
Abstract
Hamstring-to-quadriceps (H:Q) strength ratio has been used to estimate injury risk and readiness to return to sport. Previous studies have investigated if H:Q ratios are determined by the weakness of knee flexors (KF) or strength of knee extensors (KE) in soccer players. However, the results on H:Q ratio determinants are divergent. Moreover, studies with this proposal involving futsal athletes were not found. The present study aimed to verify: (a) the global correlation between KF (KFPT) and KE peak torque (KEPT) with conventional and functional H:Q ratios, (b) the correlation according to balanced and unbalanced H:Q ratio conditions and (c) the KFPT and KEPT between balanced and unbalanced legs. Male professional futsal players (46 athletes, 24.65 ± 6.78 years) participated in this study. Using a global analysis (balanced + unbalanced legs), H:Q ratios were significantly related to concentric KFPT (r = 0.36–0.46), eccentric KFPT (r = 0.37–0.63) and concentric KEPT (r = − 0.31 to − 0.30). Balanced legs had a significant negative relationship between KEPT and H:Q ratios (r = − 0.51 to − 0.35). In contrast, unbalanced legs presented significant positive associations between H:Q ratios with concentric KFPT (r = 0.39–0.41) and eccentric KFPT (r = 0.52–0.65) but not KEPT. Finally, unbalanced legs showed lower KFPT and higher KEPT than balanced legs. In the global analysis, KFPT and KEPT were correlated with H:Q ratios. However, using specific analyses, KEPT was negatively related to H:Q ratios in balanced legs but not unbalanced legs. In unbalanced legs, concentric KFPT and eccentric KFPT presented significant positive associations with H:Q ratios.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Futsal involves repeated executions of high-intensity and high-speed tasks such as sprints, changes of direction, accelerations, decelerations and kicks [1, 2]. This demand may increase the athletes' injury incidence in the lower limb, such as anterior cruciate ligament rupture and hamstring strain injury [3,4,5]. In a study involving 161 professional Spanish futsal players from 11 teams, López-Segovia et al. [6] observed that athletes are substantially harmed by lower-limb injuries (92%) during the preseason period. Additionally, the authors verified that thigh and knee joint injuries (37% of all lower-limb injuries) resulted in 403 days of missing players from matches and training [6]. Maximal strength and appropriate knee flexion–extension strength balance (i.e., hamstring-to-quadriceps relative strength ratio, H:Q are commonly suggested to protect athletes against anterior cruciate ligament rupture and hamstring strain injury [7,8,9]. According to the Croisier et al. [8] study, the hamstrings strain injury rate was 4.66 times higher in professional soccer players with untreated strength unbalances in the preseason. In this sense, maximal strength of knee flexors (KF), knee extensors (KE) and H:Q ratio assessments have been included in the preseason routine of professional futsal teams [10].
Previous studies have investigated if H:Q ratios are determined by the weakness of KF or excessively strong KE in professional soccer players [11,12,13,14]. In this sense, concentric and eccentric KF peak torque (KFPT) and KE peak torque (KEPT) showed opposite correlations with H:Q ratios. A positive correlation between concentric KFPT with conventional H:Q ratio (concentric KFPT/concentric KEPT, H:QConv) (r = 0.45) was demonstrated [13]. Similarly, a positive relationship between eccentric KFPT with functional H:Q ratio (eccentric KFPT/concentric KEPT, H:QFunc) (r = 0.66) was verified [13]. In contrast, negative relationships between concentric KEPT and H:QFunc (r = − 0.67 to − 0.30) were noted [11, 13]. Moreover, two studies reported that soccer athletes with unbalanced H:QConv (H:QConv < 0.60) had weakened KF and stronger KE than balanced players [13, 14]. Contrariwise, another study found that soccer athletes with an unbalanced H:QConv had lower KFPT but similar KEPT compared to the balanced H:QConv group [12]. Regarding H:QFunc, the unbalanced condition (H:QFunc < 0.80) was verified in weakened eccentric KFPT soccer athletes [12, 13]. However, conflicting results demonstrated that an unbalanced H:QFunc leg may have lower or similar KEPT compared to a balanced H:QFunc leg [12, 13].
