
Abstract
There are limited studies investigating the relationship between exposure to PM2.5 and the health status among the mobile population. A cross-sectional analysis was performed in a nationally representative sample (2017 China Migrants Dynamic Survey data) consisting of 169,469 mobile population. The ordered logistic regression model was used to examine the association between PM2.5 and the health status in mobile population. Stratified analyses were performed to identify whether the association varied across gender, age group, and regions in China. Overall, every 10 μg/m3 increment in annual average PM2.5 was associated with increased risk of poor self-reported health (OR = 1.021, 95% CI: 1.012–1.030). Mobile population aged 31–49 years and living in the central region suffers the highest PM2.5-associated health risk (OR = 1.030, 95% CI: 1.019–1.042; OR = 1.095, 95% CI: 1.075–1.116). Our study suggests that PM2.5 exposure was associated with an increased risk of poor self-reported health in mobile population, particularly among the population aged 31–49 years and people living in the central region of China. Policymakers should pay more attention to the vulnerable mobile population to tackle the health burden of ambient air pollution.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Ambient air pollution has aroused extensive public concern due to its adverse impacts on health (Han et al. 2021a, b, c). Among all ambient air pollutants, fine particulate matter (PM2.5, airborne particles less than or equal to 2.5 μm in aerodynamic diameter) is one of the most important pollutants that harm public health and has the highest exposure risk (Han et al. 2021a, b, c). In recent years, numerous epidemiological studies have demonstrated that long-term exposure to PM2.5 is closely related to the health status of residents (Yang et al. 2020, Han et al. 2021a, b, c). In addition, long-term or short-term exposure to ambient air pollution may lead to depression and anxiety; particularly, PM2.5 exposure was found with stronger associations with depression and anxiety (Kioumourtzoglou et al. 2017). Research shows that exposure to ambient air pollution contributed to an estimated 4.2 million deaths in 2015, of which 3.5 million were caused by exposure to fine particulate matter (PM2.5) (Thomson et al. 2020). It has been validated through various studies that exposure to PM2.5 pollution increases the risks of cardiovascular diseases (CVD), respiratory diseases, neurological diseases, and cancers (Yang et al. 2022) and has been regarded as one of the leading risk factors for disease burden (Han et al. 2021a, b, c). It is estimated that PM2.5 caused 4 million deaths worldwide and 142 million disability-adjusted life years (DALY) in 2017 (Bu et al. 2021) and has been identified as a primary pollution prevention goal by most countries.
Self-reported health (SRH) refers to a single-item health measurement in which individuals assess their health status according to a four or five-point scale from excellent to poor (Wu et al. 2013). Self-reported health is a subjective measurement method combining biological, psychological, social, and functional aspects, and they have been found to fully and objectively reflect physical and mental health, chronic diseases, and physical functioning (Lin et al. 2020), so it can represent the overall health level of the mobile population. The results of self-reported health can provide effective reference for healthy people and decision-making institutions. There are a few studies about the association between PM2.5 and SRH. There is a study using the logistic regression model to evaluate the association between air pollution and mental health and SRH in Belgium (Hautekiet et al. 2022). A nationwide longitudinal cohort study showed that long-term exposure to air pollution had significant negative effects on SRH in middle-aged and older adults, and the other longitudinal study cohort also showed that the SRH index decreases with the increase of outdoor PM2.5 (Goldberg et al. 2014; Ju et al. 2022). In addition, some researchers have conducted analyses focusing on the relationship between NO2 and SRH and the relationship between PM2.5 and health status based on data of the UK Biobank (Mutz et al. 2021).
The mobile population is a very important component in China, which is defined by the authority as people who choose to stay in the place temporarily for work, life, and other reasons but have not registered there, excluding individuals in cities (Cai et al. 2019; Zhou et al. 2019). According to the data of the National Bureau of Statistics, China’s urbanization rate rises from 17.92% in 1978 to 63.89% in 2020. At the same time, the scale of mobile population has reached 376 million, which is expected to continue to show an upward trend in the future and will exist as a special group for a long time (Cai et al. 2019; Song et al. 2022). The mobile population in China is similar to that in other countries, which are often called “migrant workers” (Slesinger 1992). It has been widely recognized in a series of previous studies that this group is usually young, of lower socioeconomic status, with often poor working conditions; thus, the mobile population is disadvantageous in health (Naing et al. 2012, Simkhada et al. 2017). There is necessity of further improving health status in the mobile population.
To our best knowledge, there is limited evidence on the association between PM2.5 and the SRH in Chinese mobile population. Therefore, the study aims to evaluate the relationship between PM2.5 exposure and SRH in the mobile population in China, especially exploring the association across different subgroups and identifying the susceptible population.
