
Abstract
Extreme temperature is closely associated with human health, but limited evidence is available for the effects of extreme temperatures on respiratory diseases in China. The goal of this study is to evaluate the effects of extreme temperatures on hospital emergency room (ER) visits for respiratory diseases in Beijing, China. We used a distributed lag non-linear model (DLNM) coupled with a generalized additive model (GAM) to estimate the association between extreme temperatures and hospital ER visits for different age and gender subgroups in Beijing from 2009 to 2012. The results showed that the exposure-response curve between temperature and hospital ER visits was almost W-shaped, with increasing relative risks (RRs) at extremely low temperature. In the whole year period, strong acute hot effects were observed, especially for the elders (age > 65 years). The highest RR associated with the extremely high temperature was 1.36 (95% CI, 0.96–1.92) at lag 0–27. The longer-lasting cold effects were found the strongest at lag 0–27 for children (age ≤ 15 years) and the relative risk was 1.96 (95% CI, 1.70–2.26). We also found that females were more susceptible to extreme temperatures than males.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Climate change draws a wide concern and has enormous impacts on public health. The frequency of extreme weather intensified with the rising of global surface temperature, which brings a great challenge to the environment and public health (IPCC 2013). Extreme weather events showed significant impacts on human health, and the effects often lasted for 14 days (Braga et al. 2001) or 40 days (Zanobetti et al. 2003). Numerous epidemiological studies have linked extreme temperatures with overall mortality (Hajat and Kosatsky 2010; O'Neill and Ebi 2009; Kovats and Hajat 2008), cardiovascular diseases (Bhaskaran et al. 2009; Basu 2009), and heart diseases (Moran et al. 2010; Stewart et al. 2010). Previous studies performed in North America (Knowlton et al. 2009; Lin et al. 2009), Europe (Curtis et al. 2017; Tataru et al. 2006; Johnson et al. 2005), and Australia (Huang et al. 2012) have proved the effect of extreme temperatures on health. In mainland China, the relationship between extreme temperatures and health has been investigated in several large cities, such as Beijing (Song et al. 2017; Wang et al. 2015), Shanghai (Guo et al. 2012; Ma et al. 2014), and Guangzhou (Yang et al. 2013). Some studies suggested that the effects of extreme temperatures can be delayed by weeks, especially for cold effects (Goldberg et al. 2011; Rocklöv and Forsberg 2008).
Previous studies found that the exposure-response curve between temperature and mortality generally was U-, J-, or V-shaped, with increased mortality risks at both high and low temperatures (Curriero et al. 2002; McMichael et al. 2008). Gasparrini et al. (2010) proposed a distributed lag non-linear model (DLNM), taking the lag effect of exposure factors into account. The non-linear relationship of the exposure-response showed that it was possible to estimate the health effect of changing the temperature by 1 °C (Kim et al. 2006). Basu (2009) found that elevated temperature increased the risk of respiratory mortality. Study in England and Wales showed that the relative risks (RRs) of the total death were 1.03 (95% CI, 1.02–1.13) and 1.06 (95% CI, 1.05–1.06) for each 1 °C higher than the thermal threshold and lower than the cold threshold respectively (Hajat et al. 2007). Numerous studies have reported the adverse effects of temperature on respiratory diseases, and most of those studies regarded mortality as a health measure (Basu 2009; Hajat et al. 2007). Extreme temperatures, both with respect to heat and cold, substantially increase the risk of disease and death (Diaz et al. 2002). A study in Taiwan showed that after accounting for 4-day cumulative temperature effect, the relative risks of emergency room (ER) visits for respiratory diseases were found to be associated with extreme cold at 1st percentile lasting for > 3 days (Wang et al. 2012). A study of the number of hospital admissions in Lhasa showed that people older than 65 years and men were more susceptible to high temperatures (Bai et al. 2014). Moreover, medical situation may confer susceptibility to extreme temperatures (Davídkovová et al. 2014; Lin et al. 2013). Some studies have estimated the association between extremely low and high temperatures and cardiovascular mortality (Guo et al. 2011; Goggins et al. 2013), but few study on the effects of extreme temperatures on ER visits for respiratory diseases.
In this study, we employed a distributed lag non-linear model to evaluate the effects of extreme temperatures on ER visits for respiratory diseases in Beijing, China. Moreover, we also performed age- and gender-specific analysis. Findings of this study may help to develop relevant preventive interventions for the government and provide a scientific basis for the prediction and guidance of medical meteorology in Beijing.