As mentioned above, there is divergence about the determinants of the H:Q ratios in professional soccer players. Importantly, studies investigating the relationship between KFPT and KEPT with H:Q ratios in professional futsal athletes were not found. Previous results showed that professional futsal players have lower H:Q ratio values than professional soccer athletes [15,16,17,18,19]. Thus, maximal strength and H:Q relationship findings in soccer players might not be directly applied to futsal athletes. Identifying the influence of KF and KE strength on the knee joint balance can contribute to informing interventions to increase athletic performance and help mitigate injuries in the futsal modality. Moreover, since balanced and unbalanced groups may have different muscle strength levels, it is possible that the impact of maximal strength on the H:Q ratio is distinct within each group, but this was not previously verified.
Thus, the present study aimed to verify: (a) the global correlation between KFPT and KEPT with H:QConv and H:QFunc, (b) the correlation according to balanced and unbalanced H:Q ratio conditions and (c) the KFPT and KEPT between balanced and unbalanced legs in futsal athletes. Our general hypothesis was that concentric KEPT would show a negative relationship with the H:Q ratios, while concentric and eccentric KFPT would demonstrate positive associations. This hypothesis was based on the results of previous studies [11, 13].
Methods
Study design
The present study had a cross-sectional design to verify the relationship between KF and KE maximal strength with H:Q ratios in professional futsal players. Initially, a researcher contacted the technical staff involved with the athletes to explain the study aims. Assessments were performed in week 1 of the preseason, after the official presentation of the athletes. Participants did not perform physical training sessions 24 h before the tests. Moreover, physical tests were not conducted before the isokinetic test. Assessments took place in just 1 day. The sample size was determined by convenience as the present study is part of an umbrella project where evaluations of the neuromuscular performance of futsal players occur.
Participants
Forty-six male professional futsal players (24.65 ± 6.78 years; 175.30 ± 7.02 cm; 73.97 ± 8.63 kg; 24.05 ± 2.25 kg/m2) from three different teams participated in this study. Participants were athletes from two professional seniors (n = 31) and one professional under-20 team (n = 15) from the Brazilian National Futsal League, who were free of musculoskeletal injuries requiring absence from training or matches for at least 6 months before the study. Participants played in the national and regional championships and represented the main category of their clubs. Additionally, the current evaluated teams use isokinetic evaluations in the preseason routine. Ninety-two legs were tested, with no adverse event identified during data collection. Participants were informed of the objectives, risks and benefits of the study before signing an informed consent form. The local Institutional Ethics Committee approved all procedures performed (Approval No. 2.903.811), conducted following the Declaration of Helsinki.
Peak torque and H:Q ratios
Peak torque was evaluated using an isokinetic dynamometer (Cybex Norm; Ronkonkoma, NY, USA). First, a five-minute warm-up was performed at a self-reported low-to-moderate effort on a cycle ergometer (Movement Technology, BM2700, São Paulo, Brazil). Then, athletes were seated in the equipment with the trunk flexed at 85° and the knee joint (lateral epicondyle of the femur) aligned with the rotation axis of the dynamometer. In addition, the leg, thigh, torso, and pelvis were secured by straps to avoid compensatory movements [17, 20, 21]. Participants were instructed to perform all contractions with maximal effort (i.e., “as fast as hard as possible”) [22]. Verbal encouragement was given, while visual feedback was provided in real-time on a screen placed in front of the participants. The right and left legs were evaluated.
Initially, a specific warm-up consisting of ten submaximal isokinetic contractions at 120°/s was conducted. Concentric KEPT and concentric KFPT were evaluated during five consecutive contractions using the concentric-concentric mode at 60°/s (range of motion: 0°–90°, 0° = full extension). Similarly, eccentric KFPT was assessed during five consecutive contractions performed at 60°/s [17, 20, 21]. Before each maximal test, three submaximal repetitions were performed as a pre-test to clear any further questions regarding the maximal tests. The pre-test and the maximal test were separated by a rest period of 30 s. After the maximal tests, there was an interval period of 60 s.