Methods
Data sources
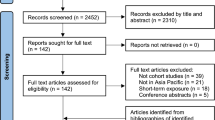
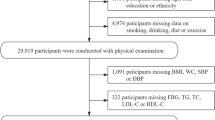
The 2017 China Migrants Dynamic Survey (CMDS) data published by the China Migration Population Service Center was used in the study (https://www.chinaldrk.org.cn). According to the random principle, the data was sampled using stratified, multistage, and scale proportional probability sampling (PPS) method. Questionnaires were used to complete a sample survey of the mobile population in 31 provinces and Xinjiang production and Construction Corps in China. The survey data covers the demographic characteristics, family status, settlement intentions, health, and social integration of the mobile population aged 15 and above who has lived in the inflow place for one month or more and is not registered in this district (county or city). In 2017, there were 169,989 valid samples of the mobile population. After removing the samples with missing PM2.5 exposure assessment data, 169,469 mobile persons (about 99.69%) of 338 cities were retained. The GDP per capita (PGDP) data in 2017 were collected from the Statistical Yearbook and the Statistical Bulletin of National Economic and Social Development of each city. Meteorological data used in the article (including annual average temperature and annual average relative humidity) were collected from the China Meteorological Data Sharing Service System (http://data.cma.gov.cn).
Measures
Self-reported health
In this study, we set “how is your health status” in the 2017 China Migrants Dynamic Survey data as the outcome variable, which is used to represent the general evaluation of the mobile population on their own health status. In order to truly and accurately reflect the SRH in mobile population, the classification and serial number of original code (including excellent or very good = 1, good = 2, fair or poor = 3, and unable to function independently = 4) were retained in the study.
PM2.5 exposure assessment
The spatiotemporal model based on satellite remote sensing, meteorological data, emission inventories, and land use information (Geng et al. 2021) was used to estimate ground-level PM2.5 concentrations at 0.1° × 0.1° (approximately 10 km × 10 km) spatial resolution from 2015 to 2017 (Han et al. 2022). We used the average value weighted by the population density of all grids within the city boundary to represent the PM2.5 concentration of each city (Renzi et al. 2019). We obtained the population density with a spatial resolution of 0.1° × 0.1° from the world gridded population (Brauer et al. 2015; CIESIN 2018). Finally, we averaged each city’s PM2.5 daily data of China to the annual average. In addition, we also obtained the annual average concentrations of O3 and NO2 in 2017 from the widely used gridded dataset by the same method (Geddes et al. 2016). Similarly, we also averaged the daily data to annual average.
Covariates
The factors affecting the health status of mobile population include demographic characteristics (age, gender, marital status, residential regions, and chronic diseases), socioeconomic factors (PGDP, education levels), and other environmental factors (temperature, relative humidity). In order to facilitate statistical analysis, some variables are remerged, grouped, and described. Among them, the education levels were divided into four categories (including primary and below, junior school, senior school/secondary specialized school, and college and above) in this study. The original marital status was divided into married and unmarried and others, according to whether there is a spouse. According to the 2017 China Migrants Dynamic Survey data, “are you suffering from hypertension or type II diabetes diagnosed by doctors” to respond to chronic diseases, and to facilitate statistics, the original categories were merged into none, hypertension/diabetes, hypertension, and diabetes. According to the existing research classification (Wang et al. 2012; Zhang et al. 2019), we divided China into three economic regions (eastern, central, and western regions). The specific classification results are shown in Fig. S1 and Table S1.
Statistical analysis
The demographic data, PM2.5, NO2, O3, temperature, relative humidity, and other related meteorological data were described by statistical charts and tables, and the factors were described as mean, median, standard deviation (SD), quartiles, and percentage. Spearman correlation was applied to assess the association between PM2.5, NO2, O3, meteorological factors, and demographic variables. Ordered logistic regression model was used to examine the association between PM2.5 and the health status of the mobile population after adjusting for the effects of temperature, relative humidity, and demographic variables. The effect of PM2.5 exposure on the risk of health was expressed by odds ratio (OR) and the 95% confidence interval (CI). Stratified analyses were performed to examine whether associations varied across gender, age, and region subgroups. Binary logistic regression model was also used to examine the association between PM2.5 and poor SRH as a dichotomous variable. Spatial distribution characteristics of PM2.5 concentration and health status of the mobile population were conducted with ArcGIS (version 10.8), and all data analyses were conducted with R software (version 4.1.3).
