
Abstract
Background
Sedentary lifestyle habits are directly related to the increase in the production of reactive oxygen species, to provide a chronic state of oxidative stress. Furthermore, the purinergic system is involved in extracellular signaling and thus influences pathological and physiological processes. Thus, physical exercise is responsible for triggering molecular and tissue changes, to condition the body’s pathophysiological processes, being often suggested as a form of non-pharmacological treatment in different health conditions.
Aim
To evaluate the effect of physical exercise on markers of oxidative stress and the purinergic system in young adults.
Method
Sixteen women students, aged between 20 and 40 years, were submitted to the physical exercise protocol, both aerobic and resistance (concurrent training) during the period of eight weeks, making a total of 20 h of training.
Results
Our findings showed that physical exercise was responsible for increasing the hydrolysis of adenosine diphosphate (ADP) (p = 0.001) and adenosine deaminase (ADA) (p = 0.041) in platelets, indicating an increase in ecto-nucleoside triphosphate diphosphohydrolase (ecto-NTPDase) after eight weeks of physical exercise. Furthermore, there was an increase in the concentration of thiobarbituric acid reactive substances (TBARS) (p = 0.012) and protein thiols (PSH) (p = 0.004) after one week of exercise. Furthermore, it can be considered that resistance exercise can stimulate the antioxidant defense mechanisms as well as promote an anti-inflammatory and anti-platelet aggregation state.
Conclusion
In conclusion, physical exercise alters both the mechanisms of oxidative stress and the purinergic system, to have the potential to attenuate inflammatory mechanisms.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Today’s life has provided the population with habits, such as being sedentary, consuming industrialized foods and constantly being exposed to stress. A sedentary life carries in its baggage the greater possibility of acquiring chronic diseases, including: hypertension, obesity, type 2 diabetes, heart disease, metabolic syndrome and a higher rate of early mortality [1]. Thus, the regular practice of physical exercise is associated with improvements in these chronic conditions acquired through sedentary lifestyle, thus helping to prevent and treat these comorbidities [2].
The practice of physical exercise enables biochemical and physiological changes that are beneficial to the human body. These activities can be subdivided into aerobic and anaerobic. Aerobic exercise is characterized by long-term and low-to-moderate intensity. Anaerobics, on the other hand, are characterized by activities of short duration and moderate to high intensity. During the practice of physical exercise, muscle contractions occur that alter the body’s functioning, namely changes in contractility and muscle tension, increased production of adenosine triphosphate (ATP), increased production of reactive oxygen species (ROS) and greater intracellular calcium influx. These changes activate cell signaling cascades to regulate systemic changes produced by exercise [3].
In addition to the aforementioned changes, regular physical exercise helps regulate the immune system, as it promotes an increase in anti-inflammatory cytokines [4]. Regular activity for 8 weeks improves the interleukin 10 (IL-10) and tumor necrosis factor alpha (TNF-α) ratio, to increase IL-10 levels and decrease TNF-α levels [5].
The purinergic system, like other biochemical systems, also undergoes changes resulting from exercise. During the muscle contraction process, ATP is released due to mechanical deformation of the muscles. Likewise, ATP is released as a cotransmitter together with norepinephrine from nerve endings of the sympathetic nervous system to the extracellular environment, which act through purinergic P2 receptors [6].
The ATP released into the extracellular environment during physical exercise can be gradually hydrolyzed to adenosine diphosphate (ADP) and adenosine monophosphate (AMP) through the action of ecto-nucleoside triphosphate diphosphohydrolase (ecto-NTPDases). The AMP formed can be converted by the action of ecto-5'nucleotidase into adenosine (ADO), which can be hydrolyzed by adenosine deaminase (ADA) and form inosine. All of these enzymes are found in the cell membrane of immune system cells. Thus, the action of ecto-NTPDases and ADA is essential for the reestablishment of the pro- and anti-inflammatory balance provided by the released cellular ATP. In lymphocytes, ATP is responsible for promoting the activation of a pro-inflammatory state, whereas ADO promotes an anti-inflammatory environment. In platelets, ADP is the pro-aggregating agent and ADO is the anti-aggregating agent [7].
ATP is a molecule responsible for providing energy for the most varied processes of cellular metabolism. Furthermore, ATP, present in all cells, is a signaling molecule of the purinergic system, which acts as a regulator of pathophysiological mechanisms in the extracellular environment [8]. The purinergic system is involved in several processes in the human body, namely endocrine and exocrine secretion, inflammatory process, pain mechanism, platelet aggregation, immune response and cell differentiation [9]. Thus, this study aimed to evaluate the effect of moderate-intensity physical exercise on markers of oxidative stress and the purinergic system in young adults.
Materials and methods
Study design and population
The study model used is non-randomized, of the before and after type, which allowed the comparison of data before and after an intervention was instituted. The sample included university students enrolled in courses in the area of health at the Federal University of Fronteira Sul (UFFS) Campus Chapecó/SC, Brazil. Including 16 participants for an α of 0.05 and β 0.20, with convenience sampling and ages between 20 and 40 years, from May 2018 to March 2020, who agreed to participate in the research by signing the Consent Form Free and Clear (TCLE) and that they met the eligibility criteria.
Inclusion and exclusion criteria
Inclusion criteria were at least twelve months enrolled in courses in the health area and age between 20 and 40 years (young adult). The study is part of a larger project that, among other objectives, aimed to analyze the psychological stress of university students enrolled in courses in the health area. So, a minimum time of twelve months was necessary for students enrolled in courses in the health area to adapt to the university routine, new schedules, new responsibilities, new social demands as a whole, that is, intrinsic requirements of the academic environment. In this way, it was possible to better analyze the psychological objectives involved in the project. Therefore, one of the inclusion criteria was a minimum time of twelve months enrolled in courses in the health area. As for the exclusion criteria, students who already practiced physical exercise on a regular basis were excluded from the research.
