
Abstract
Purpose
Static stretching (SS) improves flexibility but may impair the accuracy of joint position sense. Therefore, this study aimed to investigate the acute effects and time course of SS on the accuracy of joint position sense, range of motion (ROM), and muscle–tendon unit (MTU) stiffness.
Methods
This study randomly assigned 16 healthy, young males to the SS and control conditions. SS intervention in the SS condition was performed on the plantar flexors of the dominant leg for three sets of 60 s. The participants were instructed to sit for 240 s in the control condition. The ankle dorsiflexion (DF) ROM, passive torque at DF ROM, MTU stiffness, and joint position sense on the dominant leg side were measured before (PRE) and immediately (POST) and at 5, 10, and 20 min postintervention.
Results
A significant interaction effect was observed in the relative error in the joint position sense, and significant increases were noted in POST compared to PRE in the SS condition. Further, significant interactions were observed in DF ROM, passive torque at DF ROM, and MTU stiffness. The SS condition demonstrated significant increases in DF ROM and passive torque at DF ROM compared to PRE with POST, 5 min, and 10 min, and MTU stiffness significantly decreased in POST compared with PRE.
Conclusion
Our results indicated that the accuracy of the joint position sense decreased immediately after SS, but returned to baseline in a very short time.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Static stretching (SS) is a prevalent stretching method in rehabilitation and sports settings, and many previous studies have revealed that SS increased range of motion (ROM) and decreased muscle–tendon unit (MTU) stiffness [1,2,3,4]. Additionally, reduced flexibility, such as decreased ROM [5] and increased MTU stiffness [6, 7], caused sports injury. Therefore, SS is frequently performed as part of a warm-up to prevent sports injuries [8,9,10].
The acute effect of SS may alter the accuracy of joint position sense in addition to improving flexibility. Joint position sense is recognized when information is input from proprioceptors in all body parts [11, 12]. Walsh et al. reported that 90 s of SS intervention on the quadriceps and hamstrings reduced the absolute value of the error from the target angle at 20° and 45° knee flexion, regarding the effect of SS on the accuracy of joint position sense [13]. The results indicated an improved accuracy of joint position sense after SS. However, Larsen et al. revealed that a 90 s SS intervention for the quadriceps and hamstrings did not significantly alter the relative values to the target angle at 50° and 70° knee flexion [14]. Thus, studies that defined the outcome of the accuracy of joint position sense as the absolute value of the error from the target angle revealed improvement immediately after SS [13, 15], while the studies that defined the outcome as the relative value of the error from the target angle revealed no improvement immediately after SS [14]. Therefore, there is no consensus on whether or not SS improves the accuracy of joint position sense. Some previous studies suggest that absolute error, not relative error, should be analyzed in joint position sense measurements [16], but there are also scattered previous studies that measure relative error in addition to absolute error [17, 18]. Since absolute error alone cannot take into account the direction of error, it may be desirable to include relative error in the measurement in order to examine joint position sense in detail. Joint position sense has been involved in the risk of ankle joint disorders [19, 20], balance function [21, 22], and sports performance [23, 24]. Therefore, changes in the accuracy of joint position sense immediately after SS may affect these factors. Additionally, from the warm-up perspective, the time course of change in the accuracy of the joint position sense after SS is crucial information. Studies investigated the time course of the effects of SS on passive properties, such as ROM and MTU stiffness [3, 25], but no studies evaluated the accuracy of joint position sense.
Therefore, this study aimed to investigate the acute effects and time course of SS on the accuracy of joint position sense, ROM, and MTU stiffness. Concerning joint position sense, we hypothesized, based on previous studies, that the absolute value of the error from the target angle improves immediately after SS [13, 15]. However, the relative value of the error does not change [14]. Regarding flexibility, we hypothesized that an increase in ROM would persist longer than a decrease in MTU stiffness, based on previous studies [3].
