
Abstract
Introduction
Obstructive sleep apnea (OSA) is frequently reported among patients with chronic kidney disease resulting in considerable morbidity and mortality. OSA may cause repetitive stimulation of the sympathetic nervous system and elevations in pulmonary artery pressure leading to an elevated risk of cardiac and vascular complications in patients with chronic kidney disease. Furthermore, OSA is associated with progressive worsening of kidney injury and loss of renal function.
Methods
In this systematic review and meta-analysis, we evaluated the effect of renal transplantation on the progression of OSA in patients with end-stage kidney disease.
Results
The meta-analysis included eight studies with a total of 401 patients. Findings showed that kidney transplantation does not lead to a statistically significant effect on the apnea–hypopnea index (MD 2.6 events/hr, 95% CI −3.2 to 8.3, p = 0.21), total sleep time (MD 14.7 min/night, 95% CI −8.4 to 37.8, p = 0.76), sleep efficiency (MD 2.5%, 95% CI −1.4 to 6.3, p = 0.57), slow wave sleep (MD 0.4% of total sleep time, 95% CI −7.5 to 8.4, p = 0.05), and rapid eye movement sleep (MD 0.6% of total sleep time, 95% CI −2.2 to 3.3, p = 0.98). There was no statistically significant effect of kidney transplantation on OSA in patients with chronic renal disease.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The prevalence of chronic kidney disease (CKD), defined by an estimated glomerular filtration rate (eGFR) below 60 mL/min/1.73 m2 or the presence of at least one marker of kidney injury including albuminuria, has been on the rise over the last decades, affecting approximately 500 million adults globally [1, 2]. In addition to its strong association with multiple comorbidities including atherosclerosis, hypertension, cerebrovascular disease dyslipidemia, peripheral vascular disease, and cardiovascular disease and myocardial infarction, CKD is also strongly associated with obstructive sleep apnea (OSA) [3,4,5,6]. The repetitive activation of the sympathetic nervous system and the development of pulmonary artery hypertension which are both common consequences of OSA further elevate the risk of cardiac and vascular complications in patients with CKD [7, 8]. Even though the exact pathophysiological mechanism underlying the elevated risk of OSA in patients with CKD remains controversial, multiple hypothesis including volume overload, compensatory respiratory alkalosis in response to metabolic acidosis and/or uremic toxins have been postulated [8, 9]. In addition, multiple studies have shown an association between OSA-induced nocturnal hypoxemia and kidney injury as well as loss of renal function [10, 11]. Furthermore, central sleep apnea, a potential complication that may mimic OSA and may not always be distinguishable, is common in patients with CKD, especially in individuals receiving renal replacement therapy or those with comorbid congestive heart failure [12, 13]. Our meta-analysis aimed to evaluate the effect of kidney transplantation in the reversal of OSA and its associated complications in patients with end-stage kidney disease (ESKD).
Materials and methods
Guidelines of the Cochrane Collaboration and Meta-analysis of Observational Studies in Epidemiology [14], Quality of Reporting of Meta-Analyses [15], and the Preferred Reporting Items for Systematic Review and Meta-Analyses guidelines [16] have been followed in this meta-analysis.
Literature search
Cochrane Central Register of Controlled Trials (Wiley), Embase (Elsevier), and PubMed/Medline Web of Science databases were used for the literature search in June 2022 with the following keywords and their variations or combinations: “end stage renal disease,” “ESRD,” “ESKD,” “end stage kidney disease,” “hemodialysis,” “chronic kidney disease,” “CKD,” “peritoneal dialysis,” “dialysis,” “renal replacement therapy,” “sleep apnea,” “apnea,” “hypopnea,” “apnea–hypopnea index,” “obstructive sleep apnea,” “kidney transplantation,” “sleep disorder,” “renal transplantation,” and “transplantation.” All the authors have taken part in the assessment of the titles and abstracts the studies independently, and a consensus was achieved after examining and discussing each study in detail. The references were evaluated to not omit any additional study. The full-text evaluation of the studies that remained were performed by the authors after preliminarily eliminating from the titles and abstracts. Furthermore, the chosen studies were assessed according to the inclusion and exclusion criteria of this meta-analysis study which were as follows: any original article (i.e., randomized control trials, prospective cohort, case control, retrospective cohort, and cross-over study) that investigates kidney transplantation on the incidence or prevalence or severity of sleep apnea which is in a peer-reviewed journal in English before June 2022. Studies not including baseline data regarding sleep apnea prior to kidney transplantation or other types of study designs (i.e., case reports, case series, editorials, commentaries review, systematic review and meta-analysis), studies with unpublished data, or inadequate description of the outcomes and missing data were excluded from this meta-analysis study. Figure 1 is summarized the study selection process.

