
Abstract
Pro-thrombotic and inflammatory changes play an important role in cardiovascular morbidity and mortality, resulting from short-term exposure to fine particulate air-pollution. Part of those effects has been attributed to the ultra-fine particles (UFPs) that pass through the lung and directly contact blood-exposed and circulating cells. Despite UFP-induced platelet activation, it is unclear whether the penetrated particles exert any direct effect on endothelial cells. While exposure levels are boosting as a result of world-wide increases in economic development and desertification, which create more air-polluted regions, as well as increase in demands for synthetic UFPs in medicine and various industries, further studies on the health effects of these particles are required. In this study, human pulmonary and cardiac microvascular endothelial cells (MECs) have been exposed to 0.1, 1, 10, and 100 μg/ml suspensions of either a natural (carbon black) or a synthetic (multi-walled carbon nano-tubes) type of UFPs, in vitro. As a result, no changes in the levels of coagulation factor VIII, Von Willebrand factor, Interleukin 8, and P-selectin measured in the cells’ supernatant were observed prior to and 6, 12, and 24 h after exposure. In parallel, the spatio-temporal effect of UFPs on cardiac MECs was evaluated by Transmission Electron Microscopy. Despite phagocytic uptake of pure UFPs observed on cellular sections of the treated cells, Weibel-Palade bodies remained intact in shape and similar in number when compared with the untreated cells. Our work shows that carbon itself is a non-toxic carrier for endothelial cells.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Particulate matter (PM) comprises major environmental non-gaseous pollutants affecting health and is composed of airborne solid and liquid fractions with aerodynamic diameters ranging from < 100 to 10 μm, classified as coarse (PM10, 2.5–10 μm), fine (PM2.5, < 2.5 μm), and ultra-fine (UFP, < 100 nm) microparticles. While numerous studies in the past three decades have looked into the adverse health effects of exposure to PM10 and PM2.5, recent studies have shown that PM2.5 is the most important fraction of PM, affecting the cardiovascular system (Brook et al. 2010; Requia et al. 2018).
Exposure to ambient PM2.5 has been associated with short-term increases in hospital admission rates for cerebrovascular, peripheral, and cardiac ischemic disease; arrhythmia; and heart failure (Dominici et al. 2006; Schwartz et al. 1996; Shah et al. 2013; T. Burnett et al. 2000; Thurston et al. 2016). Upon inhalation, those particles penetrate deeply into the alveoli where they induce nervous autonomic imbalance and pulmonary inflammation (Brook et al. 2010; Niemann et al. 2017). The release of pulmonary and vascular cell-derived mediators such as histamine and microparticles subsequently results in a systemic inflammation marked by increases in C-reactive protein (Hertel et al. 2010), serum amyloid A (Meier et al. 2014), IL-6 (Kido et al. 2011), and oxidative stress (Ghio and Devlin 2001; Gurgueira et al. 2002; Huang et al. 2012; Meier et al. 2014; Seagrave 2008; Shrey et al. 2011; Steinvil et al. 2008; van Eeden et al. 2001; Wang et al. 2015).
A fraction of PM2.5, i.e., the UFPs, pass through the lung alveoli into the systemic circulation (Nemmar et al. 2002) and come in direct contact with vascular endothelial cells (ECs), peripheral blood mononuclear cells (PBMCs), and platelets. UFPs account for a major portion of the actual number of particles within the PM and have a higher surface area-to-mass ratio, which potentially increases their biological toxicity (Li et al. 2003; Oberdörster and Utell 2002). They may be produced naturally, originating from volcanoes and dust storms or by human activity, such as burning fossil fuels (HEI 2013). In addition to natural UFPs, manufactured Carbon Black (CB) and engineered carbon particles, such as “carbon nanotubes” (CNTs) recapitulate some properties of UFPs. These particles are currently used in manufacturing electronics, tires, cloths, paints, cosmetics etc., as well as in medicine for diagnosis, imaging and drug delivery (Abdalla et al. 2015). This increase in exposure level requires continued intensive studies on the health effects of UFPs, including CB and CNTs.
UFPs contribute to the risk of thrombotic/atherothrombotic injuries (Rodriguez-Yanez et al. 2015), mainly due to platelet activation (Rückerl et al. 2007) and endothelial dysfunction (Lawal et al. 2016). The 24-h exposure to diesel exhaust particles (DEPs), the main natural sources of ambient UFPs, has been associated with the release of pro-inflammatory mediators, mainly cytokines (Devouassoux et al. 2002), which subsequently result in an increased blood cell activation and ultimately can cause myocardial ischemic disorders (Hadi et al. 2005; Libby et al. 2002; Nemmar et al. 2003). The observed pro-thrombotic effect seems to be inflammation-dependent as it could be quenched in the presence of anti-inflammatory drugs or selective inhibitors of basophils, macrophages, and neutrophils (Nemmar et al. 2004; Nemmar et al. 2005). However, also direct and early inflammation-independent pro-thrombotic effects have been reported, in which platelets are activated by DEPs or DEP-associated components, as soon as 1 h after exposure (Nemmar et al. 2003). This effect is triggered by UFPs, passing the lung barrier and directly contacting circulating cells. Similar inflammation-independent platelet recruitment accompanied by deposition of fibrin and VWF on sinusoidal ECs has also been reported, during investigations in a mouse model of the effect of CB on the hepatic micro-circulation (Khandoga et al. 2004).