The equipment automatically informed the peak torque observed in each contraction (total of 5) of the maximal tests. The highest peak torque value observed in each maximal test was used for the analyses. Thus, H:QConv and H:QFunc were calculated using the contraction with the highest peak torque. Cut points based on prior studies with professional soccer players were used. Cut points of 0.60 for H:QConv and 0.80 for H:QFunc were adopted [9, 12, 13, 23]. Thus, legs with KFPT lower than 60% or 80% compared to KEPT were considered unbalanced for H:QConv or H:QFunc, respectively. Legs with KFPT values above 60% or 80% compared to KEPT were considered balanced for H:QConv and H:QFunc, respectively [9, 12, 13, 23]. The global analysis involved unbalanced and balanced legs. The specific analyses involved only legs below the cut point (unbalanced legs) or above the cut point (balanced legs).
Statistical analysis
Data distribution was assessed using the Shapiro–Wilk test, and descriptive values are shown as mean ± SD and 95% confidence interval for effect size. Independent T or Mann–Whitney tests were used to compare the right and left leg parameters, with no statistical difference observed. Thus, the right and left legs' data were pooled in the analyses. Independent T or Mann–Whitney tests were also used to compare unbalanced and balanced legs. The correlations were verified with Pearson (r) and Spearman (rs) tests, according to the distribution of the outcomes. For correlation value classification, trivial (r = ≤ 0.1), small (r = 0.1 < r ≤ 0.3), moderate (r = 0.3 < r ≤ 0.5), large (r = 0.5 < r ≤ 0.7), very large (r = 0.7 < r ≤ 0.9), nearly perfect (r = > 0.9) and perfect (r = 1) were adopted [24]. Effect sizes [Δ (unbalanced leg—balanced leg//mean pooled SD)] were calculated using Cohens'd, assuming the results as a trivial (d < 0.2), small (d < 0.5), moderate (d < 0.8) or large (d > 0.8) [24]. The level of significance (α) was set at < 0.05. All statistical procedures were performed using the Statistical Package for Social Science (SPSS) version 23.0 (IBM SPSS Inc., Chicago, IL, USA).
Results
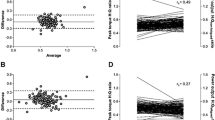
Concentric KEPT, concentric KFPT and eccentric KFPT of 220.07 ± 39.38 Nm, 129.15 ± 24.68 Nm and 159.75 ± 35.90 Nm, respectively, were observed using global analysis (unbalanced + balanced legs, n = 92). H:QConv and H:QFunc of 0.59 ± 0.10 and 0.73 ± 0.15 were verified. Parameters based on H:QConv and H:QFunc cut points are presented in Table 1. Table 2 shows the results of the correlation analyses. Considering the global analysis, concentric KEPT, concentric KFPT and eccentric KFPT were (weak to strong) correlated with H:QConv and H:QFunc (Figs. 1, 2, 3). Moreover, H:QConv and H:QFunc were positively related (r = 0.73, p < 0.01).

Global (i.e., balanced + unbalanced, n = 92) relationships between conventional (concentric:concentric) and functional (eccentric:concentric) hamstring-to-quadriceps (H:Q) ratios with concentric knee extension peak torque. Triangles represent unbalanced legs and circle balanced legs

Global (i.e., balanced + unbalanced, n = 92) relationships between conventional (concentric-concentric) and functional (eccentric-concentric) hamstring-to-quadriceps (H:Q) ratios with concentric knee flexion peak torque. Triangles represent unbalanced legs and circle balanced legs

Global (i.e., balanced + unbalanced, n = 92) relationships between conventional (concentric:concentric) and functional (eccentric:concentric) hamstring-to-quadriceps (H:Q) ratios with eccentric knee flexion peak torque. Triangles represent unbalanced legs and circle balanced legs
Unbalanced versus balanced legs
Significant differences in peak torque and H:Q ratio between unbalanced and balanced legs were observed. Considering the H:QConv cut point (0.60), unbalanced legs had superior concentric KEPT (+ 9.07%, effect size: 0.54) than balanced legs. Contrary, balanced legs showed superior concentric KFPT (+ 14.52%, effect size: 0.91) and eccentric KFPT (+ 12.52%, effect size: 0.63). Considering the H:QFunc cut point (0.80), KEPT showed no significant differences between balanced and unbalanced legs (Table 1). Contrariwise, balanced legs demonstrated higher concentric KFPT (+ 11.12%, effect size: 0.66) and eccentric KFPT (+ 21.10%, effect size: 1.22) compared to unbalanced legs (Table 1).