In the study, we set SRH as the dependent variable, and independent variable information was gathered on PM2.5, temperature, relative humidity, gender, age, PGDP, education levels, marital status, chronic diseases, and residential regions. The ordered logistic regression model is as the following three equations:
In the three equations, the dependent variable we study has four levels, so \({\pi }_{1},{\pi }_{2}{, \pi }_{3},\mathrm{ and }{\pi }_{4}\) are the probability of the corresponding value level, \({\pi }_{1}\), \({\pi }_{1}+{\pi }_{2}\), and \({\pi }_{1}+{\pi }_{2}+{\pi }_{3}\) are the cumulative probabilities of the ordered value levels of dependent variable, \(P\) is the number of independent variables, \(\alpha\) represents the constant term, and \({\beta }_{\mathcal{i}}\) represents the regression coefficients of their respective variables. In fact, this model divides the dependent variable into two levels according to different value levels and establishes a logistic regression model with the dependent variable as two categories for these two levels. No matter where the division point of the dependent variable in the model is, the coefficients of the respective variables in the model remain unchanged, and what is changed is only a constant term, which is one of the preconditions for fitting the cumulative logit model (Asare and Mensah 2020; Singh et al. 2020). Table S2 shows all categories of each variable included in the regression model.
Results
Descriptive statistics
Among the 169,469 mobile population we studied, the number of excellent or very good and good people accounted for 97.3%. The number of males was 87,600 (51.7%), and the number of females was 81,869 (48.3%). For education levels, 43.6% of the floating population attained junior school education, 22.0% of the floating population attained senior school/secondary specialized school education, and 17.4% of the floating population attained college and above education. 34.8%, 21.5%, and 43.7% of the floating population live in the western, central, and eastern regions, respectively. 82.0% of the floating population were married. In addition, the proportion of floating population without hypertension and diabetes was 94.6% (Table 1).
The demographic baseline characteristics, PM2.5, NO2, O3, and meteorological data of the mobile population are summarized in Table 2. The mean PM2.5 concentration from 2015 to 2017 was 51.81 μg/m3, 47.33 μg/m3, and 44.72 μg/m3, respectively. The mean concentration of NO2 was 35.70 ± 10.99 μg/m3 (range: 8.55–58.89 μg/m3). The mean value of O3 was 62.78 μg/m3, ranging from 37.50 μg/m3 to 104.43 μg/m3. The average temperature in 2015 and 2016 was 14.04 °C and 14.13 °C, and the average relative humidity in 2015 and 2016 was 67.51% and 67.95%, respectively. Temperature and relative humidity were from − 5.03 °C, 33.16% to 24.98 °C, 83.21%, respectively, in 2017. Among the mobile population, the maximum, minimum, and mean age were 96, 15, and 36.65 years old. The maximum value of PGDP was 358.8 thousand yuan (53,155.6 US dollars) per year, and the minimum value was 10.2 thousand yuan (1511.1 US dollars) per year. The average PGDP was 96.8 thousand yuan (14,340.7 US dollars) per year. The average residence time of the mobile population in the inflow area was 75.57 months, ranging from 2 to 827 months.
Spatial distribution of PM2.5 concentration and health status of the mobile population
There were obvious differences in the health status of the mobile population in different regions. The higher the health score means the worse the health status of the mobile population in this region. The western region was ranked first in terms of poor SRH, followed by the central region. The health status of the mobile population in the eastern region was relatively good, especially in Beijing, Shanghai, Jiangsu, Guangdong, etc. The average annual PM2.5 exposure ranged from 7.05 μg/m3 to 99.81 μg/m3 with large regional differences among the provinces and cities in China in 2017. In terms of spatial distribution patterns, the average value of PM2.5 exposure concentration (50.31 μg/m3) in the central region is relatively higher than that in the eastern (45.22 μg/m3) and western regions (40.63 μg/m3), and the air pollution is relatively severe (Figs. 1 and 2).

Health status of mobile population in China in 2017. Note: SRH, self-reported health

Spatial distribution characteristics of PM2.5 (μg/m3) concentration in China in 2017
Association between PM2.5 and SRH in the mobile population
The Spearman correlation analysis showed that PM2.5 was negatively correlated with O3, temperature, and relative humidity (\(P<0.01\)) and positively correlated with NO2 and PGDP (\(P<0.01\)). NO2 was negatively correlated with O3, temperature, and relative humidity (\(P<0.01\)) and positively correlated with PGDP (\(P<0.01\)). O3 was negatively correlated with temperature and relative humidity (\(P<0.01\)) and positively correlated with PGDP (\(P<0.01\)). Temperature was positively correlated with relative humidity and PGDP (\(P<0.01\)) (Table S3).
