
Abstract
The potential contaminations of 16 trace elements (Cr, Mn, Ni, Cu, Zn, As, Cd, Sb, Ba, Pb, Co, Be, V, Ti, Tl, Al) in drinking water collected in two remote areas in China were analyzed. The average levels of the trace elements were lower than the allowable concentrations set by national agencies, except for several elements (As, Sb, Mn, and Be) in individual samples. A health risk assessment model was conducted and carcinogenic and non-carcinogenic risks were evaluated separately. The results indicated that the total carcinogenic risks were higher than the maximum allowed risk level set by most organizations (1 × 10−6). Residents in both study areas were at risk of carcinogenic effects from exposure to Cr, which accounted for 80–90 % of the total carcinogenic risks. The non-carcinogenic risks (Cu, Zn, Ni) were lower than the maximum allowance levels. Among the four population groups, infants incurred the highest health risks and required special attention. Correlation analysis revealed significant positive associations among most trace elements, indicating the likelihood of a common source. The results of probabilistic health risk assessment of Cr based on Monte-Carlo simulation revealed that the uncertainty of system parameters does not affect the decision making of pollution prevention and control. Sensitivity analysis revealed that ingestion rate of water and concentration of Cr showed relatively high sensitivity to the health risks.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Safe drinking water is a birthright of all humankind, just as clean air is (TWAS 2002). There is no doubt that it is also one of the most important resources for sustaining humanity and human society. However, drinking water quality is particularly vulnerable to numerous anthropogenic (e.g., urban, industrial, and agricultural activities) and natural processes (e.g., changes in precipitation inputs, erosion, and weathering of crustal materials). Thus, water pollution is a worldwide public health problem, with heavy metals topping the list of priority environmental pollutants (Alves et al. 2014).
While there are many ways for trace elements to enter the human body (e.g., inhalation, dermal absorption, food, and drink), the health risks posed by oral intake are the highest among all exposure pathways (Zhang et al. 2014a, b). Metals in water can easily enter the body by ingestion, accumulating in fatty tissues or depositing in the circulatory system due to their toxicity and non-biodegradability (Lu et al. 2014; Tang et al. 2013). In the body, heavy metals can disrupt the nervous and endocrine systems or act as auxiliary factors of other diseases (Zheng et al. 2010a, b). In addition, some deleterious metals can even cause cancer (Steinemann 2000; IARC 1980; Borum and Abrnathy 1994). For example, neurological disorders resulting from drinking Mn-rich water have been reported in epidemiological studies (WHO 2008). Trace elements in drinking water could pose significant non-carcinogenic effects to their consumers (Muhammad et al. 2011; Kavcar et al. 2009). Furthermore, human exposure to As can lead to skin lesions and induce skin cancer (WHO 2011).
Metal pollutants in drinking water pose a serious threat to human health, and in recent years, heavy metal pollution has generated widespread concern (Mondal et al. 2010; Haider et al. 2012). While water quality assessment has primarily involved evaluating the concentrations of trace elements against national standards. Furthermore, some non-nutrient elements can be detrimental to human health at levels that do not exceed their maximum guideline values (Zhang et al. 2014a, b). For instance, the World Health Organization has recently discontinued its drinking water guideline value of 400 g L−1 for Mn because this health-based value was found to be well above the Mn levels normally found in drinking water (WHO 2011).
Based on research regarding the harm metal pollution inflicts on the human body, the International Agency for Research on Cancer (IARC) developed a classification system in terms of the carcinogenicity of chemical toxicants and a model of health hazard risks caused by carcinogens and non-carcinogens by US EPA (US EPA 1991, 2005, 2009). In recent years, quantitative health risk assessment has become a frequently applied methodology to evaluate the potential risks of metal pollutants (Ferré-Huguet et al. 2009). With this in mind, metal pollution in water can be viewed as a human health risk. Previous studies have paid most of their attention to potable water security in cities or developed areas, resulting in a lack of research on water quality in remote areas (Lu et al. 2015). However, drinking water in cities and developed areas is generally secure, the quality of potable water in remote areas is far from guaranteed because water monitoring in those areas is inadequate. Therefore, research in these areas is of great practical significance. For these reasons, further research is required to fully understand the distribution of trace elements and the carcinogenic and non-carcinogenic risks of exposure to metals through drinking water in remote areas.
