
Abstract
Muscle function and exercise performance measures, such as muscle endurance capacity, maximal strength, chair stand score, gait speed, and Timed Up and Go score, are evaluated to diagnose sarcopenia and frailty in older individuals. Furthermore, intramuscular adipose tissue (IntraMAT) content increases with age. Skeletal muscle oxidative capacity determines muscle metabolism and maintains muscle performance. This study aimed to investigate the association of skeletal muscle oxidative capacity with muscle function, exercise performance, and IntraMAT content in older individuals. Thirteen older men and women participated in this study. Skeletal muscle oxidative capacity was assessed by the recovery speed of muscle oxygen saturation after exercise using near-infrared spectroscopy from the medial gastrocnemius. We assessed two muscle functions, peak torque and time to task failure, and four sarcopenia-related exercise performances: handgrip strength, gait speed, 30-s chair stand, and Timed Up and Go. The IntraMAT content was measured using axial magnetic resonance imaging. The results showed a relationship between skeletal muscle oxidative capacity and gait speed but not with muscle functions and other exercise performance measures. Skeletal muscle oxidative capacity was not related to IntraMAT content. Skeletal muscle oxidative capacity, which may be indicative of the capacity of muscle energy production in the mitochondria, is related to locomotive functions but not to other functional parameters or skeletal fat infiltration.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Aging is associated with a decline in muscle strength and loss of muscle mass, a condition known as sarcopenia [1]. Assessment of sarcopenia in older individuals is important because the condition is related to risk of frailty, physical dysfunction, loss of activities of daily living (ADL), and mortality [1]. In addition to sarcopenia, age-related changes in mitochondrial content and oxidative capacity in skeletal muscle play a role in muscle deterioration. Mitochondrial contents of type I and type II muscle fibers are significantly lower in older individuals than in young and middle-aged individuals [2]. In addition, a decline in skeletal muscle oxidative capacity has been observed in older individuals [3]. Therefore, physical dysfunction and decline in ADL are not only related to decreased muscle strength and loss of muscle mass but also to primary dysfunction of skeletal muscle oxidative capacity.
Skeletal muscle oxidative capacity is recognized as mitochondrial oxidative phosphorylation function in skeletal muscles, and a decline in muscle oxidative capacity is related to lower whole-body oxygen consumption and higher muscle fatigability [4, 5]. Brizendine et al. [6] reported faster recovery rates of skeletal muscle oxygen consumption after exercise, an indicator of skeletal muscle oxidative capacity, in endurance athletes than in inactive participants, suggesting higher mitochondrial function in individuals with higher whole-body endurance performance. Time to task failure during repeated intermittent isometric contractions is used as an index of muscle endurance performance. This test has been used to investigate age-related changes in muscle endurance and fatiguability in older individuals [7,8,9]. Hence, it is reasonable to speculate that older individuals with higher muscle oxidative capacity have longer time to task failure; however, no study has assessed this relationship, especially in older individuals. Besides, skeletal muscle oxidative capacity is associated with muscle strength and exercise performance [4, 5, 10]. These parameters, assessed by isometric peak torque, gait speed, handgrip strength, chair stand test result, and Timed Up and Go (TUG) score, are important indices for risk of frailty, falls, and mortality in older individuals [1, 11]. However, the relationship between the availability of these performance indices and skeletal muscle oxidative capacity in older individuals remains unclear.
Mitochondrial function in skeletal muscle is related to lipid accumulation in the skeletal muscle [3, 12]. Intramuscular adipose tissue (IntraMAT) is determined by the balance between fatty acid delivery and mitochondrial oxidative phosphorylation, which increases with age [13, 14]. Thus, older individuals with good skeletal muscle oxidative capacity may have lower IntraMAT content. Excessive IntraMAT accumulation leads to insulin resistance and lower muscle force generation [15, 16]; therefore, it is important to elucidate whether muscle oxidative capacity is related to IntraMAT in older individuals for the prevention of metabolic disorders and sarcopenia.
Muscle oxidative capacity is indirectly assessed by evaluating mitochondrial respiratory function using muscle biopsy samples. In contrast, 31-phosphocreatine magnetic resonance spectroscopy (31P-MRS) is a noninvasive method for measuring muscle mitochondrial function. Dynamic phosphocreatine (PCr) resynthesis after exercise evaluated by 31P-MRS serves as a direct assessment of mitochondrial function [17, 18]. Muscle biopsy is an invasive technique, and 31P-MRS requires large and expensive equipment and technical expertise; thus, there is need to develop other methodologies that overcome these issues. Instead, the kinetics of muscle oxygen consumption (mVO2) after exercise obtained using near-infrared spectroscopy (NIRS) are closely related to mitochondrial oxidative capacity measured by muscle biopsy sample in human and in vivo PCr recovery [19, 20]. NIRS can be used to assess muscle oxidative capacity; it is noninvasive, low-cost, and highly reliable. Lagerwaard et al. [21] reported that mVO2 recovery was slower in older individuals than in young individuals. Hence, mVO2 recovery after exercise obtained via NIRS could be applied to assess age-related decline in skeletal muscle oxidative capacity in older individuals.
Accordingly, the present study aimed to investigate whether skeletal muscle oxidative capacity determined by NIRS is related to skeletal muscle function, including endurance performance, sarcopenia-related exercise performance, and IntraMAT content, in older individuals. Considering that skeletal muscle oxidative capacity dysfunction plays a role in muscle deterioration, we hypothesized that skeletal muscle oxidative capacity is related to muscle function, sarcopenia-related exercise performance, and IntraMAT content in older individuals.