Methods
Participants
The objectives of the study were fully explained to the participants, and those who were interested were recruited. The participants included 16 healthy, nonathletic, sedentary young males (age: 21.4 ± 3.1 years, height: 169.7 ± 4.2 cm, weight: 65.3 ± 8.6 kg). The target muscles included the plantar flexor muscles of the dominant ankle joints. The dominant leg was the preferred leg for kicking the ball [26]. The inclusion criteria were no regular resistance training within the past 6 months, no neuromuscular disease, and no orthopedic disease history [27]. None of the participants were competitive athletes or engaged in regular resistance training or stretching programs for the lower limbs [28]. The required sample size for a repeated-measure two-way analysis of variance (ANOVA) (effect size [ES] = 0.25 [middle], α error = 0.05, and power = 0.8) using G* power 3.1 software (Heinrich Heine University, Düsseldorf, Germany) was more than 14 participants. Thus, 16 participants were recruited to account for possible attrition. All participants were briefed on the study's purpose and procedures, and written consent was obtained from each participant. The Ethical Review Committee of Niigata University of Health and Welfare approved this study (Ethics Approval Number: #18,561).
Experimental set-up
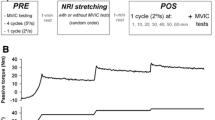
We used a randomized repeated-measures experimental design to compare the effects of SS over time in the (1) SS and (2) control conditions. SS was administered to the plantar flexors on the dominant foot side in the SS condition. Participants completed the two conditions in a random order, with the order randomly determined. The participants were instructed to visit the laboratory two times, with a ≥ 48 h break. The SS intervention was performed for three sets of 60 s each, with a 30 s rest between sets. The participants in the control condition were instructed to sit for 240 s. We measured the joint position sense, dorsiflexion (DF) ROM, passive torque at DF ROM, and MTU stiffness before (PRE) and immediately after (POST) and at 5, 10, and 20 min postintervention. POST measurements were performed immediately after SS intervention. Joint position sense was measured after measuring flexibility in PRE. Flexibility was calculated after measuring joint position sense in the POST, 5, 10, and 20 min (Fig. 1).

Experimental flow chart
Assessment of the DF ROM, passive torque at DF ROM, and MTU stiffness
DF ROM, passive torque at DF ROM, and MTU stiffness were measured as flexibility indices. The participants were secured in a seated position on the chair of an isokinetic dynamometer (Biodex System 3.0, Biodex Medical Systems, Inc., Shirley, NY, USA) with a 0° knee angle. Moreover, the trunk and pelvis of the participant were secured with a belt while the participant was reclined (70° hip angle) to prevent tension at the back of the knee [29] (Fig. 2). Thereafter, the dynamometer footplate was passively and isokinetically dorsiflexed at a speed of 5°/s from the 30° plantar flexion position to DF and stopped just before the participant started to feel discomfort or pain. Participants stopped the dynamometer after two familiarization trials by activating a safety trigger when they started to feel discomfort or pain, with the angle just before this point defined as the DF ROM [29, 30]. Stretch tolerance is the passive torque at DF ROM [3, 31]. Additionally, surface electrodes (Blue Sensor N, Ambu A/S, Ballerup, Denmark) were applied to the medial gastrocnemius muscle to confirm the absence of voluntary contraction of the ankle plantar flexor muscles, and electromyography (FA-DL-720–140; 4Assist, Tokyo, Japan) was performed to confirm muscle activity [32].

Starting limb position for measuring flexibility
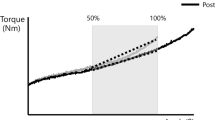
MTU stiffness was calculated from the same ankle DF angle range pre and postintervention. The calculated ankle DF angle range was the preintervention angle from the 50% maximum ankle DF angle to the maximum ankle DF angle [33]. However, the MTU stiffness pre and postintervention was calculated from the postintervention 50% maximum ankle DF angle to the maximum ankle DF angle if the maximum ankle DF angle measured postintervention was smaller than that measured preintervention. These were measured once at each time point, and the obtained values were used for statistical analysis.
Assessment of joint position sense
The starting limb position was the same as in the assessment of flexibility indices (Fig. 2). The angle obtained from the DF ROM measurement was defined as 100%, and the 50% angle was defined as the target angle. First, participants were asked to memorize the target angle while their vision was obstructed by an eye mask (10s of three sets). The ankle joint was passively dorsiflexed (angular velocity: 5°/s) from 30° plantar flexion with the footplate of the dynamometer while wearing an eye mask in PRE and POST, 5, 10, and 20 min after the measurements, and the actual angular values of the angle that the participant felt reached the target angle were calculated. The relative error, which is the value obtained by subtracting the target angle from the measured angle, and absolute error, which is the absolute difference between the measured angle and the target angle, were calculated [17]. Three measurements were taken at each period, and the average value obtained was used for statistical analysis.
