
Abstract
Purpose
Obstructive sleep apnea (OSA) can impair cognition. Continuous positive airway pressure (CPAP) is a recommended treatment for OSA but its effectiveness on cognitive improvement is uncertain, a finding which may be biased by various durations and adherence to treatment with CPAP. In a meta-analysis assessing high-quality randomized controlled trials (RCTs), we estimated whether or not CPAP benefits cognition in patients with OSA.
Methods
PRISMA criteria were followed in the performance of this meta-analysis. The weighted mean difference (WMD) and 95% confidence interval (CI) of six neuropsychological scores covering eight cognitive domains were used to evaluate the benefit between CPAP and non-CPAP interventions. Subgroups of different therapeutic durations and adherence, which were divided into short-term (< 8 weeks) and long-term (≥ 12 weeks) durations, and poor (nighttime < 4 h/night) and good (nighttime ≥ 4 h/night) adherence were also analyzed.
Results
Among 16 RCTs, 1529 participants with OSA were included. Comparing the CPAP group and the control group for all treatment durations and adherence, a mild improvement for digit span forward which reflected short-term memory was observed (WMD[95%CI] = 0.67[0.03,1.31], p = 0.04). Trail making test-part B, which reflected executive function was improved for participants with OSA who had good adherence to CPAP (WMD[95%CI] = − 6.24[− 12.60,0.12], p = 0.05). Patients with OSA who received short-term CPAP treatment (WMD[95%CI] = − 7.20[− 12.57, − 1.82], p = 0.009) had a significant improvement in executive function when compared with controls. There was no statistical difference for all scales between long-term (≥ 12 weeks) CPAP treatment group and control group.
Conclusion
The effectiveness of CPAP on cognitive improvement in patients with OSA is limited, although good adherence to CPAP can mildly benefit executive function with short-term effectiveness.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Obstructive sleep apnea (OSA) is a common sleep disorder and affects nearly one billion people worldwide aged 30–69 years [1]. Also, the prevalence of cognitive impairment and dementia is expected to rise over the next few decades due to increased life expectancy of patients [2]. An estimated 6.2 million Americans aged 65 and older currently have Alzheimer’s disease (AD), and that number could grow to 13.8 million by 2060 [3]. Therefore, both conditions have placed a heavy burden on public health [2, 4]. Epidemiological evidence from prospective and cross-sectional studies suggests that OSA is a risk factor for cognitive decline, with a 4.7–13.7% higher prevalence of cognitive impairment in adults with OSA than those without OSA [5, 6]. According to neuropsychological evaluation, OSA can cause a relatively consistent pattern of deficits in domains of attention, episodic memory, working memory, and executive function [7,8,9]. Further, the longer OSA left untreated, the higher risk of cognitive impairment and dementia, and potentially the earlier the age of onset of AD [10]. Fortunately, unlike risk factors of aging, genetic susceptibility, etc., OSA itself is modifiable, which proposes an alternative option for early prevention in cognitive impairment [11].
Continuous positive airway pressure (CPAP) is a recommended treatment for patients with OSA [12], which could effectively reduce hypoxia parameters like apnea hypopnea index (AHI, which reflects the severity of OSA) and relieve symptoms of sleep disturbance and daytime sleepiness [10, 13]. CPAP could also improve the comorbid conditions of glycemic control, insulin resistance, heart failure, etc., in patients with OSA [14,15,16]. However, the efficacy of CPAP on cognitive improvement in patients with OSA is still uncertain. The conclusions reached by different studies are inconsistent because of the diversity of impaired cognitive domains and neuropsychological scales applied, as well as the difference in the adherence and durations of CPAP in patients with OSA. Based on the published randomized controlled trials (RCTs) in this field, several meta-analysis studies have been conducted to assess the efficacy of CPAP on improving OSA-related cognitive impairment [13, 17, 18]. Labarca G. et al. indicated CPAP only had a slight improvement in short-term memory and executive function in elderly patients with OSA [13]. Kylstra WA. et al. suggested CPAP could improve the performance in the domains of attention and executive function but the benefit was modest [17]. Jiang X. et al. pointed out CPAP had a potential positive effect in cognitive domains such as attention, executive function, orienting places, and psychomotor/cognitive processing speed, although the results of meta-analysis lacked statistical significance [18]. Among these studies, the effects of CPAP on various cognitive domains and stratified population have been elaborately assessed, but a key missing point is that the therapeutic duration and compliance of CPAP varied across studies.