Correlation analyses
Global analysis (unbalanced + balanced legs) showed that KEPT and KFPT had a significant (moderate to large) correlation with H:QConv and H:QFunc (Table 2). Considering the H:QConv cut point (0.60), KEPT was negatively related (moderate to large) to H:QConv and H:QFunc in balanced but not in unbalanced legs (Table 2). In contrast, KFPT was positively related (moderate to large) to both H:QConv and H:QFunc only in unbalanced legs (Table 2). Analyses based on H:QFunc cut point (0.80) showed a significant negative moderate relationship between concentric KEPT and H:QFunc in balanced but not in unbalanced legs (Table 2). Eccentric KFPT significantly correlated with H:QFunc in unbalanced but not balanced legs (Table 2).
Discussion
The main findings of the present study were that: (a) using a global analysis (balanced + unbalanced legs), KFPT and KEPT were significantly correlated with H:Q ratios, (b) balanced legs had a negative relationship between KEPT and H:Q ratios, while (c) unbalanced legs presented positive associations between H:Q ratios with KFPT but not KEPT, and (d) unbalanced legs showed lower KFPT and higher KEPT than balanced legs.
Balanced H:Q ratio is suggested to protect athletes against lower-limb injuries such as anterior cruciate ligament rupture and hamstring strain injury [7,8,9]. Thus, previous studies investigated H:Q ratio determinants [11,12,13,14]. Fritsch et al. [13] demonstrated a negative relationship between concentric KEPT with H:QConv (r = − 0.37) and H:QFunc (r = − 0.30) in professional soccer players. In contrast, concentric KFPT presented a positive association with H:QConv (r = 0.45) [13]. Also, a significant positive relationship between eccentric KFPT and H:QFunc (r = 0.66) was verified [13]. In another study, Bogdanis and Kalapotharakos [11] observed a negative association between concentric KEPT and H:QConv (r = − 0.67). However, there was no significant correlation between H:QConv and concentric KFPT. In the present study, global analysis findings demonstrated a significant relationship between KFPT and KEPT with H:Q ratios (Table 2). Notably, the studies by Fritsch et al. [13] and Bogdanis and Kalapotharakos [11] verified KF and KE strength correlations involving pooled unbalanced and balanced legs. In the current study, KEPT demonstrated a negative association with H:QConv and H:QFunc in analysis involving balanced but not unbalanced legs (Table 2). In contrast, unbalanced legs showed positive relationships between H:Q ratios with concentric KFPT and eccentric KFPT (Table 2). These results revealed that the associations between KFPT and KEPT with H:Q ratio change according to balanced or unbalanced leg condition.
Another interesting way of investigating the determinants of the H:Q ratio is the possible strength differences between balanced and unbalanced legs. In the present study, unbalanced (0.60) H:QConv legs had superior KEPT but lower concentric KFPT than balanced legs (Table 1). Considering the H:QFunc cut point (0.80), unbalanced legs showed lower eccentric KFPT than balanced legs. KEPT was not statistically different between H:QFunc unbalanced and balanced legs. Previous studies verified that unbalanced legs present a weakened concentric and eccentric KFPT but superior [13, 14] or similar concentric KEPT [12] compared to balanced counterparts. Contrariwise, Bogdanis and Kalapotharakos [11] found that unbalanced legs had stronger KE but similar KF strength compared to balanced legs. Corroborating most studies with a similar proposal, the present results reinforce that KF weakness can be the main determinant of unbalanced H:Q ratios in team sports, such as soccer and futsal.
