
Abstract
Purpose
Music has the potential to produce several performance-enhancing effects on the rating of perceived exertion (RPE) and power output, and these effects may be influenced by exercise intensity. The aim of this systematic review was to investigate the effects of music on RPE, peak and mean power during high-intensity intermittent exercise.
Methods
The databases searched for relevant studies included PubMed, Web of Science, Scopus, SportDiscuss, and PsycInfo, from their inception until December 2022.
Results
A total of 318 were found, 9 studies attained the eligibility criteria and were included in the final analyses. Eight studies applied a sprint interval exercise protocol and one applied a long-duration high-intensity interval exercise. Out of the six studies that measured the RPE, four reported no effect of music on this parameter. Four in six studies showed that music improved peak power and two in seven studies reported that music led to an improvement in mean power when compared to control conditions.
Conclusion
Therefore, music does not seem to reduce the RPE or increase mean power, but it appears to have the ability to increase peak power during high-intensity intermittent exercise. The choice of music and timing of the intervention are important considerations when manipulating music during high-intensity intermittent exercise.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The use of music during exercise can be traced back to Ancient Greece, when athletes used to listen to the flute or oboe while practicing it [1]. In recent years, the use of music as an ergogenic aid has been the focus of several research groups, and its effects have been studied [2,3,4]. It is proposed that music has a psychological aspect that may produce several performance-enhancing effects [2] such as reducing the rating of perceived exertion (RPE) [5, 6] and improving cycling performance, including peak and mean power [6, 7].
RPE and power output are relevant exercise variables in exercise that can be impacted by music. Decreasing RPE is related to delaying the onset of fatigue during an exercise session (e.g., reducing the physiological effects of acidosis) [6, 8], which can lead to longer exercise time and increased adherence to the recommended physical activity levels for health benefits [6]. Improving power output is crucial for enhancing performance and can be a useful strategy to maximize the benefits of a workout and promote continued participation in exercise training [3, 9].
The theoretical basis for the ergogenic effects of music on RPE and power output (performance) [5, 6, 10] during exercise is based on the parallel process model [11]. According to this model, the brain has a limited capacity to process sensory signals, and during exercise, an individual’s attentional focus is redirected towards the sensations of fatigue [12]. Additionally, the performance-enhancing effect of music appears to decrease as exercise intensity increases (due to changes in attentional focus) [11, 12]. This phenomenon can be explained by the increasing dominance of internal physiological clues over external psychological factors as an exercise session progresses [3, 10]. As a result, the distraction caused by external clues tends to decrease as the exercise intensity increases [7, 11, 12]. Therefore, it is possible to conclude that the ergogenic effects of music on RPE may vary depending on the intensity and duration of physical exercise. Some studies have used different high-intensity interval exercise (HIIE) protocols and reported no effects of music on RPE during this type of exercise [13, 14]. However, Ballmann, Maynard [5] found that RPE was lower with preferred music compared to non-preferred music during an HIIE session. They explained their results by suggesting that the right type of music may be crucial in achieving a significant effect on RPE during the HIIE, which is consistent with previous systematic reviews [3]. However, this study did not apply a no-music condition.
Despite reducing RPE, the same study by Ballmann, Maynard [5] found no improvement in peak and mean power. This is consistent with previous research [15], which has found that music interventions do not improve these key measures of power output during HIIE. However, based on the previously mentioned theoretical approach [11], it has been suggested that music during exercise may increase excitatory neurotransmitters such as serotonin and endorphins and counteract the exertional response [2, 12], leading to improved physical performance during HIIE [2, 3].
Hutchinson, Sherman [10] tested the hypothesis that music can improve physical performance during high-intensity exercise by submitting active subjects to a high-intensity exercise bout. The results showed that peak and mean power were significantly higher during the bout with music compared to a control condition without music. Subsequently, these findings were confirmed by other studies [5, 6].
HIIE consists of multiple high-intensity efforts (i.e., performed above maximal lactate steady state) interspersed with low-intensity or rest periods [16, 17]. HIIE has been linked to improved cardiorespiratory fitness [18] and reduced cardiometabolic risk factors in recent years [19]. This type of exercise can be used to improve health-related variables, but its high levels of effort and metabolites accumulation can deter non-athletic individuals from participating, as the relative high exertion may be perceived as too strenuous. HIIE is often reported to evoke negative perceptions due to its physiological demands [20, 21].
Moreover, music is readily accessible and easy to incorporate, but its effectiveness in decreasing RPE remains uncertain. Understanding the use of music during HIIE may provide an alternative way to reduce negative perceptions (such as higher than expected RPE) and increase exercise participation [4]. Additionally, given that music may also result in an initial increase in power output during HIIE, it is important to determine if this initial ergogenic effect remains effective throughout the entire exercise session [6]. This information can be valuable for trainers and practitioners to improve the use of music in a HIIE session. Therefore, the purpose this systematic review was to determine the effect of music on RPE, peak and mean power during an HIIE session in physically active non-athletic individuals. Our first hypothesis was that music would reduce RPE, and as a second hypothesis, we predicted that music would increase peak power and mean power during an HIIE session.
