
Abstract
Purpose
The aim of study was to evaluate the effect of integrated exercise training programs on functional movement’s patterns, dynamic stability, jump-landing biomechanics, and muscle strength in elite young basketball players.
Methods
A study involved 31 youth most talented Lithuanian basketball players (15 male, 16 female) selected by the coaches of Lithuanian basketball federation. Functional movement patterns were evaluated with Functional Movement Screen (FMS) tests. The Y Balance test was used to assess athlete’s dynamic stability of lower extremities. Landing error scoring system (LESS) was used to assess athlete’s body and lower extremity biomechanical properties during the jump-landing task. Isokinetic dynamometry was used to measure thigh muscle’s strength. The integrated training program that incorporates multiple types of exercise, such as stability, flexibility, and strength exercises. Data analysis was performed using the dependent nonparametric Wilcoxon signed-rank test. In all statistical procedures, p ≤ 0.05 was regarded as significant. Correlation coefficients of tests results and efficiency were analyzed using Spearman correlation coefficient.
Results
The total score of FMS had increased from 15.89 ± 2.0 to 17 ± 1.23 (p = 0.04) in female basketball players. Jump-landing biomechanics measured by LESS had improved from 6.85 ± 2.34 to 4.62 ± 2.87 (p = 0.01) points in male basketball players. All the parameters of dynamic stability of lower limbs had improved after exercise training sessions. The knee flexion/extension ratio peak torque to body weight measured by isokinetic dynamometer increased in males and females except right leg at speed of 60°/s in males.
Conclusions
These results indicate that integrated exercise training program incorporated into regular basketball training sessions might have influence on performance and risk factors of sports injuries in youth basketball players.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Basketball is a very popular sport played all around the world. Professional basketball today has become a highly physical, high-contact sport [1]. The play is characterized by intensive body contact, frequent intermittent running and jumping, demanding one-on-one situations, quick direction changes in combination with challenging technique, and coordination aspects like catching, throwing, passing, and dribbling [2,3,4]. Most of the injuries in basketball involve the lower extremities [5].
It is estimated that 30–45 million youth 6–18 years of age participate in some form of athletic [6]. More young athletes are becoming professionals at a younger age [6]. Increased playing is mirrored by an increased risk of traumatic injury or overuse musculoskeletal injury by young sports participants [7]. Young athletes who participate in one of sports have more injuries and play sports shorter than those who specialize in variety of sport before puberty [8].
Systematic reviews showed evidence for the effectiveness of proprioceptive/neuromuscular training in reducing the incidence of certain types of sports injuries among adolescent and young adult athletes during pivoting sports such as basketball [7]. Basketball coaching and conditioning professionals should not assume a linear dose–response between accelerometer and internal training load models during training, and are recommended to combine internal and external approaches when monitoring training loads in players [9]. Skilled young athletes must be mentored carefully to prevent over participation, which may affect them physically as well as psychologically [6]. Research demonstrates that significant, amenable benefits can be gained from training age appropriate interventions [10]. It is very important to promote healthy participation and preventive care measures. The chronic musculoskeletal injuries associated with excessive training load can be monitored with RPE method, which is practical tool to monitor and plan individualized youth training loads. It can prevent from injuries, monotony, strain, overreaching, and burnout [11].
We hypothesized that integrated exercise training program consisted of foam rolling, flexibility, core stability, and strength exercises, incorporated into regular training sessions as a warm-up might have influence on functional movement’s patterns, dynamic stability, and jump-landing biomechanics and muscle strength in elite young basketball players. The young athletes should have good background of fundamental movements to stay injury free. It is very important that specialization do not become traumatic factor. When children are confident and competent with this skill, they can develop sport-specific and complex movement skills that allow them to enjoy sport and physical activity.
Methods
The most talented 15-year-old 31 young Lithuanian basketball players were selected by the top coaches of Lithuanian Basketball Federation for 1 year duration project “Talents U15 generation 2015” which was partially funded by FIBA Europe Youth Development Fund. All the players in our sample were right handed and dominant (jumping) leg was left. The players were tested twice before and after integrated exercise training program. The regular basketball training sessions were five times per week. Integrated exercise training program was performed for 5 months additionally to the regular basketball training sessions. In this period, players had six intensive training weekends. An exercise program has been created individually according to the test results (dosage repetition sessions and load were prescribed individually) and consisted of foam rolling, core stability, flexibility, and strength exercises. The participants were taught how to perform exercises by the team physiotherapist and it has been recommended to perform them three times per week. Physical examination consisted of the Functional Movement Screen, Y Balance test, Landing Error Scoring System, and an isokinetic dynamometry. The examiner had more than 5 years of clinical experience and theoretical and practical experience with scoring all these tests. A total of 31 participants (100%) complete follow-up testing (Fig. 1). All participants and their parents willingly signed the consent form and the rights of the participants were protected.