The values of KEPT observed in the present study (220.07 ± 39.38 Nm) are similar to those reported by previous studies investigating futsal players. KEPT values of 207.81 ± 36.63 Nm [17], 223.9 ± 33.4 Nm [16] and 214.7 ± 49.6 Nm [18] were demonstrated. Similarly, the current values of concentric KFPT (129.15 ± 24.68 Nm) agree with the findings by Machado et al. [17] (122.75 ± 22.90 Nm), de Lira et al. [16] (128.6 ± 27.6 Nm) and Nunes et al. [18] (136.6 ± 31.7 Nm) studies. Moreover, a similar eccentric KFPT compared to the verified by Machado et al. [17] (159.75 ± 35.90 Nm vs. 157.19 ± 34.84 Nm) was observed. Regarding H:Q ratios, there were similarities between the present findings and the mean H:QConv values reported by previous studies (0.59 vs. 0.59, 0.58 and 0.64) [16,17,18]. Additionally, the current H:QFunc value was similar to that demonstrated by Machado et al. [17] (0.73 vs. 0.76). In summary, the current findings corroborated the prior results verified in the futsal modality. However, these futsal studies did not investigate the relationship between KF and KE strength and H:Q ratios. This analysis was previously demonstrated only in professional soccer athletes [11, 13], which may have different levels of KEPT, KFPT and H:Q ratios compared to professional futsal players [15, 16, 18, 19].
The current findings showed that the hamstrings muscle group had lower strength than the quadriceps muscle group (Table 1). This condition agreed with a few legs demonstrating balanced values of H:QConv (n = 38) and H:QFunc (n = 29). In the current study, approximately 59% and 69% of the legs showed unbalanced conditions of H:QConv and H:QFunc, respectively. A superior resistance training focus for the KE muscle group than KF may be the main reason for strength unbalances between KF and KE. Notably, KF performance seems to be the primary determinant of a balanced H:Q ratio, mainly among unbalanced legs (Table 2). In this way, the present results reinforce the need for resistance training focused on concentric and eccentric KF in futsal athletes.
As a practical application, unbalanced legs need training programs emphasizing concentric and eccentric KF strength. Exercise recommendations for increasing concentric and eccentric KF performance include Nordic hamstring exercise, prone leg curl, slide leg curl, upright hip extension, straight‐knee bridge and deadlifts [25,26,27]. On the other hand, it is important to note that balanced legs showed lower KEPT values, which may harm sports tasks such as jumping and sprinting [28, 29]. Thus, interventions for balanced legs involve increasing KE strength without impairing the H:Q ratio. Therefore, KF needs training programs that accompany the increase in KE capacity.
Some limitations of the present study must be considered. First, only three teams were investigated, limiting the current sample size. Still, it is noteworthy that the current players evaluated have relevance in the futsal modality (regional, national and continental titles). Second, the transversal design does not allow us to infer the predictive capacity of H:Q ratio measures. This analysis would contribute to unbalanced and balanced conditions' impact on injuries. Third, the results of the present study refer to a velocity of 60°/s used in the isokinetic evaluation and should not be extrapolated to other angular velocities. Moreover, analyses with different cut points were not performed due to the low number of legs in more subdivisions. Importantly, the present study used cut points previously adopted in professional soccer players [9, 12, 13, 23]. Finally, the impact of the athletes’ strength level on the relationships between KFPT and KEPT with the H:Q ratio was not verified. Two athletes may have H:Q ratios considered balanced but be in different strength level categories (e.g., low vs. high strength level). Despite the limitations above, the current findings broaden the view of verifying the performance of KF and KE and risk factors for injuries as H:Q ratios in the sports scenario.
Conclusions
In the present study, the global analysis demonstrated a relationship between KFPT and KEPT with H:Q ratios. On the other hand, the specific analyses presented some particularities of the relationship between KF and KE performance with H:Q ratios. A negative relationship between KEPT and H:Q ratios was observed in balanced legs but not in unbalanced legs. Moreover, unbalanced legs presented positive associations between concentric KFPT and eccentric KFPT with H:Q ratios. Finally, unbalanced legs demonstrated inferior KFPT and superior KEPT than balanced legs, which helps to explain the low H:Q values.