Methods
Participants
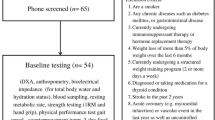
The inclusion criterion was age ≥ 65 years. The exclusion criteria were as follows: (1) receiving medical treatment for obesity or diabetes, (2) dependence on others for ADLs, (3) diagnosis of cognitive impairment and dementia by a medical doctor, (4) musculoskeletal, neuromuscular, orthopedic, and cardiovascular diseases, and (5) restriction of exercise, sports, and physical activities by a medical doctor. In total, 13 older men and women (age: 75.1 ± 3.3 years; height: 160.5 ± 8.0 cm; body mass: 59.4 ± 6.3 kg; body mass index: 22.8 ± 1.6 kg/m2, men/women = 6/7) participated in this study. Before the experiment, the purpose, procedures, and risks of the study were explained to each participant, and written informed consent was obtained from all participants. All examination protocols were approved by the Ethics Committees of Chukyo University (no. 2020–055) and Nagoya University (no. 20–07). This study was conducted in accordance with the ethical principles of the Declaration of Helsinki.
NIRS measurement
Skeletal muscle oxidative capacity was assessed as described previously [20, 21]. The NIRS system (Hb14; ASTEM, Tokyo, Japan) determined oxyhemoglobin/myoglobin (Oxy-Hb/Mb), deoxyhemoglobin/myoglobin (Deoxy-Hb/Mb), and total hemoglobin/myoglobin (Total-Hb/Mb) levels by measuring light attenuation at wavelengths of 770 and 830 nm, which were analyzed using algorithms based on a modified Beer–Lambert law. The probe consisted of one light source and two photodiode detectors, and the optode distances were 20 and 30 mm. Furthermore, the NIRS system directly provided absolute values of tissue oxygen saturation (StO2). The StO2 values were calculated using the relative absorption coefficients obtained from the slope of light attenuation over the distance measured at two focal points from the light emission. These data were transmitted to a personal computer (HP Pavilion dv6-6100; Hewlett Packard, Palo Alto, CA, USA) using a Bluetooth wireless system, and the NIRS data were sampled at 1–2 Hz.
The NIRS sensor was placed on the medial gastrocnemius (MG) of the right leg. The MG sensor was placed at 30% of the distance from the lateral joint line of the knee to the lateral malleolus. Surface layer, including subcutaneous fat, affected NIRS signal; therefore, our NIRS system had installed a calculation program to remove the influence of subcutaneous fat thickness based on a previous study [22]. Subcutaneous fat thickness was defined as the distance between the dermis and upper boundary of the ventral fascia using axial image captured by ultrasonography (Logiq e Premium; GE Healthcare Japan, Tokyo, Japan). We confirmed that subcutaneous fat thickness in all participants was ≤ 10 mm (average; 4.7 ± 1.9 mm, range; 2.0–7.6 mm). Individual subcutaneous fat thickness value was input to run the NIRS system on a personal computer before the measurement; it was used to determine the relative change in Hb/Mb and the absolute value of StO2. To measure oxygen recovery, a blood pressure cuff (Hokanson SC12; Hokanson, Bellevue, WA, USA) was placed just above the knee joint. The cuff was powered and controlled using a rapid cuff inflator system (Hokanson E20, Hokanson) set at 250 mmHg.
The NIRS experimental protocol consisted of three consecutive parts: (1) resting StO2 measurements, (2) a short duration (15 s) of isometric contraction of the MG to increase mVO2, and (3) repeated arterial occlusion without contraction. Prior to the NIRS measurement, the maximal voluntary contraction (MVC) of the participants during plantarflexion at a 10° plantarflex ankle joint angle (0° is the neutral position) was measured using a torque meter. The hip was fixed to the dynamometer using a strap, with the hip joint at 90° flexion and the knee joint at full extension; the ankle of the right leg was set on a pad linked to the torque sensor (Takei Scientific Instruments, Niigata, Japan). The highest MVC torque was selected for each trial as peak torque. We set 50% MVC torque as the target for 15 s of isometric contraction, and the target force was represented by horizontal lines on the computer monitor for visual feedback during the exercise.
The recovery kinetics of mVO2 were measured using a series of transient arterial occlusions with the following timings: 5 s on/5 s off for occlusions × 6 times (#1–6), 7 s on/7 s off for occlusions × 4 times (#7–10), 10 s on/15 s off for occlusions × 4 times (#11–14), and 10 s on/20 s off for occlusions × 4 times (#15–18) [20]. Post-exercise mVO2 was calculated for each occlusion using simple linear regression, with the start and end of each occlusion marked to allow for standardized (i.e., no user bias) calculations of mVO2. The post-exercise mVO2 measurements were fitted to a monoexponential curve as follows:
where y is the relative mVO2 during arterial occlusion, end is the mVO2 immediately following exercise, delta is the change in mVO2 from rest to end of exercise, k is the fitting rate constant, and t is time. The time constant was used as an index of skeletal muscle oxidative capacity as previously described [20]. The time constant is inversely related to muscle oxidative capacity; namely a lower time constant indicates better muscle oxidative capacity. A series of exercises and occlusion procedures were performed twice, and the results were averaged. Time constant data was calculated from fitting curve to post-exercise mVO2. We set the threshold for the fitting curve (R2 ≥ 0.75), and excluded from the data under the threshold to keep the reliability.