Systemic extrapulmonary effects of UFPs (Oberdörster et al. 2005), as a result of their distribution in other organs such as the heart (Nemmar et al. 2001), liver, spleen (Kreyling et al. 2002; Nemmar et al. 2001; Oberdörster et al. 2002), and even the brain (Nemmar et al. 2001) have long been debated, but is accepted today. Due to the possible accumulation and aggregation of UFPs in the microvasculature, it is likely that this specialized compartment of the circulation is the primary target for circulating particles or particles accumulated in extrapulmonary organs (Khandoga et al. 2004). In spite of studies that have confirmed that UFPs directly activate platelets and release pro-coagulation factors such as tissue factor (TF) (Kilinc et al. 2011), it is less clear whether penetrated UFPs exert any direct effect on the endothelium.
We have previously shown that endothelial storage pool of FVIII and VWF is releasable in response to several endogenous and/or exogenous stimuli including phorbol-myristate acetate (PMA), adrenaline, histamine, and TNF-α (Shahani et al. 2010). The acute release of FVIII from cardiac microvascular endothelial cells (MECs), following exposure to UFPs, potentially enhances thrombogenicity inside the myocardium. This may contribute to cardiac complications such as heart rate variability and arrhythmias, resulting from exposure to UFPs; subsequently, sudden cardiac death may arise (Franciosi et al. 2017). Those prevalent cardiac complications are reported to occur following exposure to airborne UFPs, as revealed by various epidemiological studies (Niemann et al. 2017; Silverman et al. 2010). Therefore, presently, we have measured FVIII and VWF release as sensitive probes, to investigate potential toxicity to endothelial cells of industrial CB and CNTs.
Methods
Cell activation
Human cardiac and pulmonary MECs at early passages (1 to 3) were purchased from ScienCell Research Laboratories (USA) and PromoCell (Germany) and cultured as described previously (Shahani et al. 2010). The cells were treated with a solution of 0.1, 1, 10, or 100 μg/ml in culture medium (ECM, 1001-ScienCell Research Laboratories) of either multi-walled carbon nanotubes (MWCNTs) (Nanocyl SA, Belgium) or carbon clack (CB) (EVONIK, Germany) 48 h after reaching confluence. Parallel cellular exposure to 100 nM PMA (Sigma-Aldrich, Belgium), a potent stimulator of regulated exocytosis from endothelial cells, was applied as a control. Nanocyl’s irregular entangled MWCNTs with 10–20 walls, 30 nm diameter and 5 μm long, were kindly provided by Katrien Luyts (Department of Public Health and Primary Care, Occupational and Environmental Toxicology, KU Leuven, Leuven, Belgium) and CB (Printex 90: average diameter, 14 nm: surface area, 300 m2/g) was a kind gift from the manufacturer, EVONIK. Atomic force microscopy (BioMAT™; JPK Instruments, Germany) and Zetasizer Nano Range (Malvern Instruments, UK) have confirmed the size and morphology of nanomaterials in suspensions by more than 95% consistency.
A 1 mg/ml stock suspension from these materials was prepared by dispersing the particles in a 2% bovine serum in Milli-Q water followed by a continuous sonication for 16 min while the suspension was kept on ice/water. The stock suspension was prepared freshly on the day of experimentation. The working dilutions (in cell culture medium) were vortexed before use. The entire preparation time took less than an hour.
Prior to, and 6, 12, and 24 h after treating the cells with MWCNT/CB suspensions, supernatant samples were collected, aliquoted, and frozen at − 80 °C. FVIII activity (FVIII: C) and VWF antigen were measured in the supernatants, according to previously described methods (Shahani et al. 2010). Soluble IL-8 and P-selectin were assayed on ELISA using an IL-8 ELISA kit (BMS204-3MST, eBioscience) and CD62P ELISA Kit (DY137, R&D), respectively, according to the manufacturer’s instructions.
An MTT assay was used to study cellular toxicity of CB and MWCNTs at the applied concentrations. To do so, confluent endothelial cells were exposed to concentrations of 10 and 100 μg/ml CB and MWCNT solutions up to 24 h. Then, the supernatant was removed and the cells were treated with 5 mg/ml MTT (3-[4, 5-dimethylthiazol-2-yl]-2,5-diphenyltetrazolium bromide, Sigma-Aldrich) solution and incubated for 4 h at 37 °C. To dissolve generated formazan crystals, dimethylsulfoxide (DMSO) was added at an equal volume for 15 min, on a shaker. The plate was then read at 570 nm on a microplate reader (BioTek, USA). Values obtained from the treated cells were calculated as a percentage of values obtained from untreated cells.
Microscopy
Confluent endothelial cells were treated with a 100 μg/ml suspension of MWCNTs or CB in culture medium for 24 h. Then, the supernatant was removed and a solution of 2.5% glutaraldehyde was gently added to the cells and incubated at room temperature for 2 h. The cells were then scraped and pelleted by centrifugation, further fixed in 1% osmium tetroxide, and dehydrated with ethanol. The cell pellet was embedded in resin, trimmed and sectioned. Transversal sections were imaged on a transmission electron microscope (ZEISS EM900, Germany).
