
Abstract
Purpose
Poor sleep quality is common in medical students and is associated with a number of negative health outcomes. However, the prevalence estimates of poor sleep quality in medical students vary widely across studies. We thus conducted a meta-analysis of the prevalence of poor sleep quality and its mediating factors in medical students.
Methods
A systematic literature search of PubMed, EMBASE, Web of Science, PsycINFO, and Medline Complete was performed. The random-effects model was used to analyze the pooled prevalence of poor sleep quality and its 95% confidence intervals (CIs).
Results
A total of 57 studies with 25,735 medical students were included. The pooled prevalence of poor sleep quality was 52.7% (95% CI: 45.3% to 60.1%) using the Pittsburgh Sleep Quality Index (PSQI). The pooled mean total PSQI score across 41 studies with available data was 6.1 (95% CI: 5.6 to 6.5). Subgroup analyses found that PSQI cutoff value and study region were associated with the prevalence of poor sleep quality (P = 0.0003 VS. P = 0.005). Across the continents, poor sleep quality was most common in Europe, followed by the Americas, Africa, Asia, and Oceania. Meta-regression analyses found that smaller sample size (slope = − 0.0001, P = 0.009) was significantly associated with higher prevalence of poor sleep quality.
Conclusions
Poor sleep quality is common among medical students, especially in Europe and the Americas continets. Due to the negative health outcomes, regular screening of poor sleep quality and effective interventions are needed for medical students.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Medical students are more likely to suffer from poor sleep quality [1] compared to other college students [2], which may have a negative impact on their academic performance, physical and mental health, and quality of life [3]. Poor sleep quality may be related to emotional problems (e.g., stress, depressive, and anxiety symptoms) [4, 5], clinical placements [6, 7], heavy study workload (e.g., hectic schedule, vast syllabus, various clinical training, and onerous academic load) [8,9,10], and significant economic pressures [11, 12],
The Pittsburgh Sleep Quality Index (PSQI) is the most widely used instrument to evaluate subjective sleep quality in the past month. It covers a broad range of indicators relevant to sleep quality [13], including subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbance, use of sleep medication, and daytime dysfunction. The PSQI has been validated in numerous languages with satisfactory psychometric properties [14], and is commonly used across a wide range of clinical and research settings [15]. The PSQI has been also validated in college students [16,17,18,19,20] including medical students [21].
In order to develop effective interventions and lower the risk of the negative outcomes related to poor sleep, such as burnout [22], depression and anxiety [23, 24], and poor academic and work performance [25, 26], it is essential to examine patterns of poor sleep quality. To date, the findings regarding the patterns of poor sleep quality among medical students has been mixed across studies [27, 28]. No meta-analysis or systematic review has yet been conducted to examine the prevalence of poor sleep quality in this population. Thus, we conducted a comprehensive meta-analysis of the prevalence of poor sleep quality worldwide and its associated factors in medical students.
Methods
The study protocol was registered in the international prospective register of systematic reviews (PROSPERO; registration number CRD42019076413).
Data sources and search strategies
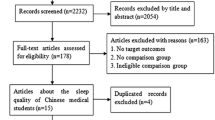
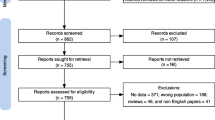
The preferred reporting items for systematic reviews and meta-analyses (PRISMA) checklist and PRISMA study flow chart were used. Four investigators (WWR, WL, HQ, and LH) conducted literature search in PubMed, EMBASE, Web of Science, PsycINFO, and Medline Complete from their inception dates until Aug 20, 2018 using the following queries: Pittsburgh Sleep Quality Index, PSQI, medical students, health occupations students, and medical education. Titles and abstracts of relevant publications were independently screened, and then the full texts were reviewed for eligibility by the same four investigators. If the same dataset was used in more than one publication, only the one with the largest sample size was included. Any disagreement was resolved after a discussion with a senior investigator (YTX). Fig. 1 presents the literature search and selection process.

Flowchart of literature selection
Study eligibility
Original studies were included if they fulfilled the following inclusion criteria: (1) cross-sectional or cohort studies (only the data at baseline were extracted) on medical students; (2) available data on sleep quality measured by the Pittsburgh Sleep Quality Index (PSQI); (3) those published in English. Review articles were excluded. The reference list of included studies was also reviewed for additional studies.
Data extraction
The following information from included studies was extracted and recorded by four investigators using an Excel data collection spreadsheet, such as mean age, gender, sampling method, sample size, year of publication, study site, response rate, country/region, and PSQI cut-off and total score.
