
Abstract
Objective
The purpose of this investigation was to assess the muscular strength of the knee extensors and flexors muscles, agility and functionality between dominant leg (DL) vs. non-dominant leg (NDL) of professional soccer players during pre-season.
Methods
Twenty-two healthy male professional soccer players (25.1 ± 3.8 years; 182.1 ± 5.9 cm; 79.3 ± 5.4 kg; body fat 14.6 ± 3.8%) from a club of the Brazilian second-division soccer league participated in this study. All soccer players underwent three tests to assess strength, power, and physical performance with an interval of 48 h inter-sessions. During the first assessment session, isokinetic tests were performed in which athletes performed maximal isokinetic concentric and eccentric contractions, as well as maximal isometric contractions. In the second and third assessment sessions, single leg step down and agility tests were performed, respectively.
Results
Maximum voluntary isometric contraction (MVIC) results showed a significant difference (p < 0.04) between DL compared to the NDL for absolute and relative values. But, the isokinetic variables of knee extensors at 60°/s (total work and power) were significantly higher (p < 0.03) in NDL. Pearson’s correlation was found to be significant between MVIC and single leg step down (SLSD) test for DL (r = 0.70, p = 0.0001) and NDL (r = 0.58; p = 0.002).
Conclusion
The results confirm that DL shows greater isometric strength than NDL. However, NDL revealed an increase in the total work and power output in professional soccer players. Furthermore, the SLSD test is recommended because it proved to be a good method for evaluating muscle strength by a positive correlation with MVIC.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Professional soccer season usually lasts from 10 to 11 months which the pre-season plays an important role in assessing, identifying injury risks, and planning training for the entire season. Pre-season is the period during a season with the highest training load for being relatively short (between 4 and 6 weeks) which is characterized by an increase of the physiological adaptation to training load and fitness level, but this improvement may not be sufficient to handle the intensity and stress associated with competitive soccer, leading to a higher risk of injuries [1, 2]. Some studies have shown that a pre-season with highest training load contributed to a lower in aerobic fitness, greater of muscle strains, especially in the thigh region and greater proportion of overuse injuries, including tendinitis and paratendinitis [1, 3,4,5]. Besides, it is important to verify whether pre-season matches are as competitive as in-season matches and whether friendly matches present higher injury risk than normal team-based training.
The substantial physiological demands, training intensity, and the body contact between players account for the generally high injury incidence in this sport and 70% of them occur in the lower limbs, even by the nature of the sport that requires movement of this body region [6,7,8]. Exercise-induced muscle damage is characterized by a temporary decrease in maximal force-generating capacity, impaired physical performance, an increase in intracellular proteins in the blood, muscle soreness, and swelling in and around the involved muscle groups [9, 10]. In this way, neuromuscular and functional assessment applied to soccer has allowed a better understanding of the physiological responses and injury prevention associated with training load during pre-season [1, 2, 8]. Hence, measurement of muscle strength, power output, agility, and functionality are crucial for providing information regarding the muscular condition in addition to functional capacity during pre-season [11]. These neuromuscular and functional information are important to understand the relationship of morphological and neural factors including muscle cross-sectional area and architecture, musculotendinous stiffness, motor unit recruitment, rate coding, motor unit synchronization, and neuromuscular inhibition. Such combinations of factors are associated with enhanced external mechanical power, general sports skill performance, decreased injury rates, and training load monitoring [12,13,14]. On the other hand, it is important to assessment between dominant leg (DL) vs. non-dominant leg (NDL) because soccer players may suffer imbalanced between DL and NDL as an effect of specific technical movements during matches and training, consequently, asymmetrical pattern may cause functional or even structural disproportionateness [15, 16].
The difference of strength between DL vs. NDL has been the topic of several studies that identified the bilateral asymmetry (BA) is detrimental to performance, increasing the risk of injury [15, 16]. Some studies report that BA higher than 10% results in a loss of muscle power, slower change of direction speed times, and increased risk of lower limb injuries [17, 18]. Further, soccer players with strength asymmetries > 15% are four-to-five times more likely to sustain a hamstring strain [19]. Therefore, the purposes of this study were to assess the muscular strength of the knee extensors and flexors, agility, and functionality between DL vs. NDL of professional soccer players during pre-season.