Research organization
Functional movement patterns were evaluated with Functional Movement Screen (FMS) tests, developed by Cook and Burton [12]. It is a comprehensive screen to assess the quality of fundamental movement patterns for presumably identifying an individual’s physical limitations or asymmetries [13, 14] in seven fundamental movement patterns: the deep squat, hurdle step, lunge, shoulder mobility, active straight leg raise, push-up, and rotary stability [7, 15]. Each participant was given three trials on each of the seven tests. The trial was scored on ordinal scale from zero to three. Final FMS score was obtained when the results of FMS tests were summed [13].
The Lower Quarter Y Balance test is a dynamic postural control test that requires balance on one leg with maximum reach of the opposite limb. The YBT-LQ is a measure of dynamic balance and has been used to assess physical performance, identify chronic ankle instability, and identify athletes at greater risk for lower extremity injury [16,17,18]. YBT consists of a stance platform to which three pieces of PVC pipe are attached in the anterior, posteromedial, and posterolateral reach directions [19]. Subject stands with the right foot on the center foot plate and the most distal aspect of the subject’s barefoot at the starting line. Three trials were completed in each direction. The same process was repeated using the contralateral limb as the stance limb [18]. Performance for all trials was recorded and maximum reach score for each reach direction was extracted for data analysis. The composite score on the test was calculated by averaging the maximum scores for each reach direction after the maximum scores were normalized to the limb length [20].
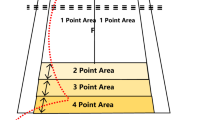
Landing Error Scoring System (LESS) was used to assess athlete’s body and lower extremity biomechanical changes during the jump-landing task. Two digital video cameras were placed in front of and to the right of the participants to capture frontal and sagittal images of three jump-landing trials [21]. The best LESS score from the three trials at each testing session was used for data analyses. The participant began the task standing on a 30-cm-high box placed at a distance of half their body height away from a landing area, which was marked by a line on the ground. Participants were instructed to jump forward, so that both limbs left the box simultaneously, to land just past the line, and to jump for maximal height immediately after landing [22, 23].
Knee muscle testing was performed on a Biodex System 4 Pro Isokinetic Dynamometer et velocities of 60 and 180°/s. Prior to isokinetic testing, each subject completed the warm-up phase. Subjects were placed in a comfortable upright-seated position on the Biodex dynamometer chair and was secured using thigh. Straps on pelvis and torso was attached in order to minimize extraneous body movements. The resistance pad was placed at a level a proximally 3 cm proximal of medial malleolus. The range of motion of the knee joint during testing was set from 0° to 90° and all limbs were gravity compensated. Bilateral isokinetic (concentric/concentric) knee extension and flexion studies with the protocol of 60°/s (5 repetitions) and 180°/s (10 repetitions) were accomplished. Vocal encouragement during the testing was consisted and standardized [24].
Statistical analysis
Data analysis was performed using the dependent nonparametric Wilcoxon signed-rank test. In all statistical procedures, p ≤ 0.05 was regarded as significant. The values are presented as arithmetical mean ± standard deviation (SD) of the sample. Correlation coefficients of tests results and efficiency were analyzed using Spearman correlation coefficient. All statistical analyses were performed using SPSS 22 (IBM Corp., Armonk, NY, USA).
Results
The average of total FMS total scores is demonstrated in Table 1. The functional movement patterns after integrated exercise training program improved in females. Dynamic balance of lower limbs measured by YBT-LQ statistically significant increased in both groups (p ≤ 0.05). Changes of YBT-LQ composite scores (normalized according limb length) are presented in Table 2. Changes of total body biomechanics during drop vertical jump task analyzed using LESS scores are demonstrated in Table 3. Jump-landing biomechanics improved in males (p ≤ 0.05). Knee flexion/extension ratio peak torque to body weight at high speed (180°/s) increased after integrated exercise training program in male and female groups.
The isokinetic knee flexion/extension ratio at speed 60 and 180°/s in female and male groups shown in Table 4. Correlational data revealed a significant correlation between FMS total score and YBT-LQ composite score of the left leg in males after the training season (r = − 0.535; p = 0.02). The jump-landing biomechanics (LESS) improved with the increase of knee flexion/extension ratio peak torque to body weight at speed of 180°/s in the left leg of males after the integrated exercise training program (r = − 0.558; p = 0.03).