Muscle and physical exercise performance tests
Time to task failure was measured as a parameter of muscle endurance. After determining the MVC, the participants performed repeated trapezoidal contractions of the calf muscles at 50% MVC following the visual template on a computer monitor, as previously described [9]. The task comprised three phases; the first phase was to increase the isometric force from 0 to 50% MVC in 5 s (10% MVC/s), the second phase was to maintain 50% MVC for 15 s, and the third phase was to decrease the force from 50 to 0% MVC in 5 s (10% MVC/s). The participants controlled the force according to the guidelines on the computer monitor and repeated the task for as many cycles as possible without any interval to the tempo of the metronome. The end of data collection was objectively determined when the participants could not maintain 45% MVC for a 5-s period during the second phase. The time to plantarflexion task failure was recorded as the number of seconds spent from the start to the end, including the increase and decrease in force. Before the measurement, the participants practiced the increase, hold, and decrease phases of the tempo. After a 10–15-min rest, the participants underwent the measurements.
All participants completed four physical exercise performance tests used in previous studies: handgrip strength, TUG, 30-s chair stand, and normal gait speed. All the tests were performed in a gymnasium. The handgrip strength of both hands was assessed using a dynamometer (TKK5401; Takei Scientific Instruments). The grip length was adjusted to the point at which the proximal interphalangeal joint of the middle finger was bent 90°. The participants were asked to squeeze the dynamometer as hard as possible with 0° shoulder flexion and fully extended elbows while standing. The maximum value was recorded as the handgrip strength. For the TUG test, we measured the time required by the participants to rise from a chair, walk 3 m in a straight line, turn around the cone, walk back to the chair, and sit down. The 30-s chair stand test involved recording the repetitive sit down and stand up actions for 30 s with the participant’s arms crossed over their chest. For the 5-m walk test, four parallel lines were taped to the floor at 1, 6, and 7 m (finish line) from the starting line (0 m). The participants were instructed to walk from the start to the finish line at their usual pace. The examiner recorded the time taken while walking alongside the participant. Normal gait speed was calculated from time and distance. Handgrip strength, TUG, and walking tests were conducted twice. The time taken for the TUG and walking tests was measured using a stopwatch, and the shortest time was used for subsequent analysis. These tests were selected because they are: (1) representative and show the relationships with the risk of falls and sarcopenia, (2) closely related to ADLs, and (3) established modalities in previous studies [1, 23].
Magnetic resonance imaging (MRI) measurement
Participants were assessed using a 3.0-T whole-body MRI scanner (MAGNETOM Verio; Siemens Healthcare Diagnostics K. K., Tokyo, Japan). Each participant was placed in the supine position and images of the calf were acquired using a body coil. T1-weighted spin-echo transaxial images of the right calf were captured from the anterior border of the tibia to the lateral malleolus using the following parameters: repetition time, 604 ms; echo time, 11 ms; voxel resolution = 0.75 mm, optimized field of view (FOV), 256 × 256 mm; slice thickness, 10 mm; and inter-slice gap, 0 mm.
Analysis of calf composition
Medical image processing, analysis, and visualization software (version 4.4.0; National Institutes of Health, Bethesda, MD, USA) was used to analyze the images on a computer (iMac; Apple, Cupertino, CA, USA). The procedure for MRI data analysis was described previously [24]. The calf image was obtained from a marker attached 30% proximally to the lateral condyle of the femur and lateral malleolus. We confirmed that the location was adequate for NIRS sensor placement. Anatomical landmarks were identified by palpation. Briefly, we assessed the images at marker points. The method for determining calf composition was similar to that used in a previous study, which used a well-established, nonparametric, and non-uniform intensity normalization algorithm to correct for image heterogeneity due to suboptimal radiofrequency coil uniformity and gradient-driven eddying currents. This step was essential for subsequent analyses, which assumed a homogeneous signal intensity across the images. The optimized image correction parameters were determined (end tolerance, 0.0001; maximum iterations, 100; signal threshold, 1; field distance, 25 mm; subsampling factor, 2; kernel full width at half maximum, 0.15; and Wiener filter noise, 0.01), and the same parameters were applied to all images from all the study participants.
The investigator drew six 5 × 5 mm region of interests (ROIs) for the determination of a threshold that distinguishes IntraMAT from muscle tissue. Three ROIs were placed on the tibialis anterior muscle of each calf; the other three were placed in the subcutaneous adipose tissue. The tibialis anterior comprises < 6% of adipose tissue and was selected to obtain a nearly pure skeletal muscle peak on the pixel number–signal intensity histogram [25]. The total number of pixels within the six ROIs, frequency distribution, histograms of all the pixels, and signal intensities were determined. To ensure minimal investigator bias in the separation of muscle and IntraMAT tissues in the pixel number–signal intensity histogram, we used the Otsu threshold method, which is a reliable histogram shape-based thresholding technique for medical image analyses [26]. To minimize manual tracing-induced errors in the thresholding values, the mean of three trials was used, and the values were applied to all muscles of interest for each participant. After carefully tracing the edge of the MG manually, the following parameters were calculated: (1) the number of pixels with a signal intensity lower than the threshold value (muscle tissue pixel number) and (2) the number of pixels with a signal intensity higher than the threshold (IntraMAT pixel number). IntraMAT and muscle tissue cross-sectional areas (CSAs) were calculated as follows: pixel number × (field of view [FOV]/matrix size)2. IntraMAT content (%) was calculated as follows: IntraMAT CSA/(IntraMAT CSA + muscle tissue CSA) × 100. Muscle tissue CSA was used for the calculation of normalized peak torque as follows: peak torque (Nm)/muscle tissue CSA (cm2).
Lower limb muscle mass
Whole-body muscle mass and fat mass were measured using InBody 430 bioelectrical impedance analyzer (InBody Japan, Tokyo, Japan). The participants were instructed to grasp the handles of the analyzer, with electrodes embedded, and stand barefoot on the electrodes. The skeletal muscle mass index (SMI) of the upper and lower limbs was calculated as follows: SMI = muscle mass (kg)/height (m)2.
