
Abstract
Background
Clusters’ behaviors can change with age, moving from adolescence to adulthood.
Aims
This study examined physical activity (PA), diet, and sedentary behavior (SB) clusters according to age groups (11–12, 13–15, 16–17, and 18–19 years) and its association with sex and maternal education.
Methods
Brazilian National School-based Health Survey (PeNSE 2015) (n = 16,522) data were analysed. Adolescents responded PA; consumption of fruits, vegetables; snacks, salt, and beverages (SSB); and SB. Two-step cluster analysis and Rao-Scott Chi square test were used.
Results
The Actives; the All-day sitters; the Inactive 1 (with moderate consumption of F&V); and the Inactive 2 (with small consumption of F&V and SSB) clusters were identified. The Actives and All-day sitters existed in all age groups. The Inactive 1 were the cluster more prevalent in 11–12 (33.9%), 13–15 (42.5%) and 16–17 (43.8%) age groups while, All-day sitters were most prevalent in 18–19 (43.7%) age group. Boys were more likely to be in the Actives; as against girls in All-day sitters, Inactive 1 and 2 clusters. The Actives had a higher proportion of adolescents with low maternal education.
Conclusions
SB increase in clusters over the increase of age group; else, adolescents in Actives groups decreased.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Physical activity (PA), diet, and sedentary behavior (SB) plays an important role in obesity and healthy-related outcomes in adolescents [1, 2] and may contribute to prevention of noncommunicable diseases in adulthood [3]. Considering a more integrated approach to promote health, researches on behavioral clustering has increased in recent times [4, 5]. Indeed, clustering is a widely used technique in data-driven applications for identifying patterns in datasets. Specifically, two-step cluster analysis is a statistical method that can automatically identify similar clusters of people within data sets using k-means clustering algorithm [6]. Previous reviews [6,7,8] have presented different cluster behaviors among adolescents, however, few studies consider identify how these synergic obesogenic behaviors cluster in different stages of adolescence; since these, modifiable behaviors can change with age increases [9] or to persist into adulthood [10, 11].
Is known that PA, diet, and SB in its unhealthy form tend to cluster in certain subgroups [4, 6]. Studies have been reported some types clusters according to age, like as in Australian children three clusters (“most healthy”, “energy dense consumer who watch TV” and “high SB with low moderate to vigorous PA”) were found in all age groups (5–6 and 10–12 years old) [6]. Two similar lifestyles patterns, “snacking and sedentary” and “varied food and PA”, were identified in French children aged 3–6 and 7–11 years old [12]. However, older adolescents were significantly more likely to be in clusters characterized with low levels of PA and SB [13] since this, younger adolescents (12.5–14.99 years old) were more likely to be in healthier cluster behaviors as compared to older adolescents (15–17.5 years old) [14]. Understand deeper how these behaviors interact differ according to age may assist the targeting of public health initiatives and then as such interventions that stimulate a positive pattern to produce health benefits.
Besides behavior clusters in different ways in adolescents its can differ according to sociodemographic indicators (e.g., sex and maternal education) [6, 15]. For instance, younger adolescent boys and girls were allocated in healthier clusters compared to the older ones [16, 17]. Studies comparing clusters between sexes, have shown that a higher proportion of boys were observed in clusters with higher levels of PA [16, 18, 19], in contrast to girls [13, 18, 19]. On the other hand, girls appeared in a greater proportion than boys in clusters characterized with better quality of diet [14, 20] and high time spent on screen activities [21]. In addition, previous studies observed an association between clusters and low education level of adolescents’ parents [6, 22, 23].
Furthermore, clusters considering PA, diet, and SB have been associated according to social, economic, and cultural aspects, which affect individual behaviors differently, however are a lack of evidence regarding factors that influence clustering behaviors [9]. Thus, to identify adolescents clusters according to age groups in low and upper-middle income countries, like Brazil, is needed [7]. A study pointed that Brazilian adolescents with higher maternal education levels were more likely to be in the healthiest clusters (e.g., Health-promoting PA and diet) [24]. Thus, this study aims to examine clusters of PA, diet, and SB according to age groups and its association with sociodemographic indicators in a representative sample of Brazilian adolescents.