Static stretching Interventions
The plantar flexor muscle on the dominant side was passively stretched using a dynamometer in the SS condition, similar to the DF ROM measurements. A previous study [34] indicated that the ankle joint with the dynamometer in passive mode (angular velocity: 5°/s) from the 30° plantarflexion angle to the angle could be tolerated to the maximum extent without pain or discomfort. Participants performed the SS intervention for three sets of 60 s each, with a 30 s rest between sets.
Measurement reliability
The test–retest reliability for all dependent variables was measured in eight men (mean age: 21.9 ± 1.1 years, height: 168.9 ± 4.7 cm, and body weight: 65.7 ± 10.1 kg) who have not participated in the study before data collection. The two tests were separated by 2–7 days and conducted at the same time of the day (± 1 h). The intraclass correlation coefficients revealed high reliability for all measures (DF ROM: 0.92; passive torque at DF ROM: 0.95; MTU stiffness: 0.96; relative error: 0.91; and absolute error: 0.82).
Statistical analysis
Statistical Package for the Social Sciences (version 28.0; SPSS Japan Inc., Tokyo, Japan) was used for statistical analysis. The Shapiro–Wilk test was used to test data normality. The values for each variable followed normality. The paired-sample t-test of variance was used for each variable to reveal that the PRE values did not differ among the conditions. All outcome variables were subjected to a two-way repeated-measures ANOVA (time [PRE vs. POST vs. 5 min vs. 10 min vs. 20 min] and conditions [SS vs. Control]) to calculate interaction effects. If no significant interaction was found, the main effect was examined. Classification of ES was set where ηp2 of < 0.01 was considered small, 0.02–0.1 was considered medium, and > 0.1 was considered a large effect size [35]. Posthoc tests were performed using multiple comparison tests with Bonferroni correction to confirm a significant interaction effect to determine differences between PRE, POST, and 5, 10, and 20 min. Additionally, we calculated Cohen’s d ES as differences in the mean value divided by the pooled SD between PRE and POST, and 5, 10, and 20 min postintervention in each condition. ES of 0.00–0.19, 0.20–0.49, 0.50–0.79, and ≥ 0.80 were considered as trivial, small, moderate, and large, respectively [35]. The significance level was set to 5%, and all results are presented as the mean ± SD.
Results
Comparison of variables during PRE in each condition
The PRE values revealed no significant differences between the two conditions for any variable.
Changes in joint position sense
Table 1 shows the results of the relative error and absolute error PRE, POST, and 5, 10, and 20 min for each condition. Relative error demonstrated a significant interaction effect (p < 0.001, F = 10.7, ηp2 = 0.416). The posthoc test results revealed a significant increase compared to PRE and POST (p = 0.012, d = 0.91) after the intervention in the SS condition. However, PRE and 5 (p = 1.000, d = 0.20), 10 (p = 0.636, d = 0.41), or 20 min (p = 1.000, d = 0.22) demonstrated no significant differences in the SS condition. The control conditions were not significantly different between PRE and POST (p = 0.678, d = − 0.23), 5 min (p = 1.000, d = 0.17), 10 min (p = 1.000, d = 0.20), and 20 min (p = 0.282, d = 0.41).
The absolute error revealed no interaction effect (p = 0.066, F = 2.33, ηp2 = 0.135). Additionally, no significant main effect for time (p = 0.113, F = 1.95, ηp2 = 0.115) and condition (p = 0.379, F = 0.82, ηp2 = 0.052).
Changes in DF ROM, passive torque at DF ROM, and MTU stiffness
Table 2 shows the results of DF ROM, passive torque at DF ROM, and MTU stiffness at PRE, POST, and 5, 10, and 20 min in each condition. DF ROM demonstrated a significant interaction effect (p < 0.001, F = 10.7, ηp2 = 0.417). The posthoc test results revealed a significant increase compared with PRE and POST (p < 0.001, d = 0.63), 5 min (p = 0.003, d = 0.43), and 10 min (p = 0.02, d = 0.32) postintervention in the SS condition. However, PRE and 20 min (p = 0.256, d = 0.29) were not significantly different in the SS condition. Control conditions were not significantly different between PRE and POST (p = 1.000, d = − 0.15), 5 min (p = 0.554, d = − 0.19), 10 min (p = 1.000, d = − 0.17), and 20 min (p = 0.536, d = − 0.29).