Discussion
Age of 13–15 is the sport specialization years. This is the time when fundamental functional movement patterns are extremely important in the athlete’s development and injury prevention. The main aim of this study was to assess an impact of integrated training program of elite young basketball players.
The FMS were being used clinically to identify athletes at risk of injury [13, 25] and subsequently to administer programs to decrease injury risk [26]. Our results showed that after training program, the quality of functional movements in females has increased by 1.1 in the FMS total score. The increase of FMS total score by 2.5 score was noted in special operations soldiers after a 6-week functional training that focused on agility, core strength, balance, and power [27]. In our study, in both groups, the composite FMS scores were higher than the injury risk cut-off point ≤ 14. Kiesel et al. claim that if the FMS result is 14 or less, it can be that the athlete have 11 times increased risk of sport injury compared with players who have scored more than 14 points [28].
YBT also was being used clinically to identify athletes at risk of injury [29]. Y Balance tests are reliable measures of postural control in active younger adults [18, 29, 30]. Investigators have published a systematic review of YBT-LQ research and have reported that poor performance has a relationship with lower extremity injury risk [29]. The composite score statistically significant increased in female and male groups after 5-month training. Research demonstrated that after injury prevention program, all athletes (youth soccer players) experienced an improvement in YBT scores [31]. Our findings are similar to Plisky et al., in his study, 235 (105 girls, 130 boys) high school basketball players were tested, the composite score in girls group was 98.4 ± 8.2, in boys group was 103.0 ± 8.0. It also states that if the composite score index is ≤ 94, the player can be at greater risk of injury for lower extremities [18]. Poor performance has also been found to be predictive of ankle sprains in college-aged individuals [32]. In Butler’s study, college football players who scored below 89.6 were 3.5 times more likely to get injured [20]. In our study, all participants were above of the risk injury index (≤ 99.43 ± 12.36).
LESS test is showing jump-landing biomechanics [21]. For all subjects, the average LESS scores was more than six points before beginning an exercise program. Individuals who had > 6 points demonstrated “poor” landing technique [22]. In our study, both groups demonstrated “poor” landing technique. After training program, our results showed that in male group, the quality of landing technique has increased (4.62 point, it demonstrates “good” landing technique). Lindsay et al. findings indicate that neuromuscular training programs are most effective with athletes who display “poor” movement techniques before beginning program [14]. Other scientists, who examined 2753 cadets, found that women biomechanics are worse than men [33], and, in our study, show the similar results after exercise training program.
Isokinetic dynamometry is frequently chosen because of their inherent patient safety, objectivity, and reproducibility in testing measures [34]. Evaluation of muscle strength characteristics at various angular velocities has provided us with a better understanding of the knee joint function [35]. Results of our study showed that all participants were below the stated mark, and then, marks were at 60°/s men 0.60, women 0.62, at 180°/s men 0.72, and women 0.76 [36,37,38]. The results of isokinetic knee flexion/extension ratio at lower angular velocities indicate that after exercise training program, statistically significant differences was noticed in male group in left side and at higher angular velocities in both sides. After training program in female group, statistically significant difference was only in left side at velocities angular 180°/s. In basketball, the left leg is dominant in take-off element, so it might explain improvement in isokinetic strength ratio. In other study, there were statistically significant differences between all parameters except at velocities of 60°/s [39].
There is no consensus in the literature about the influence of dominant leg to the performance. Two isokinetic studies, professional soccer [40] and elite handball players [41], showed no muscle strength asymmetry of the knee extensor and flexor muscles, regardless of dominance. Schiltz et al. found that there were no differences in functional or relative isokinetic variables between professional and junior basketball players regarding dominant side effect [24]. According to the studies, we have not analyzed dominant side effect.
Our results indicate that integrated exercise training program might have influence on performance and risk factors of sport injuries in youth basketball players. One research demonstrated that after training program, the level of baseline movement error affected the subjects’ abilities, which has significantly improved after completing one of the injury prevention programs [22].
Limitations of the study
There was no possibility to have control group, because the selected players were the best at their age in country. The selection of players was made by the coaches of X basketball federation. Training program was performed only during the camps and was not supervised between the weekend training sessions. The physical maturation of the players might have influence to the results.