Methods
Study design and population
Data were derived from the National Adolescents School-based Health Survey (PeNSE), a cross-sectional study conducted in 2015, whose main objective was to obtain lifestyle data of adolescents enrolled in private and public schools in Brazil. The aims, methods, sample, and ethics procedure have been described in detail previously [25]. Briefly, PeNSE is part of Brazil’s surveillance of risk and protective factors for chronic diseases. It was supported through partnerships with Brazilian Institute of Geography and Statistics (IBGE), Brazilian Ministry of Education, Brazilian Ministry of Health, Health Surveillance Secretariat, World Health Organization, Centers for Disease Control and Prevention of the United States, and Pan-American Health Organization. This study was submitted and approved by the National Research Ethics Commission (CONEP) number 1.006.467/2015.
This study used PeNSE sample two (adolescents enrolled from the 6th grade of elementary school to the 3rd grade of high school). Each geographic stratum (five macro-regions) was one unit; and in each macro-region, schools and classrooms were dimensioned and selected in advance as conglomerates. The size of the sample was calculated to provide estimates in each of the geographical strata. Further details on the sampling design and weighting can be found elsewhere [25]. All adolescents present in class were invited to participate in the study. Once they agreed to participate, they were asked to respond to an electronic questionnaire on a smartphone during regular school hours. To monitor main indicators, the questionnaire was divided into steps that included household and school contexts; eating habits; PA and body image; use of psychoactive substances; violence; accidents; and sexual behavior. All procedures were carried out by previously trained IBGE technicians for adjustments and adequacy. Briefly, IBGE state supervisors were trained so they could replicate the same training course to the interviewers, in each federative unit. The main objective of this strategy was to ensure the quality and standardization of the procedures for data collection [25]. The measures of interest were previously validated [26].
Cluster variables
Physical activity
Leisure time PA was accessed using the question: “In the past 7 days, excluding the physical education class, how many days did you partake in physical activities like sports, dance, gym exercises, combat sports, or any other activity? The answers ranged from none to seven days in a week.
Sedentary behavior
SB was accessed with the question “in a regular day, how much time do you spend watching television, playing videogames, talking with friends, or others sitting activities?” The responses ranged from one to nine hours a day.
Dietary-patterns
Seven questions were used to assess diet. Adolescents reported how often (one to seven days) during the past week they had eaten fruits, green salads or vegetables, deep-fried empanadas, candies, soda, ultra-processed food and fast foods. To identify dietary patterns Principal Component Analysis (PCA) was performed. The Kaiser–Meyer–Olkin (KMO) test of sampling adequacy and Bartlett's Test of Sphericity were used to assess the suitability of the data for PCA, considering values > 0.60 and p < 0.05, respectively [27]. The number of components were decided with the Kaiser criterion and the screen plot (eigenvalues > 1) [27]. Factor loadings represent the correlations of each predictor indicator with the dietary pattern score. Higher absolute values of factor loadings indicate that the predictor contributes the most to the construction of a particular component. The dietary components (patterns) were named according to the characteristics of the behaviors retained in each of them (Supplementary file 1). Two components were identified: 1) F&V (fruits and green salads and vegetables); and 2) Snacks, salt and beverages (SSB) (deep-fried empanadas, candies, soda, ultra-processed food and fast foods). The food items in each component were scored and divided by the number of variables present in each component (2 and 5) resulting in two dietary patterns F&V and SSB.
Sociodemographic variables
Sex and maternal education were accessed through a questionnaire. Maternal education was accessed with the question “What is your mother’s level of education?” and the possible answers were categorized as low (non-educated, elementary school); medium (high school); high (graduated, higher education) and unknown. Maternal education was chosen since is the indicator most present in clusters studies when made comparisons with sociodemographic variables [13].
Statistical analysis
Only adolescents with complete data in all the variables of the analyses were considered eligible for this secondary data analysis. The descriptive data of the sociodemographic characteristics were presented in absolute and relative frequencies, with respective confidence intervals (95% CI). Two-step cluster analysis was performed using SPSS for Windows (version 23 SPSS Inc.; Chicago, IL, USA) for each age groups (11–12, 13–15, 16–17, and 18–19 years). The two-step cluster analysis is a scalable cluster analysis algorithm that was designed to manage large datasets. The analysis has two steps: pre-clustering and clustering [28]. In the pre-clustering step, all the cases in the data are scanned and the log-likelihood distance between them is measured to determine whether they are going to form pre-clusters based on some threshold distance criterion. In the second step, the subclusters resulting from the pre-clustering step are clustered into the optimal number of clusters using an agglomerative clustering algorithm. The subclusters are regarded as single cases and merged into one cluster by satisfying the minimum distance in (1) until all data are placed within a single cluster [28].