Methods
The methodology used in this systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The protocol was carried out according to the previously published and registered protocol in the PROSPERO database (CRD42020173309).
Search strategy and selection criteria
The inclusion criteria for studies in this systematic review were established based on the PICOS (Population, Intervention, Control, Outcome and Study Design) criteria [22]. The studies had to meet the following criteria: original articles involving adult human participants over 18 years of age who were not sedentary and not athletes (Population), investigating the effects of music on HIIE sessions (Intervention), with control conditions including sessions without music or other sound stimuli/music characteristics (Comparison), measuring the effects of music on RPE, peak and/or mean power (Outcome), and using a cross-over methodology (Study design). Studies that were considered grey literature, involved unhealthy subjects, athletes, or animals were excluded, while there were no language or geographical restrictions.
The authors (MM and NH) performed a manual search of the reference lists in the included articles to identify studies that could be eligible. When a review article was found, the authors also searched its reference lists to find any other relevant studies. The authors reviewed all identified publications either as abstracts or full texts.
The definition of HIIE in this study was based on the criteria set by Buchheit and Laursen [17]. Long duration HIIE (HIIEL): Efforts at intensities between sub-maximal markers (e.g. critical power/velocity, maximal lactate steady state, or anaerobic threshold) and maximal aerobic power, or between 80 and 95% of maximal heart rate, with durations of more than 1 min to 5 min, and work-to-rest ratios of 1:1, 1:2, or 1:3. Short duration HIIE (HIIES): efforts at intensities of around 100–120% of maximal aerobic power, with durations of 15–60s, and work-to-rest ratios of 1:1 or 2:1. Repeated sprint exercise (RSE): All-out efforts or around 120–170% of maximal aerobic power, with efforts of 3–8s, recovery periods of 20–60s, and work-to-rest ratios of around 1:8. Sprint interval exercise (SIE): all-out efforts or above 180% of maximal aerobic power, with efforts of 20–30s, recovery periods of 2–4 min, and work-to-rest ratios of around or greater than 1:6.
Procedures
A computerized search on PubMed, Web of Science, Scopus, SportDiscus and PsycInfo databases from inception to December 2022 was conducted. The search terms were adapted for each database to retrieve the maximum number of articles that met the PICOS criteria. The search terms used were a combination of “music” OR “song” AND “high intensity interval training” OR “high intensity interval exercise” OR “high intensity intermittent training” OR “high intensity intermittent exercise” OR “repeated sprint training” OR “sprint interval training” OR “interval training”. The search strategy and the results of each database are described in detail in Appendix A to ensure the transparency of the search process.
After the initial search, duplicates in studies were checked using Endnote Software 20 (Clarivate, London, UK). Then, two researchers independently evaluated the studies by reading titles and abstracts, selecting them based on the eligibility criteria.
Data extraction and synthesis
Two researchers (MM and NH) extracted data from the selected studies into a spreadsheet that included the following information: authors and publication year, sample size, age, anthropometric data, details of the exercise protocol (mode and intensity), details of the music and control condition protocols, and results (RPE and power output).
Risk of bias assessment
Two researchers (MM and NH) independently analyzed the risk of bias according to the Cochrane Handbook for Systematic Reviews of Interventions [23]. The procedures were carried out by evaluating the blinding of the assessed studies, including the blinding of authors’ names and affiliations, article titles, and journal publications. Subsequently, other sources of bias were taken into account, including random sequence generation and allocation sequence concealment (selection bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias) and selective reporting (reporting bias). Finally, the risk of bias was stratified as “low”, “high” or “unclear” for each study in each risk category.
Importantly, the criteria “blinding of participant and personal” were not evaluated because they are incompatible with the experimental design of the included studies. Figures 2 and 3 were created using the software Review Manager 5.3 (Cochrane Information Management System, Copenhagen, DK).
Results
Search results and included studies.
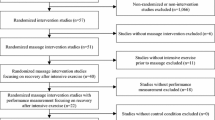
Initially, the search resulted in 318 studies: 99 were retrieved from PubMed, 96 from Web of Science, 56 from SCOPUS, 46 from SportDiscuss and 21 from PyscInfo. An additional 13 studies were inserted manually. After removing duplicates (264), 67 studies were screened based on their title and abstract, and 48 studies that did not meet the PICOS criteria (i.e., Non-HIIE interventions, non-crossover design, without RPE or power as outcomes) were excluded (Fig. 1). Finally, 19 studies were eligible for full reading.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart depicting the studies selection process
Of these 19 studies, 10 were excluded because they did not meet the purpose of the review: in four of these studies the subjects were athletes [13, 24,25,26] and in six used a protocol that was different from the HIIE types adopted in this systematic review [8, 10, 27,28,29,30]. The study by Stork and Ginis [14] met the inclusion criteria, but upon contacting the authors, they explained that this study presented secondary outcomes from a previous study [6]. As a result, RPE and power output data were the same for both studies. In the end, nine studies met the eligible criteria for methodological assessment and were included in the final systematic review (Fig. 1).
Quality of the selected studies
A summary of the risk of bias assessment for the nine included studies is presented in Figs. 2 and 3. As per evaluation, none of the studies were rated as having a high risk of bias. On the other hand, all 9 studies had an unclear risk for allocation concealment (selection bias) and blinding of outcome assessment (detection bias).