Passive torque in DF ROM demonstrated a significant interaction effect (p = 0.004, F = 4.26, ηp2 = 0.221). The posthoc test results revealed a significant increase compared with PRE and POST (p < 0.001, d = 0.60), 5 min (p < 0.001, d = 0.58), and 10 min (p = 0.005, d = 0.46) postintervention in the SS condition. However, PRE and 20 min (p = 0.056, d = 0.41) were not significantly different in the SS condition. Control conditions demonstrated no significant difference between PRE and POST (p = 1.000, d = 0.11), 5 min (p = 1.000, d = 0.05), 10 min (p = 1.000, d = 0.12), or 20 min (p = 1.000, d = 0.02).
MTU stiffness demonstrated a significant interaction effect (p < 0.001, F = 6.03, ηp2 = 0.287). The posthoc test results revealed a significant increase compared to PRE and POST (p = 0.043, d = − 0.30) after intervention in the SS condition. However, PRE and 5 (p = 1.000, d = 0.00), 10 (p = 1.000, d = 0.04), or 20 min (p = 1.000, d = 0.01) were not significantly different in the SS condition. Control conditions demonstrated no significant difference between PRE and POST (p = 1.000, d = 0.10), 5 min (p = 0.079, d = 0.12), 10 min (p = 1.000, d = 0.08), or 20 min (p = 0.556, d = 0.11).
Discussion
This study investigated the accuracy, passive properties, acute effect, and time course of SS on joint position sense. The results revealed that 180 s of SS intervention increased DF ROM and passive torque at DF ROM for > 10 min and returned to baseline after 20 min. Conversely, an increased relative error of joint position sense (error in the forward direction, i.e., overestimated) and a decrease in MTU stiffness were observed acutely but returned to baseline within 5 min. Therefore, the results confirm the hypothesis of this study that the accuracy of joint position sense decreases immediately after SS, but the effect returns to baseline within a short period, which is shorter than the effect of increased ROM. To the best of our knowledge, this is the first study to investigate changes in the accuracy of joint position sense and changes in passive properties concerning the acute effects and time course of SS.
An overestimation of joint position sense was observed immediately after SS in the SS condition, but the effect returned to baseline within 5 min. A previous study revealed that tendon tap reflex (T-reflex) significantly decreased by performing a 1 min SS on plantar flexor muscles [36]. T-reflex indicates the sensitivity of muscle spindles [37], and SS may alter the sensitivity of muscle spindles and reduce the accuracy of joint position sense. Additionally, joint position sense overestimation may be due to the sensitivity change of muscle spindles caused by the decrease in MTU stiffness. Muscle spindles, which are one of the intrinsic receptors, are largely responsible for sensations associated with muscle length and length changes [38]. Moreover, the intramuscular fibers of muscle spindles exhibited thixotropic properties [39]. Thixotropy refers to materials that change their physical properties due to being moved or “after-effects [39, 40]. This study revealed significantly reduced MTU stuffiness in SS conditions. Therefore, SS may have altered the thixotropic properties of intramuscular fibers in muscle spindles, affecting the perception of muscle length and muscle length changes, which may have been overestimated. Furthermore, joint position sense overestimation may have returned to baseline within 5 min because the SS-induced changes in muscle spindles returned to baseline within a short period. A previous study revealed that a 5-min SS on plantar flexor muscles reduced T-reflexes, which returned to baseline within 10 min [41]. Additionally, this study revealed that the decrease in MTU stiffness in the SS condition returned to baseline within 5 min, which time course of change was consistent with joint position sense overestimation. These results indicate quickly reversed SS-induced changes in muscle spindle sensitivity.
The PRE value of relative error may be involved in the absence of a significant interaction in absolute error in this study. The absolute error is calculated as the absolute value of the error from the target angle. For participants with a negative PRE value for relative error (error in the backward direction, i.e., underestimated), the absolute error may decrease as the SS changes the joint position sense to the forward direction. This may be a factor, and the absolute error, unlike the relative error, may not have had a significant interaction effect.