We used rank sum test to analyze the factors affecting the SRH of the mobile population. The results showed that PM2.5, temperature, relative humidity, gender, age, PGDP, education levels, marital status, and residential regions were statistically significant SRH-affected factors (\(P<0.05\)) (Tables S4 and S5).
The factors affecting the SRH of mobile population obtained by single factor analysis were analyzed further by ordered logistic regression. It was found that PM2.5, temperature, gender, age, PGDP, education levels, marital status, and residential regions were statistically significant (\(P<0.05\)). It was found that every 10 μg/m3 increment in annual average PM2.5 was associated with increased risk of poor SRH (OR = 1.021, 95% CI: 1.012–1.030). The risk of poor SRH of the mobile population living at or below 10 °C was 0.904 times (95% CI: 0.852–0.959) than that of living at or above 20 °C. The mobile population living at 10 °C–20 °C was 0.746 times (95% CI: 0.714–0.780) more likely to suffer poor SRH that of living at or above 20 °C. The risk of poor SRH of the mobile population living in 40%–60% humidity was 0.942 times (95% CI: 0.906–0.978) that of living in more than 60%. Mobile population of female, older age, lower PGDP, lower education level, unmarried and others, living in the central region is more vulnerable compared with other groups. Please see Table 3 for details.
Stratified analyses
Gender stratification analysis showed that the risk of poor SRH in male and female mobile population increased to 1.021 times (95% CI: 1.009–1.034) and 1.020 times (95% CI: 1.008–1.033) compared with the original for every 10 μg/m3 increment in annual average PM2.5. The results also showed that the association between PM2.5 and SRH was statistically significant, but there was no significant difference in the impact of PM2.5 on SRH between males and females. The results of the age-stratified analysis showed that the association between PM2.5 and SRH was statistically significant in the population aged 31–49. It was found that every 10 μg/m3 increment in annual average PM2.5 was associated with increased risk of poor SRH (OR = 1.030, 95% CI: 1.019–1.042). For the residential region stratification, the association between PM2.5 and SRH in the central and eastern regions was statistically significant, and the mobile population living in the central region suffers the highest PM2.5-associated health risk (OR = 1.095, 95% CI: 1.075–1.116). In addition, the differences between age and regional levels were statistically significant (Fig. 3).

Results of stratified analyses across gender, age, and region groups Note: OR, odds ratio, value corresponding to every 10 μg/m3 increment in annual average PM2.5; CI, confidence interval
Sensitivity analyses
To verify the practical significance of the impact of PM2.5 on the poor SRH of the mobile population, our study conducted several sensitivity analyses. First, to test the potential lag effects, we replaced the annual average PM2.5 data and meteorological data (including temperature and relative humidity) of the current year by using the data of 1–2 years before (with a 1-year lag and 2-year lag) based on the original model after removing the mobile population of residence time less than 24 months. The association between PM2.5 and poor SRH was robust to sensitivity analyses conducted. Second, NO2 and O3 were incorporated into the primary model, respectively; the same ordered logistic regression was performed to check the differences between sensitivity models and the primary model; the results showed that the risk effect of PM2.5 on poor SRH of the mobile population was still statistically significant in sensitivity models. Third, we included the residence time of the mobile population in the inflow area in the primary model to test its impact on PM2.5 exposure; the results showed that the PM2.5 risk effects of sensitivity analysis are close to the results from the primary model, indicating that the primary model fits well and stable (Table S6). Fourth, binary logistic regression model was also conducted and found similar results to the primary model (Table S7).
Discussion
This study evaluated the association between PM2.5 and SRH in the mobile population in China, using a nationally representative dataset. The principal findings revealed that the concentration of PM2.5 had a negative impact on the health status in the mobile population. Every 10 μg/m3 increment in annual average PM2.5 was associated with increased risk of poor SRH (OR = 1.021, 95% CI: 1.012–1.030).