Materials and methods
Study area
Beijing (116ingls and nd gu, the capital of China, has over 21.8 million permanent residents in 2015. The local climate belongs to a typical temperate semi-humid and continental monsoon climate. Four seasons are distinct, with hot and rainy, summer and cold, and dry winter. Spring and autumn are relatively short and comfortable. The annual average temperature is between 10 and 15 °C. The diurnal variation of temperature is large.
Daily respiratory visits
Daily number of emergency room (ER) visits for respiratory diseases were collected from four large general top-level hospitals in Beijing from January 1, 2009, to December 31, 2012. We choose the hospitals because they have a good reputation for the diagnosis and treatment of respiratory diseases. The data contains the date of visits, gender, age, diagnosis codes, etc. Clinic symptoms were encoded in terms of the 10th International Classification of Diseases (ICD-10: J00–J99), in which the respiratory diseases were examined and classified.
Meteorological data and air pollution data
Daily data of average temperature, maximum and minimum temperatures, sunshine time, wind speed, and relative humidity during 2009–2012 were obtained from Beijing Meteorological Bureau. Daily air pollution data were collected from Environmental Observation Center, including particulate matter less than 10 μm in aerodynamic diameter (PM10), sulfur dioxide (SO2), and nitrogen dioxide (NO2).
Statistical analysis
Considering the existence of simultaneously non-linearity and lag effects in the relationship between temperature and respiratory diseases, we made use of the distributed lag non-linear model (DLNM) combined with a Poisson regression to evaluate the effects of extreme low and high temperatures on hospital ER visits for respiratory diseases. The DLNM consists of two functions, including “crossbasis” function and “crosspred” function. The two functions are used for the study of lag effect and prediction respectively, allowing the model to estimate the exposure-response prediction across the maximum lag period. In order to determine the outcomes (ER visits) of time series, the general model representation is shown below:
The DLNM combined with generalized additive model (GAM) was employed in our study. In the model, log function is applied as the link function; E(Y) is the estimated daily number of ER visits; a is the intercept; basis.temp is a matrix obtained by applying the DLNM to daily mean temperature, β is vector of coefficients for basis.temp; s(x, df) indicates the natural cubic spline function for x with a certain df; and df is the degree of freedom. Cubic spline functions were used to control the long-term and seasonal trends. We also accounted for the effects of DOW (day of the week) and Holiday (dummy argument variate) as linear variates, where λ and η represent vector of coefficients of DOW and Holiday respectively. After controlling these variables, a maximum lag of 27 days was set to estimate the delayed effect of daily mean temperature on the ER visits. We fitted both the non-linear temperature effect and the lag effect in DLNM; the minimum value of the Akaike information criterion (AIC) was used to examine the df for daily mean temperature and lags. In the final model, 5 df and 4 df were used respectively when setting spline knots at equal intervals in the temperature range and in the log scale of lags. The mean temperature was interpreted as the reference temperature (i.e.,“centering value”) for the three-dimensional plot (Yi and Chan 2015).
We also conducted a stratified analysis on gender and age. The extremely low temperature was defined as the 1st percentile of the daily mean temperature, and the extremely high temperature was defined as 99th percentile of the daily mean temperature. The RRs for the number of ER visits were calculated for cold effects at the extremely low temperature compared with the 10th percentile of daily mean temperature and for hot effects at the extremely high temperature compared with the 90th percentile of daily mean temperature (Guo et al. 2013). We also conducted the lag effects of 0, 0–3, 0–14, and 0–27 to estimate the cumulative effects of extreme temperatures on ER visits.
Sensitivity analyses were performed by altering the df for temperature, time trend, and the maximum lag day, as well as the confounding elements including meteorological and pollutant elements in the model, taking all age groups of outpatients as the example. In addition, models were also refitted using the 25th and 75th percentiles of daily mean temperature to evaluate cold and hot effects respectively for the sensitive analysis. The DLNM and MGCV packages in R software (version 3.3.1) were used to fit all the models.
Results
During the study period between 2009 and 2012 (1461 days), 0.27 million hospital ER visits for respiratory diseases were recorded in Beijing, accounting for 22.5% of the total. The descriptive analysis was shown in Table 1. The daily mean ER visits were 188, and more males were reported. There were 117 ER visits aged 16–65 years, accounting for the biggest proportion in all respiratory diseases.
Table 2 demonstrates the descriptive statistics for meteorological factors and air pollutants. The average daily mean temperature was 13.1 °C (range, − 12.5 °C to 34.5 °C), and relative humidity was 50.8% (range, 0.0 to 97.0%). The mean concentrations of SO2, NO2, and PM10 were 26.6 μg/m3, 57.1 μg/m3, and 114.4 μg/m3 respectively.