In fact, studies have pointed out the importance of a more in-depth assessment of the therapeutic duration and adherence to CPAP for cognitive improvement in patients with OSA, as they are critical factors in evaluating the treatment effectiveness [17, 19]. Also, the efficacy of CPAP in OSA with comorbidities of hypertension, inflammatory reaction, abnormal glycolipid metabolism, and heart failure was closely associated with the adherence and duration of CPAP [16, 20, 21]. CPAP improved cardiac function in heart failure patients with co-morbid OSA, but the magnitude of the improvement was related to the duration of nighttime use rather than the duration of treatment [16]. Short-term (< 3 months) CPAP treatment could modestly reduce the level of C-reactive protein, tumor necrosis factor-α, fasting blood glucose, and low-density lipoprotein in patients with OSA, while long-term (≥ 3 months) CPAP treatment slightly decreased the level of high-density lipoprotein and total cholesterol [20]. Similarly, therapeutic duration and adherence to CPAP may have different effectiveness on improving OSA-related cognitive impairment, including memory, attention, visuospatial learning, executive function, and motor performance according to previous original studies [7, 19, 22, 23]. However, these two key points have not been taken into account in the current meta-analysis. Thus, it is difficult to determine the effect of CPAP on cognitive improvement in OSA if only combined different adherence and treatment durations of CPAP together for analysis.
Therefore, to answer this question, we estimated whether or not the cognitive improvement in patients with OSA varied depending on the therapeutic duration and adherence to CPAP, and we further studied the improvement in different cognitive domains. We found only patients with OSA who had good adherence (nighttime duration ≥ 4 h/night) to CPAP had a slight improvement in executive function compared with corresponding control group. There was a trend of improvement in other cognitive domains, although the results lacked statistical difference. Furthermore, patients with OSA who received short-term CPAP (< 8 weeks) could significantly improve the executive function, whereas those who received long-term CPAP (≥ 12 weeks) had no apparent cognitive benefit.
Method
Inclusion and exclusion criteria
Based on the principal of PICOS (participant, intervention, control, outcome, and study design), the inclusive and exclusive criteria were set:
-
(i)
Participants: all participants were diagnosed as OSA based on the polysomnography (PSG) or home sleep apnea test (HSAT); parameters of Apnea Hypopnea Index (AHI) > 5 events/h or Respiratory Disturbance Index (RDI) > 5 events/h; besides, all included OSA patients had no neurological and other diseases which would affect cognition, like AD.
-
(ii)
Intervention: patients with OSA treated with CPAP were included in the CPAP group, while patients with OSA received placebo, sham CPAP, conservative treatment, and other responsive non-CPAP interventions were included in the control group.
-
(iii)
Controls: all controls were reported the same diagnosis as OSA but had non-CPAP interventions.
-
(iv)
Outcomes: primary outcomes are (1) scores of responsive neuropsychological scales for specific cognitive domain at baseline and post interventions; (2) data format shown as or converted to mean and standard deviation (mean ± SD); (3) each neuropsychological scale must be studied in more than three studies before quantitative analysis. Also, daytime sleepiness conditions from two groups were extracted as secondary outcome.
-
(v)
Study design: randomized controlled trial (RCT).
Search strategy
Databases (Embase, Web of Science, PubMed, and Cochrane) were used to retrieve studies on the cognitive improvement effect of CPAP in patients with OSA up to August 22, 2021 at the first stage; also, we have updated the searching up to January 22, 2022. The idea of search term design includes three aspects: cognition and its sub-domains, OSA disease, and CPAP intervention. The searching strategy for different databases was attached in Supplemental Table 1.
Data extraction
For all included publications, two researchers independently extracted required data, including the publication year, first author, region, number of participants, age (years, mean ± SD), diagnosis information, intervention details for both groups, and the outcomes.
For primary outcomes, we extracted the results for responsive neuropsychological scales (mean ± SD) from eight cognitive domains: sensation, perception, motor skills and construction, attention and concentration, memory, executive functioning, processing speed, and language/verbal skills. Trail making test-part A (TMT-A) for visuomotor and information processing speed; trail making test-part B (TMT-B) for executive function and the speed of information processing; digit span (DS) for attention and working memory; digital symbol substitution (DSS) for perceptual and graphomotor speed; digit span forward (DSF) for short-term memory; digit span backward (DSB) for working memory [24].