This study revealed that DF ROM and passive torque at DF ROM increased for > 10 min and returned to baseline after 20 min in SS condition. Conversely, MTU stiffness decreased acutely but returned to baseline within 5 min. Therefore, the increase in ROM due to SS may persist longer than the decrease in MTU stiffness. Mizuno et al. revealed that after 300 s of SS for the ankle plantar flexors, DF ROM increased for > 30 min [3], but the decrease in MTU stiffness returned to baseline within 10 min [42]. These results indicate that the increase in ROM with SS lasts longer than the decrease in MTU stiffness. Sensations, such as pain and discomfort tolerance (i.e., stretch tolerance), have been reported to be a factor for increased ROM in addition to mechanical properties such as MTU stiffness [31]. Passive torque at DF ROM was an indicator of the stretch tolerance [3, 31], thus stretch tolerance may be mainly involved in the sustained effect of SS on ROM increase.
This study revealed joint position sense overestimation immediately after SS, and thus the accuracy of the joint position may decrease immediately after SS. SS is frequently performed as part of a warm-up to prevent sports injuries by improving flexibility [8,9,10]. Conversely, joint position sense has been involved in the risk of ankle joint disorders [19, 20], balance function [21, 22], and sports performance [23, 24]. Therefore, performing SS in warm-up may increase the risk of disability associated with worsened accuracy of joint position sense and decreased balance function and performance, considering the results of this study. However, this study revealed that joint position sense overestimation due to SS was reversed within 5 min, indicating that the decrease in accuracy of the joint position sense due to SS was recovered in a very short time. Therefore, to minimize the risk of sports injury, attention should be paid to the first 5 min after static stretching, and it may be desirable to perform dynamic stretching instead of static stretching.
This study has several limitations. The present study included healthy adult males with no exercise habits. Therefore, the results of this study may not apply to females, the elderly, or athletes. Future studies should focus on different participants. Additionally, this study did not use neurophysiological indices such as H-reflex and T-reflex. Thus, future studies should measure H-reflex and T-reflex and investigate the detailed mechanism by which SS reduces the accuracy of joint position sense. The results of this study indicate the decreased accuracy of the joint position sense immediately after SS. The extent to which the decrease in accuracy of the joint position sense due to SS adversely affects performance and other factors remains unknown. Further study is required to identify the negative impact of the decrease in accuracy of the joint position sense due to SS on performance and other factors.
Conclusion
This study examined the acute effects and time course of SS on the accuracy of passive properties and joint position sense. The results revealed joint position sense overestimation immediately after SS, but the effect quickly reversed. Compared to the decrease in MTU stiffness, the effect of SS on ROM increase persisted longer. Notably, the accuracy of the joint position sense decreases immediately after SS when performing SS as a warm-up.
Data availability
No datasets were generated or analysed during the current study.
Abbreviations
- SS:
-
Static stretching
- ROM:
-
Range of motion
- MTU:
-
Muscle–tendon unit
- DF:
-
Dorsiflexion
- PRE:
-
Before static stretching intervention
- POST:
-
Immediately after static stretching intervention
- T-reflex:
-
Tendon tap reflex
References
Fukaya T, Nakamura M, Sato S, Kiyono R, Yahata K, Inaba K et al (2020) The relationship between stretching intensity and changes in passive properties of gastrocnemius muscle-tendon unit after static stretching. Sports. https://doi.org/10.3390/sports8110140. (Epub 20201023 PubMed PMID: 33113901; PubMed Central PMCID: PMCPMC7690681)
