
Abstract
Purpose
To verify if pre-performance vibration exposure could negatively affect the postural control in soccer players.
Methods
Twenty-eight participants, 12 male soccer players (aged 22.4 ± 1.0 years) and 16 sedentary males (aged 26.8 ± 2.7 years), underwent two test sessions: in the first one, the optimal vibration frequency (OVF) was determined for each participant, and in the second one, postural sways, with open and closed eyes, were assessed at baseline, immediately, 10, 20 min after the WBV exposure. The vibration exposure consisted in five sets of 1 min each one, at OVF, with 1-min rest between each set.
Results
The elliptical area, containing the 95% of the centre of pressure (COP), displacements (AREA), the total linear distance covered by the COP (LENGTH), the average distance between the assessed COP position and the ideal COP position (AV-DIST) and variance of speed of the COP displacements (VAR-SPEED), have been analysed. RM-ANOVA did not show significant differences among the times of assessment. Significant differences in all the dependent variables, between the groups, especially in closed eyes condition, were found. Athletes with closed eyes showed a significantly smaller COP AREA (p = 0.00004), minor AV-DIST (p = 0.0001), which are good indicators of an optimal postural control.
Conclusion
An acute bout of WBV at the OVF did not modify the COP parameters and may be used before the performance, with no side effect on balance. Athletes have developed a postural strategy on non-visual afferent inputs that could be enhanced by the WBV chronic exposure.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Vibration is a mechanical stimulus characterized by an oscillatory motion, and the biomechanical parameters, determining its intensity, are the amplitude, frequency, and magnitude of the oscillations [1]. The whole body vibration (WBV) frequency plays an important role in the effectiveness of neuromuscular activation [2, 3]. The ideal combination frequency–amplitude, ranged between 10 and 50 Hz, with peak-to-peak amplitudes of 0.5 mm and 1.5 mm being used to stimulate the postural control [4]. Nevertheless, the optimal WBV frequency may differ from individual to individual; therefore, the WBV frequency should be determined for each subject to obtain the maximal EMG muscle response [5]. The vibration represents a strong stimulus for musculoskeletal structures, due to the need to quickly modulate muscle stiffness to react to the vibratory waves [6]. This response is mediated by monosynaptic and polysynaptic afferent pathways [7] that increase muscle spindle activation. This activation leads to a facilitation of stretch reflex [1], improving motor units’ recruitment [8], and triggering specific hormonal responses [9]. Consequently, vibration could represent an effective exercise intervention for enhancing neuromuscular performance in athletes [10]. Nevertheless, the WBV acute effect may impair the postural control of the exposed subject. Balance has been shown to play a fundamental role in many athletic activities and may contribute to a successful performance [11], although the relationship between balance ability and athletic performance needs to be investigated [12]. Factors that improve postural control responses are the strength [13], the coordination [14], and the sensory information, obtained from the somatosensory, visual, and vestibular systems [15]. WBV is used as a modality of warm-up, immediately before training and competition, as it improves speed and explosive power in soccer [7], due to a possible contribution of post-activation potentiation [16]. Moreover, WBV enhances the short latency stretch reflex response of the stretch shortening cycle [17] and the ankle stability [18]. Furthermore, WBV elicits all these positive responses in a relatively short time frame [19]. It has reported a decrement in the physical performance of soccer players during the initial phase of the second half of competitive match play. [20]. The reason for this reduced physical performance after the half-time interval has been suggested to be a consequence of a lack of preparation for the second half [21, 22], due to the inconsistent pre-match warm-up before the start of the game. Performing WBV exercises in the dressing room may be more acceptable to coaches. A short-duration, low-intensity and practical dose of WBV is ergogenic for sprint and power performance maintaining eccentric hamstring peak torque, potentially reducing the risk of injury [22]. Consequently, it is essential to assess whether an acute exposure to WBV may alter balance and postural control, if applied immediately before a sport performance [23, 24]. Acute exposures to vibration have been shown to influence the motor unit recruitment, activating more motoneurons than the need [25].