Methods
Participants
This study included 22 healthy male professional soccer players (age 25.1 ± 3.8 years; height 182.1 ± 5.9 cm; body mass 79.3 ± 5.4 kg; body fat 14.6 ± 3.8%) from a club in Brazil participating in second-division national competitions organized by the Brazilian Soccer Confederation. The participants’ training frequency was 6.1 ± 0.5 days/week, with a mean duration for each session training of 65 min, using training programs consisting of jumps, contesting possession, sprints, accelerations, and decelerations. All data collection was carried out at the beginning of training sessions during pre-season.
The participants were eligible if they had not been smorkers for the previous 3 months or more; had no cardiovascular or metabolic diseases, systemic hypertension (140/90 mm Hg or use of antihypertensive medication), recent musculoskeletal injury (in the last 6 months), or pain in any region of the body; and had not used anabolic steroids, drugs or any medication with the potential to impact physical performance (self-reported). This study was approved by the institutional Ethics Committee for Human Experiments (CAAE: 76189817.0.0000.5235) and was performed by national standards in sport and exercise science research. All participants signed the informed consent form.
Study design
This is a randomized comparative study. The sample size was determined by including all participants that complied with the eligibility criteria. All soccer players underwent three tests to assess strength, power, and physical performance with an interval of 48 h inter-sessions. During the first assessment session, isokinetic tests were performed in which athletes achieved maximal isokinetic concentric and eccentric contractions, as well as maximal isometric contractions on a Biodex isokinetic dynamometer (60°/s). In the second and third assessment sessions, single leg step down and agility tests were assessed on the same soccer field, respectively. The isokinetic and the single leg step down tests were taken in a temperature-controlled environment (temperature 21 °C, 65% relative humidity) by a Hygro-Thermometer with Humidity Alert (Extech Instruments, Massachusetts, EUA). All assessments occurred between 8:00 and 9:00 AM and were taken at the beginning of the pre-season.
Anthropometric measurements
Body composition was measured following an 8-h overnight fast by bioelectrical impedance analysis using a device with built-in hand and foot electrodes (BIO 720, Avanutri, Rio de Janeiro, Brasil). The participants wore their normal indoor clothing and were instructed to stand barefoot in an upright position with both feet on separate electrodes on the device’s surface and with their arms abducted and both hands gripping two separate electrodes on each handle of the device [8, 14]. All biometric measurements were carried out in an air-conditioned room (21 °C). No clinical problems occurred during the study.
Isokinetic and isometric testing
Assessments were made on an isokinetic dynamometer (Biodex System 4, Biodex Corporation, Shirley, NY, USA) was used to measure peak torque values, torque angle, total work, hamstring/quadriceps ratio (H/Q ratio) and maximum voluntary isometric contractions (MVIC). Before the isokinetic test, all soccer players performed a warm-up exercise for 10 min on stationary cycling (no resistance) with moderate velocity (70–80 rounds per minute). The measurements for the knee flexion and extension were carried out in a sitting position. The soccer players sat on the dynamometer chair with their torsos positioned at 85° with the motor axis aligned to the knee joint axis. The motor axis was visually aligned with the axis of the knee. All athletes were also stabilized with belts around the torso, pelvis, and thigh to avoid compensatory movements. Thus, only the knee to be tested was moving with a single degree of freedom. The knee extensors and flexors in the dominant (DL) and non-dominant leg (NDL) were tested concentrically. Isokinetic tests were carried out by random sampling. Athletes were instructed to push the lever up, and pull it down, as hard and fast as possible with extension undertaken first for concentric contractions. On the other hand, during eccentric contractions, athletes were instructed to resist the lever arm with extension as the first movement [16].
All athletes performed five continuous maximum effort concentric contractions of the knee flexors and extensors for both legs in random order at the angular velocity of 60°/s [16]. All evaluations were carried out by the same investigator and a variation coefficient below 10% was employed to estimate whether trials were valid. Peak torque was normalized and expressed relative to body mass. The difference between DL and NDL peak torque of the flexors and extensors was analyzed. The H/Q ratio was taken from the ratio of peak torque between the knee flexors and extensors at 60°/s. Maximum voluntary isometric contractions (MVIC) were conducted in the same equipment and positioning, where individuals were instructed to sustain 5-s maximal isometric contractions at a fixed knee joint position at 70°. All tests (i.e., concentric contractions of the knee flexors and extensors and isometric test, respectively) used a 5-min recovery between them. All participants were strongly encouraged to give a maximal effort for each action.