Matsuo S, Suzuki S, Iwata M, Banno Y, Asai Y, Tsuchida W et al (2013) Acute effects of different stretching durations on passive torque, mobility, and isometric muscle force. J Strength Cond Res. 27(12):3367–76 (Epub 2013/03/26 PubMed PMID: 23524367)
Mizuno T, Matsumoto M, Umemura Y (2013) Viscoelasticity of the muscle-tendon unit is returned more rapidly than range of motion after stretching. Scand J Med Sci Sports 23(1):23–30 (PubMed PMID: 21564309)
Takeuchi K, Nakamura M (2020) Influence of high intensity 20-second static stretching on the flexibility and strength of hamstrings. J Sports Sci Med 19(2):429–35 (Epub 2020/05/12 PubMed PMID: 32390737; PubMed Central PMCID: PMCPMC7196737)
Witvrouw E, Danneels L, Asselman P, D’Have T, Cambier D (2003) Muscle flexibility as a risk factor for developing muscle injuries in male professional soccer players a prospective study. Am J Sports Med. 31(1):41–6 (PubMed PMID: 12531755)
Ekstrand J, Gillquist J (1983) The avoidability of soccer injuries. Int J Sports Med 4(2):124–128. https://doi.org/10.1055/s-2008-1026025. (PubMed PMID: 6874174)
Watsford ML, Murphy AJ, McLachlan KA, Bryant AL, Cameron ML, Crossley KM et al (2010) A prospective study of the relationship between lower body stiffness and hamstring injury in professional Australian rules footballers. Am J Sports Med. 38(10):2058–64 (Epub 2010/07/03. PubMed PMID: 20595555)
Behm DG, Blazevich AJ, Kay AD, McHugh M (2016) Acute effects of muscle stretching on physical performance, range of motion, and injury incidence in healthy active individuals: a systematic review. Appl Physiol Nutr Metab 41(1):1–11 (Epub 20151208. doi: 10.1139/apnm-2015-0235. PubMed PMID: 26642915)
Ebben WP, Hintz MJ, Simenz CJ (2005) Strength and conditioning practices of Major League Baseball strength and conditioning coaches. J Strength Cond Res 19(3):538–546. https://doi.org/10.1519/r-15464.1. (PubMed PMID: 16095401)
Simenz CJ, Dugan CA, Ebben WP (2005) Strength and conditioning practices of National Basketball Association strength and conditioning coaches. J Strength Cond Res 19(3):495–504. https://doi.org/10.1519/15264.1. (PubMed PMID: 16095396)
Carpenter JE, Blasier RB, Pellizzon GG (1998) The effects of muscle fatigue on shoulder joint position sense. Am J Sports Med 26(2):262–265. https://doi.org/10.1177/03635465980260021701. (PubMed PMID: 9548121)
Ribeiro F, Mota J, Oliveira J (2007) Effect of exercise-induced fatigue on position sense of the knee in the elderly. Eur J Appl Physiol 99(4):379–85. https://doi.org/10.1007/s00421-006-0357-8. (Epub 20061213. doi: 10.1007/s00421-006-0357-8. PubMed PMID: 17165054)
Walsh GS (2017) Effect of static and dynamic muscle stretching as part of warm up procedures on knee joint proprioception and strength. Hum Mov Sci 55:189–95. https://doi.org/10.1016/j.humov.2017.08.014. (PubMed PMID: 28841537)
Larsen R, Lund H, Christensen R, Røgind H, Danneskiold-Samsøe B, Bliddal H (2005) Effect of static stretching of quadriceps and hamstring muscles on knee joint position sense. Br J Sports Med 39(1):43–46. https://doi.org/10.1136/bjsm.2003.011056. (PubMed PMID: 15618341; PubMed Central PMCID: PMCPMC1725022)
Ghaffarinejad F, Taghizadeh S, Mohammadi F (2007) Effect of static stretching of muscles surrounding the knee on knee joint position sense. Br J Sports Med 41(10):684–7. https://doi.org/10.1136/bjsm.2006.032425. (PubMed PMID: 17510229; PubMed Central PMCID: PMCPMC2465159)
Costello JT, Donnelly AE (2010) Cryotherapy and joint position sense in healthy participants: a systematic review. J Athl Train 45(3):306–316. https://doi.org/10.4085/1062-6050-45.3.306. (PubMed PMID: 20446845; PubMed Central PMCID: PMCPMC2865970)
Furmanek MP, Słomka KJ, Sobiesiak A, Rzepko M, Juras G (2018) The effects of cryotherapy on knee joint position sense and force production sense in healthy individuals. J Hum Kinet 61:39–51 (Epub 20180323 PubMed PMID: 29599858; PubMed Central PMCID: PMCPMC5873335)
