
Abstract
Introduction
Falls are very common among the elderly and can lead to high levels of morbidity and other adversities. Given the importance of preventing falls, it is suggested that physical activity can contribute to preventing such events.
Objective
To investigate the protective effect of physical exercise on episodes of falls in the elderly and, after long follow-up intervals without other interventions, to examine the effectiveness of exercise.
Method
This systematic review and meta-analysis of randomised clinical trials reporting only interventions in physical exercise and falls in the elderly searched the SPORTDiscus, PubMed, Scopus, Web of Science, and Cochrane databases for articles published until July 2022. Meta-regression was used to investigate the post-intervention time and the quality of studies on the effect of physical exercise on falls. Heterogeneity was calculated using the I2 statistic. Forest plot and funnel plot were used to represent the fall incidence rate ratio and subgroup analysis.
Results
Physical exercise alone was not enough to protect against falls, but the follow-up period without intervention proved significant in protecting against falls (0.83; CI 95% 0.75–0.92).
Conclusion
Short interventions without follow-up were not enough to protect against falls, but interventions via physical exercise showed a protective effect on falls in the elderly when there was follow-up after long periods without interventions, only follow-up.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
For some years, many countries have been observed to be undergoing a demographic transition [1]. In addition, world population growth in recent decades relates primarily to increasing life expectancy in developed countries. And under development [2]. Estimates indicate that from 1950 to 2050, the world population will have increased 3.7 times, whereas the elderly population will have increased ten times [3]. Projections also indicate that between 2010 and 2050, the elderly population will have increased by 1.3 billion [3, 4].
Given that the elderly already make up a considerable part of the population, numerous studies have focused on this age group, seeking to understand the phenomenon of aging [4]. However, there is a necessary delay in understanding the economic, social, and health implications of aging [5], because the aging process brings with it progressive loss of muscle mass, resulting in significant reduction in strength from the 6th decade of life onward [6]. Skeletal muscle in the elderly tends to be less powerful, weaker, and slower, in addition to being less stable during isometric contractions [7]. There are indications that some habits, such as diet and physical activity, can slow these aging-related conditions [8]. In this regard, investigations into the lifestyle of individuals in this age group can explore behaviour that delays the damage caused by aging and highlight chronic pathologies and accidents in everyday life. Falls are one of the major causes of mortality and morbidity among the elderly [9]. Worldwide, about 37.3 million serious falls per year require medical attention [9]. The Global Burden of Disease—GBD (2017) show a global age-standardised fall incidence rate of 2.23 per 100,000 [10]. The high frequency of such episodes also reflects in increased demand for health services, because severe events can result in loss of independence and increased likelihood of death [11, 12]. It is thus essential to investigate risk and protective factors, because falls can sometimes be avoided, thus reducing the economic burden of fall-related injuries [13].
Given the potential severity of falls in older adults, numerous researchers have turned to studying accident prevention. The literature suggests that regular physical exercise decreases the risk of falling [14]. In addition, exercise is cost-effective in preventing falls [15]. Furthermore, studies have observed the protective effect of physical exercises against falling, especially studies of interventions aiming to improve balance [16,17,18,19]. However, the most significant protection was observed in studies of interventions involving physical exercise, medical care, and environmental changes [17, 19]. Several types of physical exercise, when practiced in this age group, can develop components of physical fitness that prevent falls and related aggravation of some diseases [17]. Aerobic and resistance training tend to contribute to functional mobility and balance, and combat muscle mass loss, in addition to strengthening especially the lower muscles, which can help prevent falls [20, 21]. Several meta-analyses [18, 19] have shown the effect of physical exercise in protecting the elderly from falls. However, most studies that only involved physical exercise. They selected studies that used multifactorial interventions combining exercise with medication, psychological interventions, environmental changes, nutritional therapy, and so on. It has also yet to be investigated how long the protective effect of exercise lasts after the intervention [18, 19]. Since few meta-analyses have investigated the post-intervention follow-up period, there is little evidence of the duration of this protective effect. Given these issues, there is understood to be a need to investigate whether interventions based only on physical exercise during a specific period can prevent falls among the elderly. To that end, this article examines the protective effect of physical exercise on fall episodes in the elderly and analyses the effectiveness of exercise after long follow-up intervals without intervention.