Agility test
The protocol of the agility test consisted of four sprints (right = two sprints; left = two sprints) with 2-min rest between each one of them. The athletes, wearing footwear, started 30 cm behind the photocell beam (Brower Timing System, Salt Lake City, 174 UT, USA; accuracy of 0.01 s) and sprinted 10 m forward making a change of direction at the first point (Fig. 1). The athletes sprinted more 5 m making a second change of direction on the perpendicular and from the third point, making a new change of direction to accelerate in a straight line for 15 m over the initial start line to complete the run (Fig. 1) [11, 18]. The fastest times were recorded by photocell beam for data analysis. Verbal encouragement was always provided, and no one was excluded through injury during the experimental procedure. This test is valid when it exhibits reliability that is higher than 0.90.

Schematic image of the agility test
Single leg step down test (SLSD test)
SLSD test started with individuals stood on an 8-inch wooden box, assuming a single-limb stance, hands in the hip and performing a squat that required the heel of the free leg to make contact with a scale on the floor to confirm a successful trial. They were required to make contact with the scale but not exceed 10% of body weight to prevent weight transfer off of the test limb. Upon contacting the scale, they returned to the starting position. Individuals were asked to complete as many step-downs as possible in 60 s. Step-downs were not counted if the person did not make contact with the scale, transferred > 10% of body weight onto their free limb when contacting the scale, or did not fully return to the starting position [20].
Statistical analysis
All data are presented as mean ± SD. Statistical analysis was initially performed using the Shapiro–Wilk normality test and the homocedasticity test (Bartlett criterion). Student’s t test was used to assess differences between neuromuscular and performance response (dominant leg—DL vs. non-dominant leg—NDL). The effect size (ES) of the difference between DL and NDL was assessed using Cohen’s d [21]. Values of d < 0.1, from 0.1 to < 0.20, from 0.20 to < 0.50, from 0.50 to < 0.80, and ≥ 0.80 were considered as trivial, small, moderate, large and very large, respectively. Correlations between variables were assessed using Pearson correlation coefficients and their corresponding 95% confidence intervals. The significance level was set at 0.05 and the software used for statistics was GraphPad® (Prism 6.0, San Diego, CA, USA).
Results
Table 1 represents the values of MVIC between DL vs. NDL. Statistical results showed a significant difference between DL compared to the NDL for absolute and relative values (∆% = 4.6%).
Table 2 compares the isokinetic variables of knee extensors at 60°/s between NDL vs. DL. Student’s t test showed no significant difference between NDL vs. DL concerning values of absolute and relative in peak torque. On the other hand, the variable work and power (absolute and relative repetitions) were significantly higher (p < 0.03) in NDL when compared to DL (Table 2). In contrast, none of the isokinetic variables related to knee flexors at 60°/s showed a significant difference between DL vs. NDL (p > 0.05) (Table 3). It is worth mentioning that the magnitude of the effect showed results between trivial and moderate, except for the relative power of the knee extensors. The H/Q ratio showed no significant difference in relation to peak torque values (DL = 0.69 ± 0.1 vs. NDL = 0.64 ± 0.1; ∆% = 11%; p = 0.13).
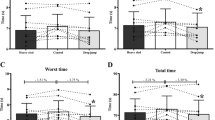
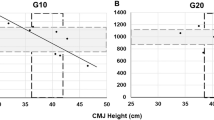
Table 4 showed no significant difference between DL vs. NDL for the agility test, (speeds in m/s and km/h) and SLSD test. Pearson's correlation was found to be significant between MVIC and the number of repetitions for DL (r = 0.70, p = 0.0001) and NDL (r = 0.58; p = 0.002) during the SLSD test (Fig. 2a, b).

Scatter plots show the correlation (Pearson’s coefficient) between MVIC and the number of repetitions during single leg step down test (SLSD) for NDL and DL
Discussion
This study aimed to assess the neuromuscular and functional responses of professional soccer players during pre-season. The main results obtained with this study were that (a) DL was greater when compared NDL during the evaluation of the MVIC, (b) NDL revealed a significant increase in total work and muscle power of knee extensors (absolute and relative values), and (c) a correlation between was found between SLSD test and MVIC for DL and NDL.