Table 3 shows the Spearman correlation between meteorological elements and pollutants. The daily average temperature has a significant positive correlation with sunshine hours, relative humidity, and PM10 and has a significant negative correlation with SO2 and NO2.
Figure 1 indicates the exposure-response curve between daily mean temperature and relative risks of respiratory ER visits. The curve is W-shaped, with the highest RR of 3.70 (95% CI, 2.94–4.63) at − 12.5 °C and RR of 1.33 (95% CI, 1.26–1.40) at 7 °C. The RRs rise sharply in extreme temperature of cold than hot.

Exposure-response between daily mean temperature and relative risks of hospital ER visits between 2009 and 2012 (solid red line) and 95% confidence intervals (gray area), using 5 df for temperature and 4 df for lag. The reference temperature was 13.1 °C
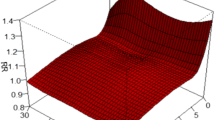
Figure 2 shows the three-dimensional plots of the relationship between mean temperature and hospital ER visits along 27 lag days. Comparing the RRs for mean temperature with the reference mean temperature of 13.1 °C, the age-specific temperature-RR curves were non-linear and high RRs were observed at low and high temperatures. For all age groups, both cold and hot effects showed positive associations. The cold effect became predominant with a lag of 3 days and showed a longer-lasting effect of more than 27 days, while the hot effect has a strong immediate positive effect and decreased from lag 0 to lag 5. Then it was almost no change after 5 days, showing a shorter and acute effect. For aged ≤ 15 years, low temperature had delayed effect of 3 days and the cold effects increased all the time, whereas the hot effects reached the peak at lag 0. For those aged 15–65 years, the lagged cold effect and the immediate hot effect were still significant, but the RRs were observed quite high at 7 °C for aged 16–65 years.

The three-dimensional graph of the relative risks for different ages (A–D: all ages, age ≤ 15 years, aged 16~65 years, age ˃ 65 years) by mean temperature along 27 lag days in Beijing, 2009–2012. Using a 5-df natural cubic spline for temperature and 4 df for lag
Figure 3 presents the estimated cumulative effects of daily mean temperature on ER visits for different age groups. The temperature-RR curves demonstrated both the shorter-time (lag 0, lag 0–3) and longer-time (lag 0–14, lag 0–27) effects on ER visits for respiratory diseases. Effects of both lower and higher temperatures were non-linear. For lag 0 and lag 0–3, the cumulative cold effects on age-specific ER visits were observed lower than lag 0–14 and lag 0–27, while the cumulative hot effect was higher than lag 0–14 and lag 0–27. In particular, the cumulative effect of 7 °C increased with lag days.

The estimated cumulative effect of daily mean temperature on hospital ER visits for different ages (age ≤ 15 years, aged 16~65 years, age > 65 years) at lag 0, lag 0–3, lag 0–14, and lag 0–27. The smooth red lines are the maximum likelihood estimate of RR, and the gray regions are the pointwise 95% confidence intervals (CI). The reference temperature is 13.1 °C
Figure 4 indicates the extreme cold and hot effects of the 1st percentile and the 99th percentile of daily mean temperature on respiratory diseases. It indicated that the cold effects delayed 3 days, and the strong impact lasted more than 20 days. The hot effects on respiratory diseases showed the strongest on lag 0 day, then gradually decreased and disappeared after 2 days.

Extreme cold and hot effects by lag at 1st (cold effect, − 7.9 °C) and 99th (hot effect, 30.8 °C) percentiles of temperature distribution from 2009 to 2012 in Beijing. The reference temperature was 13.1 °C
Table 4 demonstrates the cumulative cold and hot effects on age-specific hospital ER visits at lag 0, lag 0–3, lag 0–14, and lag 0–27. The cumulative hot effects were statistically significant at lag 0 and lag 0–3. The cumulative hot effect was the strongest in aged > 65 years, and the largest RR was 1.36 (95% CI, 0.96–1.92) at lag 0–27. Hot effects on children and those aged 16–65 years were much smaller than those on the elderly. The cumulative cold effects showed protective effects for all ages at lag 0 and lag 0–3. While for longer-time effects, children (age ≤ 15 years) were most susceptible to the cold effects at lag 0–14 and lag 0–27, and the highest RR with extremely low temperatures was 1.96 (95% CI, 1.70–2.26) at lag 0–27. Cumulative cold effects also showed a higher RR at lag 0–27 on adults (age 16–65 years).