As for secondary outcome, we extracted scores of Epworth sleepiness score (ESS) to measure the sleepiness and tracked their changes in different groups. All extracted data were shown in Supplemental Table 2.
Literature quality evaluation
The Jadad scale was used to assess the quality of included RCT studies [25]. It is mainly composed of four aspects: generation of random sequence (selection bias), blind assignment and blinding of all study participants (execution bias), blind method of result evaluation (observation bias), and result data completeness (loss to follow-up bias); with a total score of 7, score of 1–3 points are considered low quality and 4–7 are considered high quality.
Data analysis
Data analysis was performed by Review Manager 5.3 software. Weighted mean difference (WMD) and its 95% confidence interval (CI) were used to analyze the efficacy of CPAP on cognition and secondary outcome of sleepiness by comparing the mean differences of each evaluating scales between CPAP and control group. For results with the heterogeneity I2 < 50%, we used the fixed effect model for meta-analysis; otherwise, we performed the random effects model. p value < 0.05 was considered statistically different for WMD.
Firstly, we compared the baseline WMD of each outcome, which was used as comparable evidence between the two groups. Then, we analyzed the WMD for each test after different interventions. Based on the included RCTs, we compared the primary and secondary outcomes between CPAP group and control group by combining all the therapeutic durations and compliance at first. Next, we performed subgroup analysis to assess the effects of therapeutic duration and compliance on CPAP efficacy by comparing the outcomes between CPAP group and control group in different subgroups based on therapeutic duration and nighttime duration, respectively.
In addition, sensitivity analyses were performed by sequentially excluding one study and examining the change in pooled effect size. Also, publication bias for the results was presented as the whether the funnel plots were symmetric or not.
Results
Characteristics for all included publications
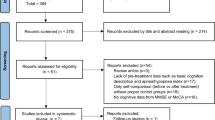
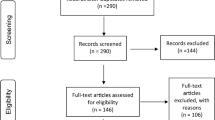
According to our inclusive and exclusive criteria, we included 16 RCTs for pooled analysis (Fig. 1). The characteristics of these publications were shown in Table 1 and Supplemental Table 2. In summary, 16 RCTs included a total of 1529 OSA participants with a mean age distribution of 44.0–75.6 years. The severity parameter AHI/RDI (mean, events/night) range from 10.0 to 61.2 for all participants. The mean usage time of CPAP was 2.4–6.1 h per night. Additionally, the treatment duration varied widely. Nine studies had treatment duration ranging from 1 to 8 weeks, and the other 7 studies had treatment duration ranging from 12 to 48 weeks (two of the studies included two follow-up visits at different therapeutic durations, which were used as two datasets for quantitative analysis). Compared with CPAP group, non-CPAP interventions included active and passive interventions. Active interventions included conservative treatment, best supportive care, mandibular repositioning splint (MRS), and habitual treatment. Passive interventions included placebo, sham CPAP, and oral placebo.

The workflow for screening publications according to inclusion and exclusion criteria
In terms of the quality of publications assessed by Jadad scale, eight studies were rated 4-7 and the other 8 studies were rated 2-3. Because it was difficult to achieve double-blind between CPAP and control group, and some studies did not describe the method of randomization, so the Jadad scores of some studies were relatively low compared with standard scale.
CPAP benefit for cognition improvement in OSA is limited
For primary outcomes, we analyzed scales of TMT-A, TMT-B, DS, DSB, DSS, and DSF, which reflected the cognitive domains of sensation, attention, motor skills and construction, memory, executive functioning, and processing speed. Firstly, we compared the baseline for each scale and found there were no significant differences in TMT-A (p = 0.13), TMT-B (p = 0.43), DSF (p = 0.82), DSS (p = 0.10), and DSB (p = 0.27) between CPAP and control groups (Table 2), supporting it was comparable for the following analysis. Nevertheless, we observed a lower baseline score of DS in the CPAP group than in the control group (WMD[95%CI] = − 0.67[− 1.16, − 0.18], p = 0.007), which needs to be considerate for interpreting following results. Then, we compared the cognitive improvement in two groups by combining all the therapeutic durations and compliance and only observed a mild improvement in DSF in CPAP group (WMD[95%CI] = 0.67[0.03, 1.31], p = 0.04). There were no statistical differences in TMT-A (p = 0.07), TMT-B (p = 0.10), DS (p = 0.71), DSS (p = 0.24), and DSB (p = 0.20) between two groups (Table 2, Supplemental Fig. 1).