The Tibetan area and Inner Mongolia region are located in the plateau area of the Chinese frontier. The climate and environmental conditions in these areas differ from conditions in developed and urban areas. In this study, the Qinghai-Tibet and Inner Mongolia regions were selected as cases representative of remote areas in China. The objectives of this present study were to (1) investigate the concentration levels of trace elements in drinking water collected in these areas and compare these measurements to national water quality guideline values, (2) evaluate the potential health risk to the population in these two study areas that is attributed to ingesting single and mixed trace elements through drinking water, (3) correlate the concentrations of trace elements in drinking water using statistical analysis to determine their origin and the relationship among them, and (4) estimate the uncertainty and variability of model parameters of health risk assessment based on Monte-Carlo simulation and sensitivity analysis.
Materials and methods
Study area
With an average elevation above 4500 m, the Qinghai-Tibet Plateau, known as the “Roof of the World” and the “Third Pole”, is the highest plateau in the world. It is located at 26°00′12″N-39°46′50″N and 73°18′52″E-104°46′59″E and is the headstream of many rivers in Asia including the Yangtze River, the Yellow River, and the Nujiang River. The headstream area is known as the “Water Tower of China”. The Inner Mongolian Plateau located in northern China is the second largest plateau in China after the Qinghai-Tibet Plateau. It is located at 40°20′N-50°50′N, and the elevation ranges from 1000 to 1400 m in the Inner Mongolia area. The present study was conducted in these two areas.
Sample preparation and analyses
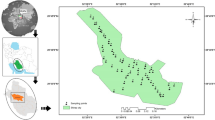
For this study, a total of 48 water samples were collected from local residential houses in these two areas. In the Tibetan area, 33 samples were collected from homes along 109 National Road, from Lhasa to Golmud and Sining city. The remaining 15 samples were collected in Inner Mongolia region. The specific location of the sampling points is shown in Fig. 1.

Location of sampling sites in study areas
The water samples were collected in plastic containers, labeled and then transported to the laboratory. The samples were filtered through 0.45-μm filter membranes, and concentrated nitric acid was added to the samples for preservation to reduce the pH <2. All samples were stored in sealed polyethylene sample bottles at 4 °C until analyzed.
The total concentrations of the following 16 trace elements were evaluated in all samples of water: chromium (Cr), manganese (Mn), nickel (Ni), cuprum (Cu), zinc (Zn), arsenic (As), cadmium (Cd), antimony (Sb), barium (Ba), lead (Pb), cobalt (Co), beryllium (Be), vanadium (V), titanium (Ti), thallium (Tl), and aluminum (Al). Element concentrations were measured using inductively coupled plasma spectrometry (ICP-MS, Perkin Elmer Elan DRC-e). For quality control, a standard reference material (Trace Element in Water, Agilent) was analyzed to check the ICP-MS accuracy. A new calibration curve was run after every 10 samples. The recovery rate was in the recommended range (90–110 %). The results showed that relative standard deviations (RSD) of the sample material were all less than 10 %, data precision and accuracy were in accordance with the requirements of the US EPA (RSD <10 %). Data analyses were carried out using the SPSS 17.0 Statistical Software Package for Windows.
Human health risk assessment
Metal concentrations in water were used to estimate the human health risks due to metal exposure for inhabitants living in the two study areas. Human health risks were assessed using US EPA (1986) methodology. Non-carcinogenic and carcinogenic risks were separately assessed. Ten elements were selected to evaluate the health risks associated with drinking water. For the current risk assessment, Cd, As, and Cr were regarded as chemical carcinogens, while Pb, Zn, Cu, Mn, Ba, Sb, and Ni were non-carcinogens (US EPA 2000). The carcinogenic and non-carcinogenic strength coefficients and values of associated parameters in risk assessment are listed in Tables S1, S2, and S3. For carcinogens, the following expressions (Eqs. 1, 2, and 3) were used to calculate cancer risks:
where R nm is the carcinogenic risk in an individual lifetime posed by the chemical carcinogen, Dj is the acceptable daily intake of heavy metals through the ingestion pathway (mg kg−1 day−1), qj is the strength coefficient (mg kg−1day−1)−1, Y is the average lifetime (years), Cj is the concentration of heavy metals in water (mg L−1), Qi is the ingestion rate of water (L day−1), and Wi refers to body weight (kg).