There is limited evidence on the association between PM2.5 and the health status in the mobile population in China. There is only some relevant research about the association between PM2.5 and SRH based on general population. Although the degree of effects of PM2.5 on SRH is different across previous studies, the correlation directions are consistent. A national longitudinal cohort study (Ju et al. 2022) used the SRH score as the outcome variable and showed that the coefficient of PM2.5 is 0.060 based on the probit model analysis (0 = self-reported healthy, 1 = self-reported unhealthy), showing that the PM2.5 concentration is positively associated with the subject’s SRH condition score (the higher the score, the worse the SRH condition), which suggests that long-term exposure to air pollution had significant negative effects on SRH in middle-aged and older adults. Another study used the logistic regression model to evaluate the association between air pollution and mental health and SRH based on Belgium, and the answer categories of the SRH were dichotomized into good SRH and poor SRH. The results showed that every 3.8 μg/m3 (an interquartile range) increment in PM2.5 was associated with increased risk of poor SRH (OR = 1.20, 95% CI: 1.09–1.32) (Hautekiet et al. 2022). We conducted a sensitivity analysis using the binary logistic regression model, and the results showed that the effect value of PM2.5 on SRH in our study was slightly lower (OR = 1.02, 95% CI: 1.01–1.03) (Table S7). In addition, the study (Mutz et al. 2021) based on the analysis of UK Biobank showed that higher PM2.5 concentration was associated with lower odds of favorable SRH (OR = 0.97, 99.9% CI 0.94–0.99). Furthermore, a research based on a longitudinal study cohort showed that the SRH decreases with the increase of outdoor PM2.5 (Goldberg et al. 2014). The correlation directions of all the above results are consistent with our research.
In terms of stratified analyses, we found that there was no significant difference in the impact of PM2.5 on SRH between males and females, and the mobile population aged 31–49 years and living in the central region suffered the highest PM2.5-associated risk (OR = 1.030, 95% CI: 1.019–1.042; OR = 1.095, 95% CI: 1.075–1.116). For gender stratification analysis, a nationwide cohort study of 30,524 adults showed that males are more likely to suffer higher PM2.5-associated health risks (Liu et al. 2021). In addition, another cohort study also suggested that the adverse effects of PM2.5 are larger among males (Liu et al. 2022). There was no significant difference in the impact of PM2.5 on SRH between males and females in our study, which may be due to the similar working environment between males and females in the mobile population. In this case, there is little difference in PM2.5-related health effects between males and females. Considering age-stratified analysis, it has been widely recognized in a series of studies that the mobile population is usually a younger group aged 31–49, of lower education, with often poor working conditions (Naing et al. 2012; Simkhada et al. 2017). Similarly, we also found that the proportion of mobile population aged 31–49 and with junior school education is relatively high (about 52.9% and 43.6%). Furthermore, the lower educated people usually engage in the occupation more associated with higher pollution exposure due to their working environment, which may increase their sensitivity to air pollution (Han et al. 2021a, b, c). This group of populations may be with low level of health knowledge to prevent and address air pollution-related diseases, so they are more likely to suffer higher PM2.5-associated health risks. Thus, special attention and tailored interventions should be given to the most vulnerable population aged 31–49 years with low education.
Regarding the residential regions, we found that mobile population in the central region suffered the highest PM2.5-SRH risk than other regions. This is consistent with several studies that the highest-impacted regions were concentrated in the central district (Song et al. 2017; Yang et al. 2018; Xu et al. 2019). Previous studies from our team showed that an inverted U-shaped relationship between PM2.5 concentration and PGDP (urbanization) existed in China (Han et al. 2022). This means that the central region, which is more developed (PGDP and urbanization) than the west but less developed than the east, suffers the highest PM2.5-associated health risk. Moreover, the central region (50.31 μg/m3) had a higher PM2.5 exposure concentration than the eastern (45.22 μg/m3) and western (40.63 μg/m3) regions in 2017. An explanation for the protective effect of the eastern region may be that the eastern has a higher economic level and better health resources and services, which can effectively reduce the negative effect of PM2.5 on individuals’ health (Xiong et al. 2022). Thus, the relevant government departments should strengthen the prevention and control of PM2.5 in the central region, to reduce the PM2.5-associated health burden of the mobile population.
For demographic factors, the effects of gender, age, PGDP, residential regions, marital status, and education levels on the SRH in mobile population were statistically significant (P < 0.05), which is consistent with several studies (Moriconi and Nadeau 2015; Zhang et al. 2021). In terms of marital status, the family structure of married mobile population is complete; through family cooperation and family unity, they can better resist external risks and mental pressure when encountering difficulties (Fu et al. 2021). In addition, some studies reported that individuals who were widowed experience worse health than those whose spouse were still alive. They experienced the effects of bereavement, which had a negative impact on their health (Fu et al. 2021, Zhang et al. 2021). Therefore, the health status of married mobile population is better than that of unmarried and others. Generally, we usually use education and PGDP to represent a person’s socioeconomic status (Han et al. 2021a, b, c). Compared with people with high socioeconomic status, people with low socioeconomic status usually are more sensitive to poor SRH (Bor et al. 2017; Heggebø et al. 2019). A reasonable explanation for this phenomenon may be that mobile population with low socioeconomic status usually has poor working environment with low income and lacks knowledge to prevent and solve health-related issues (Han et al. 2021a, b, c). Therefore, the relevant government departments provide some policy support for the mobile population registered residence and school problems and give some policy care to their work and life, so as to improve the quality of life of mobile population to the greatest extent.