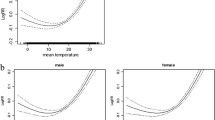
Figure 5 indicates the overall relative risks of the cumulative cold and hot effects along lag days for different genders. Females had more acute response to cold effects than males, although the RRs were almost the same after 2 weeks. While for the hot effects, females presented obviously higher RRs comparing to males. The hot effects on males lasted 8 days, while hot effects on females lasted at least 27 days.

Cumulative cold and hot effects of temperature on gender-specific respiratory ER visits and associated 95% confidence intervals (95% CI) along lag days in Beijing, China, 2009–2012
Sensitivity analysis
Sensitivity analysis was performed by changing df (4, 5, 6, and 7) for daily mean temperature with natural cubic spline function in the DLNM (Figure A1). The estimated relationship between ambient temperature and ER visits for respiratory diseases did not substantially change. Moreover, we also used different maximum lag days for mean temperature (Figure A2) and different df per year (from 6 to 13) for long-time trend (Figure A3) to fit the model, which gave the similar result. Furthermore, when excluding air pollution or meteorological factors or both of them in the DLNM, the result was still similar to the original estimates (Figure A4). In order to maintain completeness, we included all the above factors in the DLNM.
We also calculated the hot effect by comparing the 99th percentile of temperature with the 75th percentile of temperature, while the cold effect was calculated by comparing the 1st percentile of temperature with the 25th percentile of temperature, indicating the similar results to the original estimates (Table A1). Results of sensitivity analysis were shown in the supplementary material.
Discussion
We studied the effect of extreme temperature on age- and gender-specific ER visits for respiratory diseases in Beijing, China, during 2009–2012. The relationship between daily mean temperature and ER visits was almost W-shaped for all ages, with increased RR at low temperature. Strong hot and cold effects were observed in the whole year in Beijing. Children (age ≤ 15 years) were the most susceptible to extremely low temperature, while the elders (age > 65 years) were the most vulnerable to extremely high temperature. Associations between high temperature and ER visits were found acutely and strongly, while that between low temperatures were observed after 3 days and of longer duration. In terms of gender, females were more sensitive to extreme high and low temperature than males.
Previous studies showed that the temperature-mortality curve was almost U-shaped or J-shaped around the world (Anderson and Bell 2009; Martin et al. 2012; Guo et al. 2013; Ma et al. 2014), and it varied greatly by climate, geography, and society (Yu et al. 2011a; Son et al. 2011). In our study, the association between daily mean temperature and ER visits was W-shaped. This result is consistent with the results performed in Tianjin (Ma et al. 2014) and Hong Kong (Yi and Chan 2015) in China. Except for the high RR at low temperature in the W-shape, a high value of cumulative effect of around 7 °C was also observed. This result agrees with the results reported in Tibet (Bai et al. 2014) and Taiwan (Wang et al. 2012) although the temperature of high RR was various. A study in Suzhou showed a high estimated RR of daily mean temperature on respiratory mortality at around 20 °C (Wang et al. 2014). A similar study conducted in 17 large cities in mainland China suggested a high RR around 13 °C (Ma et al. 2014). However, previous studies in Bavaria, Germany (Breitner et al. 2014), and Valencia, Spain (VicedoCabrera et al. 2014) did not show the characteristic structure. The differences of the temperature corresponding to high RR are likely because of the transition and change of seasons among each area. The high RR at different temperatures also might be due to the selection of different dataset of morbidity or mortality. This finding is still not very clear and needs further investigation.
Our study performed DLNM up to 27 days to estimate the lag effects of ambient temperature on age-specific ER visits. We found high temperature had acute and shorter-term effect on ER visits, while low temperature had delayed and long-lasting effect. Many previous studies have reported similar lag effects of hot temperature in Germany (Breitner et al. 2014), Australia (Turner et al. 2012), Canada (Goldberg et al. 2011), and mainland China (Bai et al. 2014; Yi and Chan 2015). However, the impact of low temperature on respiratory ER visits was apparently prolonged. We found that cold effect lasted nearly 27 days or more, which is consistent with the studies in Chile, Italy (Muggeo and Hajat 2009), and the Netherlands (Huynen et al. 2001). Similar to our findings, previous studies suggested that the effects of extreme temperatures can be delayed by weeks, especially for cold weather (Goldberg et al. 2011; Rocklöv and Forsberg 2008). A study conducted in Santiago, Chile, and Palermo, Italy, suggested that slightly negative risk estimates associated with cold exposure at very long lags (days 25–50 after exposure) (Muggeo and Hajat 2009). Goodman et al. working in Dublin reported that heat and cold effects are up to 40 days after exposure and found that cold effects mostly occurred within the first 3 weeks of exposure (Goodman et al. 2004). Braga et al reported that in the USA, cold effects had mostly disappeared by a lag period of about 20 days (Braga et al. 2001). Guo et al. (2011) also suggested that longer lags should be required to examine the cold impact in case of ignoring harvesting effect and underestimating the cold effect.
