
Abstract
Introduction
Obstructive Sleep Apnea Syndrome (OSAS) is a respiratory disorder characterized by repeated episodes of partial or complete airway obstruction. Continuous Positive Airway Pressure therapy (CPAP) is effective in improving sleep quality and daytime sleepiness. The aim of the study was to evaluate therapeutic adherence in a sample of patients with OSAS from the Pneumology ward of the “Cardinal Massaia” Hospital in Asti.
Materials and methods
A sample of 221 patients with OSAS were collected and retrospectively analyzed from January 2019 to December 2021. Ventilation hours during device titration (T1), possible second titration (T2) and one-year control (T3) were considered. The use of the CPAP device equal to or greater than 4 h/night was considered as therapeutic adherence. Age, gender, severity of OSAS, smoking, interface used and Epworth Sleepiness Scale (ESS) score were considered.
Results
The analysis data showed that the percentage of adhesion during T1 was 84%. Only 9% needed T2, with 84% adherence. At T3 the adherence was 86%. Correlation studies showed that only smoking had a positive correlation with adherence, while OSAS severity, gender, ESS score, interface used and age had no statistically significant correlation.
Conclusion
It was important to understand that OSAS is a disease with prolonged treatment, which affects the life of the person and his family. Therefore, the concept of assistance network was born, which sees the healthcare operators, the person and his family as the main actors involved in a care process.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Obstructive Sleep Apnea Syndrome (OSAS) is a respiratory disorder characterized by repeated episodes of partial or complete airway obstruction, related to hypoxemia and oxyhemoglobin desaturations. OSAS can determine the fragmentation of night rest with daytime sleepiness, mood alterations, neurobehavioral performance and consequent reduction in quality of life [1]. The respiratory effort, resulting from OSAS, can aggravate any comorbidities such as ischemic heart disease, respiratory insufficiency, cardiac arrhythmias and arterial hypertension. The main risk factors for the development of OSAS may be obesity [2] and cigarette smoking. The main parameter used for the classification of OSAS is the number of apnea episodes occurring in one hour (AHI). Other parameters, which can be taken into consideration, are the desaturation time below 90% (T90) and the number of events in which there is a decrease in oximetry equal to 4%, compared to the baseline of the subject (ODI).
Continuous Positive Airway Pressure therapy (CPAP) is the treatment of first choice as it is effective in improving sleep quality and excessive daytime sleepiness, which is the main cause of road accidents [1]. The continued use of CPAP treatment would, also, allows to reduce long-term cardiovascular accidents [3] and total mortality. From the moment the patient accepts the treatment, the educational process begins, with the involvement of a possible caregiver. This path takes place in four phases: training planning, training, titration and prescription. In the initial phase, all the conditions necessary for training are evaluated, such as, for example, the availability of the CPAP, the planning of the day, the place and the opening of the medical record. During the training, the healthcare professional provides information relating to the operation of the device and selects the appropriate interface, simulating a situation of night rest. Titration is the process of defining the pressure parameters that allow the correction of sleep apnea. It begins during the training phase, under the supervision of highly skilled nursing staff, who manually sets the pressures of the CPAP device, based on the patient’s parameters. In anticipation of home use, the titration continues with the automatic regulation, by the device, of the pressure, based on the patient’s needs during the night (APAP). The data are collected seven days after the start of treatment and if critical issues emerge, a new titration is scheduled.
The main reasons for discontinuation of CPAP treatment may be sinusitis, congestion, nasal dryness and lack of subjective perception of improvements [4].
The aim of the study was to evaluate therapeutic adherence in a sample of patients diagnosed with OSAS, taken in charge by the Pneumology clinic of the “Cardinal Massaia” hospital in Asti. The adherence values obtained will be correlated with the variables of the enrolled subjects to understand any significant relationships.
Materials and methods
With a retrospective cohort study design, it was analysed the clinical documentation of a convenience sample made up of 221 patients with a diagnosis of OSAS, on CPAP treatment and taken in charge by the Pneumology unit of the “Cardinal Massaia” hospital in Asti. Each subject underwent a maximum of 3 checks: titration of the CPAP device (T1), a possible second titration (T2) and subsequent check after one year (T3). The reference period for data collection was between January 2019 and December 2021.