Four variables were considered in cluster analyses: (1) number of days for leisure-time PA; (2) number of days a week when F&V were eaten; (3) number of days a week when SSB were eaten; and (4) number of hours spent in SB. The best combination of a low value in Schwarz’s Bayesian Information Criterion (BIC) were used to define the number of clusters (Supplementary file 2). The log-likelihood ratio was used to measure the distance between the individual observations in the grouping variables. Leisure-time PA, SB, F&V, and SSB were analyzed by one‐way ANOVA to compare between the clusters (Actives, All-day sitters, Inactive 1, and Inactive (2) and the age groups (11–12, 13–15, 16–17, and 18–19 years old). To examine the associations between sociodemographic variables and clusters the Rao-Scott Chi square test, performed in Stata statistical software, version 15 (Stata Inc., College Station, TX, United States of America) was used. Partial eta-square effect sizes were also reported, considering small (≤ 0.05), moderate (0.06–1.3), and high (≥ 1.4) values of effect size [29]. Methods for complex analysis was used to incorporate strata, conglomerates, and sample weight. A significant level of p < 0.05 was assumed.
Results
Sample characteristics
A total of 16,522 adolescents were evaluated. Boys and girls presented almost even split (boys 50.1%); and 43% of the adolescents were in the 13 to 15 age group. More than 27% had mothers with low educational levels (Table 1).
Cluster solutions
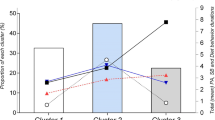
A total of 16,336 adolescents were eligible for cluster analysis, while 220 with incomplete data were excluded. Information about the best fit models are presented in Supplementary file 2 and comparison of the four age groups according to the clusters solution in Table 2. Four clusters in adolescents were identified to 11–12 age group; and three clusters comprising the 13–15, 16–17, and 18–19 age groups. Clusters were named according to the most accentuated/highlight behaviors, for example, cluster Actives were characterized with high number of days per week practicing PA. Highlight behaviors can be easily observed in Fig. 1. Silhouette coefficient indicating cohesion and separation were used to identify the quality of cluster solutions in each of the age groups and all values were 0.40, indicating fair models.

Cluster solutions for physical activity, diet, and sedentary behavior according to age group in Brazilian adolescents, National Adolescents School-based Survey—PeNSE, 2015 (n = 16,336). Note: PA physical activity; SB sedentary behavior; F&V fruit and vegetables; SSB snacks, salt and beverages
Information on the characteristics and comparisons between the clusters according to the age group can be found in Table 2. Leisure-time PA, SB, F&V, and SSB were differentiated among clusters using multivariate analysis (p < 0.001). Leisure-time PA and SB contributed most to the distinction between clusters (Partial eta-squared largest effect size). Four different cluster were observed: The Actives; the All-day sitters; the Inactive 1 (with moderate consumption of F&V); and the Inactive 2 (with small consumption of F&V and SSB). The Actives cluster were present in all age groups and was characterized by more than 5 days/week of leisure-time PA and more than 4 days/week of F&V consumption. However, this group accumulated moderate levels of SB in daily life. The All-day sitters cluster too, were present in all age groups; and included high levels of SB (more than 7 h/day, except for the 18–19 age group); small participation in leisure-time PA; and consumed SSB on more than 3 days/week. The Inactive clusters were most prevalent in all age groups (except among the 18–19 age group) and were mainly characterized by lack of leisure-time PA (Fig. 1). The Inactive clusters were different from the All-day sitters, in that their SB was less than 3 h a day. More than 55% of 11–12 years old adolescents had inactive clusters. Despite similarities, the 18–19 age group seemed to differ in some aspects. It had a smaller proportion of the Actives cluster and the most prevalent cluster was the All-day sitters. However, SB was lower than in the other age groups (less than 5 h/day); and this cluster did not present low to moderate F&V consumption as observed in other age strata (Fig. 1).