Quality assessment
The methodology quality of the studies was independently assessed by the same four investigators using the quality assessment instrument for epidemiological studies [29,30,31], with the total score ranging from 1 (lowest quality) to 8 (highest quality) points. The eight domains were: (1) target population was clearly defined; (2) probability sampling was used or the entire population was surveyed; (3) response rate was ≥ 80%; (4) non-responders were clearly described; (5) sample was representative of the target population; (6) data collection methods were standardized; (7) validated criteria were used to measure the target diagnosis or symptom; and (8) prevalence estimates were given with confidence intervals and specified by subgroups. Any discrepancies in quality assessment were resolved after a discussion with the senior researcher (YTX). This quality assessment instrument has been widely used in previous studies [32, 33].
Statistical analysis
Data were analyzed by the STATA, Version 12.0 for Windows (Stata Corporation, College Station, Texas, USA) R, version 3.3.0 and R Studio, version 0.99.903. The pooled prevalence of poor sleep quality was calculated as effect size (ES); the estimate pooled prevalence and its 95% confidence intervals (CIs) were calculated by the “metaprop” command in Stata 12.0 using the Freeman-Tukey double arcsine transformation and DerSimonian and Laird random effects model. Heterogeneity was measured by I2 statistics and Q-statistic, with I2 > 50% as high heterogeneity. Subgroup analyses were performed according to the following categorical variables: sampling methods (Cluster/Random/Convenience/Others), cut-off of PSQI (≥ 5/≥ 6/≥ 7/≥ 8), regional classification (Africa/the Americas/Europe/Asia/Oceania continents), publication year (in and after 2016/before 2016 according to the median splitting method) and clinical medical student (Yes/No/Both). For the prevalence of poor sleep quality, meta-regression analyses were performed based on continuous variables, including publication year, sample size, response rate, quality assessment score, mean age, and sex ratio. Begg and Mazumbar’s rank correlation test was used to explore publication bias. A bilateral alpha risk of 0.05 was set.
Results
Study selection
A total of 1,109 relevant articles were identified in literature search, and finally, 57 studies with 25,735 medical students were included for the analyses (Fig. 1). Of these, 50 studies had reported the prevalence of poor sleep quality and 41 had reported the PSQI total scores. One study [34] examined sleep quality in both clinical and nonclinical medical students separately; hence, this study was analyzed as two samples in subgroup analyses. Study characteristics are presented in Table 1.
Quality assessment and publication bias
The scores of study quality assessment ranged from 3 to 8 with the mean of 6. No publication bias for poor sleep quality was found in funnel plot (Fig. 3) and Begg’s test (z = 0.31, P value = 0.757).
Prevalence of poor sleep quality, subgroup analyses, and meta regression
The pooled prevalence of poor sleep quality across 50 studies with 24,884 medical students was 52.7% (95% CI: 45.3%–60.1%; I2 = 99.22; P < 0.001; Fig. 2). Subgroup analyses found that compared to other cutoff values (≥ 6, ≥ 7, and ≥ 8), studies using the PSQI cutoff value of ≥ 5 was associated with higher prevalence of poor sleep quality (P = 0.0003). Across the continents, the prevalence of poor sleep quality was highest in the studies conducted in Europe (65.13%), followed by in the Americas (59.92%), Africa (54.54%), Asia (47.44%), and Oceania (30.51%). Meta regression analyses revealed that smaller sample size (slope = − 0.0001, P = 0.009) was associated with higher prevalence of poor sleep quality.

Forest plot of the prevalence of poor sleep quality in medical students. The horizontal axis refers to effect size. Note: ES=Effect Size; CI=Confidence Interval

Funnel plot of publication bias for studies of sleep quality (n=50)
PSQI total score and subscale scores
The pooled PSQI total score from 41 studies with 16,748 medical students was 6.058 (95% CI: 5.614–6.538; I2 = 71.8; P < 0.001). The pooled mean score of the 7 PSQI subscales were as follows: subjective sleep quality: 1.22 (95% CI = 1.04–1.41), sleep latency: 0.99 (95% CI = 0.88–1.11), sleep duration: 1.05 (95% CI = 0.92–1.18), sleep efficiency: 0.27 (95% CI = 0.19–0.34), sleep disturbance: 1.17 (95% CI = 1.01–1.33), use of sleep medications: 0.33 (95% CI = 0.23–0.43), and daytime function: 1.32 (95% CI = 1.11–1.53) (Table S1).
Sleep habits
The data of sleep duration and sleep habits are shown in Table S2. The proportion of medical students who slept less than 7 h/day was 58.7% (95% CI = 45.3%–72.0%), while the proportion of more than and equal to 7 h/day was 41.3% (95% CI = 28.0%–54.7%).