Summary of risk of bias of selected studies

Individual risk of bias of selected studies
Analyzing each study individually, in general, there were more unclear risk judgments (26, 57.7%) than low risk (19, 42.2%). In addition to the fact that none of the studies provided information on allocation concealment and blinding of outcome assessment, one study did not report whether there was randomization in experimental conditions order [5], and another reported that there was randomization but did not specify how it was done [15]. One study [31] did not provide information on conflicts of interest.
Studies characteristics
It should be noted that four out of the nine studies assessed both RPE and peak and/or mean power (Table 1), and as a result, some studies may be mentioned multiple times below. The studies that assessed the effects of music on RPE included 114 healthy participants, with 72 (63.2%) being males and 42 (36.8%) being females, with (mean ± standard deviation) age of 24.4 ± 3.3 years old, body mass of 73.7 ± 6.2 kg. The studies that assessed the effects of music on peak and/or mean power, included 215 healthy participants, with 153 (71.2%) being males and 62 (28.8%), being females, with an age of 23.0 ± 2.3 years old, body mass of 76.9 ± 8.4 kg. All values for age and body mass were calculated from the mean ± standard deviation values reported on the studies.
The present systematic review analyzed crossover studies that investigated the effects of music on RPE (n = 6), peak power (n = 6) and mean power (n = 7). Eight included studies applied a SIE type HIIE-protocol using cycle ergometer and one applied a HIIEL-protocol (Table 1). Although the protocols varied between studies, some examples include: 4 × Wingate Anaerobic Test (WanT) at 7.5% of body mass (BM) as load, interspersed by 120 s passive recovery [6]; 3xWanT at 7.5%BM interspersed by 30 s passive recovery [15]; 3 × 15s all-out bouts at 7.5%BM interspersed by 120 s active recovery unloaded [5]; 3 × 20 s all-out bouts at 5%BM interspersed by 120s active recovery at 50 watts (W) [7]; 2 × WanT at 7.5%BM interspersed by 10min self-paced recovery [32]; 8 × 60s at 100% peak wattage (Wmax) interspersed by 90s active recovery at 65–70 rotations per minute (rpm) with 50 W [33]; 4 min bouts at 80% peak power output (PPO) interspersed by 120s active recovery at 40%PPO [34]; 8 × 15s all-out at 9%BM interspersed by 120s passive recovery [35]. Finally, one study applied 2 × 20-s all-out SIE exercise, however, the authors did not report the full information of the protocol [31].
The conditions under which music was utilized also presented some variation among studies and, only one study did not apply a no-music condition as a control. Ballmann, Maynard [5] compared self-selected preferred music (favorite genre such as rhythm and blues, country, rock and roll/hard rock, rap/hip hop, pop, and dance/electronic on Billboard top 10 singles) versus non-preferred music (least favorite genre on the same ranking). All other included studies applied a no-music control condition (Table 2).
The moment at which RPE was measured also presented some variation between studies. Three studies measured RPE immediately after each bout [5,6,7, 35], and one also included measures before each bout and at the last 35s of the recovery phases [7]. Karageorghis, Jones [33] measured RPE at the last 15s of the effort phases and of the recovery phase, while Maddigan, Sullivan [34] measured RPE every minute during the 4-min bout.
Effects of music on rating of perceived exertion
Among the studies that assessed the effects of music on RPE, four out of six studies [6, 7, 34, 35] reported that music had no effect on RPE when compared with a no-music condition. On the other hand, two studies reported that RPE was lower in preferred compared to non-preferred music [5], and for medium-tempo music compared to no-music [33] (Table 2). It is important to highlight that the first [5] did not include a no-music condition as a control.
Effects of music on peak and mean power
Among the studies that assessed the effects of music on peak power, four out of seven studies [6, 7, 31, 32] reported that music increased peak power when compared with a control condition. Conversely, three studies reported no effects of music on peak power for the same comparisons [15, 35] (Table 2).
Among the studies that assessed the effects of music on mean power, two out of seven studies [6, 31] reported that music increased mean power when compared with a control condition. On the other hand, five studies reported no effects of music on mean power for the same comparisons [5, 7, 15, 32, 35] (Table 2). Although we recognize that total work is an important variable that can offer more relevant information concerning performance during an HIIE session, we did not explore it because only three out of the nine included studies reported this measurement [5, 31, 35].
Discussion
This systematic review was designed to analyze studies that assessed the effects of music on RPE, peak power, and mean power during an HIIE session in physically active non-athlete humans. The complex scenario did not allow us to confirm or refute the hypotheses definitively, as our findings tended slightly in one direction or the other. Music attenuated RPE solely in two out of the six studies that assessed this outcome, which does not confirm the hypothesis that music would decrease RPE. Music increased peak power in four out of the seven studies that assessed this outcome and increased mean power in two out of seven studies. It seems that our second hypothesis (music would increase peak and mean power) was partially confirmed.