The present study has several strengths. Firstly, to the best of our knowledge, there is limited evidence on the association between PM2.5 and the health status in the mobile population in China. Therefore, our research can add more knowledge for future studies on health-related risk assessment of the mobile population. Secondly, the nationally representative data of the 2017 China Migrants Dynamic Survey has used the study; thus, the results are expected to be statistically robust and stable because of our large sample. Finally, our study estimated that the population aged 31–49 and the people living in central China had a stronger association between PM2.5 and poor SRH, which is highly significant for the policymakers to formulate the targeted preventive measures to reduce the health burden of the mobile population.
There are also several limitations. Firstly, our study cannot establish a cause-effect relationship between exposure to PM2.5 and the health status among the mobile population due to the cross-sectional study design. Secondly, the SRH belongs to the subjective judgment of the mobile population, and the use of the self-reported measurement would exist recall bias. We could not analyze some other individual-level confounding factors (such as income status and physical activity) due to the data being limited. Thirdly, ambient PM2.5 concentration at the city level in the study was used as an exposure estimate, and the indoor air quality and meteorological conditions were not taken into account due to limited data, which may reduce the correlation between PM2.5 and the health status of the mobile population. In addition, it is difficult to track the original residence information of the mobile population, so we did not further analyze the potential impact of their PM2.5 exposure before inflow here. However, although there is also limitation only focusing on the static exposure at the city level in annual average exposure compared with the local residents, it could not be big as the mobile population in this paper has lived in the district for 75.57 months averagely, ranging from 2 to 827 months.
Conclusions
The PM2.5 exposure is associated with increased risk of poor SRH of the mobile population, particularly among the population aged 31–49 years and the people living in central China. Our findings suggest that special attention and tailored interventions should be given to the vulnerable population, which includes the middle-aged population and the people living in central China, to assist them to tackle the health burden of ambient air pollution.
Data availability
The data that support the findings of this study are available upon request from the authors.
References
Asare I, Mensah A (2020) Crash severity modelling using ordinal logistic regression approach. Int J Inj Contr Saf Promot 27(4):412–419
Bor J, Cohen G, Galea S (2017) Population health in an era of rising income inequality: USA, 1980–2015. Lancet (london, England) 389(10077):1475–1490
Brauer M, Freedman G, Frostad J, Van Donkelaar A, Martin RV, Dentener F, Van Dingenen R, Estep K, Amini H, Apte JS (2016) Ambient air pollution exposure estimation for the global burden of disease 2013. Environ Sci Technol 50(1):79–88. https://doi.org/10.1021/acs.est.5b03709
Bu X, Xie Z, Liu J, Wei L, Wang X, Chen M, Ren H (2021) Global PM2.5-attributable health burden from 1990 to 2017: estimates from the Global Burden of Disease Study 2017. Environ Res 197:111123. https://doi.org/10.1016/j.envres.2021.111123
Cai X, Yang F, Bian Y (2019) Gap analysis on hospitalized health service utilization in floating population covered by different medical insurances: case study from Jiangsu Province, China. Int J Equity Health 18(1):84. https://doi.org/10.1186/s12939-019-0992-4
CIESIN (2018) Gridded Population of the World, version 4 (GPWv4): population density adjusted to match 2015 revision UN WPP country totals, revision 11. NASA Socioeconomic Data and Applications Center (SEDAC) Palisades, NY. https://doi.org/10.7927/H4F47M65
Fu Y, Lin W, Yang Y, Du R, Gao D (2021) Analysis of diverse factors influencing the health status as well as medical and health service utilization in the floating elderly of China. BMC Health Serv Res 21(1):438
Geddes J, Martin R, Boys B, van Donkelaar A (2016) Long-term trends worldwide in ambient NO2 concentrations inferred from satellite observations. Environ Health Perspect 124(3):281–289