Method
Protocols and search strategy
This systematic review was performed to the Preferred Reporting Items for Systematic Reviews and Meta-analyses [PRISMA] guidelines and the protocol was registered in the Prospective International Registry of Systematic Reviews [PROSPERO] database [No. CRD42020197589]. With a view to covering a significant number of studies, the search in the scientific literature was not limited to specific languages. The search keywords were checked against the Medical Subject Headings [MeSH] and Descriptors in Health Sciences [DeCS] health science glossaries. After verification, the Boolean expression [[[[Older adults] AND [Exercise]] AND [Accidental falls]] AND [Randomised Controlled Trial] was applied to the SPORTDiscus, PubMed, Scopus, Web of Science, and Cochrane databases, for articles published until July 2022.
Inclusion criteria and selection process
Initially, titles and abstracts of selected articles were extracted. Subsequently, those which met the following inclusion criteria were selected for further analysis:
-
1.
Follow-up randomised controlled trials of exercise-only interventions in older adults over 60 years old at all sites.
-
2.
Interventions involving physical exercise for at least 2 months.
-
3.
Elderly monitored for at least 1 year during the entire study and at least 6 months after the intervention.
-
4.
Studies with outcomes including falls in the elderly and minimal prior follow-up.
There should not be any issues if the intervention and follow-up extend beyond the minimum duration initially considered. Nevertheless, studies lacking quantitative details regarding the follow-up period, such as the number of individuals in follow-up and estimations regarding this timeframe, will be excluded from the meta-analysis. Articles with little information about the intervention and outcomes were excluded. Studies of specific populations or of samples with large numbers of older adults with neurodegenerative diseases [such as Parkinson's, Alzheimer's, stroke and others] were also excluded. If the title or abstract raised doubts as to the inclusion criteria, the reviewers accessed the full text for evaluation. If doubt remained, a third reviewer was admitted. Whenever an article was not available in full, the first author was contacted by e-mail.
Data synthesis and extraction
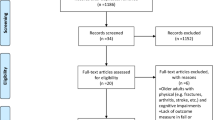
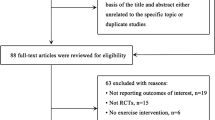
Initial searches returned 2722 articles, as follows: SPORTDiscus, n = 40; Scopus, n = 1181; Web of Science, n = 113; PubMed, n = 1062; Cochrane, n = 326. Duplicates were excluded. Titles and abstracts were then accessed to identify compatibility; the 88 articles compatible with the initial inclusion criteria were retrieved in full. Of these, 22 were eligible, and 66 were excluded for not meeting the inclusion criteria.
Quality of studies
The PEDro [Physiotherapy Evidence Database] scale was used to gauge the studies’ methodological quality. The scale classifies articles by eleven items, with a total score ranging from 0 to 10 [as the first item, which assesses the study’s external validity, is not counted]. This item was included so that all items on the Delphi scale would be represented on the PEDro scale, although the purpose of this scale is not to assess studies’ external validity. Scores are awarded only when a criterion is clearly met. Two researchers, working independently, evaluated each item and any disagreements were arbitrated by a third evaluator [22].
Data analysis [meta-analysis]
Meta-analysis was performed to investigate the effect of physical exercise on falls in the elderly. The post-intervention period was also investigated to detect possible consequences in this follow-up period. Nonstandard weighted and 95% confidence intervals [95% CI] were calculated using random-effect meta-analysis, using the incidence rate ratio as a measure of effect. Subgroup analysis was then performed to investigate whether different kinds of intervention—single [one type of physical exercise] and combined [a combination of at least two types of physical exercise]—would affect falls differently. Meta-regression also sought to investigate the role of post-intervention time and study quality in the effect of physical exercise on falls. Heterogeneity was calculated using the I2 statistic, which indicates the proportion of variability between studies that cannot be attributed to chance alone. Forest and funnel plots were used to represent the fall incidence rate ratio and the subgroup analysis. All analyses were conducted using the META package of R software, version 4.1.2.