Interventions
The students were organized into a single group, having the physical exercise plan as an intervention. The control was the group itself. The intervention consisted of aerobic exercise (20 min walk) and anaerobic exercise (20 min), initial warm-up (5 min) and stretching (5 min), distributed over eight weeks (three times a week) of exercise practice physical exercise of 50 min each class, comprising 21 training sessions (totaling 20 h), the first three being for anamnesis and adaptation to the environment and to the motor gesture of the proposed exercises. The training program followed the recommendations of the American College of Sports Medicine, which calls for at least 150 min a week of moderate-intensity exercise. The exercises were chosen to encompass the main muscle groups, being performed alternately, three series for each exercise, from 12 to 15 repetitions in each series, with the intensity controlled by the Borg Scale. The program sequence consisted of the following exercises: 20 min walk in an open space, resistance exercise for lower limbs: knee extension, hip flexion, calf and squat, and, for upper limbs: biceps, triceps and chest. This physical exercise protocol was performed by a professional physiotherapist collaborating in this study. The activities were carried out in the form of a circuit. Thus, the protocol covered aerobic and resistance exercises, that is, concurrent training of moderate intensity.
Collection of blood samples
Samples of 10 ml of fasting blood were collected at eight o’clock in the morning through peripheral venipuncture, within the laboratory of Microbiology, Parasitology and Immunology at UFFS Campus Chapecó/SC, performed by researchers duly trained for this purpose. For analysis of the purinergic system and oxidative stress, four blood samples were collected: two tube collections containing EDTA (plasma and lymphocyte-PBMC); one tube collection with sodium citrate (platelets); and a collection in a tube containing serum (for further analysis).
Serum, plasma and whole blood separation protocol with citrate
The tube containing separating gel underwent a centrifugation process through a Sigma model 3-16L centrifuge at 3500 rpm for 15 min. Soon after, the serum obtained was separated into two vials: a quantity was placed in a test tube to perform the biochemical analyzes and the remainder of the serum obtained was stored in a cryotube in the Ultrafreezer Indrel IULT 335D-486 at −80 °C to carry out the analyzes of the oxidative profile.
From the content of one of the tubes containing EDTA, the sample was centrifuged at 3500 rpm for 15 min, and the supernatant content composing the plasma was stored in a cryotube in the ultrafreezer at −80 °C for further analysis. One of the tubes containing the sample and sodium citrate anticoagulant was homogenized by inversion and, from the whole blood of this flask, a volume of 500 µL was separated in a cryotube and stored under the conditions described above.
Lymphocyte separation protocol
For the separation of the lymphocyte layer, the methodology of Böyum [10] was applied. 4 mL of whole blood with EDTA was placed in a falcon tube, to which 4 mL of 0.9% saline solution (saline) was also added; the tube was closed and then lightly homogenized. In another tube, 3 mL of Ficoll® reagent was placed, and the sample diluted in saline solution was added slightly along the edges, then the tube was centrifuged at 1800 rpm for 30 min. After centrifugation, there was the formation of a gradient containing a layer of mononuclear cells ("cloud") between the reagent and plasma layers. This “cloud” of cells was transferred to an empty falcon tube, where 10 mL of saline solution was then added; the tube was capped and centrifuged at 1500 rpm for 15 min. After this procedure, the supernatant was discarded by inversion and, to the precipitate, 5 mL of saline was added and then centrifugation was carried out at 1200 rpm for 10 min. Again, the supernatant was discarded by inversion and 1 mL of saline was added to the precipitate, followed by centrifugation at 1000 rpm for 05 min. After the last centrifugation, the supernatant was discarded and 175 µL of saline was added, storing the sample in the ultrafreezer at −80 °C to carry out the analytical protocols.
Platelet separation protocol
For platelet separation, the methodology of Pilla et al. [11] modified by Lunkes et al. [12]. With the remainder of the sample containing whole blood in sodium citrate anticoagulant, the tubes were centrifuged at 1200 rpm for 10 min. After removal from the centrifuge, the supernatant was transferred into a test tube, which was centrifuged at 5000 rpm for 30 min. The centrifuge tubes were removed and the supernatant discarded; 2 ml of 3.5 mM HEPES buffer at pH 7.2 was added to the precipitate, homogenizing until complete dissolution. This homogenate was centrifuged for another 10 min at 5000 rpm. After the last centrifugation procedure, the supernatant was removed and 500 μl of HEPES buffer was added to the platelets, storing the sample in the ultrafreezer at −80 °C.
Oxidative profile evaluation
The oxidative profile of the individuals under study was evaluated by determining indicators of oxidative stress, being the substances reactive to thiobarbituric acid (TBARS) and myeloperoxidase (MPO). The spectrophotometric readings were taken in a Thermo Fischer Scientific MultiskanTM GO microplate spectrophotometer.
The methodology adopted for TBARS assessment followed the protocol by Jentzsch et al. [13], with reading at 532 nm. This technique aims to measure the formation of malondialdehyde (MDA), which comprises a substance generated by the reaction of ROS with membrane lipids, a phenomenon called lipoperoxidation (LPO). LPO causes changes in the membrane that range from permeability disorders to loss of selectivity and impairment of extracellular matrix components. MDA, when heated in the presence of TBA, gives rise to a pink colored compound, which was measured spectrophotometrically [13, 14]. Plasma samples were evaluated in quadruplicate; 50 µL of distilled water, 5 µL of 10 mM ditert-butyl methyl phenol (BHT), 295 µL of 1% orthophosphoric acid, 25 µL of 8.1% sodium lauryl sulfate (SDS) were sequentially pipetted into the tubes, 50 µl of the sample and 50 µl of TBA. The standard curve was performed with 0.03 mM MDA solution. After preparing the samples, they were placed in a water bath at 95ºC for 60 min and then the absorbance reading was carried out. The results were calculated by multiplying the mean absorbances with the correction factor, divided by the sample volume and expressed in nmol MDA/mL.