Next, we analyzed the effectiveness of CPAP with different nighttime durations, which can also be defined as the usage time of CPAP per night (Table 3, Supplemental Fig. 1). We analyzed the data of two subgroups (nighttime duration < 4 h/night which reflected poor compliance and ≥ 4 h/night which reflected good compliance) and found that only TMT-B in patients with OSA who received CPAP nighttime duration ≥ 4 h/night had a trend of improvement, although the result lacked significant difference (WMD[95%CI] = − 6.24[− 12.60,0.12], p = 0.05) compared with controls. There were no statistical differences in DSF (p = 0.28), TMT-A (p = 0.14), DS (p = 0.80), DSS (p = 0.58), and DSB (p = 0.18) between two groups. Besides, there were no statistical differences in TMT-B (p = 0.63) and DSS (p = 0.15) in patients with OSA who received CPAP nighttime duration < 4 h/night compared with controls.
Further, we also analyzed the effectiveness of CPAP with different therapeutic durations, which were divided into short-term (< 8 weeks) and long-term (≥ 12 weeks) subgroups. As shown in Table 4 and Supplemental Fig. 1, we observed a significant improvement in TMT-B in participants with OSA who received short-term CPAP compared with corresponding control group (WMD[95%CI] = − 7.20[− 12.57, − 1.82], p = 0.009). However, there were no significant differences in other cognitive tests, including DSS (p = 0.82) and TMT-A (p = 0.11) between the two groups. As for the effectiveness of long-term CPAP, there were no significant differences in all cognitive tests, including TMT-B (p = 0.50), DSS (p = 0.24), and DSB (p = 0.27).
Therapeutic effects of CPAP on secondary outcomes
For secondary outcomes, we focused on sleepiness by measured ESS. Based on the comparable baseline scores of ESS (p = 0.70), we observed that the scores of ESS (WMD[95%CI] = − 2.93[− 4.18, − 1.69], p < 0.00001) in CPAP group were lower than control groups (Table 2). For subgroup analysis of different nighttime durations (Table 3), the score of ESS had a significant improvement in both of nighttime duration < 4 h/night (WMD[95%CI] = − 2.60 [− 5.11, − 0.09], p = 0.0002) and ≥ 4 h/night (WMD[95%CI] = − 2.97[− 4.67, − 1.27], p = 0.0006) subgroups. Then, as shown in Table 4, we perform the subgroup analysis of different therapeutic durations and found the significant improvement in ESS in both of short-term (WMD[95%CI] = − 3.64 [− 5.65, − 1.63], p = 0.0004) and long-term (WMD[95%CI] = − 2.01[− 3.44, − 0.58], p = 0.006) CPAP treatment groups.
Sensitivity analysis and publication bias analysis
As for sensitivity analysis, there was no significant change in overall effect size for most cognitive tests, except for the long-term subgroup of DSB. After removing study of Barnes M et al. 2004 [31], a significant difference could be found between CPAP and control group. This may be due to the high dropout rate (30%) of this study compared with other studies.
For the publication bias analysis, we did not notice any obvious asymmetry from all funnel plots (Supplemental Fig. 2), indicating that there was no obvious publication bias in the analysis.
Discussion
Currently, the effectiveness of CPAP on OSA-related cognitive damage is controversial. A main point is inconsistent adherence (nighttime duration) and therapeutic duration of CPAP in those published RCTs, making it difficult to assess the efficacy of CPAP on cognitive improvement. By comparing cognitive tests between CPAP and none-CPAP interventions in subgroups of different adherence and therapeutic durations, we found that only patients with OSA who received longer nighttime duration (indicating good adherence) can mildly improve executive function reflected by the score of TMT-B. We also found that CPAP could only benefit for executive function in short-term with no long-term benefit in all cognitive domains. Our results indicated that the effectiveness of CPAP on cognitive improvement in OSA was limited, and further researches of impairment mechanism and treatment strategy were needed.