Results
The search strategy identified 22 studies for inclusion in the systematic review, 14 of which were included in the meta-analysis, Fig. 1 shows the study selection flowchart. All studies were carried out between 2004 and 2021. Seventeen studies involved older adults of both sexes, while five used samples of women only. In half of the studies, participants were 70 years old or older [n = 11]. As regards the nature of the interventions, some studies comparing different physical exercise programmes also used more than one experimental group [n = 10], and some studies used more than two comparison arms [n = 7]. The most frequently observed interventions were tai chi chuan [n = 7] and strength and balance training [n = 14]. Intervention duration ranged from 3 months to 2 years. Exercise sessions generally took place twice weekly [n = 13] and lasted 60 min [n = 11]. PEDro scale scores ranged from 4 to 9 points, but most studies [n = 9] scored 6 points. Six of the studies selected found no significant differences in fall reduction. More details of the selected studies can be seen in Table 1.

Identification of studies via databases and registrations
The effect of physical exercises on the incidence rate of falls in the elderly was not significant [0.86 95% CI 0.73–1.02] [Fig. 2]. The effect of single exercises was 0.82 [95% CI 0.56–1.21], while the effect of combined exercises was 0.88 [95% CI 0.70–1.06]. This and other information can be seen in Fig. 3. The effect of physical exercise on incidence rate ratio for falls in the elderly obtained from studies that showed estimates during the post-intervention follow-up period was 0.83 [95% CI 0.75–0.92]. In some studies that continued follow-up observation after the intervention [but performed no further intervention], physical activity significantly reduced the incidence of falls. This and other information can be seen in Fig. 4. The meta-regression found that follow-up period duration did not influence the effect of physical exercise on falls [0.0008; 95% CI 0.0092–0.0107]. However, another meta-regression showed that the study quality influenced the effect of exercise on falls [− 0.1907; 95% CI, − 0.2974–0.0840]. The funnel plot in Fig. 5 suggested some asymmetry and it is thus possible that bias will be found among the selected studies. Note that less accurate studies, with small samples, appear in the broadest part of the funnel. This is the case with only one of the selected studies.

Forest graph of the fall incidence rate ratio, using randomized design meta-analysis

Forest plot of fall incidence rate ratio using subgroup analysis between single activities and combined activities

Forest plot of fall incidence rate ratio using random-effect meta-analysis—follow-up period

Funnel plot showing SE and effect size (incidence rate ratio) in falls prevention exercise trials
Discussion
This study investigated the protective effect of physical exercise against fall episodes in the elderly. The results indicated that, when analysed together, the interventions performed in the selected randomised clinical trials were insufficient to demonstrate a significant protective effect of physical exercise on falls. However, when studies that continued to observe individuals for a long time after the intervention period [but without performing further interventions] were considered, a significant reduction in the incidence of falls was noted. Also, the selected articles often mentioned different types of physical exercise, the duration of the interventions and the relationship with sex. The systematic review highlighted conflicts in the literature on falls in the elderly, such as the protection against falls provided by physical exercise, where some interventions indicated significant protection and others did not [23,24,25]. Freiberg and collaborators (2007), in a study of 217 older adults between 70 and 90 years old, evaluated the effectiveness of two interventions [one focused on body awareness and the other on physical conditioning]. After 4 months of intervention and 12 months of follow-up, the conditioning intervention showed a significant reduction in falls compared to the control group [23].
By contrast, the other intervention showed no significant reductions. This illustrates that the type and intensity of exercise can promote different kinds of protections [23]. Comparing types of physical exercise to prevent falls is related to the development of motor and cognitive valences provided by each modality [26,27,28,29]. Eggenberg and collaborators (2015) investigated 71 older people. They administered three types of intervention [virtual reality dancing, treadmill walking, and treadmill walking with memory training], together with strength and balance exercises, for 6 months. After 1 year follow-up, they noted that, in the long term, different interventions could counteract functional decline, while walking alone proved to have little effect in reducing decline [30]. This strengthened the idea that the motor skills developed through exercise, especially balance and lower limb strength, tend to protect against falls.