Considering the contribution of the proprioceptive sensory system, in particular of feet cutaneous mechanoreceptors, to coordinate lower limb movements, gait, and balance [26], Schlee et al. [27] have shown in healthy subjects, significant improvements on balance after single session of 4-min WBV exposure, despite the decreased foot sensitivity thresholds detected at all analysed anatomical locations. Other investigations have been carried out on effects of WBV training on postural balance, especially with chronic modality, in either healthy individuals [28] or ACL reconstructed athletes [29]. These studies present conflicting results, with some supporting its positive effects [28] and other showing no changes [29, 30]. The improvements in balance and movement control reported after WBV training are likely to have a neuromuscular mechanism caused by tonic vibration reflex and a consequent more efficient use of the reflex pathways rather than be related to improvements in foot sensitivity. Recent evidence suggested that the central processing of proprioceptive information from the foot was essential of centre of pressure (COP) parameters’ control [31]. During stance, somato-sensation from the ankles and feet has been shown to contribute to standing postural stability [32]. As suggested by Kavounoudias et al. [33], the ankle joint muscles and the plantar sole afferents are complementary signals to guarantee effective postural control [34]. It is basically established that human standing posture is guaranteed by a central postural programme supported by several sensory sources feedback (i.e. labyrinthine, visual, muscular and cutaneous input) that together contribute to the overall postural control.
The aim of this study is to assess the effects of short time WBV protocol on COP parameters in soccer players and healthy subjects, analysing the different postural adaptation strategies with open and closed eyes. It was hypothesized that the acute effect of a bout of WBV may temporarily impair the COP stability both in athletes and sedentary participants, so in that case, the second aim of the study is to evaluate the impairment duration.
Methods
Participants
Twenty-eight participants volunteered for the study: 12 male soccer players (experimental group; EG) and 16 healthy males that did not practiced any type of sport or physical activity (control groups; CG). The EG had the following characteristics: age 22.4 ± 1.0 years old, height 1.82 ± 0.87 m, body mass 74.7 ± 10.6 kg, and a training background of 5.00 ± 1.16 years, with at least three training sessions per week. The participants of EG competed in the Italian National Championship for Amateur players that is the most important level of competition of amateur soccer. On the contrary, the CG had the following characteristics: age 26.8 ± 2.7 years, height 1.73 ± 0.81 m, and body mass 85.02 ± 14.9 kg. The following exclusion criteria were applied: significant health problems; muscular, neurological and tendon injuries, or osteoarticular disease or injury; use of medicine influencing balance; presence of disease or other conditions influencing balance; significant postural problems/limitations. Participants of both groups had regular sleeping schedules and were requested to maintain their habitual behaviours, avoiding strenuous activity during the testing period. After being informed of the procedures of the study, written informed consent was obtained from all individual participants included in the study. This study, designed and conducted according to the ethical principles of the 2008 Declaration of Helsinki, was approved by the local Ethics Committee.
Study design
This study is an interventional trial in which the acute and short-term effects of the WBV on balance were investigated. All participants underwent two sessions of tests, separated by 1 week to limit the effect of vibration exposure between sessions.
During the first session, the optimal vibration frequency (OVF) was determined for each participant [5]. This session gave the participants the time to fully familiarize with the equipment used in the study and with the procedures proposed in the second session.
In the second session, postural sways with open and closed eyes were assessed before and after the WBV exposure at the OVF. Postural sways were assessed at baseline (before the WBV), immediately after WBV exposure and again after 10 and 20 min.
Procedures
All the evaluations of the study were carried out in the laboratory of the University of “Foro Italico”. The participants underwent a vibration exposure using a WBV platform. The vibration exposure consisted in five sets of 1 min each of vibration at the OVF, with 1-min rest in sitting position for a total of 9 min of intervention (see Fig. 1).