Statistical analysis
All values are reported as means and standard deviation. First, we performed a Shapiro–Wilk test to confirm the normality of the parametric data. Subsequently, the Mann–Whitney U test was used to determine sex differences in physical characteristics, muscle oxidative capacity, muscle composition, muscle function, and exercise performance. Spearman’s correlation coefficient (rs) was used to evaluate the relationships between parameters. Statistical significance was set at P < 0.05. All statistical analyses were performed using SPSS version 26.0 J (IBM Corp., Armonk, NY, USA).
Results
Physical characteristics of the participants
The average scores for skeletal muscle oxidative capacity, muscle and physical performance, and muscle composition are presented in Table 1. Our results showed significant differences in height, body mass, SMI, and handgrip strength between men and women (P < 0.05). All participants exceeded the sarcopenia criteria of handgrip strength (men < 28 kg; women < 18 kg). Gait speed and appendicular SMI were other parameters used to diagnose sarcopenia (cut-off values of walking speed was < 1.0 m/s, cut-off values of SMI in men was < 7.0 kg/m2, and SMI in women was < 5.7 kg/m2). Two women had lower SMI; however, they did not have sarcopenia because of their normal handgrip strength and gait speed.
Relationship between skeletal muscle oxidative capacity and muscle function and sarcopenia-related exercise performance
Skeletal muscle oxidative capacity did not have a significant relationship with time to task failure (rs = 0.26, P = 0.39), plantar flexion peak torque (rs = 0.23, P = 0.45), or normalized plantar flexion peak torque (rs = 0.32, P = 0.29) (Fig. 1). The relationship between skeletal muscle oxidative capacity and sarcopenia-related exercise performance is shown in Fig. 2. Skeletal muscle oxidative capacity was significantly related to gait speed (rs = − 0.59, P = 0.03) but not to handgrip strength, 30-s chair stand score, or TUG score (rs = − 0.30, − 0.31, 0.30; P = 0.33, 0.30, 0.33). Skeletal muscle oxidative capacity was not associated with SMI (rs = − 0.09, P = 0.76) (Fig. 2).

Relationships between skeletal muscle oxidative capacity and muscle functions. Muscle oxidative capacity was assessed by postexercise recovery time constant. Black dots: men, white dots: women

Relationship between skeletal muscle oxidative capacity and exercise performances and skeletal muscle index (SMI). Muscle oxidative capacity was assessed by postexercise recovery time constant. Black dots: men, white dots: women
Relationship between skeletal muscle oxidative capacity and IntraMAT
The relationship between muscle oxidative capacity and IntraMAT is shown in Fig. 3. Skeletal muscle oxidative capacity was not significantly associated with IntraMAT content (rs = − 0.15, P = 0.63) or muscle CSA (rs = − 0.03, P = 0.93).

Relationship between muscle oxidative capacity and intramuscular adipose tissue (IntraMAT) content and muscle cross-sectional area (CSA)
Discussion
This study investigated the relationship between skeletal muscle oxidative capacity and muscle function (time of task failure and peak torque), sarcopenia-related exercise performance, and IntraMAT content. Skeletal muscle oxidative capacity was significantly related to gait speed but not to other exercise performance measures. Muscle oxidative capacity was not related to IntraMAT content. We found that skeletal muscle oxidative capacity, which may indicate muscle energy production for mitochondrial function, is related to locomotive functions in older individuals but not to other exercise parameters or skeletal muscle fat infiltration.
Implication and validity of skeletal muscle oxidative capacity determined by NIRS
Skeletal muscle oxidative capacity was evaluated based on the kinetics of mVO2 obtained after exercise with repeated arterial occlusion using NIRS. Skeletal muscle oxidative capacity determined by NIRS has been confirmed to be related to muscle mitochondrial function with high validity [19, 20]. Furthermore, NIRS methodology was established considering the technical and ethical limitations of muscle biopsy and 31P-MRS measurements. We applied this technique in older individuals. The average muscle oxidative capacity of our participants was 52 s (Table 1). Chung et al. [27] reported that muscle oxidative capacity in older individuals (average age: 73 years) was 51.8 s, which is the same with our data. Unfortunately, we did not investigate skeletal measure muscle oxidative capacity in younger individuals. To the best of our knowledge, only few studies have measured muscle oxidative capacity in older individuals using NIRS. Southern et al. [28] reported that muscle oxidative capacity in older patients with heart failure was 13–20% lower than that in healthy middle-aged individuals. In addition, via the comparison of young and older individuals, age-related decline in muscle oxidative capacity was confirmed in the gastrocnemius and vastus lateralis but not in the tibial anterior [21]. These previous results suggested age-related change of muscle oxidative capacity depended on the muscles. We selected MG as the target muscle for the measurement of skeletal muscle oxidative capacity. Skeletal muscle oxidative capacity in our participants, with a range of values similar to those in previous studies, was affected by aging [27, 28].