Results
Direct exposure to UFPs does not affect the release of FVIII:C, VWF, P-selectin, and IL-8 from endothelial cells
Human cardiac and pulmonary microvascular endothelial cells (HCMECs and HPMECs) were exposed to 0.1, 1, 10, and 100 μg/ml of either MWCNTs or CB. The cell supernatant, collected either immediately or 6, 12, and 24 h after exposure was assayed in a modified chromogenic assay to measure FVIII: C (Shahani et al. 2010) or on ELISAs to measure the rise of VWF, P-selectin, or IL-8 antigen levels. As expected, a natural increase in the supernatant was observed for the secreted factors over the 24-h study. Secreted levels were significantly increased when the cells were treated with 100 nM PMA (Fig. 1). However, no significant changes in FVIII: C, VWF: Ag, P-selectin, or IL-8 levels were observed when CMECs were exposed to 0.1, 1, and 10 μg/ml of MWCNTs or CB. Similar results were obtained with HPMECs (data not shown).

HCMEC response to increasing doses of MWCNTs and CB. HCMECs were cultured on multiwell plates. Forty-eight hours after reaching confluence, the cells were treated with 0.1, 1, 10, and 100 μg/ml of either MWCNTs or CB. The cells’ supernatant collected either immediately (diamonds) or 6 (squares), 12 (circles), and 24 (triangle) hours after treatment were assayed to measure FVIII: C (A), VWF (B), P-selectin (C), and IL-8 levels (D). Results are expressed as the mean of at least three microculture wells in a single experiment. Four times repeat of experiments with the cells isolated from four different donors has reached the same outcome. Abbreviations are: CB (Carbon Black), MWCNTs (Multi-walled Carbon Nano-Tubes), ECM (Endothelial Cell Medium), PMA (Phorbol-Myrisatate Acetate). * P value < 0.05, ** P value < 0.005. ▲ 24 h, ● 12 h, ■ 6 h, ♦ 0 h
Treatment of the cells with 100 μg/ml CB for 24 h resulted in a slight increase in the levels of FVIII:C and VWF:Ag, compared with untreated cells or treatment with 0.1, 1, and 10 μg/ml of CB, without changing the FVIII:VWF ratio (Fig. 1 A, B, data for 0.1 and 1 μg/ml are not shown). However, those trends did not reach significance. Interestingly, the pattern was different for MWCNTs, as shown in Fig. 1. The cell toxicity assay revealed that a 24-h treatment of ECs with 100 μg/ml MWCNTs reduced cell viability by 25%. The decreased number of cultured cells, therefore, was responsible for the drop in detected FVIII: C, VWF, P-selectin, and IL-8 after 24 h (Fig. 1). MWCNTs at doses lower than 10 μg/ml did not affect endothelial cell viability (Supplementary Fig. 1).
Transmission electron microscopy confirms no effect of UFPs on endothelial Weibel-Palade bodies
The absent release of FVIII, VWF, P-selectin, and IL-8 in response to UFPs suggested that UFPs did not affect the endothelial WPBs in the exposed cells. WPBs are known as the main storage organelles for several important coagulation factors and inflammation mediators such FVIII, VWF, tissue plasminogen activator (tPA), IL-8, and P-selectin in endothelial cells (Valentijn et al. 2011).
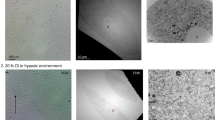
We investigated the size, distribution, and morphology of WPBs in HCMECs prior to, and after exposure to UFPs. As shown in Fig. 2, WPBs are clearly visible in the cytoplasm of untreated HCMECs in expected sizes (Valentijn et al. 2008), reported as 0.1–0.3 μm diameter and 1–5 μm length (Fig. 2A, B, pointed).

TEM image of cardiac MECs prior to and after exposure to 100 μg/ml MWCNTs. A and B illustrate untreated cells in which Weibel-Palade Bodies are clearly observed as rounded or cigar shaped structures pointed with arrow. B is a magnification of indicated position on image A. Images C, D, and E illustrate three different magnifications of one cell after 24 h treatment with a suspension of 100 μg/ml CB. WPBs are indicated with white filled arrows while phagosomes containing CB particles are indicated with white empty arrows. D, represents an almost full of MWCNT-containing exosomes. No intact WPB could be observed. Images are generated by a ZEISS EM900 transmission electron microscope
Images of HCMECs treated with CB are presented in Fig. 2C–E. Similar results were obtained for cells treated with MWCNTs. Evaluating more than ten sections revealed no change in WPBs, neither in number nor in shape, following treatment with CB or MWCNTs, although a clear phagocytic uptake of UFPs was observed. As illustrated in Fig. 2, most of the cells contained one to four phagosomes with an average size of 500 nm, each.
Or CB and MWCNTs, used as a model for manufactured carbon nanomaterial does not seem to have any direct influence on WPBs and endothelial cell activation.