Graphical rappresentation of experimental intervention
The vibrating platform used in this study was the Double Vibe (Bosco System Technologies, Rieti, Italy) that is composed by a steel and aluminium structure, with a 60 × 60 × 21 cm platform. WBV platform generates vertical oscillations with a frequency from 20 to 55 Hz, with a payload from 40 to 140 kg. The amplitude ranges are from two to four mm, and the acceleration resulting in gravitational forces ranges from 2.3 to 5.9 g, where g indicates the standard acceleration due to gravity (1 g = 9.81 m/s2). During the vibration exposure, the participants had to maintain a static half-squat position, with the heels lifted slightly off the ground, with an angle of 90 degrees at the ankle joint, 120 degrees at the knee joint and 140 degrees at the hip joint [35]. The correct joint angle was ascertained using a goniometer. Before starting the experimental sessions, the participants were instructed to stand as still as possible, limiting the possible oscillations of the trunk and avoiding voluntary contraction of the muscles in the lower limbs during vibration [35]. During the vibration exposure, the subjects wore only socks. The position on platform is shown in Fig. 2.

Correct position kept by participant during Whole Body Vibration exposure
The OVF of each participant was assessed as described below: surface electromyography (sEMG) was recorded, for each participant, on the vastus lateralis, of the dominant lower limb, during the execution of the vibration protocol. The sEMG was performed with the MuscleLab (Bosco System Technologies, Rieti, Italy). The initial vibration frequency was 20 Hz for 5 s, with an increment of 5 Hz every 5 s up to 50 Hz. The vibration frequency, with the Maximal sEMG activation (RMSmax), was considered as OVF. When the muscle OVF was different, the RMSmax of the vastus lateralis muscle frequency was considered. In all participants, the OVF was identified as the WBV frequency with the highest normalized RMS values for each limb. Median value of OVF was 35 Hz (interquartile range 30–40 Hz); the peak-to peak displacement of the vibrating platform was set on 3.2 mm, with a consequent acceleration of 4.5 g (44.13 m/s2) according to the manufactory instructions.
The balance was evaluated using the Zebris FDM-S multifunction plate system (Zebris Medical GmbH, Isny, Germany). This platform works with 2560 sensors on a surface of 33.9 × 54.2 cm (that is 1.4 sensor/cm2) at a sampling frequency of 120 Hz. Using the real-time monitoring of the centre of pressure (COP) of the body in static position for 52 s of assessments, the software of the Zebris FDM-S provided different indexes. In the present study, the following indexes were considered: the elliptical area containing the 95% of the COP, traced during the 52 s of assessment (AREA; in mm2), total linear distance covered by the COP (LENGTH; in mm), the average distance between the assessed COP position and the ideal COP position (AV-DIST; in mm), and variance of speed of the COP displacement (VAR-SPEED; in mm2/s2). The assessment of the balance was performed at baseline (T0) and after the vibration exposure. In particular, the post-vibration assessments were performed immediately after the vibration exposure (T1), and after 10 min (T10), and 20 min (T20). The balance assessment lasted 2 min in which static balance sways with open and closed eyes were, respectively, assessed (52 s of assessments each) [36]. Balance assessment was performed using bipedal static COP measures because previous studies showed that this assessment is a reliable tool for investigating general postural stability and balance performance under specific conditions [37].
Statistical analysis
Repeated measures analysis of variance (RM-ANOVA) was performed separately for the balance parameters assessed using the Zebris FDM-S (AREA, LENGTH, AV-DIST; VAR-SPEED) in order to find significant differences between the two groups (EG and CG), between the open and closed eyes conditions and among the different times of evaluation. The assumptions to perform RM-ANOVA were assessed using Mauchly’s test of sphericity and Shapiro–Wilk’s test for normality. The RM-ANOVA was performed using the experimental and control groups with open and closed eyes, respectively, as four independent groups: EG with open eyes (EGo), EG with closed eyes (EGc), CG with open eyes (CGo), and CG with closed eyes (CGc). These four groups represented the between factor of the analysis (EGo vs. EGc vs. CGo vs. CGc). The different times of assessments represented the within factor of the analysis (T0 vs. T1 vs. T10 vs. T20). The assumptions to perform RM-ANOVA were assessed using Mauchly’s test of sphericity and Shapiro–Wilk’s test for normality.