The pooled bedtime across 6 studies with 1,332 medical students was 0:23 am (95% CI: 11:13 pm–1:33 am). The pooled mean sleep latency across 13 studies with 2,930 medical students was 21.53 min (95% CI: 18.65–24.41). The mean sleep duration across 22 studies with 4,851 medical students was 6.45 h (95% CI: 6.03–6.87) and time to get up across 5 studies with 1,393 medical students was 7:13 am (95% CI: 5:46 am–8:41 am).
Discussion
To our best knowledge, this was the first comprehensive meta-analysis of studies worldwide on the pooled prevalence of poor sleep quality in medical students using the PSQI. The main finding was that the majority of medical students had self-reported poor sleep quality (52.7%, 95% CI: 45.3%–60.1%).
In this meta-analysis, the prevalence of poor sleep quality in medical students (52.7%, 95% CI: 45.3%–60.1%) is significantly higher than the corresponding figures (23.9%, 95% CI: 20.8%–27.4%; by the PSQI) in university students [35] and in older population (38.3%; 95%CI = 32.4%–44.2%; by the PSQI) [36]. This is probably related to the high academic pressure in medical schools [4] and short sleep duration among medical students necessary to meet such academic demands [37]. Additionally, certain psychological factors, such as anxiety and depressive symptoms, and even suicidality, are relatively common in medical students [38], which is associated with higher risk of sleep problems [39,40,41]. On the other hand, there is an assumption that medical students may have more medical knowledge than the general population [42], and therefore may be prone to over-reporting symptoms in surveys, which could increase the prevalence of self-reported poor sleep quality.
This study found that smaller sample size was associated with higher prevalence of poor sleep quality. Due to limited statistical power, small sample size may bias the findings to an uncertain extent [43]. As expected, lower PSQI cutoff values were associated with higher prevalence of poor sleep quality, which is consistent with previous findings [35]. In addition, the use of different PSQI cutoff values may be a major source of heterogeneity between studies. Study region was significantly associated with the prevalence of poor sleep quality in medical students. The prevalence of poor sleep quality was highest in Europe (65.13%), followed by the Americas (59.92%), Africa (54.54%), Asia (47.44%), and Oceania (30.51%). Most of the high-ranking medical schools globally are located in Europe and the Americas [44]; therefore, medical students in these regions are more likely to have rigorous academic requirements and pressure compared to those in other areas, which is associated with higher risk of poor sleep quality [45]. Moreover, medical students in Western countries may also have high self-expectation to perform [46], and may therefore have a higher likelihood of poor sleep quality.
The strengths of this meta-analysis includ the large number of studies and the large pooled sample size. However, several limitations need to be addressed. First, similar to other meta-analysis [47, 48], substantial heterogeneity was inevitable in meta-analysis of epidemiological studies, although subgroup analyses alleviated this limitation to some extent. Second, some factors related to sleep quality, such as academic achievement and pressure and family support, were not recorded in most studies. Third, only studies using the PSQI were included. However, the PSQI is considered the most widely used tool to measure poor sleep quality, and in order to minimize bias caused by different measures, other instruments on sleep, such as the Epworth Sleepiness Scale (ESS) or Insomnia Severity Index (ISI), were not included.
In conclusion, poor sleep quality is common in medical students globally, particularly in Europe and the Americas. To reduce the negative health outcomes of poor sleep quality, education on the impact of poor sleep, regular monitoring of sleep and practicing sleep hygiene should be promoted in medical students. Finally, longitudinal research on the association between poor sleep quality and other demographic and clinical variables in medical students should be conducted in the future.