Geng G-N, Xiao Q, Liu S, Liu X-D, Cheng J, Zheng Y, Xue T, Tong D, Zheng B, Peng Y, Huang X, He K, Zhang Q (2021) Tracking air pollution in china: near real-time PM2.5 retrievals from multisource data fusion. Environ Sci Technol 55(17):12106–12115. https://doi.org/10.1021/acs.est.1c01863
Goldberg MS, Wheeler AJ, Burnett RT, Mayo NE, Valois M-F, Brophy JM, Giannetti N (2014) Physiological and perceived health effects from daily changes in air pollution and weather among persons with heart failure: a panel study. J Eposure Sci Environ Epidemiol 25:187–199
Han C, Xu R, Gao C, Yu W, Zhang Y, Han K, Yu P, Guo Y, Li S (2021a) Socioeconomic disparity in the association between long-term exposure to PM and mortality in 2640 Chinese counties. Environ Int 146:106241
Han C, Xu R, Zhang Y, Yu W, Zhang Z, Morawska L, Heyworth J, Jalaludin B, Morgan G, Marks G, Abramson M, Sun L, Li S, Guo Y (2021) Air pollution control efficacy and health impacts: a global observational study from 2000 to 2016. Environ Pollut 287:117211 (Barking, Essex: 1987)
Han M, Yang F, Sun H (2021c) A bibliometric and visualized analysis of research progress and frontiers on health effects caused by PM. Environ Sci Pollut Res Int 28(24):30595–30612
Han C, Xu R, Ye T, Xie Y, Zhao Y, Liu H, Yu W, Zhang Y, Li S, Zhang Z, Ding Y, Han K, Fang C, Ji B, Zhai W, Guo Y (2022) Mortality burden due to long-term exposure to ambient PM2.5 above the new WHO air quality guideline based on 296 cities in China. Environ Int 166:107331
Hautekiet P, Saenen N, Demarest S, Keune H, Pelgrims I, Van der Heyden J, De Clercq E, Nawrot T (2022) Air pollution in association with mental and self-rated health and the mediating effect of physical activity. Environ Health: A Global Access Sci Sour 21(1):29
Heggebø K, Tøge A, Dahl E, Berg J (2019) Socioeconomic inequalities in health during the Great Recession: a scoping review of the research literature. Scandinavian J Public Health 47(6):635–654
Ju K, Lu L, Chen T, Duan Z, Chen D, Liao W, Zhou Q, Xu Z, Wang W (2022) Does long-term exposure to air pollution impair physical and mental health in the middle-aged and older adults? - A causal empirical analysis based on a longitudinal nationwide cohort in China. Sci Total Environ 827:154312
Kioumourtzoglou M, Power M, Hart J, Okereke O, Coull B, Laden F, Weisskopf M (2017) The association between air pollution and onset of depression among middle-aged and older women. Am J Epidemiol 185(9):801–809
Lin Y-H, Chen H-C, Hsu N-W, Chou P (2020) Validation of global self-rated health and happiness measures among older people in the Yilan study, Taiwan. Front Public Health 8:346. https://doi.org/10.3389/fpubh.2020.00346
Liu L, Luo S, Zhang Y, Yang Z, Zhou P, Mo S, Zhang Y (2021) Long-term exposure to fine particulate constituents and all-cause mortality in Chinese adults. Research Square. https://doi.org/10.21203/rs.3.rs-634789/v1
Liu L, Tian X, Zhao Y, Zhao Z, Luo L, Luo H, Han Z, Kang X, Wang X, Liu X, Guo X, Tao L, Luo Y (2022) Long-term exposure to PM and PM and chronic kidney disease: the Beijing Health Management Cohort, from 2013 to 2018. Environ Sci Pollut Res 30:17817–17827. https://doi.org/10.1007/s11356-022-23251-x
Moriconi PA, Nadeau L (2015) A cross-sectional study of self-rated health among older adults: association with drinking profiles and other determinants of health. Curr Gerontol Geriatr Res 2015:352947. https://doi.org/10.1155/2015/352947
Mutz J, Roscoe CJ, Lewis CM (2021) Exploring health in the UK Biobank: associations with sociodemographic characteristics, psychosocial factors, lifestyle and environmental exposures. BMC Med 19(1):240. https://doi.org/10.1186/s12916-021-02097-z
Naing TT, Geater AF, Pungrassami P (2012) Migrant workers’ occupation and healthcare-seeking preferences for TB-suspicious symptoms and other health problems: a survey among immigrant workers in Songkhla province, southern Thailand. BMC Int Health Hum Rights 12:22–22
Renzi M, Forastiere F, Schwartz J, Davoli M, Stafoggia M (2019) Long-term PM10 exposure and cause-specific mortality in the Latium region (Italy): a difference-in-differences approach. Environ Health Perspect 127(6):067004
Simkhada P, Regmi P, van Teijlingen E, Aryal N (2017) Identifying the gaps in Nepalese migrant workers’ health and well-being: a review of the literature. J Travel Med 24(4). https://doi.org/10.1093/jtm/tax021