Salgado E, Ribeiro F, Oliveira J (2015) Joint-position sense is altered by football pre-participation warm-up exercise and match induced fatigue. Knee 22(3):243–8 (Epub 20150408. PubMed PMID: 25864146)
Kobayashi T, Tanaka M, Shida M (2016) Intrinsic risk factors of lateral ankle sprain: a systematic review and meta-analysis. Sports Health 8(2):190–193. https://doi.org/10.1177/1941738115623775. (PubMed PMID: 26711693; PubMed Central PMCID: PMCPMC4789932)
Witchalls J, Blanch P, Waddington G, Adams R (2012) Intrinsic functional deficits associated with increased risk of ankle injuries: a systematic review with meta-analysis. Br J Sports Med. 46(7):515–23. https://doi.org/10.1136/bjsports-2011-090137. (Epub 20111214 PubMed PMID: 22171337)
Bouisset S, Do MC (2008) Posture, dynamic stability, and voluntary movement. Neurophysiol Clin. 38(6):345–62. https://doi.org/10.1016/j.neucli.2008.10.001. (Epub 20081018 PubMed PMID: 19026956)
Pasma JH, Boonstra TA, Campfens SF, Schouten AC, Van der Kooij H (2012) Sensory reweighting of proprioceptive information of the left and right leg during human balance control. J Neurophysiol. 108(4):1138–48. https://doi.org/10.1152/jn.01008.2011. (PubMed PMID: 22623486)
Han J, Anson J, Waddington G, Adams R, Liu Y (2015) The role of ankle proprioception for balance control in relation to sports performance and injury. Biomed Res Int. 2015:842804. https://doi.org/10.1155/2015/842804. (Epub 20151025 PubMed PMID: 26583139; PubMed Central PMCID: PMCPMC4637080)
Han J, Anson J, Waddington G, Adams R (2014) Sport attainment and proprioception. Int J Sports Sci Coach 9(1):159–170
Hatano G, Suzuki S, Matsuo S, Kataura S, Yokoi K, Fukaya T et al (2019) Hamstring stiffness returns more rapidly after static stretching than range of motion, stretch tolerance, and isometric peak torque. J Sport Rehabil. 28(4):325–31 (Epub 20181203 10.1123/jsr.2017-0203 PubMed PMID: 29252096)
Sato S, Hiraizumi K, Kiyono R, Fukaya T, Nishishita S, Nunes JP et al (2020) The effects of static stretching programs on muscle strength and muscle architecture of the medial gastrocnemius. PLoS One 15(7):e0235679 (Epub 20200709 10.1371/journal.pone.0235679. PubMed PMID: 32645095; PubMed Central PMCID: PMCPMC7347101)
Yahata K, Konrad A, Sato S, Kiyono R, Yoshida R, Fukaya T et al (2021) Effects of a high-volume static stretching programme on plantar-flexor muscle strength and architecture. Eur J Appl Physiol 121(4):1159–66. https://doi.org/10.1007/s00421-021-04608-5. (PubMed PMID: 33502614)
Nakamura M, Yahata K, Sato S, Kiyono R, Yoshida R, Fukaya T et al (2021) Training and detraining effects following a static stretching program on medial gastrocnemius passive properties. Front Physiol 12:656579 (PubMed PMID: 33868026; PubMed Central PMCID: PMCPMC8049289)
Nakamura M, Sato S, Hiraizumi K, Kiyono R, Fukaya T, Nishishita S (2020) Effects of static stretching programs performed at different volume-equated weekly frequencies on passive properties of muscle-tendon unit. J Biomech 103:109670 (Epub 20200131. doi: 10.1016/j.jbiomech.2020.109670. PubMed PMID: 32035662)
Nakamura M, Sato S, Kiyono R, Yoshida R, Murakami Y, Yasaka K et al (2021) Acute effect of vibration roller with and without rolling on various parts of the plantar flexor muscle. Front Physiol 12:716668 (Epub 20210922. doi: 10.3389/fphys.2021.716668. PubMed PMID: 34630141; PubMed Central PMCID: PMCPMC8493118)
Weppler CH, Magnusson SP (2010) Increasing muscle extensibility: a matter of increasing length or modifying sensation? Phys Ther. 90(3):438–49. https://doi.org/10.2522/ptj.20090012. (Epub 20100114. doi: 10.2522/ptj.20090012. PubMed PMID: 20075147)
Nakamura M, Ikezoe T, Takeno Y, Ichihashi N (2013) Time course of changes in passive properties of the gastrocnemius muscle-tendon unit during 5 min of static stretching. Man Ther. 18(3):211–5. https://doi.org/10.1016/j.math.2012.09.010. (Epub 2013/01/09. doi: 10.1016/j.math.2012.09.010. PubMed PMID: 23294911)