Bonferroni post hoc was used for pairwise comparison when a significant p value was detected for all the analyses. The alpha test level for statistical significance was set at 0.05. Effect size was calculated as partial eta squared (η2p). For all the statistical analyses, the SPSS statistical package software was used (IBM, v.20.0, Chicago, IL, USA).
Results
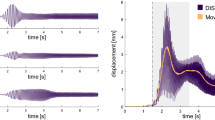
Shapiro–Wilk’s test showed a normal distribution of the data, whereas the Mauchly’s test showed that the assumption of sphericity was violated. Consequently, the Greenhouse–Geisser’s correction was applied due to the lack of sphericity. Data are reported as mean ± standard error of the mean (SEM). Concerning the differences among the groups, the RM-ANOVA analyses showed significant differences in all the four dependent variables: AREA (F3,52 = 9.619; p = 0.00004; η2p = 0.357), LENGHT (F3,52 = 5.856; p = 0.002; η2p = 0.253), AV-DIST (F3,52 = 8.856; p = 0.0001; η2p = 0.338), and VAR-SPEED (F3,52 = 5.206; p = 0.003; η2p = 0.231). Conversely, the RM-ANOVA analyses did not show any significant difference among the times of assessment in the four analysed variables: AREA (F2.2,113 = 2.464; p = 0.085; η2p = 0.045), LENGHT (F2.4,123 = 2.032; p = 0.127; η2p = 0.038), AV-DIST (F2.1,107 = 2.488; p = 0.086; η2p = 0.046), and VAR-SPEED (F1.4,71 = 3.132; p = 0.068; η2p = 0.057). Finally, significant interaction Time * Groups were found in LENGHT (F7.1,123 = 4.220; p = 0.0003; η2p = 0.196), but not in the other variables that were AREA (F6.5,113 = 1.491; p = 0.182; η2p = 0.079), AV-DIST (F6.2,107 = 1.394; p = 0.222; η2p = 0.074), and VAR-SPEED (F4.1,71 = 2.319; p = 0.064; η2p = 0.118). Due to the presence of significant interaction, one-way RM-ANOVA was performed for the 4 groups independently for the LENGTH variable, and significant results over time were found for CGo (F1.7,26 = 4.135; p = 0.032; η2p = 0.216) and CGc (F1.8,26.8 = 7.260; p = 0.004; η2p = 0.326), whereas no differences were found for EGo and EGc. Pairwise comparisons results are reported in Table 1. The average scores with the relative standard error of means (SEM) of the groups in each analysed parameter and the results of the post hoc analyses are reported in Table 1 and Fig. 3.

Results concerning the LENGTH variable
Discussion
The current study aimed to verify whether vibration exposure could negatively affect postural control and balance in soccer players. The main finding of the study was that an acute bout of WBV, at the OVF, did not modify the COP parameters in soccer players and non-athletes, both in open and closed eyes conditions. The evaluation of parameters, describing COP excursions, is a frequently used method to measure stability and any associated pathological mechanism [38]. It was expected that vibration, as a stimulus that interferes with postural control, could affect COP stability, altering the neuromuscular stability, due to a strong inhibition of spinal reflex and an altered plantar foot sensitivity [27]. This effect could get worse following soccer performance. In our study, neither positive nor negative effects were assessed after the WBV exposure [11, 29, 39].
Previous studies on the acute effects of WBV showed conflicting results. Padulo et al. [40] found that an acute bout of WBV, both at low and high intensity vibrations, altered the neuromuscular balance, due to a strong inhibition of spinal reflex and an altered plantar foot sensitivity. Nevertheless, WBV perturbation reduces, immediately afterwards, the recruitment thresholds and simultaneously elicit the tonic vibration reflex (TVR), counterbalancing the initial perturbation. It has been demonstrated that the main mechanism in improving balance and postural control after acute bout of WBV is the TVR and the consequent more efficient use of the reflex pathway [27]. Cloak et al. [41] found that an acute WBV bout significantly improved the dynamic postural stability only in elite soccer players, whereas no changes were observed among amateur soccer players. It is possible that elite athletes take better advantage of the reduced recruitment thresholds of fast-twitch fibres and the augmented joint stiffness, which guarantees ankle and knee joint stability than amateur [42, 43].