Relationship between skeletal muscle oxidative capacity and muscle function
The time until intermittent submaximal torque failure was measured as an index of muscle endurance performance and fatiguability [9]. We observed that muscle oxidative capacity did not have a significant relationship with time to task failure in older individuals (Fig. 2). Higher muscle oxidative capacity is associated with better mitochondrial respiratory function [19, 20]. Skeletal muscle mitochondrial oxidative capacity is associated with whole-body aerobic performance [6, 29]. These results implied that regional muscle oxidative capacities responded to whole-body energy demand. The intermittent submaximal torque failure test has been used to assess muscle endurance performance and fatiguability [7,8,9]. Previous studies have shown that muscle fatiguability depends on the load type and target load intensity [30, 31]. In addition, the age-related increase in fatiguability is greater in lower limb muscles than in upper limb muscles [32]. Accordingly, it was suggested that our results may be affected by the task type and target muscle. In our measurement of muscle endurance, participants’ subjective bias could not be excluded because failure timing of the task was determined by the output torque. We did not evaluate fatigue after the task; therefore, it is necessary to investigate the relationship between skeletal muscle oxidative capacity and muscle endurance determined by physiological criteria.
Handgrip strength is a major indicator for sarcopenia diagnosis [1]. Additionally, muscle strength in the lower limbs is a motor output capability and a fundamental parameter for human movement. Skeletal muscle oxidative capacity was not significantly correlated with handgrip strength (rs = − 0.30, P = 0.33) or peak torque (rs = 0.23, P = 0.45) (Figs. 2 and 3). This finding is inconsistent with that of previous studies that showed a significant relationship between PCr recovery rate after exercise and maximum quadriceps muscle strength in older individuals [10]. Mitochondrial dysfunction is associated with lower muscle strength in patients with cancer [33]. This inconsistency was suggested to be caused by methodological differences in skeletal muscle oxidative capacity (NIRS vs. 31P-MRS), target muscles (calf vs. thigh), and participants’ characteristics (healthy older vs. young patients). In addition, Zane et al. [10] investigated the correlation between the PCr recovery rate and maximum quadriceps muscle strength by adjusting for confounding factors, such as age, sex, height, weight, and % PCr depletion. Muscle size is recognized as a factor associated with muscle strength. Furthermore, we calculated normalized peak torque using muscle CSA and investigated its relationship with skeletal muscle oxidative capacity; however, similar to peak torque, there was no significant relationship (Fig. 2). In addition, other physiological factors such as the neuromuscular activation pattern, composition of fiber type, and non-contractile tissue content contribute to muscle strength [14, 34]. Further studies with a larger number of participants should consider each factor more carefully.
Skeletal muscle oxidative capacity and sarcopenia-related exercise performances
Skeletal muscle oxidative capacity is an indicator of muscle mitochondrial capacity and reflects PCr recovery after exercise. Age-related mitochondrial dysfunction reduces the capacity to generate adenosine triphosphate, leading to reduced exercise performance and gait speed [10]. Therefore, we hypothesized that muscle oxidative performance is associated with sarcopenia-related exercise performance. Skeletal muscle oxidative capacity was associated with gait speed (Fig. 2), implying that older individuals with higher oxidative capacity had a faster gait speed, and this finding agrees with that of a previous study [4]. Furthermore, this result suggests that skeletal muscle oxidative capacity plays an important role in dynamic locomotive performance. Gait speed is a parameter for the diagnosis of sarcopenia [1]; thus, maintaining a higher muscle oxidative capacity would prevent sarcopenia and frailty. Muscle oxidative capacity can be improved by resistance training or a combination of resistance and endurance training [35, 36]. Further research is required to determine a more efficient and effective training strategy for improving muscle oxidative capacity.
The chair stand and TUG tests did not correlate with skeletal muscle oxidative capacity (Fig. 2). This result can be explained by the characteristics of the participants. The chair stand test has been proposed as an easy measurement method for the assessment of lower-limb strength and is recommended for the assessment of sarcopenia [1, 23]. Moreover, TUG has been widely used in research and clinical practice to assess the risk of falls, hospitalization, and capacity to perform ADLs [37]. The cut-off TUG test score for the assessment of higher fall risk is > 13.5 s [37]. No participant had a TUG score > 13.5 s; hence, all our participants had a low risk of fall. Skeletal muscle oxidative capacity is lower in patients with heart failure [28], those with amyotrophic lateral sclerosis [38], and those with spinal cord injury [39]. These findings suggest that muscle oxidative capacity can be used in nursing care, hospitalization, and rehabilitation. Future studies comparing skeletal muscle oxidative capacity between healthy and older individuals with physical impairments such as risk of falls, frailty, and sarcopenia are warranted.
Relationships between skeletal muscle oxidative capacity and IntraMAT content
Skeletal muscle mitochondrial function is related to lipid accumulation in the skeletal muscle [12]; therefore, we speculated a significant relationship between skeletal muscle oxidative capacity and IntraMAT content. However, this relationship was not observed (Fig. 3). Skeletal muscle lipids can be classified as lipid droplets in the cytoplasm of muscle cells, known as intramyocellular lipids (IMCL), and lipids stored in the form of triglycerides around muscle cells, known as extramyocellular lipids (EMCL). IntraMAT content evaluated by T1-weighted MRI may mainly reflect EMCL but not IMCL [24]. Previous studies have focused on IMCL as an energy substrate for exercise; however, excessive IMCL accumulation is negatively related to insulin resistance [40]. Yoshiko et al. [41] reported no relationship between IMCL and EMCL in older individuals, suggesting that age-related accumulation of muscle IMCL and EMCL occurs via different pathways. Considering these findings, further techniques of evaluating IMCL are necessary to investigate the relationship between skeletal muscle oxidative capacity and lipid content. Older individuals have higher lipid content in the skeletal muscle than do younger individuals [13, 14, 25]. Patients with type II diabetes, obesity, and spinal cord injuries have higher IntraMAT content and IMCL level than do healthy young individuals [15, 42]. Erickson et al. [39] showed that skeletal muscle oxidative capacity in patients with spinal cord injury was lower than that in healthy individuals. Future research should consider the relationships between these different metabolic properties.