In some studies, the intervention’s effectiveness could only be seen in the long term [31, 32]. It can thus be highlighted that the long-term protective effect that exercise can have on physical activity passes through the period before and after the intervention [24, 30, 33, 34]. HWANG and collaborators (2016) compared tai chi chuan with lower limb training, for 6 months, among older adults aged 60 years and over. Their results demonstrate that tai chi chuan was more effective in preventing falls, and this effect lasted after 12 months of follow-up [33]. By contrast, Taylor and collaborators (2012) investigated elderly individuals for 17 months, and neither tai chi chuan nor light-intensity training yielded improvements in fall rates after a specific time. In both studies, the samples had already registered last drops, obscuring the real reasons for adherence and the benefits of exercise[29]. Fall-related mortality trends in the elderly indicate that rates are higher in men [35]. Nonetheless, women have often been investigated [19, 36, 37]. Suzuki [2004] conducted a randomised trial with elderly Japanese women where the intervention consisted of exercises to improve balance, walking ability and leg strength. The control group received a pamphlet with guidelines on fall prevention. After 8 months, 40.9% of the women in the control group has suffered falls, against 13.6% in the intervention group. After 20 months, the percentage of falls in the intervention group continued unchanged, but increased to 54.5% in the control group, showing a statistically significant difference between the two groups [38]. Note that the older women who took part in the interventions also fell, but less frequently.
Even though the research findings reported here demonstrate that most studies have found a significant effect of physical exercise on falls, there is no uniformity among the findings, because of unevenness in sample sizes, nationalities and interventions [duration of sessions, types of activity, and intervention timespan] [16, 39]. In a randomised study of elderly Australians, Oliveira (2019) assigned only a fall prevention leaflet to the control group. The intervention group received the same leaflet, plus a visit from a physical therapist, a pedometer and biweekly health training by telephone. However, even those individuals who practiced physical activity were not protected against falls [40]. It is also essential to categorise falls by type and severity, because among the elderly these accidents are related to risk of death [41]. Li (2019) investigated 1147 elderly Americans and compared three groups by intervention type (tai ji quan for balance and mobility, multimodal exercises, and stretching). Those who combined exercises for mobility and balance proved better protected from harmful falls (those that are more serious and require hospitalisation) [42].
To summarise, the findings of this systematic review suggest that physical exercise can be essential in preventing falls. When combined with proper medical care and environmental interventions, the protective effect tends to be greater [43]. However, the differences among interventions [ranging from the type of exercise to the duration of the interventions] reflect differing objectives, some aiming to improve strength, others balance, and some to improve both. Therefore, the comparison between them may need to be given coherently, biasing the conclusions, which in most cases suggest that exercises have beneficial effect in the long term [16] The meta-analysis strategy above was used to interpret the findings more cohesively. The imputations are discussed below. The direct protective effect of physical activity on the frequency of falls in the elderly could not be observed in this study. Collecting articles focused only on bodily practices that excluded environmental interventions may contribute to this result. One of the main reasons is that no single protocol is used in applying the interventions, so that they differed in modality, intensity, duration, materials used, and length of each session. However, some presented meta-analysis results that differ from those found here. Lee & Kim (2017), from a meta-analysis of 21 publications, indicated that balance and strength training may be able to decrease fall rates. However, they included randomised or quasi-randomised trials and only studies of elderly residents in institutions [17]. The literature has indicated that some physical exercises can improve muscle strength and increase resistance and balance, thus increasing protection against falls [21].
The study reported here found protective effect in studies that followed their participants for a long time after the intervention. These results align with the meta-analysis proposed by [44], which analysed randomised controlled trials, cohort studies and secondary data analyses with long-term (> 12 months) follow-up, and exercise-based interventions in an elderly population [65 years and over]. They indicated that physical exercise affected the number of falls for up to 2 years after exercise-based interventions [44]. A range of scientific evidence has indicated that physical exercise protects better against falls when other elements are added to the intervention, such as vitamin supplements, environmental modifications, eye treatment, and others [18, 45]. The meta-analysis by Tricco et al. [2017] used studies assessing the effectiveness of interventions in preventing falls in the elderly. They observed that interventions using physical exercise alone or physical exercise combined with two or more other interventions were associated with a lower risk of falling [19].