Effects of music on RPE during a HIIE session
Several aspects might explain the absence of the ergogenic aid of music on RPE. According to previous reviews concerning music and exercise, people have a natural tendency to respond to the rhythm and motivational qualities of music, and this could promote a reduction in RPE and signs of fatigue [2,3,4]. As reported elsewhere [14], a reduction of circulating epinephrine is expected when listening to music during exercise. Indeed, this music effect could modulate the sympathetic nervous system tone and influencing the cardiac output and blood delivery through peripheral tissues. Thus, there was greater muscle efficiency and lowered RPE [2]. Nevertheless, exercise intensity plays an important role in mediating these effects on RPE.
SIE has an important anaerobic energy system contribution [36, 37] (phosphagen and glycolytic pathways) concomitantly with neuromuscular load demand, promoting higher RPE values when compared to other types of HIIE [17, 38]. Therefore, considering that five out of six studies included in this review applied an SIE protocol, the high exercise intensity probably diminished the distracting effect of external clues (music) [7, 11, 12]. Another possibility is that the music may have not been interesting enough to overpower the strenuous sensations caused by the SIE protocol [35]. This inference is based on the theory already mentioned, which suggests that the ergogenic effect of music appears to gradually decrease as exercise intensity increases [11]. Some studies have applied SIE protocols with several bouts consisting of all-out efforts (eight [33, 38], four [6] and three bouts [5, 7]) or a HIEEL until volitional exhaustion [34]. Such protocols could lead to an accumulation of fatigue throughout the session, thus diminishing the potential beneficial effects of music. Our systematic review endorses these inferences. However, we also speculate that participants enrolled in all-out efforts accelerate to peak quickly, working maximally from the start of the exercise bout, and rapidly fatiguing as a result [39], with a reduced cognitive component of the exercise task. Therefore, there is not enough time for the possible ergogenic effects of music to take place.
Although most studies reported null effects of music on RPE, two studies [5, 33] detected that music attenuated RPE during an HIIE session. In Ballmann, Maynard [5] study, RPE for each of the 3 all-out bouts did not differ between conditions (preferred vs. no-preferred music). However, the authors adopted a different approach to analyze this outcome comparing also the three-bout average RPE between conditions. One hypothesis is that perhaps the non-preferred music enhanced a greater associative thought of intensity, leading the individuals to perceive the session as more effortful. Therefore, a possible explanation of these different findings is the use of a non-preferred music playlist as a control condition. Thus, the absence of a no-music control condition could also bias the findings, as it is not possible to confirm that preferred music would attenuate RPE when compared to no music. In the other study [33], medium-tempo music applied during the recovery phase of the HIIE provoked a lower RPE at the 4th bout when compared to no music condition. The authors explained that this might be a carry-over effect from the recovery to the last bout, attenuating RPE. These different methodological strategies when analyzing the findings [5] or the moment of music intervention [33] might explain the diverging findings from both studies when compared to the others.
Previous evidence has shown that music preference may impact perceptual sensations during exercise [2], enhancing feelings of energy [5] and motivation [40]. Additionally, studies that have manipulated music preference show that the largest benefits of RPE are associated with music that is preferred [4]. On the opposite direction, non-preferred music might provoke detrimental effects on perceptual sensations, feelings of energy and motivation, besides the lack of ecological validity, as it is unlikely that people perform exercise listening to a self-selected music that they do not like [3]. Thus, it is plausible to infer that performing a SIE session under this condition (listening to non-preferred music) may trigger an even more negative perception, increasing the average RPE. Therefore, preferred music presented high average RPE values, but not as high as in the non-preferred condition. Moreover, applying non-preferred music seems to be different from applying a randomly selected music, since the latter did not promote negative effects on RPE during the SIE [35].
Concerning the procedures for selecting the music for the interventions, the studies tried to sustain their music selection based on the criteria proposed by Karageorghis, Jones [41]. In four studies [6, 7, 33], the Brunel Music Rating Inventory was used to measure, classify, and standardize the motivational components of music tracks during experimental exercise protocols [3]. Although these music selections were based on aspects as high tempo, cultural background, and genre, positive effects on RPE (that is, lower RPE) were not observed. Despite all four studies supporting their findings in the same direction [11], it is worthy to speculate that the training status of the participants might have underpowered the effects of music. Previous reports showed that music had significantly greater positive effects in untrained participants than in trained subjects [25]. Trained individuals would direct their focus toward internal cues and movement execution during exercise. Therefore, they would not be responsive to the music [42]. Furthermore, music seems to promote higher ergogenic effects at the beginning of a training program, with these effects diminishing throughout the evolution of the once untrained individuals [43]. Thus, considering the training status of the participants in the included studies (most were physically active), this may also explain the null effects of music on RPE.
Aggregating the findings from the studies that assessed the effects of music on RPE, which we included, it is feasible to infer that music does not attenuate RPE during an HIIE session. This inference is in line with other studies that systematically [3, 4] or critically [2] reviewed the effects of music on sports performance. When talking about HIIE protocols, it is clear that even the “perfect” music selection might not be sufficient to offset the physiological demands of an HIIE session and lower the RPE. Therefore, the inference proposed above must be interpreted with caution since the depth of the effects of music is related to the intensity and duration of the exercise protocol.