Conclusion
Being able to identify modifiable factors related to injury has a significant value for athletic health care. Integrated exercise training program improved the quality of functional movement’s patterns in female and jump-landing biomechanics in male basketball players. Dynamic stability of lower quarter and the knee flexion/extension ratio peak torque to body weight increased in both groups after exercise training sessions. There is strong evidence that integrated exercise training program (core stability, flexibility, strength, and foam rolling exercises) incorporated into regular training sessions might have influence on performance and risk of sports injuries in youth basketball players.
References
Drakos MC, Domb B, Starkey C, Callahan L, Allen AA (2010) Injury in the National Basketball Association A 17-year overview. Sports Health 2(4):284–290
Arendt E, Dick R (1995) Knee injury patterns among men and women in collegiate basketball and soccer. NCAA data and review of literature. Am J Sports Med 23(6):694–701
Krosshaug T, Nakamae A, Boden BP, Engebretsen L, Smith G, Slauterbeck JR, Hewett TE, Bahr R (2007) Mechanisms of anterior cruciate ligament injury in basketball video analysis of 39 cases. Am J Sports Med 35(3):359–367
Piasecki D, Spindler KP, Warren TA, Andrish JT, Parker RD (2003) Intraarticular injuries associated with anterior cruciate ligament tear: findings at ligament reconstruction in high school and recreational athletes an analysis of sex-based differences. Am J Sports Med 31(4):601–605
Leppänen M, Pasanen K, Kujala UM, Parkkari J (2015) Overuse injuries in youth basketball and floorball. J Sports Med 6:173–179
Brenner JS (2017) Overuse injuries, overtraining, and burnout in child and adolescent athletes. Pediatrics 19(6):1242–1245
Yang J, Marshall SW, Bowling JM, Runyan CW, Mueller FO, Lewis MA (2005) Use of discretionary protective equipment and rate of lower extremity injury in high school athletes. Am J Epidemiol 161(6):511–519
American Academy of Pediatrics, Committee of Sports Medicine and Fitness (2000) Intensive training and sports specialization in young athletes. Pediatrics 106:154–157
Scanlan AT, Wen N, Tucker PS, Dalbo VJ (2014) The relationships between internal and external training load models during basketball training. J Strength Cond Res 28(9):2397–2405
Meyers GD, Lloyd RS, Brent JL, Faigenbaum AD (2013) How young is “Too Young” to start training? ACSMs Health Fit J 17(5):14–23
Lupo C, Tessitore A, Gasperi L, Gomez MAR (2017) Session-RPE for quantifying the load of different youth basketball training sessions. Biol Sport 34:11–17
Cook G, Burton L, Hoogenboom B (2006) Pre-participation screening: the use of fundamental movements as an assessment of function—part 1. N Am J Sports Phys Ther 1(2):62–72
O’Connor FG, Deuster PA, Davis J, Pappas CG, Knapik JJ (2011) Functional movement screening: predicting injuries in officer candidates. Med Sci Sports Exerc 43(12):2224–2230
Schneiders AG, Davidsson A, Horman E, Sullivan SJ (2011) Functional Movement Screen™ normative values in a young, active population. Int J Sports Phys Ther 6(2):75–82
Mokha M, Sprague PA, Gatens DR (2016) Predicting musculoskeletal injury in national collegiate athletic association division II athletes from asymmetries and individual-test versus composite functional movement screen scores. J Athl Train 51(4):2
Hertel J, Braham RA, Hale SA, Olmsted-Kramer LC (2006) Simplifying the star excursion balance test: analyses of subjects with and without chronic ankle instability. J Orthop Sports Phys Ther 36:131–137
Olmsted LC, Carcia CR, Hertel J, Shultz SJ (2002) Efficacy of the star excursion balance tests in detecting reach deficits in subjects with chronic ankle instability. J Athl Train 37:501–506
Plisky PJ, Rauh MJ, Kaminski TW, Underwood FB (2006) Star excursion balance test as a predictor of lower extremity injury in high school basketball players. J Orthop Sports Phys Ther 36:911–919
Robinson R, Gribble PA (2008) Support for a reduction in the number of trials needed for the star excursion balance test. Arch Phys Med Rehabil 89:364–370
Butler RJ, Lehr ME, Fink ML, Kiesel KB, Plisky PJ (2013) Dynamic balance performance and noncontact lower extremity injury in college football players: an initial study. Sports Health 5(5):417–422
Padua DA, Marshall SW, Boling MC, Thigpen CA, Garrett WE, Beutler AI (2009) The Landing Error Scoring System (LESS) is a valid and reliable clinical assessment tool of jump-landing biomechanics: the JUMP-ACL study. Am J Sports Med 37(10):1996–2002