In CPAP training, patients are instructed by healthcare personnel to assume the lateral position while using the device at night. During the three checks (T1, T2 and T3), the evaluation of the therapeutic efficacy of CPAP was based on the report data of the device, which includes residual AHI, flow curves and hours of use, but there was no feedback on the position assumed by the patient. Only in doubtful cases, further evaluation is performed, through cardiorespiratory monitoring.
The findings came from paper medical records and from the D-Shop® software database in use in the facility. For the purposes of the analysis, the hours of ventilation during the three periods (T1, T2, T3) were considered. The use of the CPAP device with a value equal to or greater than 4 h/night was considered as therapeutic adherence (< 4 h/night = therapeutic non-adherence). The Gold Standard of hours of positive pressure therapy was identified from the scientific literature [5,6,7]. Additional data taken into consideration, in order to study the link between the sample variables and therapeutic adherence, were age, gender, severity of OSAS, smoking habit, the interface used and the score of the Epworth Sleepiness Scale (ESS). The ESS scale evaluates the daytime sleepiness index perceived by the subject. It consists of 8 items in which a score is assigned from 0 (= I never fall asleep) to 3 (= I have a high probability of falling asleep). A total score between 0 and 10 indicates normal daytime sleepiness, while 11 to 14 is mild, 15 to 17 is moderate and 18 to 24 is severe. The tool has been validated at the Italian level [8].
For the study of the data, descriptive statistical methods were used, such as mean, standard deviation and range, calculated with the use of the Microsoft Office Excel® software. The correlation was analyzed using the Chi-square (X2) test with a significance level of 95%. The data were collected by the researcher, with the prior consent of the patients and processed for statistical purposes only, guaranteeing anonymity.
Results
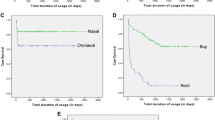
The sample analyzed consisted of 221 patients with an average age of 66 years, of which the most representative cluster was between 66 and 75 years. The other representative percentage was determined by the class between 56 and 66 years of age, 22% were over 76 years of age, more than 10% were between 46 and 55 years of age and finally only a small fraction were between 30 and 45 years of age. The sample consisted mostly of males. As concerns smoking habits, the majority of the sample declared they were non-smokers, a high percentage were former smokers, just under 20% were active smokers and in a small percentage it was not possible to detect any smoking habits (Table 1). With reference to the severity of OSAS, just over half of the sample was affected by severe OSAS, 38% by moderate OSAS and a low percentage was affected by mild OSAS. In the data analysis, ESS was also considered and it was found that the most prevalent cluster was the one that had a normal level of daytime sleepiness, 12% had mild, while moderate and severe sleepiness percentage were low. In 7% of the sample, ESS could not be detected. Just over half of the sample had used the nasal interface and remaining part used the oronasal interface (Table 2). During device titration (T1), the average hours of ventilation was 5,57 h/night and the adherence rate was 84%. Only 9% required a second titration (T2), the average hours of ventilation and adherence rate are almost the same as those found in T1. At the one-year follow-up (T3), the average CPAP hours had decreased, as they were about 5,08 h/night, while the adherence rate had increased, as it had achieved the outstanding result of 86%. In particular, in the previous controls (T1 and T2) there were 186 adherents, while at T3 there were 190, so there was an increase of 4 patients (Table 3). From the correlation analysis between the sample variables and the hours of positive pressure therapy, it emerged that the severity of OSAS, gender, ESS score, the type of interface and age had no statistically significant correlation with therapeutic adherence. The smoking habit variable, on the other hand, showed a positive correlation with the hours of ventilation (Table 4). The comparison of the ventilation hours between T1 and T3 revealed a difference between the patients adhering to the treatment which increased by 2% and the non-compliant patients which decreased by the same amount.
Discussion
From the analysis of the data, it emerged that almost all of the sample was adhering to the nocturnal CPAP treatment. The correlation study between the variables related to the enrolled patients showed that these had no link with treatment compliance, except for smoking habit. With regard to these relationships, the literature provides conflicting opinions, in fact some authors reported results comparable to those investigated in the present work [6, 7, 9], while others found significant relationships between the characteristics of the sample and adherence to the treatment [1, 5, 6, 9, 10].