Effects of music on peak power and mean power during a HIIE session
The studies that assessed the effects of music on peak power presented debatable findings. Four of the six studies that assessed the effects of music on peak power [6, 7, 31, 32] supported their findings with the careful attention to the methodological approach with music selection and moment of intervention. The other two studies supported their null findings on the intensity of the HIIE protocols [15, 35]. Brooks and Brooks [31] emphasized two important points in music selection: (i) the use of music that is already considered traditionally motivational, and (ii) allowing the subjects to rank the music to determine its motivational value (self-selected). Later, Hutchinson, Sherman [10] inferred that the carefully selected music has the potential to significantly improve peak power and that poor methodology (i.e., weak musical selection procedures) likely contributed to the non-significant findings reported by previous studies [15].
Carefully selected music based on rhythm, musicality, cultural impact, and associated factors such as beats per minute is essential to measure whether music can provoke ergogenic effects on performance [2,3,4]. In a threefold study, motivational music (i.e., “Chariots of Fire” and “Eye of the Tiger”, which are commonly associated with feelings of motivation and striving to achieve) was found to be somewhat more motivating than others music types (i.e., rock and dance) [9], suggesting that the link between the type of music and performance under extreme physical demands such as high-intensity exercise may be moderated by the motivation that this music evokes in the performers [3].
Tenenbaum, Lidor [9] also proposed that there is a limit to the effect that music can promote, named the “mental threshold”, which is the point where music is no longer capable of shifting attention away from the physiological demands of exercise. Thus, the stronger the external stimulus, the further this threshold may move. Three of the six studies tested this hypothesis by assessing whether music could enhance peak power in multiple WanT bouts [6, 15, 32]. Although there were differences in the protocols, they reported an “initial burst of power” (i.e., higher peak power on the first three bouts under the music condition when compared to the no-music condition) that persisted over the course of repeated intervals. However, this inference might be interpreted with caution. The limits of “mental threshold” are not yet totally clear and are hard to determine when the personal safety of the exercisers is considered. First, when someone engages in strenuous exercise and listens to preferred music, it may result in better feelings at the beginning of the exercise but not during later stages when the physical effort is very high [9]. The melody and rhythm of the music are associated with enjoyment and divert attention from the physiological demands experienced during the HIIE session at its outset and middle phase, but much less at the end of the effort [9]. Therefore, it is challenging to determine the threshold of the effects of music on performance given the number of personal variables involved in choosing the ideal song for each individual.
Differently from peak power, the mean power outcome across the included studies seems to be more conclusive. Among studies that reported ergogenic effects of music on mean power [6, 31], the authors interpreted their findings in a similar way to peak power. Brooks and Brooks [31] argued that, considering that WanT is only 30s long, the music appears to delay fatigue over the test, as shown by the higher mean power values in the music condition, which might be explained by the initial burst of power at the beginning of the bout. Thus, it is expected that mean power calculated over the entire test was affected. It is possible that music may provide enough impetus to the performance that participants are motivated or energized to start the task strongly, but this effect diminishes as the task progresses [10]. In this sense, Stork, Kwan [6] applied four WanT and found that music elicited a heightened and optimal state of arousal leading into the first WanT bout. The authors further inferred that the continuous play of music during the entire session, including warm-up, during bouts and rest periods), may have created additive effects for each of the four bouts and partially explain why the effects of music persisted for multiple WanT bouts.
In the opposite direction, five studies found null effects of music on mean power [5, 7, 15, 32, 35]. Also, in line with the inferences reported above, authors agreed that depending on intensity [15] or protocol configuration [7], the possible music ergogenic effects may be diminished or even insignificant. One may argue that the different duration and intensity of the recovery phase (120-s active recovery unloaded [5], 120-s active recovery with 50 W [7] or 30-s passive recovery [15]) among protocols could lead to differences in mean power output. However, these differences did not result in increases in mean power, although the study with the longer recovery duration [32] presented a higher peak power in the music condition. Finally, Ballmann, Maynard [5] supported their findings in the similarity in music tempo (bpm) between preferred and no-preferred music conditions, which could lead to similarities in terms of stimulation during the HIIE session. Karageorghis and Priest [4] suggested that music may not moderate what one feels during HIIE (i.e., RPE), but it can moderate how one feels it; our findings support this proposal. Although the majority of the included studies did not identify positive effects on RPE, performance was moderately improved during the HIIE session. Diverging from previous reviews, our findings on performance do not allow us to attest that music enhances performance.
As a possible strategy to practitioners and to exercise scientists applying music to increase the chances of promoting a reduction on RPE or improving power output during a HIIE protocol, it is possible to suggest some strategies, including: (i) carefully selecting the music (high tempo, preferred, and motivational); (ii) playing music before the first bout and keeping it playing during all protocol (effort and recovery moments); and (iii) setting up an HIIE protocol with a few bouts (i.e., two to three).