The calculation formula for health risk assessment by non-carcinogenic pollutants can be represented as:
where R c j is the health risk in an individual lifetime posed by chemical non-carcinogen, Dm is the acceptable daily intake of heavy metals through the ingestion pathway (mg kg−1 day−1), RfDm is the reference dose (mg kg−1 day−1), Y is the average lifetime (years), Cm is the concentration of heavy metals in water (mg L−1), Qi is the ingestion rate of water (L day−1), and Wi refers to body weight (kg).
where R is the sum of the Rc (carcinogenic risk) and Rn (non-carcinogenic risk), which means the potential health risks posed by all heavy metals.
Results and discussion
Trace element concentrations
The concentrations of 16 trace elements in drinking water from the two study areas are summarized in Tables 1 and 2, including the means, standard deviations, minimum values, and maximum values. All 16 elements were detected in samples from both areas, in varying concentrations. The mean concentrations in drinking water from the Tibetan area were 2.31, 0.33, 2.11, 0.88, 12.04, 1.70, 0.02, 3.44, 39.52, 0.12, 0.28, 0.08, 1.89, 1.89, 0.01, and 1.86 μg/L for Cr, Mn, Ni, Cu, Zn, As, Cd, Sb, Ba, Pb, Co, Be, V, Ti, Tl, and Al, respectively. The mean concentrations in drinking water from Inner Mongolia region were 9.28, 17.37, 1.97, 2.67, 34.06, 2.72, 0.08, 4.64, 27.38, 0.11, 0.21, 0.27, 3.77, 2.61, 0.01, and 1.63 μg/L for Cr, Mn, Ni, Cu, Zn, As, Cd, Sb, Ba, Pb, Co, Be, V, Ti, Tl, and Al, respectively. In the Tibetan area, Ba had the highest mean levels in drinking water (39.52 μg/L), while Zn had the highest mean level (34.06 μg/L) in the Inner Mongolia region. The average concentration of the 16 elements decreased in the following order in the Tibetan Area: Ba > Zn >S > Cr > Ni > V ≈ Ti > Al > As > Cu > Mn > Co > Pb > Be > Cd > Tl. In the Inner Mongolia region, the average concentration decreased in the following order: Zn > Ba > Mn > Cr > Sb > V > As > Cu > Ti > Ni > Al > Be > Co > Pb > Cd > Tl.
Surface water is categorized into five classes according to use and potential risk for public health. Based on this classification, the water samples in the present study were categorized as class 2, waters suitable for central water supply. Compared to China’s drinking water standard (GB5749-2006) and surface water standard (GB3838-2002), most of the trace elements in water from both areas met the requirements of the regulation. However, the concentrations of As and Sb in some of the water samples from the Tibetan area exceeded the national standard (Table 1), with over-limit ratios of 3.03 and 18.18 %, respectively. Additionally, the concentrations of Mn, Sb, and Be in some water samples from the Inner Mongolia region exceeded the national standard (Table 2). For these elements, the over-limit ratios were 6.67, 33.33, and 6.67 %, respectively.
A comparison revealed similarities and differences in the distribution of trace elements between the two study areas. In general, individual element levels in water samples from the Inner Mongolia region were higher than those from the Tibetan area except for Ba, Ni, Co, and Al. The orders of the mean concentrations of the elements were also different in two areas. In addition, the concentrations of As in the Tibetan area varied greatly, ranging from 0.21 to 23.07 μg/L, while the As concentrations in Inner Mongolia region were between 0.86 and 6.43 μg/L. When individually evaluating metal concentrations at each sampling point, the highest concentration of As was found in the sample collected in Ulan Moron. On the other hand, Ba, Zn, Sb, and Cr concentrations were similarly higher than other elements in the Tibetan Area and the Inner Mongolia region. Sb was the major pollutant in both study areas. With relatively higher over-limit ratios, this problem requires further attention.