Discussion
With the capability of producing several important coagulation and inflammation mediators such as FVIII, VWF, tPA, PAI-1, P-selectin, and Interleukins 6 and 8, endothelial cells are a good model to study the direct effect of air pollutants and its components. Whereas previous studies already showed that environmental UFPs activate endothelium (Emmerechts and Hoylaerts 2012; Vesterdal et al. 2012; Yamawaki and Iwai 2006) in the current study, we evaluated the effect of carbon in UFPs on microvascular endothelial cells (MEC) of human lung and heart, in vitro, in view of the omnipresence of carbon nanomaterials in various manufacturing processes. Pulmonary MECs are selected as the first EC types to which penetrated UFPs come in contact upon passage of epithelial-endothelial barriers in the lung alveoli. Cardiac MECs whose dysfunction disrupts the mechanical performance of myocardium are studied as they manifest more cardiac-specific properties than coronary or any other ECs in the heart (Brutsaert et al. 1988). In addition, pulmonary and cardiac MECs are among the main cellular sources of coagulation FVIII and VWF, the key players in blood coagulation and hemostasis (Jacquemin et al. 2006; Shahani et al. 2010). Exposure of human CMECs and PMECs to increasing doses of manufactured CB and MWCNTs, even at supra-pathophysiologic concentrations, i.e., 100 μg/ml, did not trigger any extra FVIII, VWF, P-selectin, and IL-8 release over baseline, after exposure for 24 h. Similar results were found when tPA and IL-6 were measured (data not shown).
The actual amounts of translocated UFPs into the circulation are still poorly known, despite extensive studies using these particles (Gwinn and Vallyathan 2006). The environmental PM level and composition, the health level of the lung and its alveolar structure, and presence or absence of underlying hypercoagulability diseases all determine the final impact of translocated UFPs on the endothelial surface of various vessels (Oberdörster et al. 2005). Taking all those parameters into account, a range of 1 to 100 μg/ml under normal conditions are estimated to largely cover the circulatory concentrations of translocated UFPs (Schmid et al. 2009; Yamawaki and Iwai 2006). Therefore, we studied the effects of CB and MWCNTs at 0.1, 1, 10, and 100 μg/ml.
Cell viability assays (MTT) further illustrated that EC exposure to 10–100 μg/ml for MWCNTs but not for CBs was toxic. In contrast, Walker et al., reported a dose-dependent toxicity of small-walled and multi-walled CNTs (SWCNTs and MWCNTs) on human aortic endothelial cells (HAECs) in the concentration range 1.5 to 4.5 μg/ml. They also observed parallel cytoskeleton disruption and an increase in the amount of released IL-8 upon 24 h treatment of HAECs with SWCNTs and MWCNTs, but not CB. Other studies have analyzed acute effects of UFPs on ECs, in vitro, using human umbilical vein (Pan et al. 2018; Rodriguez-Yanez et al. 2015; Yamawaki and Iwai 2006) and pulmonary artery endothelial cells (Karoly et al. 2007). Thus, Yamawaki et al. reported that a 24-h exposure of human umbilical vein endothelial cells (HUVECs) to CB at doses ranging from 10 to 100 μg/ml decreases cell viability in a dose-dependent manner. Cell growth inhibition and significant increase in the expression levels of monocyte chemoattractant protein1 (MCP-1), a pro-inflammatory cytokine, was also observed when HUVECs were exposed to 100 μg/ml CB. Based on that, the impact of EC exposure to CB in progression of arteriosclerosis and heart ischemia was proposed (Yamawaki and Iwai 2006).
In case of EC dysfunction, hemostasis would also be affected after direct contact with UFPs. In our study, the levels of FVIII, VWF, and tPA (data not shown) did not change during exposure. However, Rodriquez-Yanez et al. have shown that SWCNTs were able to alter the expression of genes and proteins involved in fibrinolysis, which in turn, may cause endothelial dysfunction and develop pro-thrombotic effect (Rodriguez-Yanez et al. 2015). Studying human pulmonary artery ECs, Karoly and colleagues reported a significant increase in tissue factor expression after 16 h exposure to 100 μg/ml ambient UFPs (Karoly et al. 2007). Up-regulation and down-regulation of several other genes involved in coagulation-inflammation pathways in that study report contributions of UFPs to a pro-thrombotic tendency, via ECs (Karoly et al. 2007). However, the ambient UFPs that were used contained various metal ions including aluminum, lead, iron, copper, silicon, and zinc at different concentrations, capable of catalyzing oxidative processes, known to be involved in inflammatory responses along with the increased oxidative stress and EC activation. (He et al. 2018; Jiang et al. 2000).
In this study, we intentionally used CB and MWCNTs as pure as possible, protecting them from exposure to ambient air, as much as possible. UFPs have a carbon core that enables formation of several chemical reactions with gases and other particles suspended in the air such as ions, metals, organic compounds, and inorganic materials (Adams et al. 2015). That makes ambient UFPs and their (adverse) effects, much more complex than the effect of pure UFPs, processes only understood in part. Compared with pure UFPs, ambient UFPs contain water soluble organic chemicals, pass through the epithelial-endothelial barriers of the lung more easily and affect epithelial and circulating cells (Kreyling et al. 2007; Schmid et al. 2009). Via transmission electron microscopy, we and others have observed phagocytosis of pure UFPs by ECs (Rodriguez-Yanez et al. 2015; Vesterdal et al. 2012; Walker et al. 2009), yet without apparent effect on WPBs. Upon exposure to pure UFPs, WPBs remained intact in shape and similar in number compared to the untreated cells. Phagocytic behavior of ECs, similar to the lung and intestinal epithelial cells, alveolar macrophages and neuronal cells (Hoet et al. 2004) seems to be a way to control the harmful effect of UFPs. Our findings substantiate that the pathophysiologic effect of UFPs in releasing inflammatory markers and coagulation factors, is driven by the soluble fraction of UFPs and is region-specific.