To determine protein (PSH) and non-protein (NPSH) thiols, the Ellman methodology [15] was used. The thiols react with 2,2'-dinitro-5,5′-dithiodibenzoic (DTNB) generating a yellow-colored compound, reading at 412 nm. These compounds are components of the non-enzymatic defense system. Plasma samples were analyzed in duplicate. For the determination of PSH, 30 µL of the sample, 260 µL of monobasic and dibasic potassium phosphate buffer solution (TKF) 10% and 15 µL of DTNB were pipetted. For NPSH dosage, the sample was deproteinized with 150 µL of 10% trichloroacetic acid (TCA) and centrifuged at 2000 rpm for 10 min and, from the supernatant, the analyzes were performed with 40 µL of the sample, 200 µL of TKF 10% and 20 µl DTNB. The cysteine correction factor (FC) was calculated, which was multiplied by the mean absorbance, divided by the sample volume, with the results expressed in µmol/mL of plasma.
The MPO analysis was performed using the method described by Suzuki et al. [16], with reading at 492 nm. MPO is a heme enzyme synthesized by inflammatory mediators and released from leukocytes (lymphocytes and neutrophils) at injured sites. MPO generates substantial amounts of hypochlorous acid (HOCl) from the catalysis reaction of chloride ions with hydrogen peroxide. HOCl consists of an ROS with high reactive capacity for the formation of singlet oxygen and hydroxyl radical. This analytical technique was performed in the presence of H2O2 as an oxidizing agent, and MPO catalyzed the oxidative coupling of phenol and aminoantipyrine (AAP), giving rise to a colored product, quinoneimine, with an absorbance read in a spectrophotometer. Plasma samples were analyzed in duplicate. 12 µL of the sample, 148 µL of 2.5 mM AAP and 170 µL of 1.7 mM H2O2 were pipetted, and the plates were incubated at 37 °C for 30 min, reading soon after incubation. The calculation was performed by multiplying the mean absorbance by the FC, and the results were expressed in mM of quinoneimine produced in 30 min.
Purinergic system evaluation
To evaluate the purinergic signaling system, samples of lymphocytes and platelets from the individuals under study were used. To measure the hydrolysis of ATP into ADP and AMP and evaluate the activity of ectoenzymes NTPDase and ecto-5'-nucleotidase, the amount of inorganic phosphate released was measured by colorimetric assay, with reading in a spectrophotometer at 630 nm, using the method de Pilla et al. [11] adapted by Lunkes et al. [12]; and the ADA activity was established through the amount of ammonia released by the action of the enzyme under reading in a spectrophotometer at 620 nm, according to the method described by Giusti and Galanti [17], according to standardized analytical procedures in the laboratory. Reagents used include adenosine 5'-triphosphate disodium salt, adenosine 5'-diphosphate sodium salt, 5'-monophosphate sodium salt, adenosine, Ficoll-Histopaque (Lymphoprep) and Coomassie Brilliant Blue G substrates. These were obtained from Sigma-Aldrich (St. Louis, MO, USA). All other reagents used in the experiment were of analytical grade and high purity.
The platelet sample kept in the HEPES buffer, used to evaluate the enzyme ecto-5'-nucleotidase and NTPDase in platelets, was thawed to perform the assays. First, the dosage of proteins was carried out according to the method of Bradford [18]. For protein determination, Coomassie Blue reagent was used, from which a standard curve was performed in triplicate with bovine albumin, reading in a Metash UV/VIS 5300 PC spectrophotometer, at 595 nm, and obtained, if the FC of the reagent is 0.073. For protein dosage, 50 µL of sample and 2.500 µL of Comassie Blue were added to a test tube and the concentrations were calculated.
To carry out the tests, it is necessary that the protein concentration in the sample is between 0.4 and 0.6 mg/mL. For values above these parameters, the sample was diluted with a HEPES buffer. The incubation solution was prepared using 1.2 M sodium chloride (NaCl), 60 mM glucose, 50 mM potassium chloride (KCl), 500 mM tris hydrochloride (Tris–HCl) (pH 7.4), 50 mM calcium chloride (CaCl2) and distilled water, which was added in a volume of 160 µL in each well of the plate along with 20 µL of the samples in duplicate and pre-incubated at 37 °C for 10 min. Upon removing the plate from the water bath, 20 µl of substrate (10 mM ATP/ADP) was added and incubated for 60 min; after this period, 100 µL of 15% TCA were added, which allows the interruption of the reaction. Then, staining was carried out using 30 µL of the sample and 300 µL of malachite green with absorbance reading at 630 nm. To determine the activity of ecto-5'-nucleotidase, a similar NTPDase incubation solution was prepared, replacing 50 mM CaCl2 with 100 mM magnesium chloride (MgCl2) and using 20 mM AMP as substrate. For both nucleotide hydrolysis determinations, the mean absorbance multiplied by the phosphate correction factor (FCF) and divided by the incubation time, volume and protein concentration were used. At the end, the results were expressed in nmolpi/min/mg of protein.