Differences in sociodemographic characteristics according to cluster
Association between clusters and sociodemographic characteristics are shown in Table 3. In all age groups there were associations between sex and clusters. The All-day sitters, Inactive 1 and Inactive 2 clusters had a majority of girls; while the Actives cluster across all age groups had a majority of boys. Maternal education had an association with all age groups. In all clusters, except in the Actives, the 11–12 age group were in a majority in the category where maternal education was unknown. There were no significant differences between the medium, low, and unknown maternal education categories in the 13–15 and 16–17 age groups. In addition, in all clusters, the 18–19 age group were in a majority in the low maternal education category.
Discussion
As far as we know, this is the first study to use cluster analysis to identify how healthy and unhealthy behaviors (including PA, diet and SB) are displayed in Brazilian adolescents according to age groups (11–12, 13–15, 16–17, and 18–19 years old) and its association with sex and maternal education. While similar studies that had used the cluster analysis approach in different age ranges were found in other populations and countries [12, 23, 30, 31], the synergic obesogenic behaviors in different stages of adolescence had been little explored. Four clusters were identified: Actives, All-day sitters, Inactive 1 (with moderate consumption of F&V); and the Inactive 2 (with small consumption of F&V and SSB). A large proportion of adolescents had an inactive cluster in all age groups. In addition, in all age groups, boys were more likely to be in the Actives cluster than girls and associations were found between clusters and educational levels. These results can contribute to create strategies to reduce SB, increase PA and stimulate a healthy diet concurrently in adolescents.
The Actives cluster was observed to be the healthiest and appeared across all age groups. They were characterized by high levels of PA and F&V consumption with a moderate time spent in SB. It seems that adolescents with higher levels of PA trigger the adoption of other healthy behaviors. This behavioral synergy that was observed was consistent with previous researches [6, 12, 30, 31]. Results similar to ours were found in studies conducted in Australia, France, and Spain that investigated clusters of obesogenic behavior in samples of younger (including children) and older adolescents. They also found that the healthiest cluster had spent the highest time in moderate-to-vigorous PA and had adopted other healthy behaviors (e.g., low consumption of energy-dense foods, spent least time watching TV, and had a high consumption of healthy foods) [12, 23, 30].
In all age groups, a pattern characterized by high time spent in SB with high consumption of SSB was observed in the All-day sitters cluster; and similar results were observed in others studies [14, 15]. Since this clusters was inductive of a moderate consumption of F&V; in this sense, compensatory health beliefs may have appeared for this group because of the adolescents rationalizing and believing that consuming healthy foods could compensate for SB and an unhealthy diet [32]. A combination of healthy and unhealthy behaviors also appears in the Inactive clusters and a good diet pattern had a synergic interaction with low levels of PA. A study indicated that calorie restriction is more effective than exercise programs for weight loss [33]. In addition, since adhering to healthy diet habits and PA involve discomfort and efforts [34]; perhaps eating healthy foods demands less effort than practicing PA. Antagonistic behaviors (positive diet and other unhealthy obesogenic behavior) are consistent with others studies [12, 14, 15].
The unhealthiest cluster (Inactive 1) was the most prevalent in the 11–12, 13–15, and 16–17 age groups. In addition, the present study showed that all clusters presented at least one unhealthy behavior in all age groups, even in the healthiest cluster, which corroborates with others studies [6, 12]. A fact worth highlighting is that adolescents in all cluster behaviors and age groups spent more than 2 h in SB. Perhaps, right from early adolescence, greater attention should be given to promoting synergistically healthy behaviors that also focus on reducing sedentary time [3] once, prolonged sitting have been related as a risk factor to chronic diseases such as mental health, cancer, obesity and cardiovascular disease [35]. Thus, considering cluster characterized with at least one unhealthy behavior it supports the need of targeting increase PA, reduce SB and improve the quality of diet in adolescents at the same time. Also, distinct strategies should be considered in accordance with the characteristics of adolescents in each cluster; for example, adolescents in the Actives cluster can be provided with actions to be taken to decrease SB and SSB consumption.
Considering the differences between age groups, previous studies reported a higher prevalence of younger adolescents in clusters with high levels of PA [6, 13, 14]. While the present study is consistent with literature, the Actives clusters was most prevalent in the 11–12 and 16–17 age groups. In addition, older adolescents had a higher presence in the Inactive 1 cluster that corroborated a study [15], which found that older adolescents had a higher presence in clusters considered unhealthy (e.g., low PA, diet quality, and time in SB). It is noteworthy that the proportion of adolescents in the Inactive 1 cluster increased with advancing age, and there was a slight decrease in the 18–19 age group. While we were not able to infer a causal relationship between health risk clusters and age groups; more than 70% of the sample in all age groups seemed to be at a risk for obesity.