Previous studies have shown that resistance-trained athletes with large muscle sizes have better muscle mitochondrial respiratory function than untrained controls [43]. However, longitudinal intervention studies showed that the effects of resistance training on muscle mitochondria function were not consistent [35, 36, 44]. Our findings showed no relationship between skeletal muscle oxidative capacity, which is represented by skeletal muscle mitochondrial function, and muscle CSA and SMI, which are muscle size parameters (Figs. 2 and 3). Although a limited number of studies have investigated the relationship between muscle oxidative capacity and muscle size in older individuals, Zane et al. [10] established a non-relationship between muscle oxidative capacity and thigh muscle CSA, which supports our result. Furthermore, Jubrias et al. [45] investigated the effect of endurance training on muscle oxidative capacity in older individuals and found that muscle oxidative capacity increased regardless of muscle hypertrophy. This result supports our finding that muscle oxidative capacity is not related to muscle size.
Limitations
Despite these interesting results, this study had some limitations. First, we found sex-based differences in height, weight, SMI, and handgrip strength (Table 1); therefore, an analysis of the relationship separately in men and women or consideration of these parameters as confounding factors, as previously investigated, is warranted. However, the sample size was small. The post hoc powers of the correlation analysis ranged from small (0.05) to medium (0.60). Therefore, all correlation results should be interpreted with caution because of the possibility of a type II error. A large sample size can prevent avoid type II errors; therefore, we aimed to perform another analysis using a larger number of participants. Secondly, we selected the MG, a calf muscle, as the target muscle. The methodology and reliability were established for measuring muscle oxidative capacity from MG [19, 20]. Muscle oxidative capacity in the MG and vastus lateralis was lower in older individuals than in young individuals; however, that of the tibial muscle was similar between both individual groups [21, 27], implying that age-related differences in muscle oxidative capacity depend on the muscles. Thigh muscles, for example, the vastus lateralis, contribute significantly to some kinds of daily activities such as going up and down stairs, walking, and sitting up and down, and some studies have selected the vastus lateralis as the target muscle for the measurement of skeletal muscle oxidative capacity [19, 21, 39]. In further research, the regional characteristics of skeletal muscle oxidative capacity should be considered by comparing different muscles, for example, thigh vs. calf, upper vs. lower, and agonist vs. antagonist muscles. Finally, the validity and reproducibility of muscle oxidative capacity in older individuals were not evaluated. Skeletal muscle oxidative capacity determined by NIRS has been confirmed to be related to muscle mitochondrial function with high validity in young healthy individuals [19, 20]. Several studies applied this technique in older individuals [21, 27]; however, to the best of our knowledge, there was no study to establish the validity in older individuals. Hart et al. [46] investigated the difference in oxidative capacity between young and older individuals. They found that the post-exercise PCr recovery obtained by 31P-MRS and time constant measured by NIRS were not statistically different between young and older individuals. Notably, the average difference was similar between PCr recovery (1.5%) and time constant (1.0%) but was not statistically evaluated. In addition, Kemp et al. [47] reported that the recovery rate of oxyhemoglobin/myoglobin obtained by NIRS after the force output was significantly correlated with that in PCr in older patients with peripheral vascular disease. This result implied that the muscle oxidative capacity evaluated by NIRS would support the result of PCr recovery in older individuals. Furthermore, the reproducibility between the first and second measurements was evaluated by interclass correlation coefficient (ICC). The ICC was 0.37, and this was considered “fair”. Southern et al. [48] reported that day-to-day reproducibility of time constant was ICC 0.24 to 0.65 in but in young individuals’ data. NIRS technique has been applied in heart failure [28], amyotrophic lateral sclerosis [38], and spinal cord injury patients [39]; it would be expected that measuring the validity and reproducibility of muscle oxidative capacity in these participants, that leading to improve the persuasiveness of the findings.
Conclusion
In the present study, we examined the relationship between skeletal muscle oxidative capacity and muscle function, sarcopenia-related exercise performance, and IntraMAT content in older individuals. Skeletal muscle oxidative capacity was associated with gait speed but not with other exercise performance measures. Furthermore, skeletal muscle oxidative capacity was not related to IntraMAT content or skeletal muscle CSA. We demonstrated that muscle oxidative capacity, which may indicate muscle energy production in the mitochondria, is related to locomotive functions but not to other functional parameters or skeletal muscle composition. A few studies have indicated that resistance training improves muscle oxidative capacity in young individuals. Hence, whether it can be applied to older individuals and eventually lead to improved gait ability should be elucidated in further research.
Data availability
Data will be provided by the corresponding author upon request.
References
Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48:16–31.
St-Jean-Pelletier F, Pion CH, Leduc-Gaudet JP, Sgarioto N, Zovile I, Barbat-Artigas S, et al. The impact of ageing, physical activity, and pre-frailty on skeletal muscle phenotype, mitochondrial content, and intramyocellular lipids in men. J Cachexia Sarcopenia Muscle. 2016;8:213–28.
Petersen KF, Befroy D, Dufour S, Dziura J, Ariyan C, Rothman DL, et al. Mitochondrial dysfunction in the elderly: possible role in insulin resistance. Science. 2003;300:1140–2.
Coen PM, Jubrias SA, Distefano G, Amati F, Mackey DC, Glynn NW, et al. Skeletal muscle mitochondrial energetics are associated with maximal aerobic capacity and walking speed in older adults. J Gerontol A Biol Sci Med Sci. 2013;68:447–55.