For ADA evaluation, two wells in the plate belonging to the same sample were identified and 30 µL of sample was pipetted only into "well 01", 90 µL of adenosine was placed in both wells, taking the plate to incubation for 60 min at 37 °C. After this period, 30 µL of the sample was pipetted into "well 02" and, in both wells, 80 µL of phenol and 80 µL of hypochlorite were added. The plate was again incubated for 30 min at 37 °C and then read at 620 nm. To define the results, the mean of the absorbances and the standard was considered, multiplied by the FC, expressing the values obtained in units/liter (U/L).
To analyze the ecto-5'-nucleotidase and NTPDase enzyme in lymphocytes, the protein concentration was measured in lymphocyte samples following the Bradford method [18], as performed in platelets. For the operation of enzyme activity, the protein concentration was adjusted to the range of 0.1–0.2 mg/mL; at the values obtained above these parameters, the sample was diluted with saline solution. The evaluation of nucleotide hydrolysis and ecto-5'-nucleotidase and NTPDase activity in lymphocytes was performed according to the protocol by Pilla et al. [11], in agreement with the one used in the platelet sample, differing only in the incubation time, which was 70 min.
For the analysis of ADA in lymphocytes, the ADA evaluation protocol was performed similarly to that performed with the platelet sample.
Statistical analysis
After preparing the electronic spreadsheets, the data were submitted to the appropriate statistical tests for each sample. Normality was tested using the Kolmogorov–Smirnov test. Statistical analyzes were performed with IBM SPSS software. The differences between the times in the group (before, after one week and after eight weeks of the physical exercise protocol), in relation to the study variables, were evaluated using the ANOVA analysis of variance. Samples that did not show normal distribution were replaced by analysis of variance ANOVA, using the Kruskal–Wallis test. When there was a difference, the times were compared to each other with Student–Newman–Keuls correction for parametric variables and Bonferroni correction for non-parametric variables. After calculating the effect size (f = 0.64), the sample size was calculated taking into account a power of 80% and a significance level of 5%. Differences in which the probability of rejection of the null hypothesis was less than 5% (p < 0.05) were considered statistically significant.
Ethical aspects
All procedures were approved by the Research Ethics Committee (CEP) of the Institute of Cardiology of Rio Grande do Sul/University Foundation of Cardiology and was registered through Plataforma Brasil under CAAE: 85,407,018.3.0000.5333. Participants were informed about the purpose of the research and about the methods used for data collection and intervention, as well as their evaluation. The guarantee of impersonality in the responses was ensured, as well as the possibility of interrupting participation when deemed necessary, as well as the right to access the results. Finally, all the requirements of the law were followed to maintain the respect, dignity and freedom of the participants.
Results
The sample consisted of 16 students from the health area of the UFFS Campus Chapecó/SC, Brazil. Of these, two were from the medical course (12.5%) and 14 from the nursing course (87.5%). The study consisted of only women, aged between 20 and 40 years (M = 23 and SD = 3.6).
Purinergic system
The laboratory analyses of the purinergic system indicated, through the Generalized Estimating Equations (GEE), with p = 0.717, that there was no difference in the mean ATP lymphocytes in relation to the moments before, one week and eight weeks after the practice of physical exercise (Fig. 1). Furthermore, with regard to the hydrolysis of ATP in platelets, through GEE, with p = 0.062, there was no difference in the mean of platelet ATP in relation to the moments before, one week and eight weeks after physical exercise (Fig. 1).

ATP hydrolysis in lymphocytes and platelets at pre, one week and eight weeks after exercise protocol. Data analyzed by the GEE test, expressed as mean and standard deviation
Regarding the hydrolysis of the ADP nucleotide in platelets, there was a significant decrease in the hydrolysis of this nucleotide in the group after 8 weeks of physical exercise, with p = 0.001. Through the GEE complemented by Bonferroni’s multiple comparisons test, at a significance level of 5%, it was found that the mean ADP platelets in the moments before and one week after exercise did not differ from each other. However, they were significantly higher than at the moment 8 weeks after exercise (Fig. 2).

ADP hydrolysis in lymphocytes and platelets at pre, one week and eight weeks after exercise protocol. Data analyzed by the GEE test, expressed as mean and standard deviation. Asterisk indicates statistical difference *p < 0.05
Regarding the AMP, through GEE, with p = 0.071 (lymphocytes) and p = 0.121 (platelets), there was no difference in the mean AMP in both lymphocytes and platelets in relation to the moments before and after the exercise protocol physical (Fig. 3).

AMP hydrolysis in lymphocytes and platelets at pre, one week and eight weeks after exercise protocol. Data analyzed by the GEE test, expressed as mean and standard deviation
Furthermore, with regard to ADA activity in lymphocytes, through GEE, with p = 0.225, it was found that there was no difference in the average of ADA lymphocytes in relation to the moments before and after physical exercise practice (Fig. 4). Regarding the ADA activity in platelets, through GEE complemented by Bonferroni’s multiple comparisons test, at a significance level of 5%, it was found that the mean in the moments before and one week after the exercise protocol did not differ between itself, however, at the moment eight weeks after exercises, the ADA activity was significantly higher than at the moment before exercise, with p = 0.041 (Fig. 4).

ADA activity in lymphocytes and platelets before, one week and eight weeks after the physical exercise protocol. Data analyzed by the GEE test, expressed as mean and standard deviation. Asterisk indicates statistical difference *p < 0.05
Oxidative profile
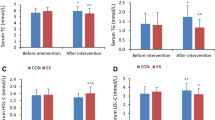
The oxidative profile of the individuals under study was evaluated by the concentrations of indicators of oxidative damage, such as lipid peroxidation by TBARS and the activity of the MPO enzyme, as well as components of the antioxidant defense system, such as PSH and NPSH. Regarding lipid peroxidation by TBARS, through GHG complemented by Bonferroni’s multiple comparisons test, at a significance level of 5%, with p = 0.012, it was found that the mean of TBARS was significantly higher in the pre moment than in the moment a week after exercises. There was no significant difference between the other moments (Table 1).