To our knowledge, in vitro, no other study has been performed on ECs from microvasculature. However, Khandoga and colleagues examined the effect of CB on the mouse hepatic micro-circulation, in vivo (Khandoga et al. 2004). Following intra-arterial infusion of CB in mice, they observed inflammation-independent platelet recruitment on ECs of sinusoids and post sinusoidal venules but not of arterioles, accompanied by deposition of fibrin and VWF, as revealed by immunostaining. Nonetheless, P-selectin remained inside the ECs. They also reported simultaneous fibrin deposition on cardiac microcirculation without providing further information (Khandoga et al. 2004). With regard to the liver vasculature, ECs of sinusoids are the single endothelial cell types of the liver which produce high amounts of FVIII, similar to cardiac MECs (Shahani et al. 2014); however, VWF production is either very low or absent in LSECs (unpublished observation). Khandoga and colleagues hypothesized that the observed prothrombotic changes on the endothelial surface of hepatic microvessels are due to the increased production of fibrinogen and coagulation factors by hepatocytes, stimulated by the exposure to CB particles crossed through the fenestrae of sinusoidal ECs. However, this hypothesis cannot simply be extrapolated to the heart microvasculature where a similar effect was observed for CB. The observed pro-thrombotic effect of CB in that study using the same material as the one we have used (CB, Printex 90, diameter 14 nm: surface area, 300 m2/g), however, could have resulted from direct platelet activation by CB, in agreement with previously reported platelet activation and subsequent pro-thrombotic effects of DEPs (Nemmar et al. 2003).
The lack of an effect for pure UFPs on ECs in our study does not reject possible pro-thrombotic effects, in vivo. Penetrated UFPs are in direct contact with platelets and PBMCs in the circulation, in addition to ECs. As stated above, direct interactions between UFPs, erythrocytes, and leukocytes enhancing thrombotic/atherothrombotic injuries have been reported (Nemmar et al. 2003; Rodriguez-Yanez et al. 2015). We and others (Rondaij et al. 2006) have shown that endothelial cells release their WPB contents in response to a series of inflammatory mediators such as TNF-α (Adams et al. 2013; Yamagami et al. 2003; and unpublished data). Treatment of THP-1, a monocyte cell line, with CB is resulted in a significant increase in IL-8 secretion (Sahu et al. 2014). Our future exposure studies, therefore, will benefit from co-incubations with platelets and monocytes, respectively other leukocytes and blood cells, to delineate a role for these cells versus ECs in thrombogenicity induction.
In conclusion, the lack of endothelial cell response to UFPs in this study does not reject the existence of pro-thrombotic and pro-inflammatory effects during exposure to ambient UFPs in man, but it shows that direct carbon-EC interactions hardly contribute to this process. Therefore, even when the widespread use of manufactured CB and engineered carbon particles in various industrial applications seems safe from a vascular point of view, our findings do not eliminate the need for detailed thrombogenicity studies during long-term occupational exposure to carbon nanomaterials.
Abbreviations
- FVIII:
-
Coagulation factor VIII
- FVIII:C:
-
FVIII activity
- HCMEC:
-
Human cardiac microvascular endothelial cells
- HPMEC:
-
Human pulmonary microvascular endothelial cells
- IL-8:
-
Interleukin 8
- LOD:
-
Limit of detection
- PM:
-
Particulate matter
- PMA:
-
Phorbol-12-myristate 13-acetate
- UFP:
-
Ultra-fine particle
- VWF:
-
Von-Willebrand factor
- WPB:
-
Weibel-Palade body
- TEM:
-
Transmission electron microscopy
References
Abdalla S, Al-Marzouki F, Al-Ghamdi AA, Abdel-Daiem A (2015) Different technical applications of carbon nanotubes. Nanoscale Res Lett 10:358
Adams K, Greenbaum DS, Shaikh R, van Erp AM, Russell AG (2015) Particulate matter components, sources, and health: systematic approaches to testing effects. J Air Waste Manag Assoc 65:544–558. https://doi.org/10.1080/10962247.2014.1001884
Adams WJ, Zhang Y, Cloutier J, Kuchimanchi P, Newton G, Sehrawat S, Aird WC, Mayadas TN, Luscinskas FW, García-Cardeña G (2013) Functional vascular endothelium derived from human induced pluripotent stem cells. Stem Cell Rep 1:105–113
Brook RD, Rajagopalan S, Pope CA 3rd, Brook JR, Bhatnagar A, Diez-Roux AV, Holguin F, Hong Y, Luepker RV, Mittleman MA, Peters A, Siscovick D, Smith SC Jr, Whitsel L, Kaufman JD, American Heart Association Council on Epidemiology and Prevention, Council on the Kidney in Cardiovascular Disease, and Council on Nutrition, Physical Activity and Metabolism (2010) Particulate matter air pollution and cardiovascular disease: an update to the scientific statement from the American Heart Association. Circulation 121:2331–2378