Our results indicated that the effectiveness of longer nighttime usages of CPAP on improving cognition in OSA is limited. First, we observed that, even with good compliance to CPAP treatment (≥ 4 h/night), there was only slight improvement in executive function tested by TMT-B scale in CPAP group in comparison with non-CPAP treatment. Our conclusion was consistent with the previous meta-analysis which indicated that nighttime duration of 4.5 h/night CPAP treatment could improve the executive function but the benefit was modest [17]. Olaithe, M.et al. also pointed out executive function could be improved when received an average nighttime duration of 5.34 h/night CPAP treatment in patients with OSA [41]. Further, there was no any significant benefits for other studied cognitive domains with long nighttime usage even though the trends were improved. These findings were consistent with previous studies which only observed mild/null improvement from CPAP in several cognitive domains for OSA patients [13, 18, 42]. Besides, we failed to find significant improvement in short-term memory evaluated by DSF score in both of good and poor compliance subgroups, although there was significant improvement in short-term memory when we analyzed all data together with different compliance. This result may be due to some studies did not provide compliance data and were excluded when we conducted the subgroup analysis. Dalmases M. et al. [22] observed a significant improvement in short-term memory in patients with OSA with an average nighttime duration of 6 h/night CPAP treatment, while Kylstra WA. et al. pointed out that patients with OSA who received an average nighttime duration of 4.5 h/night CPAP treatment had no significant improvement in short-term memory [17]. Thus, further studies are still needed to estimate whether extending the nighttime use of CPAP will show better cognition in short-term memory.
In addition, our results also indicated that the effectiveness of CPAP therapeutic duration on improving cognition in OSA is limited. First, we found that only executive function evaluated by TMT-B could be improved with short-term CPAP treatment (< 8 weeks), while such benefit was disappeared in subgroup of long-term CPAP treatment (≥ 12 weeks). Kushida, C. A., et al. found executive function could be improved when patients with OSA received 2 months of CPAP treatment, but this benefit disappeared when they received 6 months of CPAP treatment [43]. Further, we failed to find significant improvement in other assessed cognitive domains in long-term CPAP treatment subgroup. Therefore, the benefit from CPAP to executive function is temporary since long-term CPAP treatment had no apparent benefit.
Intermittent hypoxemia and sleep fragmentation are the most important pathophysiological mechanisms of OSA, which may participate in cognitive impairment in OSA [44]. The prolonged hypoxemia may lead to neurodegeneration in the hippocampus and the prefrontal cortex, which are associated with impairment of executive function and memory [44, 45]. Sleep fragmentation can lead to the deposition of toxic metabolites in the brain, resulting in pathological changes similar to AD [46]. Studies also have shown that sleep fragmentation was associated with poor performance on cognitive functions such as attention and vigilance [47]. It was supposed that CPAP might alleviate cognitive impairment by reducing the hypoxia damage and sleep disturbances [48]. Nevertheless, the observed limited improvement in our analysis suggested there are other probable mechanisms associated with cognitive impairment which cannot improve by CPAP, like the degeneration and death of neurons and the dysfunction of the blood–brain barrier [49, 50]. In addition, the shared genetic factors like allele e4 of APOE, elevated inflammation proteins of C-reaction protein, and tumor necrosis factor-α between OSA and cognitive impairment were also worth to be studied in the future [51,52,53,54].
In this study, we used six neuropsychological scales covering eight cognitive domains to thoroughly assess the effects of CPAP on cognition based on different therapeutic durations and compliance. Besides, we only included patients without comorbidity of neurological disease (e.g., Parkinson’s disease (PD), AD, and stroke), which had advantages of eliminating the impact of other comorbidities on cognitive assessment. Additionally, we used WMD rather than standardized mean difference (SMD) to analyze the objective efficacy of CPAP on cognitive improvement to reduce the exaggerated effect.
There are limitations with the current study. First, individual data such as age, severity of OSA, and adherence to CPAP were limited. Thus, we could not adjust for those variables as covariates. Second, some estimation tools for cognition changes in specific domains may be lacking, which makes it difficult to describe the therapeutic effect of those domains. Third, there was no washout period in some of the random crossover studies, which may lead to overlapping effects of different interventions.