Our results showed that the cumulative hot effect of temperature has the greatest impact on elderly people (age > 65 years). A previous study in the Philippines also suggested that the elderly had the greatest risk of temperature-related mortality (Seposo et al. 2015). This might be due to the fact that the body function and adaptability of the elderly are gradually decreasing with age (D’Ippoliti et al. 2010; Son et al. 2012; Basu and Ostro 2008; Michelozzi et al. 2009). The cumulative cold effect had greater and longer impacts on children (age ≤ 15 years). A greater susceptibility to lower temperature effects was also found in Sao Paulo, Brazil (Gouveia et al. 2003) and Manila, Philippines (Seposo et al. 2015). Vulnerability of children to cold effect might be due to the following: (i) children are more sensitive to extreme temperatures because of their greater metabolic rate (Bunyavanich et al. 2003) and (ii) for children, asthma is the most common chronic illness in childhood and cold weather can be a trigger to asthma symptom like coughing, wheezing, shortness of breath, and tightness in the chest (Mireku 2009).
Many previous studies have pointed out that the magnitude of the effect of temperature on human beings varies from population to population (Curriero et al. 2002; Revich and Shaposhnikov 2008; Iniguez et al. 2010; Yu et al. 2011b). The cold and hot effects of extreme temperatures on the hospital ER visits for respiratory diseases in the current study were less than the results performed in the mainland cities of Suzhou (Wang et al. 2014) and Guangzhou (Luo et al. 2014) in China. This might be attributed to the hotter summer and no heating suppling winter of Suzhou and Guangzhou.
Our findings confirmed that females were more vulnerable to both high and low temperatures compared to males, which agrees with those of previous studies (D’Ippoliti et al. 2010; Son et al. 2012; Xiang et al. 2014). But, studies conducted in mainland China (Yang et al. 2012), the USA (Medina-Ramón et al. 2006), and Europe (Stafoggia et al. 2006; Hajat et al. 2007) reported that females were more susceptible to hot but not cold weather than males. Sex-related differences may be dependent on physiology and socioeconomic factors (Ma et al. 2015; Zeng et al. 2014) and need further investigation.
Some limitations of our work should be noticed: (a) some studies classified respiratory diseases, such as bronchitis, asthma, and influenza, and also made the classification statistics for the outpatient profession and educational level (Qiu et al. 2015; Kan et al. 2008), in which we will launch more researches and (b) data we used exists limitation in a certain degree. The meteorological element information was only derived from a platform of Beijing, which cannot reflect the average situation of Beijing. And, the hospital ER visits data were collected from four hospitals, which may not include all the residents as potential patients, but these bias could not be completely eliminated due to many practical factors.
Conclusion
Our study showed that extreme temperatures have adverse effects on the number of hospital ER visits for respiratory diseases. The effect of hot effect is more acute and strong, while the cold effect is observed after 3 days and longer duration. Children are mostly susceptible to extremely low temperature, while the elders are the most vulnerable to extremely high temperature. In addition, females are more susceptible to extreme temperature than males. These results can provide useful information for the local government to develop relevant preventive interventions to extreme temperatures and develop public health strategies in Beijing, China.
References
Anderson BG, Bell ML (2009) Weather-related mortality: how heat, cold, and heat waves affect mortality in the United States. Epidemiology 20:205–213
Bai L, Cirendunzhu, Woodward A, Dawa, Zhaxisangmu, Chen B, Liu QY( 2014) Temperature, hospital admissions and emergency room visits in Lhasa, Tibet: a time-series analysis. Science of the Total Environment. 490, 838–848.
Basu R (2009) High ambient temperature and mortality: a review of epidemiologic studies from 2001 to 2008. Environ Health 8:40
Basu R, Ostro BD (2008) A multicounty analysis identifying the populations vulnerable to mortality associated with high ambient temperature in California. Amer J Epidemiol 168:632–637
Bhaskaran K, Hajat S, Haines A, Herrett E, Wilkinson P (2009) Effects of ambient temperature on the incidence of myocardial infarction. Heart 95(21):1760
Braga AL, Zanobetti A, Schwartz J (2001) The time course of weather-related deaths. Epidemiology 12(6):662–667
Breitner S, Wolf K, Devlin RB, DiazSanchez D, Peters A, Schneider A (2014) Short-term effects of air temperature on mortality and effect modification by air pollution in three cities of Bavaria, Germany: a time-series analysis. Sci Total Environ 485–486(1):49–61
Bunyavanich S, Landrigan CP, McMichael AJ (2003) The impact of climate change on child health. Ambul Pediatr 3:44–52
Curriero FC, Heiner KS, Samet JM, Zeger SL, Strug L, Patz JA (2002) Temperature and mortality in 11 cities of the eastern United States. Am J Epidemiol 155:80–87
Curtis S, Fair A, Wistow J, Val DW, Oven K (2017) Impact of extreme weather events and climate change for health and social care systems. Environ Health, 16(suppl 1), 128: 24–32.