Santanasto AJ, Glynn NW, Jubrias SA, Conley KE, Boudreau RM, Amati F, et al. Skeletal muscle mitochondrial function and fatigability in older adults. J Gerontol A Biol Sci Med Sci. 2015;70:1379–85.
Brizendine JT, Ryan TE, Larson RD, McCully KK. Skeletal muscle metabolism in endurance athletes with near-infrared spectroscopy. Med Sci Sports Exerc. 2013;45:869–75.
Hunter SK, Griffith EE, Schlachter KM, Kufahl TD. Sex differences in time to task failure and blood flow for an intermittent isometric fatiguing contraction. Muscle Nerve. 2009;39:42–53.
Kent-Braun JA. Skeletal muscle fatigue in old age: whose advantage? Exerc Sport Sci Rev. 2009;37:3–9.
Mota JA, Stock MS. Rectus femoris echo intensity correlates with muscle strength, but not endurance, in younger and older men. Ultrasound Med Biol. 2017;43:1651–7.
Zane AC, Reiter DA, Shardell M, Cameron D, Simonsick EM, Fishbein KW, et al. Muscle strength mediates the relationship between mitochondrial energetics and walking performance. Aging Cell. 2017;16:461–8.
Newman AB, Kupelian V, Visser M, Simonsick EM, Goodpaster BH, Kritchevsky SB, et al. Strength, but not muscle mass, is associated with mortality in the health, aging and body composition study cohort. J Gerontol A Biol Sci Med Sci. 2006;61:72–7.
Moro C, Bajpeyi S, Smith SR. Determinants of intramyocellular triglyceride turnover: implications for insulin sensitivity. Am J Physiol Endocrinol Metab. 2008;294:E203–13.
Ryan AS, Nicklas BJ. Age-related changes in fat deposition in mid-thigh muscle in women: relationships with metabolic cardiovascular disease risk factors. Int J Obes Relat Metab Disord. 1999;23:126–32.
Goodpaster BH, Carlson CL, Visser M, Kelley DE, Scherzinger A, Harris TB, et al. Attenuation of skeletal muscle and strength in the elderly: the health ABC study. J Appl Physiol. 2001;90:2157–65.
Goodpaster BH, Thaete FL, Kelley DE. Thigh adipose tissue distribution is associated with insulin resistance in obesity and in type 2 diabetes mellitus. Am J Clin Nutr. 2000;71:885–92.
Choi SJ, Files DC, Zhang T, Wang ZM, Messi ML, Gregory H, et al. Intramyocellular lipid and impaired myofiber contraction in normal weight and obese older adults. J Gerontol A Biol Sci Med Sci. 2016;71:557–64.
Lanza IR, Bhagra S, Nair KS, Port JD. Measurement of human skeletal muscle oxidative capacity by 31P-MR spectroscopy: a cross-validation with in vitro measurements. J Magn Reson Imaging. 2011;34:1143–50.
McCully KK, Fielding RA, Evans WJ, Leigh JS Jr, Posner JD. Relationships between in vivo and in vitro measurements of metabolism in young and old human calf muscles. J Appl Physiol. 1993;75:813–9.
Ryan TE, Brophy P, Lin CT, Hickner RC, Neufer PD. Assessment of in vivo skeletal muscle mitochondrial respiratory capacity in humans by near-infrared spectroscopy: a comparison with in situ measurements. J Physiol. 2014;592:3231–41.
Ryan TE, Southern WM, Reynolds MA, McCully KK. A cross-validation of near-infrared spectroscopy measurements of skeletal muscle oxidative capacity with phosphorus magnetic resonance spectroscopy. J Appl Physiol. 2013;115:1757–66.
Lagerwaard B, Nieuwenhuizen AG, de Boer VCJ, Keijer J. In vivo assessment of mitochondrial capacity using NIRS in locomotor muscles of young and elderly males with similar physical activity levels. Geroscience. 2020;42:299–310.
Niwayama M, Lin L, Shao J, Kudo N, Yamamoto K. Quantitative measurement of muscle hemoglobin oxygenation using near-infrared spectroscopy with correction for the influence of a subcutaneous fat layer. Rev Sci Instrument. 2000;71:4571–5.
Jones CJ, Rikli RE, Beam WC. A 30-s chair-stand test as a measure of lower body strength in community-residing older adults. Res Q Exer Sport. 1999;70:113–9.
Akima H, Hioki M, Yoshiko A, Koike T, Sakakibara H, Takahashi H, et al. Intramuscular adipose tissue determined by T1-weighted MRI at 3 T primarily reflects extramyocellular lipids. Magn Reson Imaging. 2016;34:397–403.
Kent-Braun JA, Ng AV, Young K. Skeletal muscle contractile and noncontractile components in young and older women and men. J Appl Physiol. 2000;88:662–8.
Sezgin M, Sankur B. Survey over image thresholding techniques and quantitative performance evaluation. J Electron Imaging. 2004;13:146–65.
Chung S, Rosenberry R, Ryan TE, Munson M, Dombrowsky T, Park S, et al. Near-infrared spectroscopy detects age-related differences in skeletal muscle oxidative function: promising implications for geroscience. Phys Reports. 2018;6: e13588.
Southern WM, Ryan TE, Kepple K, Murrow JR, Nilsson KR, McCully KK. Reduced skeletal muscle oxidative capacity and impaired training adaptations in heart failure. Phys Reports. 2015;3: e12353.
Lagerwaard B, Keijer J, McCully KK, de Boer VCJ, Nieuwenhuizen AG. In vivo assessment of muscle mitochondrial function in healthy, young males in relation to parameters of aerobic fitness. Eur J Appl Physiol. 2019;119:1799–808.