Regarding the activity of the MPO enzyme, through the GEE, with p = 0.907, there was no difference in the average of MPO in relation to the moments before, one week and eight weeks after the practice of physical exercise (Table 1).
Regarding the PSH antioxidant defense system, through GEE complemented by Bonferroni’s multiple comparisons test, at a significance level of 5%, with p = 0.004, it was found that the mean PSH was significantly lower in the pre-exercise than at other times. Furthermore, there was no significant difference between one week and eight weeks after exercise (Table 1). Finally, with regard to the NPSH antioxidant defense system, with p = 0.445, it was found that there was no difference in the mean of NPSH in relation to the moments before, one week and eight weeks after the practice of the exercise protocol (Table 1).
Discussion
As a result of the change in the population’s lifestyle in recent decades, physical inactivity has significantly contributed to the increase in sedentary lifestyles. Furthermore, a sedentary lifestyle contributes to the increase of health problems, such as hypertension, obesity, cardiovascular diseases, type 2 diabetes mellitus, among other comorbidities [19]. Thus, many studies are carried out to seek new knowledge regarding the effects of physical exercise on human health. Among the numerous alternatives studied, the components of the purinergic system and oxidative stress stand out.
Over time, the role of purinergic signaling as a mediator of the intracellular communication process, especially in immune system cells, has been recognized [7, 20]. Enzymes, such as ecto-NTPDase and ADA, stand out in terms of immune modulation, given that extracellular ATP has pro-inflammatory and platelet pro-aggregating properties and, on the other hand, ADO has anti-inflammatory and anti-aggregating properties platelet [7].
In the present study, concurrent training was associated with an increase, although not significant, in the enzymatic activity of ecto-NTPDases enzymes in lymphocytes, through increased hydrolysis of ATP and ADP. Such enzymatic activity can be explained by an increase in the concentration of ATP in the extracellular environment as a result of cell damage and the inflammatory process caused by the practice of physical exercise [7]. Activation of ecto-NTPDase in lymphocytes has also been observed in research involving swimming exercise in hypertensive patients [21].
Furthermore, concurrent training showed a correlation, although not significant, with a decrease in ADA activity in lymphocytes, indicating a high concentration of ADO available in the extracellular environment. ADO is responsible for inhibiting the effector cells of the immune system through signaling via the A2A receptor. Associating the increased activity of ecto-NTPDases and ADO, we can infer that concurrent training acts to provide the activation of anti-inflammatory mediators [21, 22].
In a study, it was demonstrated that the anti-inflammatory action resulting from regular physical exercise can be achieved through the induction of an anti-inflammatory environment at each exercise session [22]. Several mechanisms may be involved in this process, namely increased production of IL-6; increased release of adrenaline and cortisol from the adrenals; increased circulation of regulatory T cells (TReg); decreased infiltration of macrophages and monocytes in adipose tissue; decreased expression of Toll Like receptors (TLRs) in macrophages and monocytes; and decreased circulation of pro-inflammatory monocytes [22].
This study demonstrated that, although concurrent training increased the amount of extracellular ATP, possibly as a result of the cellular damage caused by the exercise itself, to increase the activity of ecto-NTPDases, we hypothesized that there must be a compensatory mechanism regarding to the immune system, since the ADA activity was reduced, to provide a greater amount of ADO, providing an anti-inflammatory action. Thus, physical training is directly related to the modulation of the purinergic system with regard to mechanisms related to inflammation. The decrease in ADA activity may be related to the maintenance of ADO in the environment, thus providing an anti-inflammatory environment [22].
In addition to the inflammatory mechanism, the purinergic system is also involved in the platelet aggregation mechanism. This work showed that there was a significant reduction in the action of the ecto-NTPDase enzyme on platelets (ADP hydrolysis) and a significant increase in ADA activity after eight weeks of concurrent training. The decrease in ADP hydrolysis after eight weeks of exercise indicates that ADP is in greater concentration in the extracellular environment. It is known that ADP in high concentration stimulates platelet aggregation [23, 24]. This result can be explained by the increase in AMP levels, although not significant, due to the increased level of ecto-NTPDase and ecto-nucleotide pyrophosphatase/phosphodiesterase (NPP) activity, responsible for the production of AMP through hydrolysis of ATP and ADP [19]. On the other hand, the increase in ADA activity corresponds to an increase in the concentration of ADO, a cytoprotective molecule responsible for the anti-inflammatory and immunosuppressive mechanism, as well as for the anti-platelet aggregation mechanism [23]. ADO competitively inhibits the ADP-induced platelet coagulation process, which corroborates the results found in our work [19].
In a study with young sedentary male adults undergoing a moderate-intensity aerobic exercise protocol, it was found that there was a significant increase in ADA activity in platelets, data similar to those found in our study [19]. With these data, it is suggested that physical exercise is able to modulate purinergic signaling, modifying the action of nucleotidases in the cell communication process. Thus, the activity of ecto-NTPDases and ADA contributes to the modulation of the inflammatory and thrombotic response resulting from physical exercise, so as to trigger alterations in the concentration of ATP, ADP, AMP and ADO.