PRISMA flow chart of the study selection process
Quality assessment
The Newcastle–Ottawa Scale was used for evaluating the quality of the studies. The Newcastle–Ottawa Scale consists of three main parts: the selection of study groups, comparability of the groups, and assessment of outcomes with the highest quality of research given nine stars. The quality assessment was conducted with the participation of all authors, and a consensus decision was reached for each study.
Statistical analysis
Review Manager (RevMan) Version 5.4 (The Cochrane Collaboration 2012) was used for statistical analyses [17]. For the continuous outcomes, random-effects model for meta-analysis was used and reported all the values as mean and standard deviation (AHI (events/hr), total sleep time (TST) (min/night), sleep efficiency (%), slow wave sleep (% TST), rapid eye movement (REM) sleep (% TST), and BMI (kg/m2)). When the mean difference and standard deviation were reported for separated groups, we calculated the group’s mean difference and standard deviation by using the RevMan calculator. Standard formulas were used to transform median and interquartile range to mean and standard deviation, if needed [18]. The inconsistencies throughout the individual studies were evaluated via the I2 statistic [19]. An I2 > 50% indicated a large heterogeneity which was not explained by chance. P value < 0.05 was defined as statistically significant.
Results
Our analysis included eight prospective, cohort studies on kidney transplant recipients (Table 1) [5, 20,21,22,23,24,25,26]. A total of 401 patients were included in the meta-analysis (with a minimum of 9 [5] and a maximum of 221 [23]).
Studies evaluated the effect of kidney transplantation on sleep quality by assessing different parameters either measured through polysomnography (PSG) or reported through standardized questionnaires such as the Epworth Sleepiness Scale (ESS). For this analysis, we selected the following parameters: apnea–hypopnea index (AHI in events/hr), TST (min/night), sleep efficiency (%), slow wave sleep (%TST), and REM sleep (%TST). Additionally, an analysis of the BMI, before and after transplantation was performed.
An analysis of the time trend of nocturnal O2 saturation could not be performed, since these data were reported differently throughout the studies: oxygen desaturation index (ODI) in Mallamaci 2020, Rodrigues 2010, and Ogna 2019; minimal O2 saturation in Mallamaci 2020 and Jurado-Gamez 2008, % TST under 90% in Tandukar 2019 and Jurado-Gamez 2008; and mean O2 saturation in Beecroft 2007 and Mahajan 2017.
Apnea–hypopnea index (AHI, events/hr)
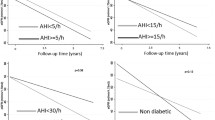
All eight studies [5, 20,21,22,23,24,25,26] reported AHI [27] as the primary indicator for sleep apnea (Fig. 2). AHI was measured through polysomnography (PSG) in all cohorts before and after transplantation. Differences in the final results did not reach statistical significance. Two of the studies [20, 21] divided their cohorts into two groups, specifically apneic and non-apneic groups according to an AHI > 10/h in pre-transplant PSG. Another study [26] selected its cohort from adult patients with ESKD who were on the kidney transplantation waiting list and were screened by pre-transplant PSG, only apneic patients with severe pre-transplantation sleep apnea (AHI ≥ 15/h) who underwent kidney transplantations were reassessed after 6 months (post-transplant) using the same protocol. Thus, we chose to conduct a sub-analysis on the evolution of AHI in these groups (Fig. 3). The result did not reach statistical significance (MD 2.6 events/hr, 95% CI − 3.2–8.3, P = 0.21).

Forest plot of the included studies for apnea–hypopnea index

Forest plot of the included studies for sub-analysis on apnea–hypopnea index
Total sleep time (TST, min/night)
Three studies [20, 22, 26] reported the total sleep time, before and after transplantation (Fig. 4). Differences for these results did not reach statistical significance (MD 14.7 min/night, 95% CI − 8.4–37.8, P = 0.76). There was no heterogeneity in this cohort (I2 = 0%).

Forest plot of the included studies for total sleep time
Sleep efficiency (%)
Sleep efficiency was reported as an outcome in five studies [5, 20, 22, 24, 26] (Fig. 5). Four studies reported an increase in sleep efficiency, with only one study reporting a negative effect of kidney transplantation [22]. Overall, differences in the results did not reach statistical significance (MD 2.5%, 95% CI − 1.4–6.3, P = 0.57).