Abbreviations
- KF:
-
Knee flexion
- KE:
-
Knee extension
- KFPT :
-
Knee flexion peak torque
- KEPT :
-
Knee extension peak torque
- H:Q:
-
Hamstring-to-quadriceps ratio
- H:QConv :
-
Conventional hamstring-to-quadriceps ratio
- H:QFunc :
-
Functional hamstring-to-quadriceps ratio
References
Spyrou K, Freitas TT, Marín-Cascales E, Alcaraz PE (2020) Physical and physiological match-play demands and player characteristics in futsal: a systematic review. Front Psychol. https://doi.org/10.3389/fpsyg.2020.569897
Taylor JB, Wright AA, Dischiavi SL, Townsend MA, Marmon AR (2017) Activity demands during multi-directional team sports: a systematic review. Sports Med 47:2533–2551. https://doi.org/10.1007/s40279-017-0772-5
Della Villa F, Hägglund M, Della Villa S, Ekstrand J, Waldén M (2021) High rate of second ACL injury following ACL reconstruction in male professional footballers: an updated longitudinal analysis from 118 players in the UEFA elite club injury study. Br J Sports Med. https://doi.org/10.1136/bjsports-2020-103555
Gronwald T, Klein C, Hoenig T, Pietzonka M, Bloch H, Edouard P, Hollander K (2022) Hamstring injury patterns in professional male football (soccer): a systematic video analysis of 52 cases. Br J Sports Med 56:165–171. https://doi.org/10.1136/bjsports-2021-104769
Ruiz-Pérez I, López-Valenciano A, Elvira JL, García-Gómez A, de Ste Croix M, Ayala F (2020) Epidemiology of injuries in elite male and female futsal: a systematic review and meta-analysis. Sci Med Footb. https://doi.org/10.1080/24733938.2020.1789203
López-Segovia M, Vivo Fernández I, Herrero Carrasco R, Pareja Blanco F (2022) Preseason injury characteristics in spanish professional futsal players: the LNFS project. J Strength Cond Res 36:232–237. https://doi.org/10.1519/JSC.0000000000003419
Coombs R, Garbutt G (2002) Developments in the use of the hamstring/quadriceps ratio for the assessment of muscle balance. J Sports Sci Med 1:56–62
Croisier JL, Ganteaume S, Binet J, Genty M, Ferret JM (2008) Strength imbalances and prevention of hamstring injury in professional soccer players: a prospective study. Am J Sports Med 36:1469–1475. https://doi.org/10.1177/0363546508316764
Dauty M, Menu P, Fouasson-Chailloux A, Ferréol S, Dubois C (2016) Prediction of hamstring injury in professional soccer players by isokinetic measurements. Muscles Ligaments Tendons J 6:116–123. https://doi.org/10.11138/mltj/2016.6.1.116
Spyrou K, Freitas TT, Herrero Carrasco R, Marín-Cascales E, Alcaraz PE (2022) Load monitoring, strength training, and recovery in futsal: Practitioners’ perspectives. Sci Med Footb. https://doi.org/10.1080/24733938.2022.2144641
Bogdanis GC, Kalapotharakos VI (2015) Knee extension strength and hamstrings-to-quadriceps imbalances in elite soccer players. Int J Sports Med 37:119–124. https://doi.org/10.1055/s-0035-1559686
de Camarda SRA, Denadai BS (2012) Does muscle imbalance affect fatigue after soccer specific intermittent protocol? J Sci Med Sport 15:355–360. https://doi.org/10.1016/j.jsams.2011.11.257
Fritsch CG, Dornelles MP, dos Oliveira GS, Baroni BM (2020) Poor hamstrings-to-quadriceps torque ratios in male soccer players: Weak hamstrings, strong quadriceps, or both? Sports Biomech. https://doi.org/10.1080/14763141.2020.1766100
Greco CC, da Silva WL, Camarda SRA, Denadai BS (2012) Rapid hamstrings/quadriceps strength capacity in professional soccer players with different conventional isokinetic muscle strength ratios. J Sports Sci Med 11:418–422
Baroni BM, Ruas CV, Ribeiro-Alvares JB, Pinto RS (2020) Hamstring-to-quadriceps torque ratios of professional male soccer players: a systematic review. J Strength Cond Res 34:281–293. https://doi.org/10.1519/JSC.0000000000002609
de Lira CAB, Mascarin NC, Vargas VZ, Vancini RL, Andrade MS (2017) Isokinetic knee muscle strength profile in brazilian male soccer, futsal, and beach soccer players: a cross-sectional study. Int J Sports Phys Ther 12:1103–1110. https://doi.org/10.26603/ijspt20171103