Oxidative stress is characteristic of a diverse set of pathophysiological states of the most varied systems, from neurological diseases, such as Parkinson’s disease and Alzheimer’s disease; cardiovascular diseases, such as atherosclerosis and myocardial infarction; cancer, diabetes, kidney failure and various inflammations [25]. For the assessment of oxidative stress in the body, appropriate indicators are used, such as TBARS, MPO, PSH and NPSH.
MDA, a product of lipid peroxidation of cell membranes due to LPO reactions mediated by ROS, is an important substrate that reacts with TBA, originating the compound identified by TBARS [26]. In a study carried out with depressive patients undergoing exercise, it showed a decrease in serum TBARS levels after three weeks, a result that is in line with the decrease observed in our study when comparing the levels measured between the pre and post-exercise moments (this is, after a week of concurrent training) [27]. In another study, women with metabolic syndrome undergoing 12 weeks of physical training also demonstrated a reduction in TBARS levels; however, in our study, despite a reduction in this parameter between measurements performed in the pre- and post-periods (i.e., after eight weeks of concurrent training), the difference was not statistically significant [28].
MDA is the main and most studied product of the peroxidation of polyunsaturated fatty acids, and its interaction with deoxyribonucleic acid (DNA) and proteins is linked to the possibility of the existence or formation of systemic alterations, for example, as a mutagenic and also atherogenic factor [29]. A range of pathologies have significant potential to correlate with changes in MDA, such as liver fibrosis, progression of the inflammatory process in atherosclerosis, as well as increased platelet activation, especially in pathological conditions such as metabolic syndrome; therefore, the reduction obtained in TBARS levels may be correlated with the reduction in the development or progression of the pathological conditions just mentioned [30,31,32]. In this sense, the results of our study highlight the convergent benefit found in changing some markers (increased ADA activity and reduced TBARS levels) with regard to pathological platelet aggregation, as described in the literature on the relationship of these associated markers to this condition [23, 32].
MPO is a peroxidase expressed in leukocytes, mainly neutrophils and monocytes. In the presence of hydrogen peroxide and halides, MPO catalyzes the formation of reactive oxygen intermediates, including HOCl. In addition to playing an important role in microbial killing by neutrophils, MPO has been shown to be a local mediator of tissue damage and responsible for the resulting inflammation in several inflammatory diseases [33].
Furthermore, thiols play important roles in various aspects of cellular functions, including cellular protection against reactive oxygen and nitrogen species [34]. Thiols help maintain redox homeostasis in various cell compartments, protecting organisms from oxidative and xenobiotic stressors, acting as hydrogen peroxide scavengers in antioxidant enzymes [35]. Thus, the drop in the plasma level of thiol groups suggests a decrease in the plasma antioxidant capacity [36].
One study evaluated the oxidative profile of 16 young males after an exercise test, which was performed weekly for four months; the results showed no change in thiol levels [37]. In our study, there was a statistically significant increase in the PSH marker after one week of the exercise protocol when compared to the pre-exercise moment, suggesting an increase in the antioxidant capacity mediated by protein thiols. The slight reduction in NPSH levels, although not statistically significant, may reveal a response of this antioxidant defense in an attempt to avoid damage to the body due to oxidative stress [38]. The statistically significant increase in PSH levels in our study reveals a likely beneficial outcome for the body, as the drop in the level of protein thiols suggests a decrease in the antioxidant capacity of the plasma, which may be associated with the participation in the genesis and/or worsening of clinical conditions, as in the inflammatory process of asthma and chronic obstructive pulmonary disease, in the pathophysiology of obesity, in atherogenesis and progression of atherosclerotic plaque, and even having central nervous system outcomes, such as dopaminergic neurodegeneration of the nigrostriatal pathway [36, 39,40,41,42].
The study carried out had important limitations regarding its sample, given that many participants gave up on the physical exercise protocol (concurrent training). Furthermore, another factor that may have contributed to non-significant results, but with a tendency toward significance, concerns the training time (many studies suggest a 10-week concurrent training time) and the training frequency per week (studies have shown that a frequency of five times a week gives better results regarding the parameters of oxidative stress and the purinergic system).
Therefore, concurrent training was responsible for providing biochemical changes regarding purinergic signaling, to trigger alterations in the enzymatic activities of both ecto-NTPDases and ADA in lymphocytes and platelets. Furthermore, the modifications in oxidative stress markers converge with the results found in purinergic signaling markers, given that the reduction in TBARS levels is directly related to the decrease in the progression of inflammatory processes and decrease in platelet aggregation. Thus, it can be inferred that there is a relationship between the purinergic signaling mechanism and the oxidative stress mechanism with the inflammatory process, so that concurrent training has the ability to modulate these systems to provide an anti-inflammatory environment and anti-platelet agent, favoring a protective biological state.