In contrast, Sanudo et al. [44] identified an improvement in amateur athlete balance after an acute WBV exposure. These conflicting results could be attributable to the nature of the participants’ training that could influence the postural responses but mainly to the different vibration frequency chosen (> 40 Hz) for the WBV protocols. To solve this problem, in the present study, the OVF of an acute exposure WBV was calculated, with the hypothesis that an individualized vibration frequency would be more effective than a fixed vibration frequency.
Significant differences between soccer players and control group were found especially in closed eye condition. Giagazoglou et al. [45] found that COP displacements significantly increased when visual information was absent. When the athletes performed balance with closed eyes, they were significantly better than the control group in overall parameters considered. Moreover, athletes with closed eyes showed a significantly smaller AREA and minor AV-DIST than controls with open eyes. These parameters are good indicators of an optimal postural control [38], especially the AV-DIST parameter which indicates the average distance between the assessed COP position and the ideal COP position, in stance. The soccer players could have developed a postural strategy on non-visual afferent inputs, in closed eye condition. These results highlighted that athletes based their postural control on the vestibular and proprioceptive systems, whereas the role of visual system in postural control is limited. Moreover, the soccer players have strongly developed lower limb strength, proprioceptive sensitivity, and joint stiffness, which guarantees ankle and knee joint stability that highly improves balance [42, 43]. Han et al. [46] found a high correlation between ankle proprioception scores and performance in soccer. The central processing of proprioceptive information from the foot was essential for balance control [31]. In fact, as mentioned previously, the somato-sensation from the ankles and feet contribute to standing postural stability [32], whereas the ankle joint muscles and the plantar sole afferents are complementary signals to guarantee effective postural control [33, 47]. The results of this study confirmed the efficacy of this kind of control also after the WBV exposure. The variability in overall COP parameters, shown by a high standard deviation, confirmed the individual organization of postural control adjustments. The high variability among subjects, in overall groups, may be attributable to the illusory perception of loss in postural stability due to the plantar surface vibration, rather than a postural instability per sè [1].
This study presents, however, some limitations that need to be addressed. The sham condition in which the subjects were in the squat position with the vibration platform in off is missing in this study. No EMG analysis was carried out during the strength evaluation of hip and ankle muscles. Further randomized controlled studies are needed to address these factors. Finally no test–retest of the postural assessment was performed.
Conclusions
This study demonstrated that an acute WBV session did not alter COP stability both in athletes and sedentary subjects. The finding that no adverse effects occurred, after the vibration exposure, suggests that WBV may be a safe application before soccer performance. WBV, as warm-up method, may sufficiently prepare the athletes, without fatiguing, increasing muscle temperature, and reducing the pain sensation of working muscles [48]. The experienced soccer players show greater neuromuscular characteristics of COP parameters probably due to their major rate of strength, motor unit firing rate, and tendon stiffness than non-athletes [22, 48, 49]. Only occasionally skilled athletes use sensory checking such as visual control for successful execution of their sport performance. This strategy allows them to devote more attention to tasks, such as locating the other players and determining the best opportunity to shoot the ball. Proprioception is the source for a good COP stability and for the automatic organization of precise and coordinated movements in competitive sports.