In recent years, the issue of drinking water polluted by trace elements has received increased attention around the world, especially in developed areas. For instance, a previous study assessed tap water quality in Shenzhen China (Lu et al. 2015). In that study, the mean concentrations of Mn, Cr, As, Cd, and Sb were 0.90, 0.15, 0.37, 0.038, and 0.30 μg/L, respectively. Pb was not detected in most of the samples. The concentrations of these heavy metals measured in the present study were much higher than those reported by Lu et al. (2015). Another study investigated six heavy metals (Cr, Ni, Cu, Zn, As, and Cd) in water in Zhalong wetland in China (Zhang et al. 2014a, b). Almost all mean concentrations of the studied heavy metals in water were lower than those in the present study except for Cd. Overall, the concentrations of most heavy metals in drinking water in the studied remote areas were likely to be higher than levels found in inland cities. On the one hand, it may derive from the local geological characteristics. The two studied areas belong to plateau areas, the special geological characteristics may be different from the inland. On the other hand, the drinking water treatment in remote areas may be not defective and water monitoring may be inadequate, so that the drinking water quality is hard to be guaranteed. The specific reason is not clear yet, and need to be further researched.
Health risk assessment
The concentrations of metals in water were used to assess human exposure through ingestion of drinking water. Four population groups were considered: infants, teenager, adults, and the elderly. The predicted health risks of exposure to metals through water ingestion, according to both study areas, are summarized in Tables 3 and 4. The carcinogenic risks of three metals and the non-carcinogenic risks of seven metals were assessed in the present study.
Carcinogenic risk assessment
The average values of lifetime carcinogenic risk were different among heavy metals in both study areas. It is notable that Cr showed the highest carcinogenic risk among all of the metals assessed in this study. The mean values of Cr carcinogenic risk in the Tibetan area were 6.60 × 10−5, 5.62 × 10−5, 6.33 × 10−5, and 5.42 × 10−5 for infants, teenagers, adults, and the elderly, respectively. The mean values of Cr carcinogenic risk in the Inner Mongolia region were 2.63 × 10−4, 2.24 × 10−4, 2.52 × 10−4, and 2.16 × 10−4 for infants, teenagers, adults, and the elderly, respectively. The carcinogenic risks posed by Cr to the four groups in the Inner Mongolia region were all above the maximal acceptable risk levels. The Cr carcinogenic risks to the four groups in the Tibetan area were above the maximal acceptable risk levels, except for the levels specified by the US EPA (Table 2). The mean value of carcinogenic risks induced by As reached 10−5, which is above the maximal acceptable risk level set by most organizations (1 × 10−6) but below the maximal acceptable risk level set by the US EPA and ICRP. However, the carcinogenic risks induced by Cd were less than 10−6, which is below the maximal acceptable risk level. Figure S1 illustrates the relative contribution of each metal to the carcinogenic risks of drinking water in these two study areas. In the Tibetan area, approximately 80 % of the carcinogenic risks to the four population groups of people were induced by Cr, approximately 21 % were induced by As, and only 0.1 % were induced by Cd. In the Inner Mongolia region, the risks induced by Cr accounted for almost 90 % of the total carcinogenic risks, and As and Cd accounted for less than 10 %.
Non-carcinogenic risk assessment
Tables 3 and 4 summarize the non-carcinogenic health risk assessment for the selected metals in water for the different age groups included in this study. The mean non-carcinogenic health risk levels were found in the following descending order in the Tibetan area: Sb > Ba > Cu > Ni > Pb > Zn > Mn. In the Inner Mongolia region, the descending order was as follows: Sb > Mn > Cu > Ba > Zn > Ni > Pb. Sb, Cu, and Ba were found to be major contributors of non-carcinogenic risks, whereas Ni, Pb, and Zn contributed the least in both areas. In the Tibetan area, the non-carcinogenic risk induced by Mn was the lowest among all seven metals. In contrast, Mn was the second most significant contributor to non-carcinogenic risks in the Inner Mongolia region.