Availability of data and material
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
World health organization. Global recommendations on physical activity for health. https://www.who.int/dietphysicalactivity/factsheet_recommendations/en/ (2010). Accessed 5 june 2020
Dempsey PC, Owen N, Biddle SJH, Dustan DW (2014) Managing sedentary behavior to reduce the risk of diabetes and cardiovascular disease. Curr Diab Rep 14:522. https://doi.org/10.1007/s11892-014-0522-0
Egan B, Zierath JR (2013) Exercise metabolism and the molecular regulation of skeletal muscle adaptation. Cell Metab 17:162–184. https://doi.org/10.1016/j.cmet.2012.12.012
Mathur N, Pedersen BK (2008) Exercise as a mean to control low-grade systemic inflammation. Mediat Inflamm 2008:1–6. https://doi.org/10.1155/2008/109502
Nunes RB, Alves JP, Kessler LP, Lago PD (2013) Aerobic exercise improves the inflammatory profile correlated with cardiac remodeling and function in chronic heart failure rats. Clinics (São Paulo) 68:876–882. https://doi.org/10.6061/clinics/2013(06)24
Greaney JL, Wenner MM, Farquhar WB (2015) Exaggerated increases in blood pressure during isometric muscle contraction in hypertension: role for purinergic receptors. Auton Neurosci 188:51–57. https://doi.org/10.1016/j.autneu.2014.12.003
Junger WG (2011) Immune cell regulation by autocrine purinergic signaling. Nat Rev Immunol 11:201–212. https://doi.org/10.1038/nri2938
Burnstock G (2007) Purine and pyrimidine receptors. Cell Mol Life Sci 64:1471–1483. https://doi.org/10.1007/s00018-007-6497-0
North RA (2002) Molecular physiology of P2X receptors. Physiol Rev 82:1013–1067. https://doi.org/10.1152/physrev.00015.2002
Böyum A (1968) Isolation of mononuclear cells and granulocytes from human blood. Isolation of mononuclear cells by one centrifugation, and of granulocytes by combining centrifugation and sedimentation at 1 g. Scand J Clin Lab Invest Suppl 97:77–89
Pilla C, Emanuelli T, Frassetto SS, Battastini AM, Dias RD, Sarkis JJ (1996) ATP diphosphohydrolase activity (Apyrase, EC 3.6.1.5.) in human blood platelets. Platelets 7:225–230. https://doi.org/10.3109/09537109609023582
Lunkes GI, Lunkes D, Stefanello F, Morsch A, Morsch VM, Mazzanti CM, Schetinger MRC (2003) Enzymes that hydrolyze adenine nucleotides in diabetes and associated pathologies. Thromb Res 109:189–194. https://doi.org/10.1016/s0049-3848(03)00178-6
Jentzsch AM, Bachmann H, Fürst P, Biesalski HK (1996) Improved analysis of malondialdehyde in human body fluids. Free Radic Biol Med 20:251–256. https://doi.org/10.1016/0891-5849(95)02043-8
Ohkawa H, Ohishi N, Yagi K (1979) Assay for lipid peroxides in animal tissues by thiobarbituric acid reaction. Anal Biochem 95:351–358. https://doi.org/10.1016/0003-2697(79)90738-3
Ellman GL (1959) Tissue sulfhydryl groups. Arch Biochem Biophys 82:768–774. https://doi.org/10.1016/0003-9861(59)90090-6
Suzuki K, Ota H, Sasagawa S, Sakatani T, Fujikura T (1983) Assay Method for myeloperoxidase in human polymorphonuclear leukocytes. Anal Biochem 132:345–352. https://doi.org/10.1016/0003-2697(83)90019-2
Giusti G, Galanti B (1984) Adenosine deaminase: colorimetric method. Methods Enzym Anal 4:315–323
Bradford MA (1976) Rapid and sensitive method for the quantification of microgram quantities of protein utilizing the principie ofprotein-dyebinding. Anal Biochem 72:248–254. https://doi.org/10.1006/abio.1976.9999
Moritz CEJ, Teixeira BC, Rockenbach L, Reischak-Oliveira A, Casali EA, Battastini AMO (2017) Altered extracellular ATP, ADP, and AMP hydrolysis in blood serum of sedentary individuals after an acute, aerobic, moderate exercise session. Clin Trial 426:55–63. https://doi.org/10.1007/s11010-016-2880-1
Bours MJL, Swennen ELR, Di Virgilio F, Cronstein BN, Dagnelie PC (2006) Adenosine 5’-triphosphate and adenosine as endogenous signaling molecules in immunity and inflammation. Pharmacol Ther 112:358–404. https://doi.org/10.1016/j.pharmthera.2005.04.013
Cardoso AM, Abdalla FH, Bagatini MD, Martins CC, Zanini D, Schmatz R, Jaques JA, Leal DBR, Morsch VM, Schetinger MRC (2015) Swimming training prevents alterations in ecto-NTPDase and adenosine deaminase activities in lymphocytes from Nω-nitro-L-arginine methyl ester hydrochloride induced hypertension rats. J Hypertens 33:763–772. https://doi.org/10.1097/hjh.0000000000000468
Gleeson M, Bispo NC, Stensel DJ, Lindley MR, Mastana SS, Nimmo MAV (2011) The anti-inflammatory effects of exercise: mechanisms and implications for the prevention and treatment of disease. Nat Rev Immunol 11:607–615. https://doi.org/10.1038/nri3041
Fürstenau CR, Trentin DDS, Barreto-chaves MLM, Sarkis JJF (2006) Ecto-nucleotide pyrophosphatase/phosphodiesterase as part of a multiple system for nucleotide hydrolysis by platelets from rats: kinetic characterization and biochemical properties. Platelets 17:84–91. https://doi.org/10.1080/09537100500246641
Podgorska K, Derkacz A, Szahidewicz-Krupska E, Jasiczek J, Dobrowolski P, Radziwon-Balicka A, Skomro R, Szuba A, Mazur G, Doroszko A (2017) Effect of regular aerobic activity in young healthy athletes on profile of endothelial function and platelet activity. Biomed Res Int 2017:1–9
Uppu RM, Woods D, Nl Parinandi (2020) Measurement of Oxidative Stress Status in Human Populations: a critical need for a metabolomic profiling. Measuring Oxidants And Oxidative Stress In Biological Systems. Springer, Cham, pp 123–131