As consistent with previous studies [6, 15,16,17,18,19]; boys in all age groups, were more likely to be in the Actives cluster than girls; whereas girls were more likely to be in the All-day sitters, Inactive 1, and Inactive 2 clusters than boys. There is, therefore, a need for intervention programs that would target the reduction in SB and increase of PA for Brazilian girls in all age groups. Investigate how these obesogenic behaviors are grouped according to different age groups, in a representative sample, was reported as a gap in a previous review [6]. It is worth mentioning that clustering of people who share similar characteristics is a concept that has been successfully applied to understanding the relationships between different lifestyle behaviors [6]. Since these obesogenic behaviors combine in complex ways have a cumulative effect on the development of overweight, obesity, and/or non-communicable diseases, this has important implications for public health because understanding which behaviors need to be targeted simultaneously and in whom obesogenic behaviors cluster together can be used to assist in the elaboration of targeted obesity prevention initiatives [6]. Tailoring interventions for appropriately targeted and effectively bring about multiple behavior changes, may be more cost-effective and maximize reach to those most in need [6].
There were associations between clusters and educational levels in all groups, except the 11–12 age group, which perhaps, occurred because of their difficulties in reporting about their mothers’ schooling. In our study, the Actives group had a higher proportion of adolescents with low maternal education; which was consistent with studies from Brazil and Portugal [36] and inconsistent with previous studies conducted in Brazil [37] and high-income countries [6, 13, 20, 23]. Indeed, health-risk clusters were associated with low maternal education as was previously observed in the literature on younger and older adolescents [6, 13, 20, 23]. It would expect that parents with a higher level of education are generally better informed and are more aware of the importance of PA on the health status of their children and adolescents [38]. Then, better-educated parents more likely to encourage their children to engage in some form of sports or PA. The educational level reflects parental knowledge on healthy lifestyle and influence in youth engagement in healthy behaviors [39]. However, even that parents recognized the importance of PA, barriers like lack of environmental barriers (e.g., safety issues, heavy traffic, lack local and unsafe neighborhood) and personal (e.g., prefer SB activities as screen-based technologies) are barriers to PA [39]. As these screen-based technologies are probably few accessible to families with low levels of education, adolescents may become more physically active, especially outside the home. However, caution is needed to extrapolate these results since we do not test this hypothesis. In addition, differences, particularly in the Actives, call attention to Brazil’s high social inequality [40], where adverse social conditions seem to impose a negative synergy in adolescents’ behaviors, even in healthy groups.
It needs to be acknowledged some limitations since the measures were self-reported, it could have resulted in participants’ answers being influenced by social desirability and memory bias. Moreover, since the design included the biases of cross-sectional cluster analysis where the causal relationship cannot be assumed; the assumed similarities and differences between the age groups cannot be expected only as a consequence of early age behavior antecedents. The transition and stability of clustering behavior over time should be distinguished through more robust research designs considering PA, diet, and SB using recalls and objective measures. Despite these limitations, this study was a nationally representative sample of Brazilian adolescents, utilizing a previously validated questionnaire, applying a sophisticated statistical analysis based on a data-driven procedure, and it facilitated the investigation of adolescents’ groups with similar behaviors based on age in an upper-middle-income country.
Conclusions
Four clusters of obesogenic behaviors were identified in Brazilian adolescents and its formation was similar across different adolescent age groups. All the age groups were highly exposed to an unhealthy cluster and even those with a healthy cluster were exposed to higher SB. Despite the fact that unhealthy behavior declines in older age groups; this proportion reaches a maximum drop of one third. We considered risk-groups of girls and we suggested intervention including more than one behavior to this group. Finally, our study suggested a reduction of SB in clusters at all ages and both sexes; an increase in PA in girls, and in adolescents aged 13–15 and 18–19 years.