In conclusion, good adherence to CPAP can mildly benefit executive function, which was improved with short-term CPAP treatment while such benefit disappeared with long-term CPAP intervention. Overall, the effectiveness of CPAP on cognitive improvement in OSA is limited.
Data availability
The authors confirm that the data supporting the findings of this study are available within the article and its Supplementary materials.
References
Benjafield AV, Ayas NT, Eastwood PR et al (2019) Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med 7(8):687–698
Ganguli M, Albanese E, Seshadri S et al (2018) Population neuroscience: dementia epidemiology serving precision medicine and population health. Alzheimer Dis Assoc Disord 32(1):1–9
Alzheimer’s disease facts and figures (2021) Alzheimers Dement 17(3):327–406
Jennum P, Rejkjaer-Knudsen M, Ibsen R et al (2020) Long-term health and socioeconomic outcome of obstructive sleep apnea in children and adolescents. Sleep Med 75:441–447
Shieu MM, Dunietz GL, Paulson HL et al (2022) The association between obstructive sleep apnea risk and cognitive disorders: a population-based study. J Clin Sleep Med 18(4):1177–1185
Yaffe K, Laffan AM, Harrison SL et al (2011) Sleep-disordered breathing, hypoxia, and risk of mild cognitive impairment and dementia in older women. JAMA 306(6):613–619
Ferini-Strambi L, Baietto C, Di Gioia MR et al (2003) Cognitive dysfunction in patients with obstructive sleep apnea (OSA): partial reversibility after continuous positive airway pressure (CPAP). Brain Res Bull 61(1):87–92
Bédard MA, Montplaisir J, Richer F et al (1991) Nocturnal hypoxemia as a determinant of vigilance impairment in sleep apnea syndrome. Chest 100(2):367–370
Mathieu A, Mazza S, Décary A et al (2008) Effects of obstructive sleep apnea on cognitive function: a comparison between younger and older OSAS patients. Sleep Med 9(2):112–120
Bucks RS, Olaithe M, Rosenzweig I et al (2017) Reviewing the relationship between OSA and cognition: where do we go from here? Respirology 22(7):1253–1261
Patil SP, Ayappa IA, Caples SM et al (2019) Treatment of adult obstructive sleep apnea with positive airway pressure: an American academy of sleep medicine clinical practice guideline. J Clin Sleep Med 15(2):335–343
Gottlieb DJ, Punjabi NM (2020) Diagnosis and management of obstructive sleep apnea: a review. JAMA 323(14):1389–1400
Labarca G, Saavedra D, Dreyse J et al (2020) Efficacy of CPAP for improvements in sleepiness, cognition, mood, and quality of life in elderly patients with OSA: systematic review and meta-analysis of randomized controlled trials. Chest 158(2):751–764
Martinez-Ceron E, Barquiel B, Bezos AM et al (2016) Effect of continuous positive airway pressure on glycemic control in patients with obstructive sleep apnea and type 2 diabetes. A randomized clinical trial. Am J Respir Crit Care Med 194(4):476–85
Abuzaid AS, Al Ashry HS, Elbadawi A et al (2017) Meta-analysis of cardiovascular outcomes with continuous positive airway pressure therapy in patients with obstructive sleep apnea. Am J Cardiol 120(4):693–699
Lin R, Yi M, Yan W et al (2022) Positive airway pressure therapy in heart failure patients comorbid with obstructive sleep apnea: cardiovascular outcomes and nighttime-duration effect. Eur J Clin Invest 31:e13821
Kylstra WA, Aaronson JA, Hofman WF et al (2013) Neuropsychological functioning after CPAP treatment in obstructive sleep apnea: a meta-analysis. Sleep Med Rev 17(5):341–347
Jiang X, Wang Z, Hu N et al (2021) Cognition effectiveness of continuous positive airway pressure treatment in obstructive sleep apnea syndrome patients with cognitive impairment: a meta-analysis. Exp Brain Res 239(12):3537–3552
Wang G, Goebel JR, Li C et al (2020) Therapeutic effects of CPAP on cognitive impairments associated with OSA. J Neurol 267(10):2823–2828
Wang Y, Lin YN, Zhang LY et al (2022) Changes of circulating biomarkers of inflammation and glycolipid metabolism by CPAP in OSA patients: a meta-analysis of time-dependent profiles. Ther Adv Chronic Dis 13:20406223211070920