The total health risk of exposure to metals through drinking water for the different age groups in the two study areas is presented in Fig. 2. According to the results of this study, the total health risk in the Inner Mongolia region was much higher than that in the Tibetan Area. In both study areas, the total health risk in descending order was infant > adult > teenager > the elderly. As the most sensitive population, infants require dedicated attention. In this study, carcinogenic risk induced by Cr, As, and Cd exceeded the maximal acceptable risk level, indicating that carcinogenic risk from these three metals in drinking water is higher than the non-carcinogenic risk from seven metals from drinking water in both areas. This result is similar to most other related studies (Zhang et al. 2014a, b; Cao et al. 2015), but different from the study conducted in Shenzhen, China, which concluded that the non-cancer risk was higher than the cancer risk from heavy metals in drinking water (Lu et al. 2015).

The total health risk of exposure to metals through drinking water for different age groups in the two study areas
Correlation analysis
A correlation analysis was carried out to examine associations of selected elements in drinking water from the Tibetan area (Table S4) and the Inner Mongolia region (Table S5). In the Tibetan area, highly significant correlations were found between Co-Mn, Co-Ni, Cu-Ni, As-Ni, Ti-Ni, Ni-Tl, Cu-As, Cu-Ti, Cu-Tl, Zn-Cd, Ti-As, Tl-As, and Ti-Tl (p < 0.01). Significant correlations between Ba-Cr, Ni-V, Co-Cu, Be-Cu, Co-As, Co-Ti, Al-Co, and Be-Tl were also found (p < 0.05). Correlations among other elements were not significant (p > 0.05). Furthermore, strong positive correlations (r > 0.6) were found between Al-Co (r = 0.788), Cu-Ni (r = 0.946), As-Ni (r = 0.953), Ti- Ni (r = 0.718), Ni-Tl (r = 0.871), Cu-As (r = 0.955), Cu-Ti (r = 0.641), Cu-Tl (r = 0.866), Zn-Cd (r = 0.695), Ti- As (r = 0.698), Tl-As (r = 0.890), and Ti- Tl (r = 0.692). A negative association was found between Be-Cu (r = −0.386). Significant correlations were also noted between Ba-Cr (r = 0.360), Ni-V (r = 0.351), Co-Cu (r = 0.365), As-Co (r = 0.351), Co-Ti (r = 0.363), Be-Tl (r = 0.388), Co-Mn (r = 0.507), and Ni-Co (r = 0.446).
In the Inner Mongolia region, highly significant correlations were found between Tl-Mn, Cu-Co, Zn-Be, As-V, Cd-Sb, and Ba-V (p < 0.01). Significant correlations between Ni-Co, Ni-Ti and Ti-Tl were also found (p < 0.05). Correlations among other elements were not significant (p > 0.05). Strong positive associations (r > 0.6) were found between Zn-Be (r = 0.927), Cd-Sb (r = 0.812), As-V (r = 0.764), Cu-Co (r = 0.742), Mn-Tl (r = 0.733), Ba-V (r = 0.701), and Tl-Ti (r = 0.633). Significant correlations were also noted between Ni-Co (r = 0.554) and Ni-Ti (r = 0.524). These findings suggest that elements showing positive mutual associations were likely to be contributed by the same sources, while elements showing negative associations were found to have opposite distributions (Muhammad et al. 2014).
Probabilistic health risk assessment based on Monte-Carlo simulation
The uncertainty and variability were unavoidable in health risk assessment method. Therefore, a probabilistic health risk assessment based on Monte-Carlo simulation was introduced in this present research. The results of traditional certain health risk assessment model was compared with a probabilistic health risk assessment based on Monte-Carlo simulation to analyze the influence extent of parameter uncertainty. In addition, sensitivity analysis was also developed to estimate the relative contribution of related random variable. Four characteristic parameters were selected as random variable in this study, including concentration of heavy metals (C), body weight (W), average lifetime (Y), and ingestion rate of water (Q). Because almost 90 % of the total health risks were induced by Cr, and infants were the most susceptible to adverse health risks, RCr to infants were selected and evaluated using probabilistic health risk assessment based on Monte-Carlo simulation in this present study. Then, by building the factor probability distribution models of the parameters, the probabilistic health assessment was applied with the preferences of maximum number of trials 1000, confidence level 95 % and Latin hypercube sampling method.