References
Cardinale M, Lim J (2003) Electromyography activity of vastus lateralis muscle during whole-body vibrations of different frequencies. J Strength Cond Res 17:621–624. https://doi.org/10.1519/1533-4287
Ritzmann R, Gollhofer A, Kramer A (2013) The influence of vibration type, frequency, body position and additional load on the neuromuscular activity during whole body vibration. Eur J Appl Physiol 113(1):1–11
Di Giminiani R, Masedu F, Padulo J, Tihanyi J, Valenti M (2015) The EMG activity–acceleration relationship to quantify the optimal vibration load when applying synchronous whole-body vibration. J Electromyogr Kinesiol 25(6):853–859. https://doi.org/10.1016/j.jelekin.2015.09.004
Dickin DC, McClain MA, Hubble RP, Doan JB, Sessford D (2012) Changes in postural sway frequency and complexity in altered sensory environments following whole body vibrations. Hum Mov Sci 31(5):1238–1246. https://doi.org/10.1016/j.humov.2011.12.007
Di Giminiani R, Tihanyi J, Safar S, Scrimaglio R (2009) The effects of vibration on explosive and reactive strength when applying individualized vibration frequencies. J Sports Sci 27(2):169–177. https://doi.org/10.1080/02640410802495344
Mesumeci G (2017) The use of vibration as physical exercise and therapy. J Funct Morphol Kinesiol 2(2):17
Cochrane D (2013) The sports performance application of vibration exercise for warm-up flexibility and sprint speed. Eur J Sport Sci 13(3):256–271. https://doi.org/10.1080/17461391.2011.606837
Rittweger J (2010) Vibration as an exercise modality: how it may work, and what its potential might be. Eur J Appl Physiol 108:877–904. https://doi.org/10.1007/s00421-009-1303-3
Erskine J, Smillie I, Leiper J, Ball D, Cardinale M (2007) Neuromuscular and hormonal responses to a single session of whole body vibration exercise in healthy young men. Clin Physiol Funct Imaging 27(4):242–248. https://doi.org/10.1111/j.1475-097X.2007.00745.x
Padulo J, Di Giminiani R, Ibba G, Zarrouk N, Moalla W, Attene G, Migliaccio GM, Pizzolato F, Bishop D, Chamari K (2014) The acute effect of whole body vibration on repeated shuttle-running in young soccer players. Int J Sports Med 35(1):49–54. https://doi.org/10.1055/s-0033-1345171
Despina T, Dallas G, Tsiganos G, Sotiris P, di Cagno A, George K, Maria R, Stavros K (2014) Short-term effect of whole-body vibration training on balance, flexibility and lower limb explosive strength in elite rhythmic gymnasts. Hum Mov Sci 33:149–158. https://doi.org/10.1016/j.humov.2013.07.023
di Cagno A, Fiorilli G, Iuliano E, Aquino G, Giombini A, Battaglia C, Piazza M, Tsopani D, Calcagno G (2014) Time-of-day effects on static and dynamic balance in elite junior athletes and untrained adolescents. Int J Sports Sci Coach 9(4):615–625. https://doi.org/10.1260/1747-9541.9.4.615
Piazza M, Battaglia C, Fiorilli G, Innocenti G, Iuliano E, Aquino G, Calcagno G, Giombini A, Di Cagno A (2014) Effects of resistance training on jumping performance in pre-adolescent rhythmic gymnasts: a randomized controlled study. Ital J Anat Embryol 119(1):10–19. https://doi.org/10.13128/ijae-14635
Erkmen N, Suveren S, Göktepe A (2012) Effects of exercise continued until anaerobic threshold on balance performance in male basketball players. J Hum Kinet 33:73–79. https://doi.org/10.2478/v10078-012-0046-0
Hammami R, Behm DG, Chtara M, Othman AB, Chaouachi A (2014) Comparison of static balance and the role of vision in elite athletes. J Hum Kinet 41(1):33–41. https://doi.org/10.2478/hukin-2014-0030
McBride JM, Nuzzo JL, Dayne AM, Israetel MA, Nieman DC, Triplett NT (2010) Effect of an acute bout of whole body vibration exercise on muscle force output and motor neuron excitability. J Strength Cond Res 24(1):184–189. https://doi.org/10.1519/JSC.0b013e31819b79cf
Fernandes IA, Kawchuk G, Bhambhani Y, Gomes PSC (2013) Does whole-body vibration acutely improve power performance via increased short latency stretch reflex response? J Sci Med Sport 16(4):360–364. https://doi.org/10.1016/j.jsams.2012.08.010