Forest plot of the included studies for sleep efficiency (%)
Slow wave sleep (% TST)
Three studies [20, 22, 24] reported the time of slow wave sleep, reported to the total sleep time (stages 3 and 4 of the non-REM sleep) (Fig. 6). This analysis showed that kidney transplantation did not influence this parameter (MD 0.4% total sleep time, CI 95% − 7.5–8.4, P = 0.05).

Forest plot of the included studies for slow wave sleep (%total sleep time)
Rapid eye movement sleep (REM, % TST)
Four studies [5, 20, 22, 24] analyzed the five stages of sleep (non-REM, stages 1 to 4, and REM) separately through polysomnography (Fig. 7). While these studies reported an overall increase in total sleep time, there were no significant reports on the increase or decrease of the duration of the different sleep stages after kidney transplantation (MD 0.6% TST, 95% CI − 2.2–3.3, P = 0.98).

Forest plot of the included studies for REM sleep (%total sleep time)
Body mass index (BMI, kg/m2)
Five studies [20, 22, 24,25,26] reported the BMI at baseline and post kidney transplantation (Fig. 8). All reported an increase in BMI after transplantation, confirmed by the overall analysis (MD 1.2 kg/m2, 95% CI 0.2–2.1, P = 0.69). Heterogeneity was absent in this cohort, with an I2 of 0%.

Forest plot of the included studies for body mass index
Discussion
In this meta-analysis which includes eight studies with a total of 401 participants, the effect of kidney transplantation on the progression of sleep apnea in patients with ESKD was assessed. The meta-analysis showed that kidney transplantation does not lead to a statistically significant effect in apnea–hypopnea index, total sleep time, sleep efficiency, slow wave sleep, or REM sleep. It is crucial to emphasize the considerable variation across individual studies. The meta-analysis is the first study evaluating the effect of kidney transplantation on sleep apnea, a highly common comorbidity and cause of morbidity in patients with ESKD.
The associations between ESKD and sleep apnea including its potential underlying pathophysiological mechanism have largely been investigated in multiple pre-clinical and clinical studies without a definitive result. In addition to the traditional risk factors of OSA in the general population including metabolic syndrome, obesity, and anatomical variations of airways, individuals with ESKD are prone to develop obstructive or central sleep apnea as a result of fluid overload. Studies demonstrating the association between internal jugular vein dilatation and sleep apnea in patients with ESKD and attenuation of such findings following nocturnal dialysis support the pathophysiological role of fluid overload in sleep apnea [28, 29]. Similarly, nocturnal rostral fluid shifts and fluid overload were also suggested to contribute to the high risk of sleep apnea in patients with heart failure [29]. In a cross-sectional study conducted on 100 individuals with CKD who were not on renal replacement therapy, fluid overload markers such as serum brain natriuretic peptide levels and the diameter of inferior vena cava were shown to correlate with sleep apnea, independent from the traditional confounding factors [30]. Similar findings have been established in few other clinical studies [27, 31]. Fluid overload may lead to the stimulation of pulmonary irritant receptors causing cycles of hyperventilation and apnea [32]. In addition, the respiratory adaptation to metabolic acidosis and uremia, which are the complications of ESKD, alters chemoreceptor sensitivity and enhances central and peripheral chemoreflexes. These augmented reflexes may impair the stability of ventilation and may predispose to sleep apnea [4, 33]. Obstructive sleep apnea may develop due to neuropathy or myopathy secondary to the complications associated with ESKD such as chronic uremia, which can disrupt the upper airway muscles, and cause compromised upper airway dynamics [4, 33]. Furthermore, the association between sleep apnea and renal function rather appears to be bidirectional. Patients with nocturnal hypoxia have higher risk of renal function decline after controlling for confounders such as diabetes, BMI, age, and heart failure according to a prospective study conducted on 858 patients with a 2 year follow-up period [10]. Another study conducted on 161 patients with stage 3–4 CKD demonstrated that patients with 4% oxygen desaturation index over 15% developed three to four times higher decline in eGFR over a 12-month follow-up period [11].