The simulative figure of RCr based on health assessment method and Monte-Carlo simulation in Tibetan area and Inner Mongolia region was shown in Fig. S2. The interval value of health risks in Tibetan area and Inner Mongolia region induced by Cr were (3.86 × 10−5, 8.93 × 10−4), (1.36 × 10−4, 3.13 × 10−3), respectively, and the certain health risk assessment values in Tibetan area and Inner Mongolia region were 6.60 × 10−5 and 2.63 × 10−4, both of which were in their interval values. The values were all above the maximal acceptable risk level (1 × 10−6), indicating that the uncertainty of system parameters did not affect the decision making of pollution prevention and control.
Sensitivity analysis was conducted to evaluate the impact of the variability and uncertainty of parameters on the estimation of health risks induced by Cr in Tibetan area and Inner Mongolia region (Fig. S3). The sensitivity of four random variables in descending orders in Tibetan area and Inner Mongolia region were Q (49.8 %) > CCr (27.5 %) > W (−12.7 %) > Y (−10.1 %), Q (45.1 %) > CCr (33.8 %) > W (−13.8 %) > Y (−7.3 %), respectively. Ingestion rate of water and concentration of Cr appeared positive sensitivity, while body weight and average lifetime showed negative sensitivity. Moreover, the ingestion rate of water and concentration of Cr showed possibly high sensitivity to the health risks, suggesting that collecting local information of these two sensitive parameters to reduce their uncertainty can improve the reliability of results in further research.
Conclusion
The current study revealed that the concentrations of 16 trace elements in samples of water collected in the Tibetan area and the Inner Mongolia region were generally in accordance with quality standards (GB5749-2006), as only individual samples exceeded the standard values. Compared to other related studies in China, the mean levels of trace elements in drinking water in both study areas were relatively higher than the levels found in other areas. The health risk assessment indicated that the intake of water from the both areas might be a threat to the local population, as carcinogenic risks considerably exceeded the maximum recommended levels. The results revealed that carcinogenic risk is higher than non-carcinogenic risk from drinking water in both areas, and Cr was found to present the highest carcinogenic risk. Among the four population groups studied, infants were the most susceptible to adverse health risks. Correlation analysis reflected significant positive correlations among most elements, suggesting that the elements were likely to have common sources. Monte Carlo analysis indicates that the uncertainty of system parameters do not affect the decision making of pollution prevention and control, and sensitivity analysis shows that ingestion rate of water and concentration of Cr are the sensitive parameters, indicating that reducing the uncertainty can improve the reliability of results.
References
Alves RI, Carolina F et al (2014) Metal concentrations in surface water and sediments from Pardo River, Brazil: human health risks. Environ Res 133:149–155
Borum D, Abrnathy C (1994) Human oral exposure to inorganic arsenic. In: arsenic exposure and health. Environ Geochem Health 16:21–30
Cao SZ, Duan XL, Zhao XG, Wang BB et al (2015) Health risk assessment of various metal (loid)s via multiple exposure pathways on children living near a typical lead-acid battery plant, China. Environ Pollut 200:16–23
Ferré-Huguet N, Nadal M, Schuhmacher M, Domingo JL (2009) Human health risk assessment for environmental exposure to metals in the Catalan stretch of The Ebro River, Spain. Human Ecol Risk Assess 15:604–623
GB 3838–2002: Environmental quality standards for surface water (2002).
GB 5749–2006: Standards for drinking water quality (2006).
