève; 2003.
Vandyk AD, Harrison MB, VanDenKerkhof EG, Graham ID, Ross-White A. Frequent emergency department use by individuals seeking mental healthcare: a systematic search and review. Archives of Psychiatric Nursing. 2013;27:171–178.
Bailey KP. Physical symptoms comorbid with depression and the new antidepressant duloxetine. Journal of Psychosocial Nursing Mental Health Services. 2003;41(12):13–18.
Carleton RN, Duranceau S, Freeston MH, Boelen PA, McCabe RE, Antony MM. "But it might be a heart attack": intolerance of uncertainty and panic disorder symptoms. Journal of Anxiety Disorders. 2014;28(5):463–470.
Moukaddam N, Flores A, Matorin A, Hayden N, Tucci VT. Difficult patients in the emergency department: personality disorders and beyond. Psychiatric Clinics of North America. 2017;40(3):379–395.
Pasic J, Russo J, Roy-Byrne P. High utilizers of psychiatric emergency services. Psychiatric Services. 2005;56(6):678–684.
Fleury MJ, Fortin M, Rochette L, et al. Assessing quality indicators related to mental health emergency room utilization. BMC Emergency Medicine. 2019;19(1):8.
Krieg C, Hudon C, Chouinard MC, Dufour I. Individual predictors of frequent emergency department use: a scoping review. BMC Health Services Research. 2016;16(1):594.
Douzenis A, Seretis D, Nika S, et al. Factors affecting hospital stay in psychiatric patients: the role of active comorbidity. BMC Health Services Research. 2012;12:166.
Fleury MJ, Bamvita JM, Grenier G, Schmitz N, Piat M, Tremblay J. Adequacy of help received by individuals with severe mental disorders after a major healthcare reform in quebec: predictors and changes at 5-year follow-up. Administration and Policy in Mental Health. 2016;43(5):799–812.
Slade M, Taber D, Clarke MM, et al. Best practices for the treatment of patients with mental and substance use illnesses in the emergency department. Disease-a-month. 2007;53(11–12):536–580.
Macias Konstantopoulos WL, Dreifuss JA, McDermott KA, et al. Identifying patients with problematic drug use in the emergency department: results of a multisite study. Annals of Emergency Medicine. 2014;64(5):516–525.
Parkman T, Neale J, Day E, Drummond C. Qualitative exploration of why people repeatedly attend emergency departments for alcohol-related reasons. BMC Health Services Research. 2017;17(1):140.
Institut de la statistique du Québec. Portrait statistique de la santé mentale des québécois. Résultats de l'Enquête sur la santé dans les collectivités canadiennes Santé mentale 2012; Portrait chiffré: Québec: Gouvernement du Québec, Institut de la statistique du Québec; 2015.
Fleury MJ, Grenir G, Robitaille D. Implementation of the Consultation-Liaison model in Quebec and its impact on primary care providers. Mental Health in Family Medicine. 2016; 12:228–240
Walters P, Tylee A, Golberg D. Psychiatry in Primary Care. In RM Murray, KS Kendler, P McGuffin, S Wessely, DJ Castle (eds). Essential psychiatry .UK: Cambridge University Press; 2008, pp. 479–497.
Tortajada S, Giménez-Campos MS, Villar-López J, et al. Case management for patients with complex multimorbidity: development and validation of a coordinated intervention between primary and hospital care. International Journal of Integrated Care. 2017;17(2):4.
Crane S, Collins L, Hall J, Rochester D, Patch S. Reducing utilization by uninsured frequent users of the emergency department: combining case management and drop-in group medical appointments. Journal of the American Board of Family Medicine. 2012;25(2):184–191.
Addington D, Anderson E, Kelly M, Lesage A, Summerville C. Canadian practice guidelines for comprehensive community treatment for schizophrenia and schizophrenia spectrum disorders. Canadian Journal of Psychiatry. 2017;62(9):662–672.
Moe J, Kirkland SW, Rawe E, et al. Effectiveness of interventions to decrease emergency department visits by adult frequent users: a systematic review. Academic Emergency Medicine. 2017;24(1):40–52.
Acknowledgments
We gratefully acknowledge the financial support of the Fonds de la recherche en santé du Québec (FRSQ) and l’Institut Universitaire sur les Dépendances du Québec (Addiction University Institute). We would also like to thank Judith Sabetti for editorial assistance.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kaltsidis, G., Bamvita, JM., Grenier, G. et al. Predictors of Frequent Emergency Department Utilization for Mental Health Reasons. J Behav Health Serv Res 48, 259–273 (2021). https://doi.org/10.1007/s11414-020-09695-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11414-020-09695-4