Brutsaert DL, Meulemans AL, Sipido KR, Sys SU (1988) Effects of damaging the endocardial surface on the mechanical performance of isolated cardiac muscle. Circ Res 62:358–366
Devouassoux G, Saxon A, Metcalfe DD, Prussin C, Colomb MG, Brambilla C, Diaz-Sanchez D (2002) Chemical constituents of diesel exhaust particles induce IL-4 production and histamine release by human basophils. J Allergy Clin Immunol 109:847–853
Dominici F, Peng RD, Bell ML, Pham L, McDermott A, Zeger SL, Samet JM (2006) Fine particulate air pollution and hospital admission for cardiovascular and respiratory diseases. Jama 295:1127–1134
Emmerechts J, Hoylaerts M (2012) The effect of air pollution on haemostasis. Hämostaseologie 32:5–13
Franciosi S, Perry FK, Roston TM, Armstrong KR, Claydon VE, Sanatani S (2017) The role of the autonomic nervous system in arrhythmias and sudden cardiac death. Autonomic Neuroscience: Basic and Clinical 205:1–11
Ghio AJ, Devlin RB (2001) Inflammatory lung injury after bronchial instillation of air pollution particles. Am J Respir Crit Care Med 164:704–708. https://doi.org/10.1164/ajrccm.164.4.2011089
Gurgueira SA, Lawrence J, Coull B, Murthy GG, Gonzalez-Flecha B (2002) Rapid increases in the steady-state concentration of reactive oxygen species in the lungs and heart after particulate air pollution inhalation. Environ Health Perspect 110:749–755
Gwinn MR, Vallyathan V (2006) Nanoparticles: health effects—pros and cons. Environ Health Perspect 114:1818–1825
Hadi HA, Carr CS, Al Suwaidi J (2005) Endothelial dysfunction: cardiovascular risk factors, therapy, and outcome Vascular health and risk management 1:183
He R-W, Shirmohammadi F, Gerlofs-Nijland ME, Sioutas C, Cassee FR (2018) Pro-inflammatory responses to PM 0.25 from airport and urban traffic emissions. Sci Total Environ 640:997–1003
Hei, H (2013) Review panel on ultrafine particles. Understanding the health effects of ambient ultrafine particles HEI Perspectives 3Health Effects Institute, Boston, MA:122
Hertel S, Viehmann A, Moebus S, Mann K, Bröcker-Preuss M, Möhlenkamp S, Nonnemacher M, Erbel R, Jakobs H, Memmesheimer M, Jöckel KH, Hoffmann B (2010) Influence of short-term exposure to ultrafine and fine particles on systemic inflammation. Eur J Epidemiol 25:581–592
Hoet PH, Brüske-Hohlfeld I, Salata OV (2004) Nanoparticles–known and unknown health risks. J Nanobiotechnol 2(1):12
Huang W, Wang G, Lu SE, Kipen H, Wang Y, Hu M, Lin W, Rich D, Ohman-Strickland P, Diehl SR, Zhu P, Tong J, Gong J, Zhu T, Zhang J (2012) Inflammatory and oxidative stress responses of healthy young adults to changes in air quality during the Beijing Olympics. Am J Respir Crit Care Med 186:1150–1159. https://doi.org/10.1164/rccm.201205-0850OC
Jacquemin M, Neyrinck A, Hermanns MI, Lavend'homme R, Rega F, Saint-Remy JM, Peerlinck K, van Raemdonck D, Kirkpatrick CJ (2006) FVIII production by human lung microvascular endothelial cells. Blood 108:515–517
Jiang N, Dreher KL, Dye JA, Li Y, Richards JH, Martin LD, Adler KB (2000) Residual oil fly ash induces cytotoxicity and mucin secretion by guinea pig tracheal epithelial cells via an oxidant-mediated mechanism. Toxicol Appl Pharmacol 163:221–230
Karoly ED, Li Z, Dailey LA, Hyseni X, Huang Y-CT (2007) Up-regulation of tissue factor in human pulmonary artery endothelial cells after ultrafine particle exposure. Environ Health Perspect 115:535–540
Khandoga A, Stampfl A, Takenaka S, Schulz H, Radykewicz R, Kreyling W, Krombach F (2004) Ultrafine particles exert prothrombotic but not inflammatory effects on the hepatic microcirculation in healthy mice in vivo. Circulation 109:1320–1325
Kido T, Tamagawa E, Bai N, Suda K, Yang HHC, Li Y, Chiang G, Yatera K, Mukae H, Sin DD, van Eeden SF (2011) Particulate matter induces translocation of IL-6 from the lung to the systemic circulation. Am J Respir Cell Mol Biol 44:197–204
Kilinc E et al (2011) Factor XII activation is essential to sustain the procoagulant effects of particulate matter. J Thromb Haemost 9:1359–1367
Kreyling WG, Möller W, Semmler-Behnke M, Oberdörster G (2007) Particle dosimetry: deposition and clearance from the respiratory tract and translocation towards extrapulmonary sites. Particle toxicology:2007
Kreyling WG, Semmler M, Erbe F, Mayer P, Takenaka S, Schulz H, Oberdörster G, Ziesenis A (2002) Translocation of ultrafine insoluble iridium particles from lung epithelium to extrapulmonary organs is size dependent but very low. J Toxicol Environ Health A 65:1513–1530. https://doi.org/10.1080/00984100290071649
Lawal A, Davids L, Marnewick J (2016) Diesel exhaust particles and endothelial cells dysfunction: an update. Toxicol in Vitro 32:92–104