Haider D, Bhowmick S, Biswas A et al (2012) Risk of arsenic exposure from drinking water and dietary components: implications for risk management in rural Bengal [J]. Environ Sci Technol 47(2):1120–1127
IARC (1980) Arsenic and arsenic compounds. IARC Monogr Eval Carcinogen Risk Hum 23:39–141
Kavcar P, Sofuoglu A, Sofuoglu SC (2009) A health risk assessment for exposure to trace metals via drinking water ingestion pathway. Int J Hyg Environ Health 212:216–227
Lu XW, Zhang XL, Li YL, Chen H (2014) Assessment of metals pollution and health risk in dust from nursery schools in Xi’an China. Environ Res 128:27–34
Lu SY, Zhang HM, Samuel O et al (2015) Trace elements contamination and human health risk assessment in drinking water from Shenzhen, China. Environ Monit Assess 187:4220
Mondal D, Banerjee M, Kundu M et al (2010) Comparison of drinking water, raw nee and cooking of rice as arsenic exposure routes in three contrasting areas of West Bengal, India. Environ Geochem Health 32(6):463–477
Muhammad S, Shah MT, Khan S (2011) Health risk assessment of heavy metals and their source apportionment in drinking water of Kohistan region, northern Pakistan. Microchem J 98:334–343
Muhammad S, Javed I, and Munir HS (2014) Dissolved Concentrations, Sources, and Risk Evaluation of Selected Metals in Surface Water from Mangla Lake, Pakistan. The Scientific World Journal 948396.
Steinemann A (2000) Rethinking human health impact assessment. Environ Impact Assess Rev 20:627–645
Tang RL, Ma KM, Zhang YX, Mao QZ (2013) The spatial characteristics and pollution levels of metals in urban street dust of Beijing. China Appl Geochem 35:88–98
TWAS (Third World Academy of Sciences) (2002) Safe drinking water the need, the problem, solutions and an action plan, report of the Third World Academy of Sciences. Third World Academy of Science, Trieste Italy
US EPA (United States Environmental Protection Agency) (1986) Superfund Public Health Evaluation Manual. Washington DC
US EPA (United States Environmental Protection Agency) (1991) Risk assessment guidance for superfund Volume I-human health evaluation manual (Part B, development of risk based preliminary remediation goals). EPA-540-R-92-003. Washington DC
US EPA (United States Environmental Protection Agency) (2005) Guidelines for carcinogen risk assessment. EPA-603-P-03-001F, Washington DC
US EPA (United States Environmental Protection Agency) (2009) Exposure factors handbook. EPA-600-R-09-052A, Washington DC
US EPA (United States Environmental Protection Agency) (2000) Available information on assessment exposure from pesticides in food. U. S. Environmental Protection Agency Office of Pesticide Programs
WHO (2008) Guideline for Drinking Water Quality. In: Recommendations (third ed.) vol. 1. World Health Organization (WHO), Geneva
WHO (2011) Guideline for Drinking Water Quality (fourth ed.) World Health Organization (WHO), Geneva
Zhang NN, Zang SY, Sun Q (2014a) Health risk assessment of heavy metals in the water environment of Zhalong Wetland, China. Ecotoxicology 23:518–526
Zhang YL, Ma R, Li ZH (2014b) Human health risk assessment of groundwater in Hetao Plain (Inner Mongolia Autonomous Region, China). Environ Monit Assess 186:4669–4684
Zheng N, Liu JS, Wang QC, Liang ZZ (2010a) Health risk assessment of heavy metal exposure to street dust in the zinc smelting district, Northeast of China. Sci Total Environ 408:726–733
Zheng N, Liu JS, Wang QC, Liang ZZ (2010b) Heavy metals exposure of children from stairway and sidewalk dust in the smelting district, northeast of China. Atmos Environ 44:3239–3245
Acknowledgments
This research is financially supported by the China National Instrumentation Program (grant no. 2011YQ14015009).
Author information
Authors and Affiliations
Corresponding authors
Additional information
Responsible editor: Philippe Garrigues
Menghan Geng and Hongjuan Qi contributed equally to this work.
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(DOC 263 kb)
Rights and permissions
About this article

Cite this article
Geng, M., Qi, H., Liu, X. et al. Occurrence and health risk assessment of selected metals in drinking water from two typical remote areas in China. Environ Sci Pollut Res 23, 8462–8469 (2016). https://doi.org/10.1007/s11356-015-6021-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-015-6021-2