From the literature it emerges that the greatest compliance is obtained from patients with the most severe OSAS level [1, 5, 9, 11, 12]. Even if a significant relationship between these two parameters was absent in the study conducted, in agreement with other studies which highlighted this weak relationship, [7, 13] it is plausible to state that at the stage of greater severity, the patient’s need for supportive treatment also increases. This also leads, indirectly, to greater therapeutic adherence. Furthermore, the results obtained could be different from the literature, due to the different sample numbers, the case mix of enrolled patients and the timing of the duration of the studies [1, 5, 9]. Above all this last variable can influence the person’s prospects for recovery, in fact, if the treatment is planned for a limited period of time, the person will be more predisposed to the use of the device. In the event that the therapeutic treatment becomes an extremely prolonged or even chronic condition, it is plausible to state that it will probably decrease the adherence of the person. For these reasons, it is difficult to establish whether the severity of OSAS is always a predictor of compliance.
The literature showed that the use of the CPAP device for a time equal to or greater than 4 h/night for at least 70% of the nights produced positive results in terms of improvement of OSAS and associated daytime symptoms [5,6,7]. At the same time, however, other studies had set, as a minimum hours of adherence, a higher time [10] and this may have influenced the adherence results obtained by the authors. This disparity can also be attributed to the subjective characteristics of each patient; in fact, some people may get optimal results even using CPAP for a shorter time [14].
The age variable taken individually does not seem to influence therapeutic adherence, even if the literature results are often different from each other [4, 9, 12, 15,16,17]. It should be noted, however, that if compared in the light of other characteristics of the sample (such as gender) it acquires a different meaning [18]. However, it is possible to state that age influences adherence results and that this depends on the physiological mechanisms of aging and on any co-morbidities. It should be considered that the average age of the analyzed sample is higher than that found by the other authors.
The literature showed that the use of nocturnal CPAP seemed to produce significant improvements in daytime sleepiness. This is plausible, since the continuous and prolonged use of the device, during the night hours, allows to reduce the events of OSAS. This guarantees the improvement of the quality of sleep and, consequently, also reduces daytime sleepiness, favoring the use of CPAP support by patients [19]. All nocturnal and diurnal benefits are detectable early (for example during training and titration) and these may affect long-term adherence [1]. Similarly, nocturnal CPAP is certainly able to affect the patient’s sleep pattern, due to device noise and interface usage.
The estimated average hours of rest for an adult are around 8, but this value tends to decrease with advancing age. If, for a young individual, applying an average of device usage less than hours of night rest can be an effective strategy, for an elderly person an estimate of the hours of sleep should be carried out. If disturbances such as nocturia and the use of diuretics in evening therapy are associated with insomnia, the average value of night rest undergoes a further reduction. Healthcare professionals must, therefore, consider these aspects in the pharmacology prescription. On the contrary, it can be argued that in the elderly, the reduction or loss of hearing and the use of drugs to treat insomnia [6, 20] can favour the use of CPAP support, as sensory perception is reduced.
In the literature, the relationship between adherence and smoking habit is inconstant, in fact, it is likely to hypothesize that smokers may accept the treatment, as they are accustomed to iatrogenic stimuli or they may refuse it as they are not inclined to follow the instructions of the health personnel [19, 21,22,23].
Another factor that could affect therapeutic adherence, although this was not found in this study, is the choice of interface to be used for CPAP. This is, in fact, able to cause effects such as claustrophobia, sinusitis, congestion and nasal dryness, resulting in less use by the patient. It is important that healthcare professionals collaborate with the person in order to carefully choose the most suitable interface, in terms of comfort and therapeutic efficacy [24]. The discomfort that nasal masks often produce can be treated by replacing them with oronasal ones. The nasal masks, however, are not prescribable to subjects who at night breathe mainly with the mouth and, for this reason, it is preferable to use oronasal interfaces, which encourage less the opening of the mouth. The disadvantages of these masks lie in a high number of leaks [25] and the need for higher pressure. To reduce the side effects caused by the masks it is also possible to use air humidification, in order to reduce the dryness of the mucous membranes. The person will also be informed that the symptoms of discomfort often cease with continuous use of the device [7]. Social support with involvement of the caregiver is also important for these patients [6]. They must actively participate in the entire training and education process, also because they can be a spectator of the improvement of OSAS symptoms, especially during the night hours [26].
Most of the literature was uniform on the non-incidence of gender [9, 15], although some studies claimed the opposite [5, 10], as they highlighted distinctions between male and female gender, even if the reasons for these differences were scarce and relatively weak.