Li N, Sioutas C, Cho A, Schmitz D, Misra C, Sempf J, Wang M, Oberley T, Froines J, Nel A (2003) Ultrafine particulate pollutants induce oxidative stress and mitochondrial damage. Environ Health Perspect 111:455–460
Libby P, Ridker PM, Maseri A (2002) Inflammation and atherosclerosis. Circulation 105:1135–1143
Meier R, Cascio WE, Ghio AJ, Wild P, Danuser B, Riediker M (2014) Associations of short-term particle and noise exposures with markers of cardiovascular and respiratory health among highway maintenance workers. Environ Health Perspect 122:726–732
Nemmar A, Hoet PH, Vermylen J, Nemery B, Hoylaerts MF (2004) Pharmacological stabilization of mast cells abrogates late thrombotic events induced by diesel exhaust particles in hamsters. Circulation 110:1670–1677
Nemmar A, Hoet PHM, Vanquickenborne B, Dinsdale D, Thomeer M, Hoylaerts MF, Vanbilloen H, Mortelmans L, Nemery B (2002) Passage of inhaled particles into the blood circulation in humans. Circulation 105:411–414
Nemmar A, Nemery B, Hoet PH, Van Rooijen N, Hoylaerts MF (2005) Silica particles enhance peripheral thrombosis: key role of lung macrophage–neutrophil cross-talk. Am J Respir Crit Care Med 171:872–879
Nemmar A, Nemery B, Hoet PH, Vermylen J, Hoylaerts MF (2003) Pulmonary inflammation and thrombogenicity caused by diesel particles in hamsters: role of histamine. Am J Respir Crit Care Med 168:1366–1372
Nemmar A, Vanbilloen H, Hoylaerts M, Hoet P, Verbruggen A, Nemery B (2001) Passage of intratracheally instilled ultrafine particles from the lung into the systemic circulation in hamster. Am J Respir Crit Care Med 164:1665–1668
Niemann B, Rohrbach S, Miller MR, Newby DE, Fuster V, Kovacic JC (2017) Oxidative stress and cardiovascular risk: obesity, diabetes, smoking, and pollution: part 3 of a 3-part series. J Am Coll Cardiol 70:230–251
Oberdörster G, Oberdörster E, Oberdörster J (2005) Nanotoxicology: an emerging discipline evolving from studies of ultrafine particles. Environ Health Perspect 113:823–839
Oberdörster G, Sharp Z, Atudorei V, Elder A, Gelein R, Lunts A, Kreyling W, Cox C (2002) Extrapulmonary translocation of ultrafine carbon particles following whole-body inhalation exposure of rats. J Toxicol Environ Health, Part A 65:1531–1543
Oberdörster G, Utell MJ (2002) Ultrafine particles in the urban air: to the respiratory tract--and beyond? Environ Health Perspect 110:A440–a441
Pan X, Gong YY, Xu Y, Ariens RA, Routledge MN (2018) Urban particulate matter induces changes in gene expression in vascular endothelial cells that are associated with altered clot structure in vitro. Thromb Haemost 118:266–278
Requia WJ, Adams MD, Arain A, Papatheodorou S, Koutrakis P, Mahmoud M (2018) Global association of air pollution and cardiorespiratory diseases: a systematic review, meta-analysis, and investigation of modifier variables. Am J Public Health 108:S123–S130
Rodriguez-Yanez Y, Bahena-Uribe D, Chavez-Munguia B, López-Marure R, Gonzalez-Monroy S, Cisneros B, Albores A (2015) Commercial single-walled carbon nanotubes effects in fibrinolysis of human umbilical vein endothelial cells. Toxicol in Vitro 29:1201–1214
Rondaij MG, Bierings R, Kragt A, van Mourik JA, Voorberg J (2006) Dynamics and plasticity of Weibel-Palade bodies in endothelial cells. Arterioscler Thromb Vasc Biol 26:1002–1007
Rückerl R et al (2007) Ultrafine particles and platelet activation in patients with coronary heart disease – results from a prospective panel study. Part Fibre Toxicol 4(1):1
Sahu D, Kannan G, Vijayaraghavan R (2014) Carbon black particle exhibits size dependent toxicity in human monocytes. Int J Inflamm 2014:1–10
Schmid O, Möller W, Semmler-Behnke M, A. Ferron G, Karg E, Lipka J, Schulz H, Kreyling WG, Stoeger T (2009) Dosimetry and toxicology of inhaled ultrafine particles. Biomarkers 14:67–73
Schwartz J, Dockery DW, Neas LM (1996) Is daily mortality associated specifically with fine particles? J Air Waste Manage Assoc 46:927–939
Seagrave J (2008) Mechanisms and implications of air pollution particle associations with chemokines. Toxicol Appl Pharmacol 232:469–477. https://doi.org/10.1016/j.taap.2008.08.001
Shah ASV, Langrish JP, Nair H, McAllister DA, Hunter AL, Donaldson K, Newby DE, Mills NL (2013) Global association of air pollution and heart failure: a systematic review and meta-analysis. Lancet 382:1039–1048. https://doi.org/10.1016/S0140-6736(13)60898-3
Shahani T, Covens K, Lavend'Homme R, Jazouli N, Sokal E, Peerlinck K, Jacquemin M (2014) Human liver sinusoidal endothelial cells but not hepatocytes contain factor VIII. J Thromb Haemost 12:36–42
Shahani T, Lavend'homme R, Luttun A, Saint-Remy JM, Peerlinck K, Jacquemin M (2010) Activation of human endothelial cells from specific vascular beds induces the release of a FVIII storage pool. Blood 115:4902–4909. https://doi.org/10.1182/blood-2009-07-232546