Quantification of muscle strength is an essential component of the neuromuscular assessment in athletes, being an important component of fitness for successful soccer play [12,13,14]. The neuromuscular assessments in professional soccer players have been mostly based on maximal strength assessed under non-fatigued and shorter muscle lengths [8, 22]. Some studies showed a difference of 6.8–7.8% between DL in relation to NDL during MVIC test in non-athletes individuals [23, 24]. On the other hand, our findings showed a significant difference of 4.6% between DL vs. NDL during the MVIC test. Corroborating with our results, a study observed that young soccer players showed a 5.2% increase in the MVIC in DL when compared to NDL [25]. However, the difference of maximal strength values between DL and NDL measured by MVIC remains unknown and without reference values in professional soccer players during pre-season. Despite our results showing a BA < 10%, it is important to mention that muscle injury frequency caused by strength asymmetry is significantly increased for unbalanced soccer players up to 16%; compared to 4% for balanced players [19].
The total work is defined as the energy developed by the muscle (action of a force) through a specified distance in space (product of the torque during all its displacement angular) [26]. The lower the angular speed, the greater the work. Although some studies show a bilateral difference in knee flexors, our findings showed that total work (absolute and relative values) were significantly higher in NDL when compared to DL during knee extension. On the other hand, our examined soccer players, with an angular velocity of 60°/s, the average bilateral relationship was 8.8 ± 6.3%, but bilateral asymmetry (≥ 10%) in pre-season testing was lower than 10%. Consequently, total work for providing information in terms of the muscle ability to generate strength over a longer time leads us to understand that this difference at 60°/s represents a lower risk of injury when compared to higher velocities because the majority of muscle injuries occur during higher velocity movements [16, 27]. It is worth mentioning that despite the bilateral difference being < 10% in 60°/s, this fact does not exclude the need to conduct individual evaluations to identify this potential injury risk factor. Concerning power, this variable is characterized by the pattern of realized total work divided by contraction time. Hence, the angular velocity is directly proportional to the power in which the greater the angular velocity, the greater the power [26]. Following the results of the total work, the power values (absolute and relative) were significantly higher in NDL when compared to DL during knee extension. However, the lower extremity muscle power bilateral difference was less than 15% (10.8 ± 7.5%). But, despite the bilateral difference being < 15% in 60°/s, it becomes irresponsible to allow an athlete to maintain their training, and competitions with an inadequate functional power favor the predisposition of muscle injury and/or submaximal performance [17, 19]. In general, these results make us believe that the bilateral difference found in the total work and power for the knee extensors muscle can be explained by the specific motor demands during the soccer activity; i.e. while the dominant leg exerts its specific action, the non-dominant leg remains active, providing postural (stabilizing) support [16, 27, 28]. In particular, the dominant leg kicks while the non-dominant leg actively contributes with the knee and hip flexion and extension are required to support the individual’s weight [27]. Also, it is important to mention that the performance of power on an isokinetic dynamometer may be quantitatively accurate and reliable; however, it does not necessarily insinuate adequate functionality during activity.
SLSD test has been commonly used for evaluations of neuromuscular control, screening for injury prevention, appraising athletic injuries, functionality, and endurance of the lower limb for involving repetitive eccentric and concentric contractions of the quadriceps [20, 29, 30]. However, we found no studies that correlated the performance during SLSDs tests and muscle strength between DL and NDL in professional soccer players. Our results showed a positive correlation between the performance during SLSDs tests and MVIC. Some studies observed a vastus medialis activity equal to 27 ± 12% MVIC and a vastus lateralis activity of 32 ± 3% MVIC during SLSDs tests [29, 31]. During the SLSD test occurs an eccentric contraction of the quadriceps demanding greater vastus medialis activity for control the excursion of the body’s center of mass over a single leg [29]. However, it has been observed that concentric contractions produce greater activity than eccentric contractions for both the vastus lateralis and the vastus medialis during the SLSD test [31]. Thus, it is suggested that the number of motor units and frequency of activation of those motor units is less for eccentric contraction than for concentric contraction [32, 33]. This result is mainly attributed to economical tension development which might be a result of better utilization of elastic energy it takes to step up against gravity (concentric phase) [31]. In addition, it is important to mention that the hip abductor muscles contribute to a pelvis and lower limb stability by eccentric control during weight-bearing activities [30, 34]. On the other hand, significant strength deficits during the SLSD test contribute with a lower extremity kinematic pattern consisting of hip adduction, internal rotation, and knee valgus. Consequently, it has been proposed that strength deficits and biomechanics changes increase the risk factor for patellofemoral pain syndrome, iliotibial band friction syndrome and anterior cruciate ligament injury [12, 20, 34, 35]. Thus, the SLSD test may be a simple/economic method in clinical practice for evaluating muscle strength for presenting a positive correlation with MVIC.