Singh V, Dwivedi S, Deo S (2020) Ordinal logistic regression model describing factors associated with extent of nodal involvement in oral cancer patients and its prospective validation. BMC Med Res Methodol 20(1):95
Slesinger DP (1992) Health status and needs of migrant farm workers in the United States: a literature review. J Rural Health: Official J Am Rural Health Assoc Natl Rural Health Care Assoc 8(3):227–234
Song C, He J, Wu L, Jin T, Chen X, Li R, Ren P, Zhang L, Mao H (2017) Health burden attributable to ambient PM2.5 in China. Environ Pollut 223:575–586
Song Y, Zhu N, Luo F (2022) City size and permanent settlement intention: evidence from rural-urban migrants in China. Int J Environ Res Public Health 19:676. https://doi.org/10.3390/ijerph19020676
Thomson E, Christidis T, Pinault L, Tjepkema M, Colman I, Crouse D, van Donkelaar A, Martin R, Hystad P, Robichaud A, Ménard R, Brook J, Burnett R (2020) Self-rated stress, distress, mental health, and health as modifiers of the association between long-term exposure to ambient pollutants and mortality. Environ Res 191:109973
Wang K, Wei Y-M, Zhang X (2012) A comparative analysis of China’s regional energy and emission performance: which is the better way to deal with undesirable outputs? Energy Policy 46:574–584
Wu S, Wang R, Zhao Y, Ma X-Q, Wu M-J, Yan X, He J (2013) The relationship between self-rated health and objective health status: a population-based study. BMC Public Health 13:320–320
Xiong Y, Xue Y, Jiao G, Xie J, Cheng J (2022) Comparative analysis of the status and influencing factors of immunization among children between registered and floating population. Front Public Health 10:872342
Xu L, Chen F, Zhong X, Zhang LE, Ye R, Cai W, Rao Q, Li J (2019) Spatial disequilibrium of fine particulate matter and corresponding health burden in China. J Clean Prod 238:117840. https://doi.org/10.1016/J.JCLEPRO.2019.117840
Yang Z, Mahendran R, Yu P, Xu R, Yu W, Godellawattage S, Li S, Guo Y (2022) Health Effects of long-term exposure to ambient PM in Asia-Pacific: a Systematic review of cohort studies. Curr Environ Health Rep 9(2):130–151
Yang Y, Luo L, Song C, Yin H, Yang J (2018) Spatiotemporal assessment of PM2.5-related economic losses from health impacts during 2014–2016 in China. Int J Environ Res Public Health 15:1278. https://doi.org/10.3390/ijerph15061278
Yang Y, Qi J, Ruan Z, Yin P, Zhang S, Liu J, Liu Y, Li R, Wang L, Lin H (2020) Changes in life expectancy of respiratory diseases from attaining daily PM2.5 standard in China: a nationwide observational study. Innovation(Camb) 1(3):100064. https://doi.org/10.1016/j.xinn.2020.100064
Zhang Y-L, Wu B, Chen P, Guo Y (2021) The self-rated health status and key influencing factors in middle-aged and elderly. Medicine (Baltimore) 100(46):e27772. https://doi.org/10.1097/MD.0000000000027772
Zhang Z, Shao C, Guan Y, Xue C (2019) Socioeconomic factors and regional differences of PM health risks in China. J Environ Manage 251:109564
Zhou Y, Wang T, Fu J, Chen M, Meng Y, Luo Y (2019) Access to reproductive health services among the female floating population of childbearing age: a cross-sectional study in Changsha, China. BMC Health Serv Res 19(1):540
Acknowledgements
We thank the Migration Population Service Center for providing the floating population data. Thanks to Dr. Rongbin Xu of Monash University in Melbourne, Australia, for his revision.
Funding
This study is funded by the Social Science Planning Research Project of Shandong Province (20BGLJO1).
Author information
Authors and Affiliations
Contributions
Chunlei Han, Guangcheng Wang, and Yang Zhao contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Yukun Shi, Haiyun Liu, Luyang Wang, Junyan Liu, Haotian Chen, Baoshun Yang, Haifeng Shan, Shijia Yuan, and Wenhui Gao. The first draft of the manuscript was written by Yukun Shi, Yang Zhao, and Hongyu Li. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
None declared.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Responsible Editor: Lotfi Aleya
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Yukun Shi and Yang Zhao are co-first authors.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Shi, Y., Zhao, Y., Li, H. et al. Association between exposure to ambient PM2.5 and the health status in the mobile population from 338 cities in China. Environ Sci Pollut Res 30, 63716–63726 (2023). https://doi.org/10.1007/s11356-023-26453-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-023-26453-z