Shrey K, Suchit A, Deepika D, Shruti K, Vibha R (2011) Air pollutants: the key stages in the pathway towards the development of cardiovascular disorders. Environ Toxicol Pharmacol 31:1–9. https://doi.org/10.1016/j.etap.2010.09.002
Silverman RA, Ito K, Freese J, Kaufman BJ, De Claro D, Braun J, Prezant DJ (2010) Association of ambient fine particles with out-of-hospital cardiac arrests in New York City. Am J Epidemiol 172:917–923
Steinvil A, Kordova-Biezuner L, Shapira I, Berliner S, Rogowski O (2008) Short-term exposure to air pollution and inflammation-sensitive biomarkers. Environ Res 106:51–61. https://doi.org/10.1016/j.envres.2007.08.006
Burnett RT et al (2000) Association between particulate-and gas-phase components of urban air pollution and daily mortality in eight Canadian cities. Inhal Toxicol 12:15–39
Thurston GD, Burnett RT, Turner MC, Shi Y, Krewski D, Lall R, Ito K, Jerrett M, Gapstur SM, Diver WR, Pope CA III (2016) Ischemic heart disease mortality and long-term exposure to source-related components of US fine particle air pollution. Environ Health Perspect 124:785–794
Valentijn K, Valentijn J, Jansen K, Koster A (2008) A new look at Weibel–Palade body structure in endothelial cells using electron tomography. J Struct Biol 161:447–458
Valentijn KM, Sadler JE, Valentijn JA, Voorberg J, Eikenboom J (2011) Functional architecture of Weibel-Palade bodies. Blood 117:5033–5043
van Eeden SF et al (2001) Cytokines involved in the systemic inflammatory response induced by exposure to particulate matter air pollutants (PM(10)). Am J Respir Crit Care Med 164:826–830. https://doi.org/10.1164/ajrccm.164.5.2010160
Vesterdal LK, Mikkelsen L, Folkmann JK, Sheykhzade M, Cao Y, Roursgaard M, Loft S, Møller P (2012) Carbon black nanoparticles and vascular dysfunction in cultured endothelial cells and artery segments. Toxicol Lett 214:19–26
Walker VG, Li Z, Hulderman T, Schwegler-Berry D, Kashon ML, Simeonova PP (2009) Potential in vitro effects of carbon nanotubes on human aortic endothelial cells. Toxicol Appl Pharmacol 236:319–328
Wang J, Tang B, Liu X, Wu X, Wang H, Xu D, Guo Y (2015) Increased monomeric CRP levels in acute myocardial infarction: a possible new and specific biomarker for diagnosis and severity assessment of disease. Atherosclerosis 239:343–349. https://doi.org/10.1016/j.atherosclerosis.2015.01.024
Yamagami H, Yamagami S, Inoki T, Amano S, Miyata K (2003) The effects of proinflammatory cytokines on cytokine-chemokine gene expression profiles in the human corneal endothelium. Invest Ophthalmol Vis Sci 44:514–520
Yamawaki H, Iwai N (2006) Mechanisms underlying Nano-sized air-pollution-mediated progression of atherosclerosis. Circ J 70:129–140
Acknowledgements
Special thanks to Mrs. Zahra Ramezani for her technical support with TEM at Biomedical Engineering and Medical Physics Department of Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Funding
This work is supported by Zanjan University of Medical Sciences (ZUMS) grant number A-12-776-2 and Iran’s National Institute for Medical Research Development (NIMAD) grant number 940200.
Author information
Authors and Affiliations
Contributions
HD, MH, and TSH wrote the manuscript. HD, ZP, LS, and RN performed/analyzed the experiments. MH, AB, MJ, and TSH contributed to the study design and data analysis. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
The study was conducted in accordance with the Helsinki Declaration and approved by Zanjan University of Medical Sciences Ethics Committee (ZUMS.REC.1394.132; 01-Sept 2015).
Consent for publication
Not applicable.
Availability of data and material
The data that support the findings of this study are available from the corresponding authors on reasonable request.
Competing interests
The authors declare that they have no conflict of interest.
Additional information
Responsible editor: Philippe Garrigues
Electronic supplementary material
Figure S1
Effect of CB and MWCNTs on endothelial cell viability assayed by MTT test. Cells were incubated with 10 and 100 μg/ml of CB or MWCNTs for 24 h. The values for cell viability represent the mean of three experiments shown as percentage to the untreated cells, indicated as controls. Error bars represent standard deviation (SD). The abbreviations are: CB (Carbon Black), MWCNTs (Multi-wall Carbon Nano-Tube). * P value <0.001. (PDF 62 kb)
Rights and permissions
About this article

Cite this article
Dinmohammadi, H., Pirdel, Z., Salarilak, L. et al. Pure ultra-fine carbon particles do not exert pro-coagulation and inflammatory effects on microvascular endothelial cells. Environ Sci Pollut Res 26, 991–999 (2019). https://doi.org/10.1007/s11356-018-3783-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-018-3783-3