Takeuchi K, Takemura M, Nakamura M, Tsukuda F, Miyakawa S (2022) The effects of using a combination of static stretching and aerobic exercise on muscle tendon unit stiffness and strength in ankle plantar-flexor muscles. Eur J Sport Sci. 22(2):297–303 (Epub 20210118. doi: 10.1080/17461391.2020.1866079. PubMed PMID: 33331805)
Nakamura M, Yoshida R, Sato S, Yahata K, Murakami Y, Kasahara K et al (2021) comparison between high- and low-intensity static stretching training program on active and passive properties of plantar flexors. Front Physiol 12:796497 (Epub 20211217. doi: 10.3389/fphys.2021.796497. PubMed PMID: 34975544; PubMed Central PMCID: PMCPMC8718681)
Cohen J (1988) Statistical power analysis for the behavioral sciences. Hillsdale Routledge, Hillsdale
Budini F, Gallasch E, Christova M, Rafolt D, Rauscher AB, Tilp M (2017) One minute static stretch of plantar flexors transiently increases H reflex excitability and exerts no effect on corticospinal pathways. Exp Physiol. 102(8):901–10. https://doi.org/10.1113/ep086374.PubMedPMID:28585766. (Epub 20170630)
Proske U, Morgan DL, Gregory JE (1993) Thixotropy in skeletal muscle and in muscle spindles: a review. Prog Neurobiol 41(6):705–721. https://doi.org/10.1016/0301-0082(93)90032-n. (PubMed PMID: 8140258)
Proske U, Gandevia SC (2012) The proprioceptive senses: their roles in signaling body shape, body position and movement, and muscle force. Physiol Rev 92(4):1651–1697. https://doi.org/10.1152/physrev.00048.2011. (PubMed PMID: 23073629)
Proske U, Tsay A, Allen T (2014) Muscle thixotropy as a tool in the study of proprioception. Exp Brain Res 232(11):3397–412. https://doi.org/10.1007/s00221-014-4088-5. (PubMed PMID: 25200179)
Hagbarth KE, Hägglund JV, Nordin M, Wallin EU (1985) Thixotropic behaviour of human finger flexor muscles with accompanying changes in spindle and reflex responses to stretch. J Physiol 368:323–342. https://doi.org/10.1113/jphysiol.1985.sp015860. (PubMed PMID: 2934547; PubMed Central PMCID: PMCPMC1192599)
Budini F, Kemper D, Christova M, Gallasch E, Rafolt D, Tilp M (2019) Five minutes static stretching influences neural responses at spinal level in the background of unchanged corticospinal excitability. J Musculoskelet Neuronal Interact 19(1):30–7 (PubMed PMID: 30839301; PubMed Central PMCID: PMCPMC6454261)
Mizuno T, Matsumoto M, Umemura Y (2013) Decrements in stiffness are restored within 10 min. Int J Sports Med 34(6):484–90 (PubMed PMID: 23143704)
Acknowledgements
The authors gratefully acknowledge all participants involved in this study.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
YM contributed to study design and data collection, and drafted the manuscript, and made critical revision to the manuscript. KK, and RY contributed to data collection and made critical revisions to the manuscript. KT, SM, TM, and MN contributed to study design, data analysis and made critical revisions to the manuscript. All authors approved the final version of the manuscript and agreed to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Conflict of interests
No conflict of interest.
Ethical approval
The study was approved by the Ethical Review Committee of Niigata University of Health and Welfare (Ethics Approval Number: #18561).
Consent to participate
All subjects provided written informed consent after being fully informed of the procedures and purpose of the study.
Consent for publication
The participant in the picture provided written informed consent that the picture can be published.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Murakami, Y., Kasahara, K., Yoshida, R. et al. Time course of changes in passive properties and joint position sense after static stretching. Sport Sci Health 20, 881–889 (2024). https://doi.org/10.1007/s11332-024-01172-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11332-024-01172-1