D’Ippoliti D, Michelozzi P, Marino C, De’Donato F, Menne B, Katsouyanni K, Kirchmayer U, Analitis A, Medina-Ramón M, Paldy A (2010) The impact of heat waves on mortality in 9 European cities: results from the EuroHEAT project. Environ Health 9(1):37
Davídkovová H, Plavcová E, Kynˇcl J, Kyselý J (2014) Impacts of hot and cold spells differ for acute and chronic ischaemic heart diseases. BMC Public Health 14(1):480
Diaz J, Garcia R, Velazquez de Castro F, Hernandez E, Lopez C (2002) Effects of extremely hot days on people older than 65 years in Seville (Spain) from 1986 to 1997. Int J Biometeorol 46:145–149
Gasparrini A, Armstrong B, Kenward MG (2010) Distributed lag non-linear models. Stasistics in Medicine 29, 2224–2234.
Goggins WB, Chan EY, Yang C, Chong M (2013) Associations between mortality and meteorological and pollutant variables during the cool season in two Asian cities with sub-tropical climates: Hong Kong and Taipei. Environ Health 12(1):59
Goldberg MS, Gasparrini A, Armstrong B, Valois MF (2011) The short-term influence of temperature on daily mortality in the temperate climate of Montreal, Canada Environmental Research 111(6), 853–860.
Goodman PG, Dockery DW, Clancy L (2004) Cause-specific mortality and the extended effects of particulate pollution and temperature exposure. Environ Health Perspect 112:179–185
Gouveia N, Hajat S, Armstrong B (2003) Socioeconomic differentials in the temperature-mortality relationship in Sao Paulo. Brazil Int J Epidemiol 32:390–397
Guo Y, Barnett AG, Pan X, Yu W, Tong S (2011) The impact of temperature on mortality in Tianjin, China: a case-crossover design with a distributed lag nonlinear model. Environ Health Perspect 119:1719–1725
Guo Y, Li S, Zhang Y, Armstrong B, Jaakkola JJ, Tong S, Pan X (2013) Extremely cold and hot temperatures increase the risk of ischaemic heart disease mortality: epidemiological evidence from China. Heart 99(3):195–203
Guo YM, Punnasiri K, Tong SL (2012) Effect of temperature on mortaltiy in Chiang Mai city, Thailand: a time series study. Environmental Health 11(36):1–9
Hajat S, Kosatsky T (2010) Heat-related mortality: a review and exploration of heterogeneity. J Epidemiol Community Health 64(9):753–760
Hajat S, Kovats RS, Lachowycz K (2007) Heat-related and cold-related deaths in England and Wales: who is at risk? Occup Environ Med 64(2):93–100
Huang CR, Barnett AG, Wang XM, Tong SL (2012) Effects of extreme temperature on years of life lost for cardiovascular deaths: a time series study in Brisbane. Australian Circ Cardiovasc Qual Outcomes:609–614
Huynen MM, Martens P, Schram D (2001) The impact of heat waves and cold spells on mortality rates in the Dutch population. Environ Health Perspect 109:463–470
Iniguez C, Ballester F, Ferrandiz J, Perez-Hoyos S, Saez M, Lopez A (2010) Relation between temperature and mortality in thirteen Spanish cities. Int J Environ Res PublicHealth 7:3196–3210
IPCC (2013) Climate change 2013: the physical science basis. Contribution of Working Group I to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change. [Stocker, T.F., D. Qin, G.-K. Plattner, M. Tignor, S.K. Allen, J. Boschung, A. Nauels, Y. Xia, V. Bex and P.M. Midgley (eds.)]. Cambridge University Press, Cambridge, United Kingdom and New York, NY, USA.