From the data analyzed and from the literature study, it is possible to state that taking charge of these patients should happen with a case management model. The educational process that concerns these patients consists in making them understand the advantages of using the device and the interface, justifying the benefits for the quality of life [6]. Training, as suggested by some authors, must take place in a supportive way and in suitable settings, such as Pneumology clinics. In these realities, the nursing staff with advanced skills has a significant impact on therapeutic adherence [27, 28]. In Italy, no post-basic academic training or certification is required for the care of this type of patient. The management of the OSAS and the use of CPAP devices by healthcare personnel is acquired through specific training courses that include not only technical skills but also educational and relational management. Experience and the support of expert personnel also play an important role in building the background of knowledge useful for taking care of the person. The same professionals who work in contact with OSAS patients are instructors of courses for the use of CPAP. The skills achieved with the training are not limited to the acquisition of technical ability, but also relational management useful not only for the person but also for a possible caregiver.
In OSAS patients, the entire period preceding the final prescription of CPAP treatment is fundamental, since if an optimal adaptation of the patient is achieved (in terms of ventilator pressure values, adequate use of the device and interface comfort), they will immediately get positive feedback. If the patient perceives an improvement in nocturnal and daytime symptoms, he will be more inclined to use the device, even in the long term. The good therapeutic adherence result of the study conducted (86%) is probably also related to Primary Nursing (PN) applied to treated patients. This care model places the person at the center of the care process. The fundamental aspect of the PN is that the responsibility for the care of the patient belongs to a single professional defined as the referent (primary). The Primary has the responsibility and discretion to inform other professionals about everything related to the patient, verifying the adequacy of the services provided [29].
In fact, healthcare personnel do not exhaust their competence in the mere training phase, but involve the caregiver early by educating him about patient monitoring during the first use of CPAP support. The comfort of the interface, the improvement of sleep quality and daytime sleepiness are also evaluated. If negative feedback emerges, deriving from the download of data or relating to the patient’s experience, the treatment plan is immediately reformulated. In the context examined, remote monitoring of the ventilation parameters is also in use, which allows for timely intervention, reducing the time elapsed between one check and another.
Our study had some limitations. Firstly, the retrospective study did not allow to obtain the advantages of a prospective study, which would have allowed to evaluate a possible attrition rate. In addition, the panel of researchers compared the sample variables with adherence alone. It could also have been exhaustive to consider patients who had discontinued treatment. A further limitation was that the study of the variables was not supported by sufficient literature.
Conclusions
In the survey conducted it was possible to demonstrate how a model of personalized patient taking charge can improve compliance with CPAP treatment. The relational skills play a fundamental role as they influence the perception of the subject and, consequently, also the adherence to the treatment. It was important to understand that OSAS is a disease with prolonged treatment, which affects the life of the person and his family. Therefore, the concept of assistance network was born, which sees the healthcare operators, the person and his family as the main actors involved in a care process.