Methodological quality of included studies
Although none of the studies were judged to present a high risk of bias, the methodological quality of the included studies is predominantly unclear. Therefore, it is uncertain whether the knowledge of the experimental conditions order by the subjects can influence the phenomena studied by this systematic review. Studies have shown that when individuals are mentally prepared for a motor task, they are capable of improving both their motor performance and psychological outcomes [44,45,46]. All of the included studies also did not report whether the outcome assessment was blinded, which is a common issue in exercise sciences [47, 48]. The lack of information about blinding during data analysis is a concern in the health sciences area in general [49] because when the result assessment is not blind, studies tend to present exaggerated intervention effects [50,51,52]. Two of the studies also did not clearly report the random sequence generation process clearly, or if they did, they did not report how it was done [5, 15]. Therefore, a random sequence of session orders in a counterbalanced way, as reported by the other half of included studies, guarantees equal and balanced opportunities for participants so that the session order does not interfere with their outcomes [53]. Despite the predominance of unclear risk judgments, there were also criteria that enhanced the reliability of the results of studies included in general, such as low risk of attrition and reporting bias.
Limitations and future projects
Based on the findings of the present systematic review, it is recommended for future studies to provide greater clarity in the music selection and in the description of experimental design, including detailed procedures for preventing selection and detection bias. Additionally, other precautions should be taken, such as a better description of the sample. All studies included in this systematic review used only age, body mass, and training status to characterize the sample. A more detailed description regarding body composition and physical fitness can be fundamental for a better understanding of the outcomes, as both factors are associated with the modulation of psychological responses to exercise [54, 55]. Furthermore, all original studies analyzed young adults. Thus, future studies might investigate other age groups (e.g., adolescents, elderly) since physiological and affective responses may vary across different age ranges.
A recent discussion concerning RPE anchors was proposed, aiming to anchor the upper limits appropriately [56] (i.e., 6–20 Borg scale, 20 is anchored as “maximal effort” and 19 is “…extremely strenuous exercise level”; for CR10, 10 is anchored as “…extremely strenuous exercise level”). Two of the studies included in this review reported that specific orientation had been given [6, 7] (“participants were carefully instructed to report how they felt during the final few seconds of the exercise”), and one was extremely careful when measuring RPE [33] (“The participant was prompted to report RPE…in the last 15 s of each of the eight bouts of high-intensity exercise and in the last 15 s of each recovery period”). Considering that some studies applied 6–20 scales [34, 35], others CR10 [5,6,7, 33] and it was not clear if specific guidance was given, this could limit more conclusive findings. Future studies that apply RPE scales to quantify physical effort during an HIIE session could consider standardizing the anchors of the scales to better control of this measure.
Despite the limitations, such as the number of studies that fit the established PICOS criteria, this systematic review could contribute to the knowledge within this field. We summarized the possible effects of music in RPE, peak and mean power outputs on physically active subjects during an HIIE protocol and identified common methodological errors. Additionally, this systematic review could offer guidance to trainers and exerciser practitioners seeking to understand the effects of using music as an ergogenic aid during an HIIE session.
Conclusions
After systematically reviewing the literature, our findings leaned slightly in one direction. It appears that music is not able to reduce RPE in physically active subjects, as only two out of the six studies that assessed this outcome, was the RPE attenuated by music. Regarding the effects of music on performance outcomes, four out of six studies indicated that music was able to improve peak power, and two out of five studies reported that music promoted an improvement in mean power. Thus, music seems to improve peak power; however, it is not able to improve mean power.
Data availability
All relevant data are presented in the manuscript.
References
Van Looy H (1993) The Festivals. In: Bertelsmann J (ed) Olympism in Antiquity Musee Olympique Lausanne. Quai d’Ouchy, Lausanne, pp 23–28
Franco-Alvarenga PE, Brieztke C, Canestri R, Pires FO (2019) Psychophysiological responses of music on physical performance: a critical review. Rev Bras Ciênc Mov 27(2):218–224