Munn J, Sullivan SJ, Schneiders AG (2010) Evidence of sensorimotor deficits in functional ankle instability: a systematic review with meta-analysis. J Sci Med Sport 13(1):2–12. https://doi.org/10.1016/j.jsams.2009.03.004
di Cagno A, Giombini A, Iuliano E, Moffa S, Caliandro T, Parisi A, Borrione P, Calcagno G, Fiorilli G (2017) Acute effect of whole body vibration on postural control in congenitally blind subject: a preliminary evidence. Disab Rehabil 40(22):2632–2636. https://doi.org/10.1080/09638288.2017.1353650
Weston M, Batterham AM, Castagna C, Portas MD, Barnes C, Harley J, Lovell RJ (2011) Reduction in physical match performance at the start of the second half in elite soccer. Int J Sport Physiol 6(2):174–182
Mohr M, Krustrup P, Nybo L, Nielsen JJ, Bangsbo J (2004) Muscle temperature and sprint performance during soccer matches–beneficial effect of re-warm-up at half-time. Scand J Med Sci Sports 14(3):156–162. https://doi.org/10.1111/j.1600-0838.2004.00349.x
Lovell RJ, Kirke I, Siegler J, McNaughton LR, Greig MP (2007) Soccer half-time strategy influences thermoregulation and endurance performance. J Sports Med Phys Fitness 47:263–269
Naka M, Fujiwara K, Kiyota N (2015) Postural responses to various frequencies of vibration of the triceps surae and forefoot sole during quiet standing. Perception 44(1):39–51. https://doi.org/10.1068/p7738
Karim A, Roddey T, Mitchell K, Ortiz A, Olson S (2019) Immediate effect of whole body vibration on saute height and balance in female professional contemporary dancers a randomized controlled trial. J Dance Med Sci 23(1):3–10
Fiorilli G, Iuliano E, Mitrotasios M, Pistone EM, Aquino G, Calcagno G, di Cagno A (2017) Are change of direction speed and reactive agility useful for determining the optimal field position for young soccer players? J Sports Sci Med 16(2):247–253
Lowrey CR, Strzalkowski ND, Bent LR (2010) Skin sensory information from the dorsum of the foot and ankle is necessary for kinesthesia at the ankle joint. Neurosci Lett 485:6–10. https://doi.org/10.1016/j.neulet.2010.08.033
Schlee G, Reckmann D, Milani TL (2012) Whole body vibration training reduces plantar foot sensitivity but improves balance control of healthy subjects. Neurosci Lett 506(1):70–73
Ritzmann R, Kramer A, Bernhardt S, Gollhofer A (2014) Whole body vibration training-improving balance control and muscle endurance. PLoS ONE 9(2):e89905
Pistone EM, Laudani L, Camillieri G, Di Cagno A, Tomassi G, Macaluso A, Giombini A (2016) Effects of early whole-body vibration treatment on knee neuromuscular function and postural control after anterior cruciate ligament reconstruction: a randomized controlled trial. J Rehabil Med 48(10):880–886
Piecha M, Krol P, Juras G, Sobota G, Polak A, Bacik B (2013) The effect of short-and long-term vibration training on postural stability in men. Acta Bioeng Biomech 15(3):29–35
Goble DJ, Coxon JP, Van Impe A, Geurts M, Doumas M, Wenderoth N, Swinnen SP (2011) Brain activity during ankle proprioceptive stimulation predicts balance performance in young and older adults. J Neurosci 31(45):16344–16352. https://doi.org/10.1523/JNEUROSCI.4159-11.2011
Diener HC, Dichgans J, Guschlbauer B, Mau H (1984) The significance of proprioception on postural stabilization as assessed by ischemia. Brain Res 296(1):103–109. https://doi.org/10.1016/0006-8993(84)90515-8
Kavounoudias A, Roll R, Roll JP (2001) Foot sole and ankle muscle inputs contribute jointly to human erect posture regulation. J Physiol 532(3):869–878. https://doi.org/10.1111/j.1469-7793.2001.0869e.x
Kirialanis P, Dallas G, Di Cagno A, Fiorilii G (2015) Knee injuries at landing and take-off phase in gymnastics. Sci Gymnast J 7(1):17–25
Di Giminiani R, Masedu F, Tihanyi J, Scrimaglio R, Valenti M (2013) The interaction between body position and vibration frequency on acute response to whole body vibration. J Electromyogr Kinesiol 23(1):245–251