References
Cvejic E, Huang S, Vollmer-Conna U (2018) Can you snooze your way to an ‘a’? Exploring the complex relationship between sleep, autonomic activity, wellbeing and performance in medical students. Aust N Z J Psychiatry 52(1):39–46. https://doi.org/10.1177/0004867417716543
Preisegolaviciute E, Leskauskas D, Adomaitiene V (2010) Associations of quality of sleep with lifestyle factors and profile of studies among Lithuanian students. Medicina-Lithuania 46(7):482–489. https://doi.org/10.3390/medicina46070070
Saravanan C, Wilks R (2014) Medical students' experience of and reaction to stress: the role of depression and anxiety. Sci World J 2014:737382. https://doi.org/10.1155/2014/737382
Almojali AI, Almalki SA, Alothman AS, Masuadi EM, Alaqeel MK (2017) The prevalence and association of stress with sleep quality among medical students. J Epidemiol Global Health 7(3):169–174. https://doi.org/10.1016/j.jegh.2017.04.005
Eller T, Aluoja A, Vasar V, Veldi M (2006) Symptoms of anxiety and depression in Estonian medical students with sleep problems. Depress Anxiety 23(4):250–256. https://doi.org/10.1002/da.20166
Azad MC, Fraser K, Rumana N, Abdullah AF, Shahana N, Hanly PJ, Turin TC (2015) Sleep disturbances among medical students: a global perspective. J Clin Sleep Med 11(1):69–74. https://doi.org/10.5664/jcsm.4370
Daugherty SR, Baldwin DC Jr (1996) Sleep deprivation in senior medical students and first-year residents. Acad Med 71(1 Suppl):S93–S95. https://doi.org/10.1097/00001888-199601000-00054
Altaf M, Altaf KF, Iftikhar A, Goha S (2013) Yusra, workload and health problems in medical students. Int J Endorsing Health Sci Res 1(2):69–72
Mahendran R, Lim HMA, Kua EH (2019) Medical students' experiences in learning the mental state examination with standardized patients. Asia Pac Psychiatry 11(4):e12360
Puthran R, Zhang MW, Tam WW, Ho RC (2016) Prevalence of depression amongst medical students: a meta-analysis. Med Educ 50(4):456–468
Gomes AA, Tavares J, de Azevedo MHP (2011) Sleep and academic performance in undergraduates: a multi-measure, multi-predictor approach. Chronobiol Int 28(9):786–801
Sharifirad G, Marjani A, Abdolrahman C, Mostafa Q, Hossein S (2012) Stress among Isfahan medical sciences students. J Res Med Sci 17(4):402–406
Buysse DJ, Reynolds CF III, Monk TH, Berman SR, Kupfer DJ (1989) The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res 28(2):193–213
Mollayeva T, Thurairajah P, Burton K, Mollayeva S, Shapiro CM, Colantonio A (2016) The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: a systematic review and meta-analysis. Sleep Med Rev 25:52–73. https://doi.org/10.1016/j.smrv.2015.01.009
Buysse DJ, Hall ML, Strollo PJ, Kamarck TW, Owens J, Lee L, Reis SE, Matthews KA (2008) Relationships between the Pittsburgh sleep quality index (PSQI), Epworth sleepiness scale (ESS), and clinical/polysomnographic measures in a community sample. J Clin Sleep Med 4(6):563–571
Dietch JR, Taylor DJ, Sethi K, Kelly K, Bramoweth AD, Roane BM (2016) Psychometric evaluation of the PSQI in US college students. J Clin Sleep Med 12(08):1121–1129
Guo S, Sun W, Liu C, Wu S (2016) Structural validity of the Pittsburgh sleep quality index in Chinese undergraduate students. Front Psychol 7:1126
Marques D, Gomes AA, Meiavia A, Salgueiro A, Ribeiro CC, Dischler J (2013) Reliability and initial validation of the Pittsburgh sleep quality index, European Portuguese version: a preliminary study in a sample of higher education students. Sleep Med 14(s1):e140
Aloba OO, Adewuya AO, Ola BA, Mapayi BM (2007) Validity of the Pittsburgh sleep quality index (PSQI) among Nigerian university students. Sleep Med 8(3):266–270
Manzar MD, Moiz JA, Zannat W, Spence DW, Pandi-Perumal SR, Ahmed SB, Hussain ME (2015) Validity of the Pittsburgh sleep quality index in Indian University students. Oman Med J 30(3):193–202. https://doi.org/10.5001/omj.2015.41
Hashmi AM, Khawaja IS, Butt Z, Umair M, Naqvi SH, Ul-Haq J (2014) The Pittsburgh sleep quality index: validation of the Urdu translation. J Coll Physicians Surg Pak 24(2):123–126
Giorgi F, Mattei A, Notarnicola I, Petrucci C, Lancia L (2018) Can sleep quality and burnout affect the job performance of shift-work nurses? A hospital cross-sectional study. J Adv Nurs 74(3):698–708. https://doi.org/10.1111/jan.13484