The current meta-analysis study is significant by being the first meta-analysis investigating the effects of kidney transplantation on sleep parameters in patients with ESKD. However, we appreciate certain limitations to our results. First, the number of total participants is considerably low, with more than half of the participants from single clinical study which affects the generalizability of our results. Second, there was a statistically significant increase in BMI which is a known strong risk factor for sleep apnea. Therefore, the increased BMI in renal transplant patients may undermine the improvements gained from the transplantation procedure and may have prevented the investigated parameters from reaching statistically significance. Furthermore, one reason for AHI to remain similar to baseline despite a higher BMI after kidney transplantation could be the better management of fluid overload. Another explanation could be that the higher BMI might potentially be a result of an increase in muscle mass and not due to fat deposits following renal transplantation, thus, not leading to a change in sleep parameters [34, 35]. Third, considerable variations exist across individual studies regarding the investigated parameters, study design, and patient characteristics all of which limit the evaluation of results. Fourth, potential confounding factors including BMI, anatomical variations, comorbid medical conditions including heart failure and hypertension have not been adequately eliminated or assessed in subgroup analysis of most included studies.
The effects of renal transplantation in improving OSA in patients with ESKD did not reach statistically significant differences.
Data availability
This is not applicable.
References
Mills KT, Xu Y, Zhang W, Bundy JD, Chen CS, Kelly TN et al (2015) A systematic analysis of worldwide population-based data on the global burden of chronic kidney disease in 2010. Kidney Int 88(5):950–957
Charles C, Ferris AH (2020) Chronic kidney disease. Prim Care 47(4):585–595
Sharma S, Sarnak MJ (2017) Epidemiology: the global burden of reduced GFR: ESRD, CVD and mortality. Nat Rev Nephrol 13(8):447–448
Zoccali C, Roumeliotis S, Mallamaci F (2021) Sleep apnea as a cardiorenal risk factor in CKD and renal transplant patients. Blood Purif 50(4–5):642–648
Jurado-Gámez B, Martin-Malo A, Rodriguez-Benot A, Muñoz-Cabrera L, CosanoPovedano A, Aljama P (2008) Kidney transplantation improves sleep-related breathing in hemodialysis patients. Blood Purif 26(6):485–490
Tanriover C, Ucku D, Akyol M et al (2022) Potential use of SGLT-2 inhibitors in obstructive sleep apnea: a new treatment on the horizon. Sleep Breath. https://doi.org/10.1007/s11325-022-02606-1
Zoccali C (2000) Sleep apnoea and nocturnal hypoxaemia in dialysis patients: mere risk-indicators or causal factors for cardiovascular disease? Nephrol Dial Transplant 15(12):1919–1921
Moradzadeh M, Mirmohammadkhani M, Tamadon MR, Mansori K, Malek F (2021) Prevalence of sleep apnea and its associated factors in chronic kidney disease patients. Tanaffos 20(2):116–125
Jhamb M, Unruh ML (2012) Volume overload as a mechanism for obstructive sleep apnea in CKD? Nephrol Dial Transplant 27(4):1291–1293
Ahmed SB, Ronksley PE, Hemmelgarn BR, Tsai WH, Manns BJ, Tonelli M et al (2011) Nocturnal hypoxia and loss of kidney function. PLoS ONE 6(4):e19029
Sakaguchi Y, Hatta T, Hayashi T, Shoji T, Suzuki A, Tomida K et al (2013) Association of nocturnal hypoxemia with progression of CKD. Clin J Am Soc Nephrol 8(9):1502–1507
Dharia SM, Unruh ML, Brown LK (2015) Central sleep apnea in kidney disease. Semin Nephrol 35(4):335–346
Nigam G, Pathak C, Riaz M (2016) A systematic review of central sleep apnea in adult patients with chronic kidney disease. Sleep Breath 20(3):957–964
Brooke BS, Schwartz TA, Pawlik TM (2021) MOOSE reporting guidelines for meta-analyses of observational studies. JAMA Surg 156(8):787–788
McDonough PG (2003) Quorum guidelines for meta-analyses. Fertil Steril 80(1):228
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339:b2535
Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327(7414):557–560
Wan X, Wang W, Liu J, Tong T (2014) Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol 14:135
DerSimonian R, Kacker R (2007) Random-effects model for meta-analysis of clinical trials: an update. Contemp Clin Trials 28(2):105–114