Scoppa F, Capra R, Gallamini M, Shiffer R (2013) Clinical stabilometry standardization: definitions–acquisition interval–sampling frequency. Gait Posture 37(2):290–292
Ruhe A, Fejer R, Walker B (2010) The test–retest reliability of centre of pressure measures in bipedal static task conditions–a systematic review of the literature. Gait Posture 32(4):436–445
Doyle RJ, Hsiao-Wecksler ET, Ragan BG, Rosengren KS (2007) Generalizability of center of pressure measures of quiet standing. Gait Posture 25(2):166–171. https://doi.org/10.1016/j.gaitpost.2006.03.004
Billot M, Handrigan GA, Simoneau M, Teasdale N (2015) Reduced plantar sole sensitivity induces balance control modifications to compensate ankle tendon vibration and vision deprivation. J Electromyogr Kinesiol 25:155–160. https://doi.org/10.1016/j.jelekin.2014.06.003
Padulo J, Filingeri D, Chamari K, Migliaccio GM, Calcagno G, Bosco G, Annino G, Tihanyi J, Pizzolato F (2014) Acute effects of whole-body vibration on running gait in marathon runners. J Sports Sci 32(12):1120–1126. https://doi.org/10.1080/02640414.2014.889840
Cloak R, Nevill A, Wyon M (2016) The acute effects of vibration training on balance and stability amongst soccer players. Eur J Sport Sci 16(1):20–26. https://doi.org/10.1080/17461391.2014.973912
Siu PM, Tam BT, Chow DH, Guo JY, Huang YP, Zheng YP, Wong SH (2010) Immediate effects of 2 different whole-body vibration frequencies on muscle peak torque and stiffness. Arch Phys Med Rehabil 91(10):1608–1615. https://doi.org/10.1016/j.apmr.2010.07.214
Pollock KM (2010) The star excursion balance test as a predictor of lower extremity injury in high school football players. Theses University of Toledo
Sañudo B, Feria A, Carrasco L, de Hoyo M, Santos R, Gamboa H (2012) Does whole body vibration training affect knee kinematics and neuromuscular control in healthy people? J Sports Sci 30(14):1537–1544
Giagazoglou P, Amiridis IG, Zafeiridis A, Thimara M, Kouvelioti V, Kellis E (2009) Static balance control and lower limb strength in blind and sighted women. Eur J Appl Physiol 107:571–579. https://doi.org/10.1007/s00421-009-1163-x
Han J, Waddington G, Adams R, Anson J, Liu Y (2016) Assessing proprioception: a critical review of methods. J Sport Health Sci 5(1):80–90. https://doi.org/10.1016/j.jshs.2014.10.004
Cochrane DJ (2011) Vibration exercise: potential benefit. Int J Strength Sport Med 32:75–99. https://doi.org/10.1055/s-0030-1268010
Sundstrup E, Jakobsen MD, Andersen JL, Randers MB, Petersen J, Suetta C, Aagaard P, Krustrup P (2010) Muscle function and postural balance in lifelong trained male footballers compared with sedentary elderly men and youngsters. Scand J Med Sci Sports 20(s1):90–97. https://doi.org/10.1111/j.1600-0838.2010.01092.x
di Cagno A, Battaglia C, Giombini A, Piazza M, Fiorilli G, Calcagno G, Pigozzi F, Borrione P (2013) Time of day - effects on motor coordination and reactive strength in elite athletes and untrained adolescents. J Sports Sci Med 12(1):182
Acknowledgements
The experiments comply with the current Italian laws. The Study was carried out with no external financial supports.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by GF, EI, AB, FQ, and MC. The first draft of the manuscript was written by AC, GC, AG, and FP commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This study, designed and conducted according to the ethical principles of the 2008 Declaration of Helsinki, was approved by the local Ethics Committee (CAR 30/2020).
Informed consent
Written informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Fiorilli, G., Iuliano, E., Giombini, A. et al. The optimal whole body vibration frequency effects on postural responses in soccer players. Sport Sci Health 16, 435–442 (2020). https://doi.org/10.1007/s11332-020-00621-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11332-020-00621-x