Hunter SK, Yoon T, Farinella J, Griffith EE, Ng AV. Time to task failure and muscle activation vary with load type for a submaximal fatiguing contraction with the lower leg. J Appl Physiol. 2008;105:463–72.
Rudroff T, Justice JN, Holmes MR, Matthews SD, Enoka RM. Muscle activity and time to task failure differ with load compliance and target force for elbow flexor muscles. J Appl Physiol. 2011;110:125–36.
Senefeld J, Yoon T, Hunter SK. Age differences in dynamic fatigability and variability of arm and leg muscles: associations with physical function. Exp Gerontol. 2017;87:74–83.
Kunz HE, Port JD, Kaufman KR, Jatoi A, Hart CR, Gries KJ, et al. Skeletal muscle mitochondrial dysfunction and muscle and whole body functional deficits in cancer patients with weight loss. J Appl Physiol. 2022;132:388–401.
Frontera WR, Ochala J. Skeletal muscle: a brief review of structure and function. Calcif Tissue Int. 2015;96:183–95.
Porter C, Reidy PT, Bhattarai N, Sidossis LS, Rasmussen BB. Resistance exercise training alters mitochondrial function in human skeletal muscle. Med Sci Sports Exerc. 2015;47:1922–31.
Irving BA, Lanza IR, Henderson GC, Rao RR, Spiegelman BM, Nair KS. Combined training enhances skeletal muscle mitochondrial oxidative capacity independent of age. J Clin Endocriol Metab. 2015;100:1654–63.
Shumway-Cook A, Brauer S, Woollacott M. Predicting the probability for falls in community-dwelling older adults using the Timed Up & Go Test. Phys Ther. 2000;80:896–903.
Ryan TE, Erickson ML, Verma A, Chavez J, Rivner MH, McCully KK. Skeletal muscle oxidative capacity in amyotrophic lateral sclerosis. Muscle Nerve. 2014;50:767–74.
Erickson ML, Ryan TE, Young H-J, McCully KK. Near-infrared assessments of skeletal muscle oxidative capacity in persons with spinal cord injury. Eur J Appl Physiol. 2013;113:2275–83.
Goodpaster BH, He J, Watkins S, Kelley DE. Skeletal muscle lipid content and insulin resistance: evidence for a paradox in endurance-trained athletes. J Clin Endocrinol Metab. 2001;86:5755–61.
Yoshiko A, Maeda H, Takahashi H, Koike T, Tanaka N, Akima H. Importance of skeletal muscle lipid levels for muscle function and physical function in older individuals. Appl Physiol Nutr Metab. 2022;47:649–58.
Gorgey AS, Dudley GA. Skeletal muscle atrophy and increased intramuscular fat after incomplete spinal cord injury. Spinal Cord. 2007;45:304–9.
Salvadego D, Domenis R, Lazzer S, Porcelli S, Rittweger J, Rizzo G, et al. Skeletal muscle oxidative function in vivo and ex vivo in athletes with marked hypertrophy from resistance training. J Appl Physiol. 2013;114:1527–35.
Berg OK, Kwon OS, Hureau TJ, Clifton HL, Thurston TS, Le Fur Y, et al. Skeletal muscle mitochondrial adaptations to maximal strength training in older adults. J Gerontol A Biol Sci Med Sci. 2020;75:2269–77.
Jubrias SA, Esselman PC, Price LB, Cress ME, Conley KE. Large energetic adaptations of elderly muscle to resistance and endurance training. J Appl Physiol. 2001;90:1663–70.
Hart CR, Layec G, Trinity JD, Liu X, Kim SE, Groot HJ, et al. Evidence of preserved oxidative capacity and oxygen delivery in the plantar flexor muscles with age. J Gerontol A Biol Sci Med Sci. 2015;70:1067–76.
Kemp GJ, Roberts N, Bimson WE, Bakran A, Harris PL, Gilling-Smith GL, et al. Mitochondrial function and oxygen supply in normal and in chronically ischemic muscle: a combined 31P magnetic resonance spectroscopy and near infrared spectroscopy study in vivo. J Vasc Surg. 2001;34:1103–10.
Southern WM, Ryan TE, Reynolds MA, McCully K. Reproducibility of near-infrared spectroscopy measurements of oxidative function and postexercise recovery kinetics in the medial gastrocnemius muscle. Appl Physiol Nutr Metab. 2014;39:521–9.
Acknowledgements
The authors thank all volunteers for their participation. The authors are also grateful to those who assisted with the MR data collection: Dr. Haruo Isoda and Mr. Akira Ishizuka (Brain & Mind Research Center, Nagoya University).
Funding
This work was supported by JSPS KAKENHI, Grant Number 20K19691, awarded to A.Y.
Author information
Authors and Affiliations
Contributions
Akito Yoshiko: conceptualization, data curation, formal analysis, investigation, methodology, writing—original draft preparation. Kana Shiozawa: data curation, writing, review and editing. Shiori Niwa: data curation, writing, reviewing, and editing. Hideyuki Takahashi: data curation, writing, reviewing, and editing. Teruhiko Koike: conceptualization, writing, reviewing, and editing. Kohei Watanabe: conceptualization, writing, review and editing. Keisho Katayama: conceptualization, methodology, writing, review and editing. Hiroshi Akima: conceptualization, methodology, writing, review and editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
Yoshiko, A., Shiozawa, K., Niwa, S. et al. Association of skeletal muscle oxidative capacity with muscle function, sarcopenia-related exercise performance, and intramuscular adipose tissue in older adults. GeroScience 46, 2715–2727 (2024). https://doi.org/10.1007/s11357-023-01043-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11357-023-01043-6