Sanchez-de-la-Torre M, Gracia-Lavedan E, Benitez ID et al (2022) Long-term Effect of OSA and CPAP Treatment on Blood Pressure in Patients with Acute Coronary Syndrome. Ann Am Thorac Soc. https://doi.org/10.1513/AnnalsATS.202203-260OC
Dalmases M, Sole-Padulles C, Torres M et al (2015) Effect of CPAP on cognition, brain function, and structure among elderly patients with OSA: a randomized pilot study. Chest 148(5):1214–1223
Joyeux-Faure M, Naegele B, Pepin JL et al (2016) Continuous positive airway pressure treatment impact on memory processes in obstructive sleep apnea patients: a randomized sham-controlled trial. Sleep Med 24:44–50
Harvey PD (2019) Domains of cognition and their assessment. Dialogues Clin Neurosci 21(3):227–237
Clark HD, Wells GA, Huët C et al (1999) Assessing the quality of randomized trials: reliability of the Jadad scale. Control Clin Trials 20(5):448–452
Ponce S, Pastor E, Orosa B et al (2019) The role of CPAP treatment in elderly patients with moderate obstructive sleep apnoea: a multicentre randomised controlled trial. Eur Respir J 54(2):1900518. https://doi.org/10.1183/13993003.00518-2019
Wan Y, Zhao F, Liu L et al (2018) Influence of continuous positive airway pressure on sleep status, neuropsychological characteristics in patients with stroke combined with obstructive sleep apnea syndrome [Article]. Chin J Neurol 51(4):256–262
Rosenzweig I, Glasser M, Crum WR et al (2016) Changes in neurocognitive architecture in patients with obstructive sleep apnea treated with continuous positive airway pressure. EBioMedicine 7:221–229
Martinez-Garcia MA, Chiner E, Hernandez L et al (2015) Obstructive sleep apnoea in the elderly: role of continuous positive airway pressure treatment. Eur Respir J 46(1):142–151
McMillan A, Bratton DJ, Faria R et al (2014) Continuous positive airway pressure in older people with obstructive sleep apnoea syndrome (PREDICT): a 12-month, multicentre, randomised trial. Lancet Respir Med 2(10):804–812
Barnes M, McEvoy RD, Banks S et al (2004) Efficacy of positive airway pressure and oral appliance in mild to moderate obstructive sleep apnea. Am J Respir Crit Care Med 170(6):656–664
Engleman HM, McDonald JP, Graham D et al (2002) Randomized crossover trial of two treatments for sleep apnea/hypopnea syndrome: continuous positive airway pressure and mandibular repositioning splint. Am J Respir Crit Care Med 166(6):855–859
Montserrat JM, Ferrer M, Hernandez L et al (2001) Effectiveness of CPAP treatment in daytime function in sleep apnea syndrome: a randomized controlled study with an optimized placebo. Am J Respir Crit Care Med 164(4):608–613
Monasterio C, Vidal S, Duran J et al (2001) Effectiveness of continuous positive airway pressure in mild sleep apnea-hypopnea syndrome. Am J Respir Crit Care Med 164(6):939–943
Bardwell WA, Ancoli-Israel S, Berry CC et al (2001) Neuropsychological effects of one-week continuous positive airway pressure treatment in patients with obstructive sleep apnea: a placebo-controlled study. Psychosom Med 63(4):579–584
Barbe F, Mayoralas LR, Duran J et al (2001) Treatment with continuous positive airway pressure is not effective in patients with sleep apnea but no daytime sleepiness: a randomized, controlled trial. Ann Intern Med 134(11):1015–23
Engleman HM, Kingshott RN, Wraith PK et al (1999) Randomized placebo-controlled crossover trial of continuous positive airway pressure for mild sleep Apnea/Hypopnea syndrome. Am J Respir Crit Care Med 159(2):461–467
Engleman HM, Martin SE, Kingshott RN et al (1998) Randomised placebo controlled trial of daytime function after continuous positive airway pressure (CPAP) therapy for the sleep apnoea/hypopnoea syndrome. Thorax 53(5):341–345
Engleman HM, Martin SE, Deary IJ et al (1997) Effect of CPAP therapy on daytime function in patients with mild sleep apnoea/hypopnoea syndrome. Thorax 52(2):114–119
Engleman HM, Martin SE, Deary IJ et al (1994) Effect of continuous positive airway pressure treatment on daytime function in sleep apnoea/hypopnoea syndrome. Lancet 343(8897):572–575