The literature supporting what was claimed in the study allows us to say that the variables related to the patient are not able to influence treatment compliance in a certain way. Further studies would be needed to confirm what was obtained from the data examined.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Chen YF, Hang LW, Huang CS, Liang SJ, Chung W (2015) Polysomnographic predictors of persistent continuous positive airway pressure adherence in patients with moderate and severe obstructive sleep apnea. Kaohsiung J Med Sci 31(2):83–89. https://doi.org/10.1016/j.kjms.2014.11.004
Romero-Corral A, Caples SM, Lopez-Jimenez F, Somers VK (2010) Interactions between obesity and obstructive sleep apnea: implications for treatment. Chest 137(3):711–719. https://doi.org/10.1378/chest.09-0360
Campos-Rodriguez F, Martinez-Garcia MA, de la Cruz-Moron I, Almeida-Gonzalez C, Catalan-Serra P, Montserrat JM (2012) Cardiovascular mortality in women with obstructive sleep apnea with or without continuous positive airway pressure treatment: a cohort study. Ann Intern Med 156(2):115–122. https://doi.org/10.7326/0003-4819-156-2-201201170-00006
Janson C, Nöges E, Svedberg-Randt S, Lindberg E (2000) What characterizes patients who are unable to tolerate continuous positive airway pressure (CPAP) treatment? Respir Med 94(2):145–149. https://doi.org/10.1053/rmed.1999.0703
Baratta F, Pastori D, Bucci T, Fabiani M, Fabiani V, Brunori M, Loffredo L, Lillo R, Pannitteri G, Angelico F, Del Ben M (2018) Long-term prediction of adherence to continuous positive air pressure therapy for the treatment of moderate/severe obstructive sleep apnea syndrome. Sleep Med 43:66–70. https://doi.org/10.1016/j.sleep.2017.09.032
Mehrtash M, Bakker JP, Ayas N (2019) Predictors of continuous positive Airway pressure adherence in patients with obstructive sleep apnea. Lung 197(2):115–121. https://doi.org/10.1007/s00408-018-00193-1
Sawyer AM, Gooneratne NS, Marcus CL, Ofer D, Richards KC, Weaver TE (2011) A systematic review of CPAP adherence across age groups: clinical and empiric insights for developing CPAP adherence interventions. Sleep Med Rev 15(6):343–356. https://doi.org/10.1016/j.smrv.2011.01.003
Vignatelli L, Plazzi G, Barbato A, Ferini-Strambi L, Manni R, Pompei F, D’Alessandro R (2003) GINSEN (Gruppo Italiano Narcolessia Studio Epidemiologico Nazionale. Italian version of the Epworth sleepiness scale: external validity. Neurol Sci 23(6):295–300. https://doi.org/10.1007/s100720300004
Kohler M, Smith D, Tippett V, Stradling JR (2010) Predictors of long-term compliance with continuous positive airway pressure. Thorax 65(9):829–832. https://doi.org/10.1136/thx.2010.135848
Somers ML, Peterson E, Sharma S, Yaremchuk K (2011) Continuous positive airway pressure adherence for obstructive sleep apnea. ISRN Otolaryngol 943586. https://doi.org/10.5402/2011/943586
Campos-Rodriguez F, Martinez-Alonso M, Sanchez-de-la-Torre M, Barbe F (2016) Spanish Sleep Network. Long-term adherence to continuous positive airway pressure therapy in non-sleepy sleep apnea patients. Sleep Med 17 ;1–6. https://doi.org/10.1016/j.sleep.2015.07.038
Krieger J, Kurtz D, Petiau C, Sforza E, Trautmann D (1996) Long-term compliance with CPAP therapy in obstructive sleep apnea patients and in snorers. Sleep 19(9 Suppl):S136–S143. https://doi.org/10.1093/sleep/19.suppl_9.s136
Hussain SF, Irfan M, Waheed Z, Alam N, Mansoor S, Islam M (2014) Compliance with continuous positive airway pressure (CPAP) therapy for obstructive sleep apnea among privately paying patients-a cross sectional study. BMC Pulm Med 14:188. https://doi.org/10.1186/1471-2466-14-188
Schwab RJ, Badr SM, Epstein LJ, Gay PC, Gozal D, Kohler M, Lévy P, Malhotra A, Phillips BA, Rosen IM, Strohl KP, Strollo PJ, Weaver EM, Weaver TE, ATS Subcommittee on CPAP Adherence Tracking Systems (2013) An official American Thoracic Society statement: continuous positive airway pressure adherence tracking systems. The optimal monitoring strategies and outcome measures in adults. Am J Respir Crit Care Med 188(5):613–620. https://doi.org/10.1164/rccm.201307-1282ST
Orth M, Kotterba S, Walther JW, Rasche K, Schultze-Werninghaus G, Duchna HW (2006) Langzeit-Compliance Der CPAP-Therapie–Aktueller stand, Prädiktoren Und Interventionsmöglichkeiten [Long-term compliance of cpap-therapy–update, predictors and interventions]. Pneumologie 60(8):480–484. https://doi.org/10.1055/s-2006-944234