Karageorghis CI, Priest DL (2012) Music in the exercise domain: a review and synthesis (Part I). Int Rev Sport Exerc Psychol 5(1):44–66
Karageorghis CI, Priest DL (2012) Music in the exercise domain: a review and synthesis (Part II). Int Rev Sport Exerc Psychol 5(1):67–84
Ballmann CG, Maynard DJ, Lafoon ZN, Marshall MR, Williams TD, Rogers RR (2019) Effects of listening to preferred versus non-preferred music on repeated wingate anaerobic test performance. Sports 7(8):185
Stork MJ, Kwan MY, Gibala MJ, Ginis KA (2015) Music enhances performance and perceived enjoyment of sprint interval exercise. Med Sci Sports Exerc 47(5):1052–1060
Stork MJ, Karageorghis CI, Ginis KAM (2019) Let’s Go: psychological, psychophysical, and physiological effects of music during sprint interval exercise. Psychol Sport Exerc. https://doi.org/10.1016/j.psychsport.2019.101547
Karlovic M, Jaksic M, Baric R (2016) Effect of motivational music on psychological and physiological responses during high-intensity interval training. Int J Sport Psychol 47(6):571–584
Tenenbaum G, Lidor R, Lavyan N, Morrow K, Tonnel S, Gershgoren A et al (2004) The effect of music type on running perseverance and coping with effort sensations. Psychol Sport Exerc 5(2):89–109
Hutchinson JC, Sherman T, Davis L, Cawthon D, Reeder NB, Tenenbaum G (2011) The influence of asynchronous motivational music on a supramaximal exercise bout. Int J Sport Psychol 42(2):135–148
Rejeski WJ (1985) Perceived exertion–an active or passive process. J Sport Psychol 7(4):371–378
Bigliassi M (2015) Use the brain: complementary methods to analyse the effects of motivational music. Front Hum Neurosci 9:3
Jones L, Tiller NB, Karageorghis CI (2017) Psychophysiological effects of music on acute recovery from high-intensity interval training. Physiol Behav 170:106–114
Stork MJ, Ginis KAM (2017) Listening to music during sprint interval exercise: the impact on exercise attitudes and intentions. J Sports Sci 35(19):1940–1946
Pujol TJ, Langenfeld ME (1999) Influence of music on wingate anaerobic test performance. Percept Mot Skills 88(1):292–296
Julio UF, Panissa VLG, Paludo AC, Alves ED, Campos FAD, Franchini E (2020) Use of the anaerobic speed reserve to normalize the prescription of high-intensity interval exercise intensity. Eur J Sport Sci 20(2):166–173
Buchheit M, Laursen P (2013) High-intensity interval training, solutions to the programming puzzle: Part I: cardiopulmonary emphasis. Sports Med 43(5):313–338
Sultana RN, Sabag A, Keating SE, Johnson NA (2019) The effect of low-volume high-intensity interval training on body composition and cardiorespiratory fitness: a systematic review and meta-analysis. Sports Med 49(11):1687–1721
Andreato LV, Esteves JV, Coimbra DR, Moraes AJP, de Carvalho T (2019) The influence of high-intensity interval training on anthropometric variables of adults with overweight or obesity: a systematic review and network meta-analysis. Obes Rev 20(1):142–155
Decker ES, Ekkekakis P (2017) More efficient, perhaps, but at what price? Pleasure and enjoyment responses to high-intensity interval exercise in low-active women with obesity. Psychol Sport Exerc 28:1–10
Hardcastle SJ, Ray H, Beale L, Hagger MS (2014) Why sprint interval training is inappropriate for a largely sedentary population. Front Psychol. https://doi.org/10.3389/fpsyg.2014.01505
Tacconelli E (2010) Systematic reviews: CRD’s guidance for undertaking reviews in health care. Lancet Infect Dis 10(4):226
Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD et al (2011) The cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ Br Med J. https://doi.org/10.1136/bmj.d5928
Chtourou H, Jarraya M, Aloui A, Hammouda O, Souissi N (2012) The effects of music during warm-up on anaerobic performances of young sprinters. Sci Sports 27(6):e85–e88
Eliakim M, Meckel Y, Nemet D, Eliakim A (2007) The effect of music during warm-up on consecutive anaerobic performance in elite adolescent volleyball players. Int J Sports Med 28(4):321–325
Rendi M, Szabo A, Szabo T (2008) Performance enhancement with music in rowing sprint. The Sport Psychologist 22(2):175–182
Guerrero C, Tran R, Gutierrez E, Campbell C, Rodgers J, Alencar M et al (2020) Metabolic costs of a 58 minute multi-intensity exercise session with and without music and cueing. Int J Exerc Sci 13(2):358–365
Atan T (2013) Effect of music on anaerobic exercise performance. Biol Sport 30(1):35–39
Loizou G, Karageorghis CI (2015) Effects of psychological priming, video, and music on anaerobic exercise performance. Scand J Med Sci Sports 25(6):909–920
Yamamoto T, Ohkuwa T, Itoh H, Kitoh M, Terasawa J, Tsuda T et al (2003) Effects of pre-exercise listening to slow and fast rhythm music on supramaximal cycle performance and selected metabolic variables. Arch Physiol Biochem 111(3):211–214
Brooks K, Brooks K (2010) Difference in wingate power output in response to music as motivation. J Exer Physiol Online. 13(6).