Ayala A, Muñoz MF, Argüelles S (2014) Lipid peroxidation: production, metabolism, and signaling mechanisms of malondialdehyde and 4-hydroxy-2-nonenal. Oxid Med Cell Longev 2014:1–31
Schuch FB, Vasconcelos-Moreno MP, Borowsky C, Zimmermann AB, Wollenhaupt-Aguiar B, Ferrari P, Fleck MPA (2014) The effects of exercise on oxidative stress (TBARS) and BDNF in severely depressed inpatients. Eur Arch Of Psychiatry Clin Neurosci 264:605–613. https://doi.org/10.1007/s00406-014-0489-5
Farinha JB, Steckling FM, Stefanello ST, Cardoso MS, Nunes LS, Barcelos RP, Duarte T, Kretzmann NA, Mota CB, Bresciani G, Moresco RN, Duarte MMMF, Santos DL, Soares FAA (2015) Response of oxidative stress and inflammatory biomarkers to a 12-week aerobic exercise training in women with metabolic syndrome. Sports Med Open 1:19. https://doi.org/10.1186/s40798-015-0011-2
Rio D, Stewart AJ, Pellegrini NA (2005) A review of recent studies on malondialdehyde as toxic molecule and biological marker of oxidative stress. Nutr Metab Cardiovasc Dis 15:316–328. https://doi.org/10.1016/j.numecd.2005.05.003
Albano E, Mottaran E, Vidali M, Reale E, Saksena S, Occhino G, Burt AD, Dia CP (2005) Immune response towards lipid peroxidation products as a predictor of progression of non-alcoholic fatty liver disease to advanced fibrosis. Gut 54:987–993
Papac-Milicevic N, Busch CJL, Binder CJ (2016) malondialdehyde epitopes as targets of immunity and the implications for atherosclerosis. Adv Immunol 131:1–59. https://doi.org/10.1016/bs.ai.2016.02.001
Zagol-Ikapite I, Sosa IR, Oram D, Judd A, Amarnath K, Amarnath V, Stec D, Oates JA, Boutaud O (2015) Modification of platelet proteins by malondialdehyde: prevention by dicarbonyl scavengers. J Lipid Res 56:2196–2205
Aratani Y (2018) Myeloperoxidase: its role for host defense, inflammation, and neutrophil function. Arch Biochem Biophys 640:47–52. https://doi.org/10.1016/j.abb.2018.01.004
Yang Y, Guan X (2017) Non-protein thiol imaging and quantification in live cells with a novel benzofurazan sulfide triphenylphosphonium fluorogenic compound. Anal Bioanal Chem 409:3417–3427. https://doi.org/10.1007/s00216-017-0285-y
Ulrich K, Jakob U (2019) The role of thiols in antioxidant systems. Free Radic Biol Med 140:14–27. https://doi.org/10.1016/j.freeradbiomed.2019.05.035
Rossi R, Giustarini D, Milzani A, Dalle-Donne I (2008) Cysteinylation and homocysteinylation of plasma protein thiols during ageing of healthy human beings. J Cell Mol Med 13:3131–3140. https://doi.org/10.1111/j.1582-4934.2008.00417.x
Zinellu A, Sotgia S, Caria MA, Tangianu F, Casu G, Deiana L, Carru C (2006) Effect of acute exercise on low molecular weight thiols in plasma. ScandJ Med Sci Sports 17:452–456. https://doi.org/10.1111/j.1600-0838.2006.00542.x
Laaksonen DE, Atalay M, Niskanen L, Uusitupa M, Hänninen O, Sen CK (1999) Blood glutathione homeostasis as a determinant of resting and exercise-induced oxidative stress in young men. Redox Rep 4:53–59. https://doi.org/10.1179/135100099101534648
Zinellu A, Fois AG, Sotgia S, Zinellu E, Bifulco F, Pintus G, Mangoni AA, Carru C, Pirina P (2016) Plasma protein thiols: an early marker of oxidative stress in asthma and chronic obstructive pulmonary disease. Eur J Clin Invest 46:181–188. https://doi.org/10.1111/eci.12582
Picklo MJ, Idso JP, Jackson MI (2013) S-Glutathionylation of Hepatic and Visceral Adipose Proteins Decreases in Obese Rats. Obesity 21:297–305
Lepedda AJ, Formato M (2020) oxidative modifications in advanced atherosclerotic plaques: a focus on in situ protein sulfhydryl group oxidation. Oxid Med Cell Longev 2020:1–7
Patsoukis N, Papapostolou I, Zervoudakis G, Georgiou CD, Matsokis NA, Panagopoulos NT (2004) Thiol redox state and oxidative stress in midbrain and striatum of weaver mutant mice, a genetic model of nigrostriatal dopamine deficiency. Neurosci Lett 376:24–28. https://doi.org/10.1016/j.neulet.2004.11.019
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
Conceptualization: MRB, FBG and DTReS; Methodology: ECS, FM, BSRB and MDB; Formal analysis and investigation: MRB and FBH; Writing–preparation of the original sketch: MRB and ECS; Writing–revision and editing: MRB and DTReS.
Corresponding author
Ethics declarations
Conflicts of interest
All authors declares there is no conflict of interest.
Ethical approval
All procedures were approved by the Research Ethics Committee (CEP) of the Institute of Cardiology of Rio Grande do Sul/University Foundation of Cardiology and was registered through Brazil Platform under CAAE: 85407018.3.0000.5333. Participants were informed about the purpose of the research and about the methods used for data collection and intervention, as well as their evaluation. Finally, all the requirements of the law were followed to maintain the respect, dignity and freedom of the participants.
Informed consent
Not applicable.
Consent for publication
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Bizuti, M.R., de Camargo Schwede, E., Haag, F.B. et al. Concurrent training is able to increase the activity of adenosine deaminase in platelets in young women. Sport Sci Health 19, 849–859 (2023). https://doi.org/10.1007/s11332-022-00970-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11332-022-00970-9