The individual's state of health is decisive in fall episodes. Meta-analysis by Sherrington et al. [2017] of 88 studies totalling 19,478 participants observed a more significant fall reduction effect in balanced physical exercise programmes. However, they did include studies of older adults with neurodegenerative diseases [18]. On the other hand, that analysis excluded studies with a significant sample of older people with neurodegenerative diseases, because they influence falls directly. Although too few studies were examined to identify the protective effect of physical exercise on falls, the meta-analysis reported here suggests a long-term protective effect by physical exercise against falls in the elderly. This can be explained by the fact that study quality was higher among those that analysed the post-intervention effect on falls. Remember also that the meta-regression showed that study quality was found to influence the effect of physical exercise on falls. This article has some limitations: first, the high statistical heterogeneity across studies calls for caution when data are analysed and interpreted. Also, in this regard, physical exercise programme content and duration were diverse and differed significantly between studies. Second, few studies examined follow-up, which may have interfered with the results. However, this study provides important and innovative information about the long-term protective effect of exercise on falls in the elderly. In short, this article investigated the protective effect of physical exercise on falls. The meta-analysis results suggest that physical exercise in short interventions without follow-up was insufficient to protect against falls. However, interventions using physical exercise had a protective effect on falls in the elderly when researchers followed-up on their samples after long periods without performing other interventions.
In conclusion, this meta-analysis contributes insights into the protective effect of physical exercise on falls in the elderly. Future research should focus on refining exercise protocols, exploring the impact on specific populations, and addressing the limitations identified in this study. About clinical practice, healthcare providers should consider implementing long-term exercise interventions and individualized monitoring to reduce fall risk effectively among elderlies.
Data availability
With this, we affirm that all data is available for verification if requested.
References
King EM, Randolph HL, Floro MS, Suh J (2021) Demographic, health, and economic transitions and the future care burden. World Dev 1:140
Kontis V, Bennett JE, Mathers CD, Li G, Foreman K, Ezzati M (2017) Future life expectancy in 35 industrialised countries: projections with a Bayesian model ensemble. The Lancet 389(10076):1323–1335
Carstensen LL, Fried LP (2012) The meaning of old age. Global population ageing: Peril or promise?. Geneva, Switzerland: World Economic Forum, p 15–17
World health organization et al. OMS-envelhecimento-2015-port. Resumo Relatório Mundial de Envelhecimento e Saúde Brasília: WHO. 2015;
Travassos GF, Coelho AB, Arends-Kuenning MP (2020) The elderly in Brazil: Demographic transition, profile, and socioeconomic condition. Rev Bras Estud Popul 37:1–27
Hunter SK, Pereira HM, Keenan KG, Hunter SK (2016) HIGHLIGHTED TOPIC Aging and Exercise The aging neuromuscular system and motor performance. J Appl Physiol [Internet] 121:982–995
Wu R, Ditroilo M, Delahunt E, De Vito G (2021) Age Related Changes in Motor Function [II]Decline in Motor Performance Outcomes. Int J Sports Med 42:215–226
Weyh C, Krüger K, Strasser B (2020) Physical activity and diet shape the immune system during aging. Nutrients 12:622
World Health Organization. Falls [Internet]. https://www.who.int/news-room/fact-sheets/detail/falls. 2021 [cited 2022 Sep 29]. Available from: https://www.who.int/news-room/fact-sheets/detail/falls
James SL, Lucchesi LR, Bisignano C, Castle CD, Dingels ZV, Fox JT et al (2019) The global burden of falls: Global, regional and national estimates of morbidity and mortality from the Global Burden of Disease Study 2017. Inj Prev 26:i3