The limitation of the study is the absence of measures of physiological parameters of physical exertion, which would be interesting; this yet does not affect the answer to the study question. However, our sample was homogeneous although longitudinal studies are needed to define a cause-and-effect relationship among training sessions, strength muscle, physiological adaptations, and bilateral deficit in professional soccer players.
Conclusion
The results of this investigation confirm that DL shows greater isometric strength than NDL. On the hand other, NDL revealed an increase in the total work and power output in professional soccer players. Furthermore, the use of the SLSD test is recommended because it proved to be a good method for evaluating muscle strength by a positive correlation with MVIC. Thus, these assessments may be a helpful for coaches, physicians and physical therapists regarding neuromuscular performance, injury prevention and recovery strategies.
References
Eliakim E, Doron O, Meckel Y, Nemet D et al (2018) Pre-season fitness level and injury rate in professional soccer–a prospective study. Sports Med Int Open 2:E84–E90
Coppalle S, Rave G, Abderrahman AB et al (2019) Relationship of pre-season training load with in-season biochemical markers, injuries and performance in professional soccer players. Front Physiol 10:409
Salces JN, Gómez-Carmona PM, Moliner-Urdiales D et al (2014) An examination of injuries in Spanish professional soccer league. J Sports Med Phys Fitness 54:765–771
Brito J, Rebelo A, Soares JM et al (2011) Injuries in youth soccer during the preseason. Clin J Sport Med 21:259–260
Hawkins RD, Hulse MA, Wilkinson C et al (2001) The association football medical research programme: an audit of injuries in professional football. Br J Sports Med 35:43–47
Maior AS, Leporace G, Tannure M et al (2017) Profile of infrared thermography in professional soccer players. Motriz Rev Educ Fis 23:1–6
Maior AS, Viana J, Hall E et al (2018) Correlation between match efforts and serum creatine kinase level: implications for injury prevention in professional soccer players. JEPonline 21:109–120
Matta L, Rhea M, Maior AS (2019) Physiological evaluation post-match as implications to prevent injury in professional soccer players. Arch Med Deporte 36:138–144
Maior AS, Tannure M, Eiras F et al (2020) Effects of intermittent negative pressure and active recovery therapies in the post-match period in professional soccer players: a randomized, parallel arm, comparative study. Biomed Hum Kinet 12:59–68
Jones CM, Griffiths PC, Mellalieu SD (2017) Training load and fatigue marker associations with injury and illness: a systematic review of longitudinal studies. Sports Med 47:943–974
Meckel Y, Doron O, Eliakim E et al (2018) Seasonal variations in physical fitness and performance indices of professional soccer players. Sports (Basel) 6:14
Suchomel TJ, Nimphius S, Stone MH (2016) The importance of muscular strength in athletic performance. Sports Med 46:1419–1449
Cormie P, McGuigan MR, Newton RU (2011) Developing maximal neuromuscular power: part 1—biological basis of maximal power production. Sports Med 41:17–38
Maior AS (2020) Absolute and relative peak power during pneumatic squat exercise using different percentages of load in professional soccer players. Hum Mov 21:64–70
Gkrilias P, Zavvos A, Fousekis K et al (2018) Dynamic balance asymmetries in pre-season injury-prevention screening in healthy young soccer players using the modified star excursion balance test-a pilot study. J Phys Ther Sci 30:1141–1144
Bonetti LV, Floriano LL, dos Santos TA et al (2017) Isokinetic performance of knee extensors and flexors in adolescent male soccer athletes. Sport Sci Health 13:315–321
Bell DR, Sanfilippo JL, Binkley N et al (2014) Lean mass asymmetry influences force and power asymmetry during jumping in collegiate athletes. J Strength Cond Res 28:884–891
Hoffman JR, Ratamess NA, Klatt M et al (2007) Do bilateral power deficits influence direction-specific movement patterns? Res Sports Med 15:1–8