DiStefano LJ, Padua DA, DiStefano MJ, Marshall SW (2009) Technique, and exercise program on movement patterns after an anterior cruciate ligament injury prevention program in youth soccer players. Am J Sports Med 37(3):495–505
Padua DA, DiStefano LJ, Beutler AI, de la Motte SJ, DiStefano MJ, Marshall SW (2015) The landing error scoring system as a screening tool for an anterior cruciate ligament injury—prevention program in elite-youth soccer athletes. J Athl Train 50(6):589–595
Schiltz M, Lehance C, Maquet D, Bury T, Crielaard JM, Croisier JL (2009) Explosive strength imbalances in professional basketball players. J Athl Train 44(1):39–47
Chorba RS, Chorba DJ, Bouillon LE, Overmyer CA, Landis JA (2010) Use of a functional movement screening tool to determine injury risk in female collegiate athletes. N Am J Sports Phys Ther 5(2):47–54
Kiesel K, Plisky P, Butler R (2011) Functional movement test scores improve following a standardized off-season intervention program in professional football players. Scand J Med Sci Sports 21(2):287–292
Goss DL, Christopher GE, Faulk RT, Moore J (2009) Functional training program bridges rehabilitation and return to duty. J Spec Oper Med. 9(2):29–48
Kiesel K, Plisky P, Voight M (2007) Can serious injury in professional football be predicted by a preseason functional movement screen? N Am J Sports Phys Ther 2(3):147–158
Gribble PA, Hertel J, Plisky P (2012) Using the Star Excursion Balance Test to assess dynamic postural-control deficits and outcomes in lower extremity injury: a literature and systematic review. J Athl Train 47:339–357
Plisky PJ, Gorman PP, Butler RJ et al (2009) The reliability of an instrumented device for measuring components of the star excursion balance test. N Am J Sports Phys Ther 4(2):92–99
Bodden JG, Needham RA, Chockalingam N (2015) The effect of an intervention program on functional movement screen test scores in mixed martial arts athletes. J Strength Cond Res 29(1):219–225
de Noronha M, Franca LC, Haupenthal A, Nunes GS (2013) Intrinsic predictive factors for ankle sprain in active university students: a prospective study. Scand J Med Sci Sports 23(5):541–547
Beutler AI, Motte SJ, Marshall SW, Padua DA, Boden BP (2009) Muscle strength and qualitative jump-landing differences in male and female military cadets: the jump-ACL study. JSSM 8:663–671
Saenz A, Avelanet M, Hijos E, Chaler J, Garreta R, Pujol E, Sandoval B, Buen C, Farreny A (2010) Knee isokinetic test-retest: a multicentre knee isokinetic test–retest study of a fatigue protocol. Eur J Phys Rehabil Med 46(1):81–88
Rezaei M, Ebrahimi I, Vassaghi- Gharamaleki B, Pirali M, Mortaza N, Malmir K, Ghasemi K, Jamshidi AA (2014) Isokinetic dynamometry of the knee extensors and flexors in Iranian healthy males and females. Med J Islam Repub Iran 28:108
Davies G (1992) Compendium of isokinetics in clinical usage and rehabilitation techniques, 4th edn. S&S Publishers, Onalaska
Dvir Z (1995) Isokinetics: muscle testing, interpretation, and clinical applications. Churchill Livingstone, Edinburgh
Perrin D (1993) Isokinetic exercise and assessment. Human Kinetics Publishers, Champaign
Cvjetkovic DD, Bijeljac S, Palija S, Talic G, Radulovic TN, Kosanovic MG, Manojlovic S (2015) Isokinetic testing in evaluation rehabilitation outcome after ACL reconstruction. Med Arch 69(1):21–23
Zakas A (2006) Bilateral isokinetic peak torque of quadriceps and hamstring muscles in professional soccer players with dominance on one or both two sides. J Sports Med Phys Fitness 46(1):28–35
Zouita Ben Moussa A, Layouni R, Dziri C, Ben Salah FZ, Hammami N (2005) Isokinetic exploration of muscle force of the knee in Tunisian handball players. J Trauma Sport. 22(4):226–231
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared no conflict of interest.
Ethical approval
All procedures were approved by Kaunas Regional Ethics Committee (no. BE–2–27) and were carried out in line with the Declaration of Helsinki.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Garbenytė-Apolinskienė, T., Šiupšinskas, L., Salatkaitė, S. et al. The effect of integrated training program on functional movements patterns, dynamic stability, biomechanics, and muscle strength of lower limbs in elite young basketball players. Sport Sci Health 14, 245–250 (2018). https://doi.org/10.1007/s11332-017-0409-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11332-017-0409-y