Zhang K, Qi J, Zuo P, Yin P, Liu Y, Liu J et al (2022) The mortality trends of falls among the elderly adults in the mainland of China, 2013–2020: A population-based study through the National Disease Surveillance Points system. Lancet Reg Health-West Pac 19:1
Pimentel WRT, Pagotto V, Stopa SR, Hoffmann MCCL, Malta DC, de Menezes RL (2018) Falls requiring use of health services by the older adults: An analysis of the Brazilian national health survey 2013. Cad Saude Publica 34(8):1
Peng K, Tian M, Andersen M, Zhang J, Liu Y, Wang Q et al (2019) Incidence, risk factors and economic burden of fall-related injuries in older Chinese people: A systematic review. Inj Prev 25:4–12
Sherrington C, Fairhall N, Kwok W, Wallbank G, Tiedemann A, Michaleff ZA et al (2020) Evidence on physical activity and falls prevention for people aged 65+ years: systematic review to inform the WHO guidelines on physical activity and sedentary behaviour. Int J Behav Nutr Phys Act. https://doi.org/10.1186/s12966-020-01041-3
Winser SJ, Chan HTF, Ho L, Chung LS, Ching LT, Felix TKL et al (2020) Dosage for cost-effective exercise-based falls prevention programs for older people: A systematic review of economic evaluations. Ann Phys Rehabil Med 63:69–80
Karinkanta S, Kannus P, Uusi-Rasi K, Heinonen A, Sievänen H (2015) Combined resistance and balance-jumping exercise reduces older women’s injurious falls and fractures: 5-year follow-up study. Age Ageing 44(5):784–789
Lee SH, Kim SH (2017) Evidence Review Exercise Interventions for Preventing Falls Among Older People in Care Facilities: A Meta-Analysis. Worldviews Ev Based Nurs 14:74
Sherrington C, Michaleff ZA, Fairhall N, Paul SS, Tiedemann A, Whitney J et al (2017) Exercise to prevent falls in older adults: An updated systematic review and meta-analysis. Br J Sports Med 51:1749–1757
Tricco AC, Thomas SM, Veroniki AA, Hamid JS, Cogo E, Strifler L et al (2017) Comparisons of interventions for preventing falls in older adults: A systematic review and meta-analysis. JAMA-J Am Med Assoc 318(17):1687–1699
Mcardle WD, Katch FI, Katch VL (2010) Exercise physiology: nutrition, energy, and human performance. Lippincott Williams & Wilkins, p 68–250
Fragala MS, Cadore EL, Dorgo S, Izquierdo M, Kraemer WJ, Peterson MD et al (2019) Resistance Training for Older Adults: Position Statement From the National Strength and Conditioning Association. J Strength Cond Res 33:2019
Shiwa SR, Costa LOP, Moser ADL, Aguiar IC, Oliveira LVF (2011) PEDro: a base de dados de evidências em fisioterapia. Fisioterapia em Movimento 24:523–533
Freiberger E, Menz HB, Abu-Omar K, Rütten A (2007) Preventing falls in physically active community-dwelling older people: A comparison of two intervention techniques. Gerontology 53(5):298–305
Gawler S, Skelton DA, Dinan-Young S, Masud T, Morris RW, Griffin M et al (2016) Reducing falls among older people in general practice: The ProAct65+ exercise intervention trial. Arch Gerontol Geriatr 1(67):46–54
Iliffe S, Griffin M, Haworth D, Dinan-Young S, Morris R, Kendrick D et al (2015) Promoting physical activity in older people in general practice: ProAct65+ cluster randomised controlled trial. Br J Gen Pract 65(640):e731–e738
Liu-Ambrose T, Donaldson MG, Ahamed Y, Graf P, Cook WL, Close J et al (2008) Otago home-based strength and balance retraining improves executive functioning in older fallers: A randomized controlled trial. J Am Geriatr Soc 56(10):1821–1830
Rosendahl E, Gustafson Y, Nordin E, Lundin-Olsson L, Nyberg L (2008) A randomized controlled trial of fall prevention by a high-intensity functional exercise program for older people living in residential care facilities Aging Clinical and Experimental Research. Aging Clin Exp Res 20(1):67–75
Shigematsu R, Okura T, Sakai T, Rantanen T (2008) Square-stepping exercise versus strength and balance training for fall risk factors Aging Clinical and Experimental Research. Aging Clin Exp Res 20:19
Taylor D, Hale L, Schluter P, Waters DL, Binns EE, McCracken H et al (2012) Effectiveness of tai chi as a community-based falls prevention intervention: A randomized controlled trial. J Am Geriatr Soc 60(5):841–848
Eggenberger P, Theill N, Holenstein S, Schumacher V, de Bruin ED (2015) Multicomponent physical exercise with simultaneous cognitive training to enhance dual-task walking of older adults: A secondary analysis of a 6-month randomized controlled trial with I-year follow-up. Clin Interv Aging 28(10):1711–1732