References
Ells LJ, Rees K, Brown T, Mead E, Al-Khudairy L, Azevedo L et al (2018) Interventions for treating children and adolescents with overweight and obesity: an overview of Cochrane reviews. Int J Obes 42(11):1823–1833
Weihrauch-Blüher S, Kromeyer-Hauschild K, Graf C, Widhalm K, Korsten-Reck U, Jödicke B et al (2018) Current guidelines for obesity prevention in childhood and adolescence. Obes Facts 11(3):263–276
WORLD HEALTH ORGANIZATION (2019) Global action plan on physical activity 2018–2030: more active people for healthier world. World Health Organization
Gubbels JS, van Assema P, Kremers SPJ (2013) Physical activity, sedentary behavior, and dietary patterns among children. Curr Nutr Rep 2(2):105–112
Dumuid D, Olds T, Lewis LK, Martin-Fernández JA, Barreira T, Broyles S et al (2018) The adiposity of children is associated with their lifestyle behaviours: a cluster analysis of school-aged children from 12 nations: children’s adiposity relates to their lifestyle behaviours. Pediatr Obes 13(2):111–119
Leech RM, McNaughton SA, Timperio A (2014) The clustering of diet, physical activity and sedentary behavior in children and adolescents: a review. Int J Behav Nutr Phys Act 11(1):4
D’Souza NJ, Kuswara K, Zheng M, Leech R, Downing KL, Lioret S et al (2020) A systematic review of lifestyle patterns and their association with adiposity in children aged 5–12 years. Obes Rev 21(8):13029
Parker KE, Salmon J, Costigan SA, Villanueva K, Brown HL, Timperio A (2019) Activity-related behavior typologies in youth: a systematic review. Int J Behav Nutr Phys Act 16(1):1–13. https://doi.org/10.1186/s12966-019-0804-7
Viner RM, Ozer EM, Denny S, Marmot M, Resnick M, Fatusi A et al (2012) Adolescence and the social determinants of health. The Lancet 379(9826):1641–1652
Craigie AM, Lake AA, Kelly SA, Adamson AJ, Mathers JC (2011) Tracking of obesity-related behaviours from childhood to adulthood: a systematic review. Maturitas 70(3):266–284
Gordon-Larsen P, Adair LS, Popkin BM (2002) Ethnic differences in physical activity and inactivity patterns and overweight status. Obes Res 10(3):141–149
Lioret S, Touvier M, Lafay L, Volatier J-L, Maire B (2008) Dietary and physical activity patterns in French children are related to overweight and socioeconomic status. J Nutr 138(1):101–107
Liu J, Kim J, Colabianchi N, Ortaglia A, Pate RR (2010) Co-varying patterns of physical activity and sedentary behaviors and their long-term maintenance among adolescents. J Phys Act Health 7(4):465–474
Ottevaere C, Huybrechts I, Benser J, De Bourdeaudhuij I, Cuenca-Garcia M, Dallongeville J et al (2011) Clustering patterns of physical activity, sedentary and dietary behavior among European adolescents: the HELENA study. BMC Public Health 11(1):328
Cuenca-García M, Huybrechts I, Ruiz JR, Ortega FB, Ottevaere C, González-Gross M et al (2013) Clustering of multiple lifestyle behaviors and health-related fitness in European Adolescents. J Nutr Educ Behav 45(6):549–557
Patnode CD, Lytle LA, Erickson DJ, Sirard JR, Barr-Anderson DJ, Story M (2011) Physical activity and sedentary activity patterns among children and adolescents: a latent class analysis approach. J Phys Act Health 8(4):457–467
Marshall SJ, Biddle SJH, Sallis JF, McKenzie TL, Conway TL (2002) Clustering of sedentary behaviors and physical activity among youth: a cross-national study. Pediatr Exe Sci 14(4):401–417
Seghers J, Rutten C (2010) Clustering of multiple lifestyle behaviours and its relationship with weight status and cardiorespiratory fitness in a sample of Flemish 11- to 12-year-olds. Public Health Nutr 13(11):1838–1846
Jago R, Fox KR, Page AS, Brockman R, Thompson JL (2010) Physical activity and sedentary behaviour typologies of 10–11 year olds. Int J Behav Nutr Phys Act 7(1):59
Boone-Heinonen J, Gordon-Larsen P, Adair LS (2008) Obesogenic clusters: multidimensional adolescent obesity-related behaviors in the US. Ann Behav Med 36(3):217–230
Nuutinen T, Lehto E, Ray C, Roos E, Villberg J, Tynjälä J (2017) Clustering of energy balance-related behaviours, sleep, and overweight among Finnish adolescents. Int J Public Health 62(8):929–938
Cameron AJ, Crawford DA, Salmon J, Campbell K, McNaughton SA, Mishra GD et al (2011) Clustering of obesity-related risk behaviors in children and their mothers. Ann Epidemiol 21(2):95–102
Leech RM, McNaughton SA, Timperio A (2014) Clustering of children’s obesity-related behaviours: associations with sociodemographic indicators. Eur J Clin Nutr 68(5):623–628
Matias TS, Silva KS, da Silva JA, de Mello GT, Salmon J (2018) Clustering of diet, physical activity and sedentary behavior among Brazilian adolescents in the national school - based health survey (PeNSE 2015). BMC Public Health. https://doi.org/10.1186/s12889-018-6203-1
de Oliveira MM, Campos MO, de Andreazzi MAR, Malta DC, de Oliveira MM, Campos MO et al (2017) Characteristics of the national adolescent school-based health survey–PeNSE, Brazil. Epidemiol E Serv Saúde 26(3):605–616
Guedes DP, Lopes CC (2010) Validation of the Brazilian version of the 2007 youth risk behavior survey. Rev Saúde Púb 5:44
Kaiser HF (1974) An index of factor simplicity. Psychometrika 39:31–36
IBM (2020) IBM SPSS statistics algorithms.