Johnson H, Kovats S, McGregor G, Stedman J, Gibbs M, Walton H (2005) The impact of the 2003 heat wave on daily mortality in England and Wales and the use of rapid weekly mortality estimates. Euro Surveill 10:161–165
Kan HD, London SJ, Chen GH (2008) Season, sex age, and education as modifiers of the effects of outdoor air pollution on daily mortality in Shanghai, China: the Public Health and Air Pollution in Asia (PAPH) study. Environ Health Perspect 116:1183–1188
Kim H, Ha JS, Park J (2006) High temperature, heat index, and mortality in 6 major cities in South Korea. Arch Environ Occup Health 61(6):265–270
Knowlton K, Rotkin-Ellman M, King G, Margolis HG, Smith D, Solomon G et al (2009) The 2006 California heat wave: impacts on hospitalizations and emergency department visits. Environ Health Perspect 117:61–67
Kovats RS, Hajat S (2008) Heat stress and public health: a critical review. Annu Rev Public Health 29(1):41–55
Lin S, Luo M, Walker RJ, Liu X, Hwang SA, Chinery R (2009) Extreme high temperatures and hospital admissions for respiratory and cardiovascular diseases. Epidemiology 20:738–746
Lin YK, Chang CK, Wang YC, Ho TJ (2013) Acute and prolonged adverse effects of temperature on mortality from cardiovascular diseases. PLoS One 8(12):e82678
Luo HJ, Zeng SQ, Hu MJ, Luo Y, Ma WJ (2014) Effect of extreme low temperature on respiratory hospital admissions: a time-series study. South China J Prev Med 40(6):504–511
Ma WJ, Chen RJ, Kan HD (2014) Temperature-related mortality in 17 large Chinese cities: how heat and cold affect mortality in China. Environ Res 134:127–133
Ma W., Zeng W, Zhou M, Wang L, Rutherford S, Lin H, Liu T, Zhang Y, Xiao J ( 2015) The short-term effect of heat waves on mortality and its modifiers in China: an analysis from 66 communities. Environ Int 75, 103–109.
Martin SL, Cakmak S, Hebbern CA, Avramescu ML, Tremblay N (2012) Climate change and future temperature-related mortality in 15 Canadian cities. Int J Biometeorol 56(4):605–619
McMichael AJ, Wilkinson P, Kovats RS, Pattenden S, Hajat S, Armstrong B, Vajanapoom N, Niciu EM, Mahomed H, Kingkeow C (2008) International study of temperature, heat and urban mortality: the “ISOTHURM” project. Int J Epidemiol 37:1121–1131
Medina-Ramón M, Zanobetti A, Cavanagh DP, Schwartz J (2006) Extreme temperatures and mortality: assessing effect modification by personal characteristics and specific cause of death in a multi-city case-only analysis. Environ Health Perspect 114:1331–1336
Michelozzi P, Accetta G, Sario MD, D’Ippoliti D, Marino C, Baccini M, Biggeri A, Anderson HR, Katsouyanni K, Ballester F (2009) High temperature and hospitalizations for cardiovascular and respiratory causes in 12 European cities. Amer J Respir Crit Care Med 179:383–389
Mireku NA (2009) Changes in weather may trigger child’s asthma. Eur Ann Allergy Clin Immunol 160(5):41
Moran A, Gu D, Zhao D, Coxson P, Wang YC (2010) Future cardiovascular disease in China markov model and risk factor scenario projections from the coronary heart disease policy model–China. CircCardiovascQual Out-comes 3(3):243
Muggeo VM, Hajat S (2009) Modelling the non-linear multiple-lag effects of ambient temperature on mortality in Santiago and Palermo: a constrained segmented distributed lag approach. Occup Environ Med 66(9):584–591
O'Neill MS, Ebi KL (2009) Temperature extremes and health: impacts of climate variability and change in the United States. J Occup Environ Med 51:13–25
Qiu H, Tian LW, Ho KF (2015) Air pollution and mortality: effect modification by personal characteristics and specific cause of death in a case-only study. Environ Pollut 199:192–197
Revich B, Shaposhnikov D (2008) Temperature-induced excess mortality in Moscow, Russia. Int JBiometeorol 52:367–374
Rocklöv J, Forsberg B (2008) The effect of temperature on mortality in Stock-holm 1998-2003: a study of lag structures and heatwave effects. Scand J Public Health 36:516–523
Seposo XT, Dang TN, Yasushi H (2015) Evaluating the effects of temperature on mortality in Manila City (Philippines) from 2006–2010 using a distributed lag nonlinear model. Int J Environ Res Public Health 12:6842–6857
Son JY, Lee JY, Anderson GB, Bell ML (2011) Vulnerability to temperature-related mortality in Seoul. Korea Environ Res Lett 6(3):034027