Beecroft JM, Zaltzman J, Prasad R, Meliton G, Hanly PJ (2007) Impact of kidney transplantation on sleep apnoea in patients with end-stage renal disease. Nephrol Dial Transplant 22(10):3028–3033
Lee JJ, Kim GS, Kim JA, Kim SJ, Kang JG, Kim GH et al (2011) Improvement of sleep-related breathing disorder in patients with end-stage renal disease after kidney transplantation. Clin Transplant 25(1):126–130
Mahajan S, Gupta K, Sinha S, Malhotra A, Mahajan S (2018) Effect of kidney transplantation on sleep-disordered breathing in patients with end stage renal disease: a polysomnographic study. Sleep Med 45:140–145
Mallamaci F, Tripepi R, D’Arrigo G, Panuccio V, Parlongo G, Caridi G et al (2020) Sleep-disordered breathing and 24-hour ambulatory blood pressure monitoring in renal transplant patients: longitudinal study. J Am Heart Assoc 9(13):e016237
Rodrigues CJ, Marson O, Togeiro SM, Tufik S, Ribeiro AB, Tavares A (2010) Sleep-disordered breathing changes after kidney transplantation: a polysomnographic study. Nephrol Dial Transplant 25(6):2011–2015
Tandukar S, Hou S, Yabes J, Ran X, Fletcher M, Strollo P et al (2019) Does kidney transplantation affect sleep and fatigue in patients with kidney disease? Transplant Direct 5(6):e461
ForniOgna V, Ogna A, Haba-Rubio J, Nowak G, Venetz JP, Golshayan D et al (2020) Impact of kidney transplantation on sleep apnea severity: a prospective polysomnographic study. Am J Transplant 20(6):1659–1667
Lyons OD, Inami T, Perger E, Yadollahi A, Chan CT, Bradley TD (2017) The effect of fluid overload on sleep apnoea severity in haemodialysis patients. Eur Respir J 49(4):1601789
Elias RM, Chan CT, Paul N, Motwani SS, Kasai T, Gabriel JM et al (2013) Relationship of pharyngeal water content and jugular volume with severity of obstructive sleep apnea in renal failure. Nephrol Dial Transplant 28(4):937–944
Elias RM, Bradley TD, Kasai T, Motwani SS, Chan CT (2012) Rostral overnight fluid shift in end-stage renal disease: relationship with obstructive sleep apnea. Nephrol Dial Transplant 27(4):1569–1573
Tanaka A, Inaguma D, Ito E, Kamegai N, Kato A, Mizutani M et al (2017) Factors associated with severity of sleep apnoea syndrome in patients with chronic kidney disease. Acta Cardiol 72(4):440–445
Harmon RR, De Lima JJG, Drager LF, Portilho NP, Costa-Hong V, Bortolotto LA et al (2018) Obstructive sleep apnea is associated with interdialytic weight gain and increased long-term cardiovascular events in hemodialysis patients. Sleep Breath 22(3):721–728
Anastassov GE, Trieger N (1998) Edema in the upper airway in patients with obstructive sleep apnea syndrome. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 86(6):644–647
Voulgaris A, Bonsignore MR, Schiza S, Marrone O, Steiropoulos P (2021) Is kidney a new organ target in patients with obstructive sleep apnea? Research priorities in a rapidly evolving field. Sleep Med 86:56–67
Dienemann T, Ziolkowski SL, Bender S, Goral S, Long J, Baker JF et al (2021) Changes in Body composition, muscle strength, and fat distribution following kidney transplantation. Am J Kidney Dis 78(6):816–825
Vieira NM, Silva MZC, Costa FL, Presti PT, Silva TM, Silveira LM et al (2021) Nutritional parameters in early and late kidney transplantation. Transplant Proc 53(7):2162–2167
Author information
Authors and Affiliations
Contributions
Mehmet Kanbay, Sidar Copur, Carina Ureche, and Alexandra Covic contributed substantially to the conception or design of the work. Carina Ureche, Alexanda Covic, and Mehmet Kanbay contributed substantially to acquisition, analysis, or interpretation of data. Mehmet Kanbay, Sidar Copur, Carina Ureche, Bugra H. Esen, and Cem Tanriover drafted the manuscript. Mehmet Kanbay, Adrian Covic, Carina Ureche, Alexandra Covic, Cem Tanriover, Asiye Kanbay, and Sidar Copur were involved in the revision of the manuscript for important intellectual content.
Corresponding author
Ethics declarations
Ethical approval
This is not applicable.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kanbay, M., Ureche, C., Copur, S. et al. Kidney transplantation: a possible solution to obstructive sleep apnea in patients with end-stage kidney disease. Sleep Breath 27, 1667–1675 (2023). https://doi.org/10.1007/s11325-023-02803-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11325-023-02803-6