Cohen J (1988) Statistical power analysis for the behavioral sciences, 2nd edn. Hillsdale. L Erlbaum Associates, p 567
Leech RM, McNaughton SA, Timperio A (2015) Clustering of diet, physical activity and sedentary behaviour among Australian children: cross-sectional and longitudinal associations with overweight and obesity. Int J Obes 39(7):1079–1085
Pérez-Rodrigo C, Gil Á, González-Gross M, Ortega R, Serra-Majem L, Varela-Moreiras G et al (2015) Clustering of dietary patterns, lifestyles, and overweight among spanish children and adolescents in the ANIBES study. Nutrients 8(1):11
Knäuper B, Rabiau M, Cohen O, Patriciu N (2004) Compensatory health beliefs: scale development and psychometric properties. Psychol Health 19(5):607–624
Miller W, Koceja D, Hamilton E (1997) A meta-analysis of the past 25 years of weight loss research using diet, exercise or diet plus exercise intervention. Internat J Obes 21(10):941–947
Baranowski T (2004) Why combine diet and physical activity in the same international research society? Int J Behav Nutr Phys Act 21(10):941–947
Chandrasekaran B, Ganesan TB (2021) Sedentarism and chronic disease risk in COVID 19 lockdown–a scoping review. Scott Med J 66(1):3–10
Sherar LB, Griffin TP, Ekelund U, Cooper AR, Esliger DW, van Sluijs EMF et al (2016) Association between maternal education and objectively measured physical activity and sedentary time in adolescents. J Epidemiol Commun Health 70(6):541–548
Ferrari G, Rezende LFM, Wagner GA, Florindo AA, Peres MFT (2020) Physical activity patterns in a representative sample of adolescents from the largest city in Latin America: a cross-sectional study in Sao Paulo. BMJ Open 10(9):e037290
Maric D, Kvesic I, Lujan IK, Bianco A, Zenic N, Separovic V et al (2020) Parental and familial factors influencing physical activity levels in early adolescence: a prospective study. Healthcare 8(4):532
Trigwell J, Murphy RC, Cable NT, Stratton G, Watson PM (2015) Parental views of children’s physical activity: a qualitative study with parents from multi-ethnic backgrounds living in England. BMC Public Health 15(1):1005
PNAD (2016) Pesquisa nacional por Amostra de Domicílios: Síntese de indicadores, 2015. IBGE
Acknowledgements
The authors would like to thank the Brazilian Ministry of Health, Brazilian Ministry of Education and the Brazilian Institute of Geography and Statistics who conducted the survey. The Coordination for the Improvement of Higher Education Personnel [CAPES, code 001] supported GTM with schoolership. And, the Foundation for Research Support of the State of Amazonas [FAPEAM] supported RMC with schoolership.
Funding
The PeNSE survey was funded by the Brazilian Ministry of Health, Brazilian Ministry of Education and the Brazilian Institute of Geography and Statistics.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This study was submitted and approved by the National Research Ethics Commission (CONEP) number 1.006.467/2015.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
de Mello, G.T., Silva, K.S., da Costa, R.M. et al. How physical activity, diet, and sedentary behavior cluster according to age in adolescents?. Sport Sci Health 18, 499–507 (2022). https://doi.org/10.1007/s11332-021-00830-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11332-021-00830-y