Arrieta H, Rezola-Pardo C, Gil SM, Virgala J, Iturburu M, Antón I et al (2019) Effects of Multicomponent Exercise on Frailty in Long-Term Nursing Homes: A Randomized Controlled Trial. J Am Geriatr Soc 67(6):1145–1151
Uusi-Rasi K, Patil R, Karinkanta S, Kannus P, Tokola K, Lamberg-Allardt C et al (2017) A 2-Year Follow-Up After a 2-Year RCT with Vitamin D and Exercise: Effects on Falls, Injurious Falls and Physical Functioning Among Older Women. J Gerontol-Series A Biol Sci Med Sci 72(9):1239–1245
Hwang HF, Chen SJ, Lee-Hsieh J, Chien DK, Chen CY, Lin MR (2016) Effects of Home-Based Tai Chi and Lower Extremity Training and Self-Practice on Falls and Functional Outcomes in Older Fallers from the Emergency Department - A Randomized Controlled Trial. J Am Geriatr Soc 64(3):518–525
Kim H, Yoshida H, Suzuki T (2014) Falls and fractures in participants and excluded non-participants of a fall prevention exercise program for elderly women with a history of falls: 1-year follow-up study. Geriatr Gerontol Int 14(2):285–292
Hagiya H, Koyama T, Zamami Y, Tatebe Y, Funahashi T, Shinomiya K et al (2019) Fall-related mortality trends in older Japanese adults aged ≥65 years: A nationwide observational study. BMJ Open 9(12):e033462
Grahn Kronhed AC, Hallberg I, Ödkvist L, Möller M (2009) Effect of training on health-related quality of life, pain and falls in osteoporotic women. Adv Physiother 11(3):154–165
Kamide N, Shiba Y, Shibata H (2009) Effects on balance, falls, and bone mineral density of a home-based exercise program without home visits in community-dwelling elderly women: A randomized controlled trial. J Physiol Anthropol 28(3):115–122
Suzuki T, Kim H, Yoshida H, Ishizaki T (2004) Randomized controlled trial of exercise intervention for the prevention of falls in community-dwelling elderly Japanese women. J Bone Miner Metab 22(6):602–611
Li F, Harmer P, Eckstrom E, Fitzgerald K, Chou LS, Liu Y (2019) Effectiveness of Tai Ji Quan vs Multimodal and Stretching Exercise Interventions for Reducing Injurious Falls in Older Adults at High Risk of Falling: Follow-up Analysis of a Randomized Clinical Trial. JAMA Netw Open 2(2):e188280
Oliveira JS, Sherrington C, Paul SS, Ramsay E, Chamberlain K, Kirkham C et al (2019) A combined physical activity and fall prevention intervention improved mobility-related goal attainment but not physical activity in older adults: a randomised trial. J Physiother 65(1):16–22
Alamgir H, Muazzam S, Nasrullah M (2012) Unintentional falls mortality among elderly in the United States: Time for action. Injury 43(12):2065–2071
Li F, Harmer P, Chou LS (2019) Dual-task walking capacity mediates tai Ji quan impact on physical and cognitive function. Med Sci Sports Exerc 51(11):2318–2324
Fitzharris MP, Day L, Lord SR, Gordon I, Fildes B (2010) The Whitehorse NoFalls trial: Effects on fall rates and injurious fall rates. Age Ageing 39(6):728–733
Finnegan S, Seers K, Bruce J (2019) Long-term follow-up of exercise interventions aimed at preventing falls in older people living in the community: a systematic review and meta-analysis. Physiotherapy 105:187–199
El-Khoury F, Cassou B, Latouche A, Aegerter P, Charles MA, Dargent-Molina P (2015) Effectiveness of two year balance training programme on prevention of fall induced injuries in at risk women aged 75–85 living in community: Ossébo randomised controlled trial. BMJ [Online] 22:351
Acknowledgements
We offer our deepest thanks to the institutions that provided technical support for the development and implementation of this study.
Funding
None.
Author information
Authors and Affiliations
Contributions
The idea for the article came up: JAF and AJO. Performed the bibliographical research: JAF, MCG and AJO. Data analysis: JAF, MCG and AJO. Wrote and/or critically revised the work: JAF, MCG and AJO.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Ethical Approval
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
de Figueiredo, J.A., Garcia, M.C. & de Oliveira, A.J. Effect of physical exercise on fall episodes in the elderly: a meta-analysis. Sport Sci Health 20, 309–319 (2024). https://doi.org/10.1007/s11332-023-01145-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11332-023-01145-w