Amfilochiou A, Tsara V, Kolilekas L, Gizopoulou E, Maniou C, Bouros D, Polychronopoulos V (2009) Determinants of continuous positive airway pressure compliance in a group of Greek patients with obstructive sleep apnea. Eur J Intern Med 20(6):645–650. https://doi.org/10.1016/j.ejim.2009.07.004
Galetke W, Anduleit N, Richter K, Stieglitz S, Randerath WJ (2008) Comparison of automatic and continuous positive airway pressure in a night-by-night analysis: a randomized, crossover study. Respiration 75(2):163–169. https://doi.org/10.1159/000097767
Pelletier-Fleury N, Rakotonanahary D, Fleury B (2001) The age and other factors in the evaluation of compliance with nasal continuous positive airway pressure for obstructive sleep apnea syndrome. A Cox’s proportional hazard analysis. Sleep Med 2(3):225–232. https://doi.org/10.1016/s1389-9457(00)00063-0
McArdle N, Devereux G, Heidarnejad H, Engleman HM, Mackay TW, Douglas NJ (1999) Long-term use of CPAP therapy for sleep apnea/hypopnea syndrome. Am J Respir Crit Care Med 159(4 Pt 1):1108–1114. https://doi.org/10.1164/ajrccm.159.4.9807111
Lettieri CJ, Shah AA, Holley AB, Kelly WF, Chang AS, Roop SA, CPAP Promotion and Prognosis-The Army Sleep Apnea Program Trial (2009) Effects of a short course of eszopiclone on continuous positive airway pressure adherence: a randomized trial. Ann Intern Med 151(10):696–702. https://doi.org/10.7326/0003-4819-151-10-200911170-00006
Reeves-Hoche MK, Meck R, Zwillich CW (1994) Nasal CPAP: an objective evaluation of patient compliance. Am J Respir Crit Care Med 149(1):149–154. https://doi.org/10.1164/ajrccm.149.1.8111574
Russo-Magno P, O’Brien A, Panciera T, Rounds S (2001) Compliance with CPAP therapy in older men with obstructive sleep apnea. J Am Geriatr Soc 49(9):1205–1211. https://doi.org/10.1046/j.1532-5415.2001.49238.x
Jacobsen AR, Eriksen F, Hansen RW, Erlandsen M, Thorup L, Damgård MB, Kirkegaard MG, Hansen KW (2017) Determinants for adherence to continuous positive airway pressure therapy in obstructive sleep apnea. PLoS ONE 12(12):e0189614. https://doi.org/10.1371/journal.pone.0189614
Neuzeret PC, Morin L (2017) Impact of different nasal masks on CPAP therapy for obstructive sleep apnea: a randomized comparative trial. Clin Respir J 11(6):990–998. https://doi.org/10.1111/crj.12452
Ebben MR, Oyegbile T, Pollak CP (2012) The efficacy of three different mask styles on a PAP titration night. Sleep Med 13(6):645–649. https://doi.org/10.1016/j.sleep.2012.02.004
McArdle N, Kingshott R, Engleman HM, Mackay TW, Douglas NJ (2001) Partners of patients with sleep apnoea/hypopnoea syndrome: effect of CPAP treatment on sleep quality and quality of life. Thorax 56(7):513–518. https://doi.org/10.1136/thorax.56.7.513
Weaver TE, Grunstein RR (2008) Adherence to continuous positive airway pressure therapy: the challenge to effective treatment. Proc Am Thorac Soc 5(2):173–178. https://doi.org/10.1513/pats.200708-119MG
Weaver TE (2006) Adherence to positive airway pressure therapy. Curr Opin Pulm Med 12(6):409–413
Manthey M (2002) The practice of primary nursing. Creative Health Care Management, Minneapolis
Funding
No funding was received for this research.
Author information
Authors and Affiliations
Contributions
Conceptualization: Carmen Samà, Sandro Longu, Giorgio Bergesio. Investigation: Carmen Samà. Resources: Sandro Longu. Visualization: Carmen Samà, Sandro Longu, Giorgio Bergesio, Francesca Samà, Alessia Faioli. Writing-Original Draft: Carmen Samà, Sandro Longu, Giorgio Bergesio, Francesca Samà, Alessia Faioli. Writing-Review e Editing: Carmen Samà.
Corresponding author
Ethics declarations
Ethics approval
This article does not contain any studies with animals performed by any of the authors.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Consent for publication
All authors have approved the final version for publication.
Conflict of interest
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest, or non-financial interest in the subject matter or materials discussed in this manuscript.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Samà, C., Longu, S., Bergesio, G. et al. Therapeutic adherence in patients with Obstructive Sleep Apnea Syndrome: a retrospective cohort study. Sleep Breath (2024). https://doi.org/10.1007/s11325-024-03097-y
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11325-024-03097-y