Hutchinson JC, O’Neil BJ (2020) Effects of respite music during recovery between bouts of intense exercise. Sport Exerc Perform Psychol 9(1):102
Karageorghis CI, Jones L, Howard LW, Thomas RM, Moulashis P, Santich SJ (2021) When it hiits, you feel no pain: psychological and psychophysiological effects of respite–active music in high-intensity interval training. J Sport Exerc Psychol 43(1):41–52
Maddigan ME, Sullivan KM, Halperin I, Basset FA, Behm DG (2019) High tempo music prolongs high intensity exercise. Peer J 6:e6164
Marques M, Staibano V, Franchini E (2022) Effects of self-selected or randomly selected music on performance and psychological responses during a sprint interval training session. Sci Sports 37(2):139–149
Gillen JB, Gibala MJ (2014) Is high-intensity interval training a time-efficient exercise strategy to improve health and fitness? App Physiol Nutr Metab 39(3):409–412
Malta E, Brisola G, Poli R, Dutra Y, Franchini E, Zagatto A (2018) Metabolic profile and performance responses during two consecutive sessions of sprint interval training. J Strength Cond Res 34(4):1078–1085
Marques M, Alves E, Henrique N, Franchini E (2020) Positive affective and enjoyment responses to four high-intensity interval exercise protocols. Percept Mot Skills 127(4):742–765
Martin K, Thompson KG, Keegan R, Ball N, Rattray B (2015) Mental fatigue does not affect maximal anaerobic exercise performance. Eur J App Physiol 115(4):715–725
Ballmann CG, McCullum MJ, Rogers RR, Marshall MM, Williams TD (2018) Effects of preferred vs. nonpreferred music on resistance exercise performance. J Strength Cond Res. https://doi.org/10.1519/JSC.0000000000002981
Karageorghis CI, Jones L, Low DC (2006) Relationship between exercise heart rate and music tempo preference. Res Q Exerc Sport 77(2):240–250
Eliakim M, Bodner E, Eliakim A, Nemet D, Meckel Y (2012) Effect of motivational music on lactate levels during recovery from intense exercise. J Strength Cond Res 26(1):80–86
Hamburg J, Clair AA (2003) The effects of a movement with music program on measures of balance and gait speed in healthy older adults. J Music Ther 40(3):212–226
Hammoudi-Nassib S, Nassib S, Chtara M, Briki W, Chaouachi A, Tod D et al (2017) Effects of psyching-up spint on performance. J Strength Cond Res 31(8):2066–2074
Paravlic AH, Slimani M, Tod D, Marusic U, Milanovic Z, R. P. (2018) Effects and dose-response relationships of motor imagery practice on strength development in healthy adult populations: a systematic review and meta-analysis. Sports Med 48(5):1165–1187
Tempest G, Parfitt G (2013) Imagery use and affective responses during exercise: an examination of cerebral hemodynamics using near-infrared spectroscopy. J Sport Exerc Psychol 35(5):503–513
Brietzke C, Franco-Alvarenga PE, Coelho HJ, Silveira R, Asano RY, Pires FO (2019) Effects of carbohydrate mouth rinse on cycling time trial performance: a systematic review and meta-analysis. Sports Med 49(1):57–66
Silveira R, Prado RCR, Brietzke C, Coelho-Junior HJ, Santos TM, Pires FO et al (2019) Prefrontal cortex asymmetry and psychological responses to exercise: a systematic review. Physiol Behav. https://doi.org/10.1016/j.physbeh.2019.112580
Kahan BC, Rehal S, Cro S (2015) Blinded outcome assessment was infrequently used and poorly reported in open trials. PloS One. https://doi.org/10.1371/journal.pone.0131926
Hrobjartsson A, Thomsen ASS, Emanuelsson F, Tendal B, Hilden J, Boutron I et al (2012) Observer bias in randomised clinical trials with binary outcomes: systematic review of trials with both blinded and non-blinded outcome assessors. Bmj Brit Med J. https://doi.org/10.1136/bmj.e1119
Hrobjartsson A, Thomsen ASS, Emanuelsson F, Tendal B, Hilden J, Boutron I et al (2013) Observer bias in randomized clinical trials with measurement scale outcomes: a systematic review of trials with both blinded and nonblinded assessors. Can Med Associ J 185(4):E201–E211
Hrobjartsson A, Thomsen ASS, Emanuelsson F, Tendal B, Rasmussen JV, Hilden J et al (2014) Observer bias in randomized clinical trials with time-to-event outcomes: systematic review of trials with both blinded and non-blinded outcome assessors. Int J Epidemiol 43(3):937–948
Suresh K (2011) An overview of randomization techniques: An unbiased assessment of outcome in clinical research. J Hum Reproduct Sci 4(1):8–11
Alvarez-Alvarado S, Chow GM, Gabana NT, Hickner RC, Tenenbaum G (2019) Interplay between workload and functional perceptual-cognitive-affective responses: an inclusive model. J Sport Exerc Psychol 41(2):107–118
Yanez-Sepulveda R, Barraza-Gomez F, Baez-San Martin E, Araneda OF, Zavala JP, Hecht GK et al (2018) Differences in energy expenditure, amount of physical activity and physical exertion level during a Zumba fitness class among adult women who are normal weight, overweight and obese. J Sports Med Phys Fit 58(1–2):113–119
Malleron T, Har-Nir I, Vigotsky AD, Halperin I (2023) Rating of perceived effort but relative to what? a comparison between imposed and self-selected anchors. Psychol Sport Exerc. https://doi.org/10.1016/j.psychsport.2023.102396
Acknowledgements
The authors would like to thank the Coordination of Improvement of Higher Education Personnel (CAPES/Brazil) for the scholarship conferred to MM (doctoral) and to the National Council for Scientific and Technological Development (CNPQ) to NH (masters).
Funding
No funding has been received for this research.
Author information
Authors and Affiliations
Contributions
MM had the idea of the article. MM and NH performed the literature search, studies election, data extraction and analysis. MM and NH wrote the first version of the manuscript. EF and MT critically reviewed the manuscript. All authors are in agreement with the final version.
Corresponding author
Ethics declarations
Conflict of interest
All authors declare no potential or actual conflicts of interest. It is an original piece of work. It has not been previously published in full or partially. It is not under review in any other publication.
Ethical approval and informed consent
For this type of study, informed consent and ethical approval are not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Marques, M., Henrique, N., Takito, M. et al. Effects of music on perceptive and performance responses during high-intensity exercise: a systematic review. Sport Sci Health 20, 727–738 (2024). https://doi.org/10.1007/s11332-024-01189-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11332-024-01189-6