Olaithe M, Bucks RS (2013) Executive dysfunction in OSA before and after treatment: a meta-analysis. Sleep 36(9):1297–1305
Kylstra WA, Aaronson JA, Hofman WF et al (2013) Neuropsychological functioning after CPAP treatment in obstructive sleep apnea: a meta-analysis [Review]. Sleep Med Rev 17(5):341–347
Kushida CA, Nichols DA, Holmes TH et al (2012) Effects of continuous positive airway pressure on neurocognitive function in obstructive sleep apnea patients: the Apnea Positive Pressure Long-term Efficacy Study (APPLES). Sleep 35(12):1593–1602
Filipovic B, Duric V, Filipovic N et al (2021) Anatomical brain changes and cognitive abilities in patients with obstructive sleep apnea syndrome and nonalcoholic fatty liver disease. Can J Gastroenterol Hepatol 2021:8873652
Feng J, Wu Q, Zhang D et al (2012) Hippocampal impairments are associated with intermittent hypoxia of obstructive sleep apnea. Chin Med J (Engl) 125(4):696–701
Calvo-Flores Guzman B, Elizabeth Chaffey T, Hansika Palpagama T et al (2020) The interplay between beta-amyloid 1–42 (Abeta1-42)-induced hippocampal inflammatory response, p-tau, vascular pathology, and their synergistic contributions to neuronal death and behavioral deficits. Front Mol Neurosci 13:522073
Bucks RS, Olaithe M, Eastwood P (2013) Neurocognitive function in obstructive sleep apnoea: a meta-review. Respirology 18(1):61–70
Pun M, Beaudin AE, Raneri JK et al (2021) Impact of nocturnal oxygen and CPAP on the ventilatory response to hypoxia in OSA patients free of overt cardiovascular disease. Exp Neurol 346:113852
Li M, Sun H, Shen T et al (2022) Increased serum levels of cyclophilin a and matrix metalloproteinase-9 are associated with cognitive impairment in patients with obstructive sleep apnea. Sleep Med 93:75–83
Fernandes M, Placidi F, Mercuri NB et al (2021) The importance of diagnosing and the clinical potential of treating obstructive sleep apnea to delay mild cognitive impairment and Alzheimer’s disease: a special focus on cognitive performance. J Alzheimers Dis Rep 5(1):515–533
Yi M, Zhao W, Tan Y et al (2022) The causal relationships between obstructive sleep apnea and elevated CRP and TNF-alpha protein levels. Ann Med 54(1):1578–1589
Yi M, Tan Y, Pi Y et al (2022) Variants of candidate genes associated with the risk of obstructive sleep apnea. Eur J Clin Invest 52(1):e13673
Custodero C, Ciavarella A, Panza F et al (2022) Role of inflammatory markers in the diagnosis of vascular contributions to cognitive impairment and dementia: a systematic review and meta-analysis. Geroscience 44(3):1373–1392
Ward DD, Wallace LMK, Rockwood K (2021) Cumulative health deficits, APOE genotype, and risk for later-life mild cognitive impairment and dementia. J Neurol Neurosurg Psychiatry 92(2):136–142
Funding
This research was supported by the National Natural Science Foundation of China (No. 82001357), the Hunan Provincial Natural Science Foundation of China (No. 2021JJ80079), the Youth Science Foundation of Xiangya Hospital (No. 2019Q17), the Degree & Postgraduate Education Reform Project of Central South University (No. 2021YJSKSA10), the Undergraduate Education Reform Project of Central South University (No. 2021CG065, No. 2021CG068), and the Research Project of Laboratory Construction and Management of Central South University (No. 202120).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
Not applicable. No human participants included. For this type of study formal consent is not required.
Consent to participate
This article does not contain any studies with human participants performed by any of the authors.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Li, J., Yan, W., Yi, M. et al. Efficacy of CPAP duration and adherence for cognitive improvement in patients with obstructive sleep apnea: a meta-analysis of randomized controlled trials. Sleep Breath 27, 973–982 (2023). https://doi.org/10.1007/s11325-022-02687-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11325-022-02687-y