Son JY, Lee JT, Anderson GB, Bell ML (2012) The impact of heat waves on mortality in seven major cities in Korea. Environ Health Perspect 120:566–571
Song XP, Wang SG, Li TS, Tian JH, Ding GW, Wang JX, Wang JX, Shang KZ (2017) The impact of heat waves and cold spells on respiratory emergency department visits in Beijing. China Science of the Total Environment 615:1499–1505
Stafoggia M, Forastiere F, Agostini D, Biggeri A, Bisanti L, Cadum E, Caranci N, De’Donato F (2006) Vulnerability to heat-related mortality: a multicity, population-based, case-crossover analysis. Epidemiology 17:315–323
Stewart S, Ekman I, Ekman T, Odén A, Rosengren A (2010) Population impact of heart failure and the most common forms of cancer a study of 1,162,309 hospital cases in Sweden (1988 to 2004). Circ Cardiovasc Qual Outcomes 3(6):573–580
Tataru N, Vidal C, Decavel P, Berger E, Rumbach L (2006) Limited impact of the summer heat wave in France (2003) on hospital admissions and relapses for multiple sclerosis. Neuroepidemiology 27:28–32
Turner LR, Connell D, Tong SL (2012) Exposure to hot and cold temperatures and ambulance attendances in Brisbane, Australia: a time-series study. BMJ Open 2(4):e001074
VicedoCabrera AM, Iñíguez C, Barona C, Ballester F (2014) Exposure to elevated temperatures and risk of preterm birth in Valencia, Spain. Environ Res 134:210–217
Wang YC, Lin YK, Chuang CY, Li MH, Chou CH, Liao CH, Sung FC (2012) Associating emergency room visits with first and prolonged extreme temperature event in Taiwan: a population-based cohort study. Sci Total Environ 416, 97–104.
Wang CC, Chen RJ, Kuang XY, Duan XL, Kan HD (2014) Temperature and daily mortality in Suzhou, China: a time series analysis. Sci Total Environ 466–467(1):985–990
Wang XY, Li GX, Liu LQ et al (2015) Effect of extreme temperatures on cause-specific cardiovascular mortality in China. International Journal of Environmental Research and Public Health 12:16136–16156
Xiang J, Bi P, Pisaniello D, Hansen A (2014) The impact of heatwaves on workers’ health and safety in Adelaide. South Australia Environ Res 133:90–95
Yang J, Ou CQ, Ding Y, Zhou YX, Chen PY (2012) Daily temperature and mortality: a study of distributed lag non-linear effect and effect modification in Guangzhou. Environ Health 11(1):63
Yang J, Liu HZ, Ou CQ, Lin GZ, Ding Y, Zhou Q et al (2013) Impact of heat wave in 2005 on mortality in Guangzhou. China Biomed Environ Sci 26:647–654
Yi W, Chan AP (2015) Effects of temperature on mortality in Hong Kong: a time series analysis. Int J Biometeorol 59:927–936
Yu W, Hu W, Mengersen K, Guo Y, Pan X, Connell D, Tong S (2011a) Time course of temperature effects on cardiovascular mortality in Brisbane. Australia Heart 97:1089–1093
Yu W, Mengersen K, Hu W, Guo Y, Pan X, Tong S (2011b) Assessing the relationship between global warming and mortality: lag effects of temperature fluctuations by age and mortality categories. Environ Pollut 159:1789–1793
Zanobetti A, Schwartz J, Samoli E, Gryparis A, Touloumi G (2003) The temporal pattern of respiratory and heart disease mortality in response to air pollution. Environ Health Perspect 111(9), 1188–1193.
Zeng W, Lao X, Rutherford S, Xu Y, Xu X, Lin H, Liu T, Luo Y, Xiao J, Hu M (2014) The effect of heat waves on mortality and effect modifiers in four communities of Guangdong province. China Sci Total Environ 482-483(1):214–221
Funding
This work is supported by Fundamental Research Funds for the Central Universities Grant No. lzujbky-2017-69, National Natural Science Foundation of China Grant No. 41475095, No. 91737101, and No. 41561037. Part of the work is funded by a Scholarship awarded to Yuxia Ma (File No.201308625022) supported by the China Scholarship Council (CSC).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Responsible editor: Philippe Garrigues
Electronic supplementary material
ESM 1
(DOC 390 kb)
Rights and permissions
About this article

Cite this article
Ma, Y., Zhou, J., Yang, S. et al. Effects of extreme temperatures on hospital emergency room visits for respiratory diseases in Beijing, China. Environ Sci Pollut Res 26, 3055–3064 (2019). https://doi.org/10.1007/s11356-018-3855-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-018-3855-4