Croisier JL, Ganteaume S, Binet J (2008) Strength imbalances and prevention of hamstring injury in professional soccer players: a prospective study. Am J Sports Med 36:1469–1475
Kline PW, Johnson DL, Ireland ML et al (2016) Clinical predictors of knee mechanics at return to sport after ACL reconstruction. Med Sci Sports Exerc 48:790–795
Cohen J (1988) Statistical power analysis for the behavioural sciences, vol 88. L. Erbraum Associates, Hillside, NJ, pp 23–97
Grazioli R, Lopez P, Andersen LL et al (2019) Hamstring rate of torque development is more affected than maximal voluntary contraction after a professional soccer match. Eur J Sport Sci 19:1336–1341
Meldrum D, Cahalane E, Conroy R et al (2007) Maximum voluntary isometric contraction: reference values and clinical application. Amyotrop Lateral Scler 8:47–55
Courel-Ibáñez J, Hernández-Belmonte A, Cava-Martínez A et al (2020) Familiarization and reliability of the isometric knee extension test for rapid force production assessment. Appl Sci 10:4499
Rouissi M, Chtara M, Owen A et al (2016) Effect of leg dominance on change of direction ability amongst young professional soccer players. J Sports Sci 34:542–548
Kannus P (1994) Isokinetic evaluation of muscular performance: implications for muscle testing and rehabilitation. Int J Sports Med 1:S11–S18
Greig M (2008) The influence of soccer-specific fatigue on peak isokinetic torque production of the knee flexors and extensors. Am J Sports Med 36:1403–1409
Vaisman A, Guiloff R, Rojas J et al (2017) Lower limb symmetry: comparison of muscular power between dominant and nondominant legs in healthy young adults associated with single-leg-dominant sports. Orthop J Sports Med 5:2325967117744240
Bolgla LA, Shaffer SW, Malone TR (2008) Vastus medialis activation during knee extension exercises: evidence for exercise prescription. J Sport Rehabil 17:1–10
Park KM, Cynn HS, Choung SD (2013) Musculoskeletal predictors of movement quality for the forward step-down test in asymptomatic women. J Orthop Sports Phys Ther 43:504–510
Selseth A, Dayton M, Cordova ML et al (2000) Quadriceps concentric EMG activity is greater than eccentric EMG activity during the lateral step-up exercise. J Sport Rehabil 9:124–134
Moritani T, Muramatsu S, Muro M (1988) Activity of motor units during concentric and eccentric contractions. Am J Phys Med Rehabil 66:338–350
Howell JN, Fuglevand AJ, Walsh ML et al (1995) Motor unit activity during isometric and concentric-eccentric contractions of the human first dorsal interosseus muscle. J Neurophysiol 74:901–904
Ireland ML, Willson JD, Ballantyne BT et al (2003) Hip strength in females with and without patellofemoral pain. J Orthop Sports Phys Ther 33:671–676
Eitzen I, Holm I, Risberg MA (2009) Preoperative quadriceps strength is a significant predictor of knee function two years after anterior cruciate ligament reconstruction. Br J Sports Med 43:371–376
Acknowledgements
The investigator would like to thank the 22 healthy male professional soccer players from a club in the Brazilian second-division that participates in national competitions organized by the Brazilian Soccer Confederation. The study was supported by the Coordenação de Aperfeicoamento de Pessoal de Nivel Superior, Brazil (CAPES), Finance Code 001.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors state no conflict of interest.
Ethical approval
This study was approved by the institutional Ethics Committee for Human Experiments (CAAE: 76189817.0.0000.5235) and was performed by national standards in sport and exercise science research.
Informed consent
All participants signed the informed consent form.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Maior, A.S., Lopes, R.T. Neuromuscular and functional responses in professional soccer players during pre-season: implications for injury prevention. Sport Sci Health 17, 1017–1024 (2021). https://doi.org/10.1007/s11332-021-00769-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11332-021-00769-0