Machado CLF, Nakamura FY, Brusco CM, Andrade MX, Carlet R, Voser RC, Pinto RS (2022) The relationship between lower-limb body composition with isokinetic performance in futsal players: Body composition and performance in futsal players. Braz J Motor Behav 16:304–314. https://doi.org/10.20338/bjmb.v16i3.285
Nunes RFH, Dellagrana RA, Nakamura FY, Buzzachera CF, Almeida FAM, Flores LJF, Guglielmo LGA, da Silva SG (2018) Isokinetic assessment of muscular strength and balance in Brazilian elite futsal players. Int J Sports Phys Ther 13:94–103. https://doi.org/10.26603/ijspt20180094
Vieira LHP, de Souza Serenza F, de Andrade VL, de Paula Oliveira L, Mariano FP, Santana JE, Santiago PRP (2016) Kicking performance and muscular strength parameters with dominant and nondominant lower limbs in Brazilian elite professional futsal players. J Appl Biomech 32:578–585. https://doi.org/10.1123/jab.2016-0125
Minozzo F, Lopez P, Machado CLF, Wilhelm EN, Grazioli R, Pinto RS (2018) Alternative assessment of knee joint muscle balance of soccer players through total work-based hamstring: quadriceps ratios. Eur J Sport Sci. https://doi.org/10.1080/17461391.2018.1495271
Veeck F, Lopez P, Grazioli R, Machado CLF, Wilhelm EN, Cadore EL, Pinto RS (2022) Dissociation between fatigued power output and traditional peak torque for isokinetic hamstring:quadriceps ratios in professional soccer players. Sport Sci Health 18:967–973. https://doi.org/10.1007/s11332-021-00881-1
Maffiuletti NA, Aagaard P, Blazevich AJ, Folland J, Tillin N, Duchateau J (2016) Rate of force development: physiological and methodological considerations. Eur J Appl Physiol 116:1091–1116. https://doi.org/10.1007/s00421-016-3346-6
Dauty M, Menu P, Fouasson-Chailloux A (2018) Cutoffs of isokinetic strength ratio and hamstring strain prediction in professional soccer players. Scand J Med Sci Sports 28:276–281. https://doi.org/10.1111/sms.12890
Cohen J (1998) Statistical power analysis for the behavioral sciences, 2nd edn. Lawrence Erlbaum Associates, Hillsdale
Bourne MN, Timmins RG, Opar DA, Pizzari T, Ruddy JD, Sims C, Williams MD, Shield AJ (2018) An evidence-based framework for strengthening exercises to prevent hamstring injury. Sports Med 48:251–267. https://doi.org/10.1007/s40279-017-0796-x
Hegyi A, Csala D, Péter A, Finni T, Cronin NJ (2019) High-density electromyography activity in various hamstring exercises. Scand J Med Sci Sports 29:34–43. https://doi.org/10.1111/sms.13303
van Dyk N, Behan FP, Whiteley R (2019) Including the Nordic hamstring exercise in injury prevention programmes halves the rate of hamstring injuries: a systematic review and meta-analysis of 8459 athletes. Br J Sports Med 53:1362–1370. https://doi.org/10.1136/bjsports-2018-100045
Aktuğ ZB, Harbili E, Harbili S (2016) Comparison of isokinetic knee strength between the dominant and non-dominant legs and relationships among isokinetic strength, vertical jump, and speed performance in soccer players. Turk Klinikleri J Sports Sci 8:8–14. https://doi.org/10.5336/sportsci.2015-47409
Newman MA, Tarpenning KM, Marino FE (2004) Relationships between isokinetic knee strength, single-sprint performance, and repeated-sprint ability in football players. J Strength Condit Res 18:867. https://doi.org/10.1519/13843.1
Author information
Authors and Affiliations
Contributions
C.L.F.M., R.P.F and R.S.P. contributed to the study conception and design. C.L.F.M. and R.P.F. performed data collection and analysis. The first draft of the manuscript was written by R.P.F. and C.L.F.M. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Conflict of interest
The authors report no conflict of interest.
Consent to participate
All participants provided written informed consent to participate in the study.
Ethics approval
The study was approved by the local Human Research Ethics Committee.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Fortes, R.P., Machado, C.L.F., Baroni, B.M. et al. Relationship between maximal strength and hamstring-to-quadriceps ratios in balanced and unbalanced legs in futsal athletes. Sport Sci Health 19, 1169–1176 (2023). https://doi.org/10.1007/s11332-023-01046-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11332-023-01046-y