Baroni A, Bruzzese JM, Di Bartolo CA, Ciarleglio A, Shatkin JP (2018) Impact of a sleep course on sleep, mood and anxiety symptoms in college students: a pilot study. J Am Coll Heal 66(1):41–50. https://doi.org/10.1080/07448481.2017.1369091
Tsuno N, Besset A, Ritchie K (2005) Sleep and depression. J Clin Psychiatry 66(10):1254–1269
Park E, Lee HY, Park CS (2018) Association between sleep quality and nurse productivity among Korean clinical nurses. J Nurs Manag 26(8):1051–1058. https://doi.org/10.1111/jonm.12634
Barbe T, Kimble LP, Rubenstein C (2018) Subjective cognitive complaints, psychosocial factors and nursing work function in nurses providing direct patient care. J Adv Nurs 74(4):914–925. https://doi.org/10.1111/jan.13505
Wu X, Tao S, Zhang Y, Zhang S, Tao F (2015) Low physical activity and high screen time can increase the risks of mental health problems and poor sleep quality among Chinese college students. PLoS One 10(3):e0119607
Uyar K, Gundogan R, Gurbuz OB, Ozcakar N (2016) Status of fatigue and sleep quality in clinical medical students. Marmara Med J 29(3):164–169. https://doi.org/10.5472/MMJoa.2903.05
Boyle MH (1998) Guidelines for evaluating prevalence studies. Evidence-based Mental Health 1(2):37–39
Pringsheim T, Jette N, Frolkis A, Steeves TD (2014) The prevalence of Parkinson's disease: a systematic review and meta-analysis. Mov Disord 29(13):1583–1590
Loney PL, Chambers LW, Bennett KJ, Roberts JG, Stratford PW (1998) Critical appraisal of the health research literature: prevalence or incidence of a health problem. Chronic Dis Canada 19(4):170–176
Xu D-D, Rao W-W, Cao X-L, Wen S-Y, Che W-I, Ng CH, Ungvari GS, Du Y, Zhang L, Xiang Y-T (2018) Prevalence of major depressive disorder in children and adolescents in China: a systematic review and meta-analysis. J Affect Disord 241:592–598. https://doi.org/10.1016/j.jad.2018.07.083
Ibrahim AK, Kelly SJ, Adams CE, Glazebrook C (2013) A systematic review of studies of depression prevalence in university students. J Psychiatr Res 47(3):391–400
Chutani A, Shenvi DN, Singhal A (2017) Sleep, sleepiness and medical college students: a comparative study among medical and paramedical students of a tertiary care teaching hospital from a west Indian Metropolitan City. Annals Med Health Sci Res 7(2):85–91
Li L, Wang YY, Wang SB, Zhang L, Li L, Xu DD, Ng CH, Ungvari GS, Cui X, Liu ZM, De Li S, Jia FJ, Xiang YT (2018) Prevalence of sleep disturbances in Chinese university students: a comprehensive meta-analysis. J Sleep Res 27(3):e12648. https://doi.org/10.1111/jsr.12648
Lu L, Wang S-B, Rao W, Zhang Q, Ungvari GS, Ng CH, Kou C, Jia F-J, Xiang Y-T (2018) The prevalence of sleep disturbances and sleep quality in older Chinese adults: a comprehensive Meta-analysis. Behav Sleep Med 17(6):683–697. https://doi.org/10.1080/15402002.2018.1469492
Waqas A, Khan S, Sharif W, Khalid U, Ali A (2015) Association of academic stress with sleeping difficulties in medical students of a Pakistani medical school: a cross sectional survey. Peerj 3(12):e840. https://doi.org/10.7717/peerj.840
Zeng W, Chen R, Wang X, Zhang Q, Deng W (2019) Prevalence of mental health problems among medical students in China: a meta-analysis. Medicine 98(18):e15337. https://doi.org/10.1097/md.0000000000015337
Drapeau CW, Nadorff MR (2017) Suicidality in sleep disorders: prevalence, impact, and management strategies. Nat Sci Sleep 9:213–226. https://doi.org/10.2147/NSS.S125597
Krystal AD (2012) Psychiatric disorders and sleep. Neurol Clin 30(4):1389–1413. https://doi.org/10.1016/j.ncl.2012.08.018
Khurshid KA (2018) Comorbid insomnia and psychiatric disorders: an update. Innov Clin Neurosci 15(3–4):28–32
Moss-Morris R, Petrie KJ (2001) Redefining medical students’ disease to reduce morbidity. Med Educ 35(8):724–728
Cao XL, Wang SB, Zhong BL, Zhang L, Ungvari GS, Ng CH, Li L, Chiu HF, Lok GK, Lu JP, Jia FJ, Xiang YT (2017) The prevalence of insomnia in the general population in China: a meta-analysis. PLoS One 12(2):e0170772. https://doi.org/10.1371/journal.pone.0170772
The Times Higher Education World University Rankings 2019 Best universities for medicine 2019. 2019 [March 11, 2019].Available from: https://www.timeshighereducation.com/student/best-universities/best-universities-medicine
Mishra T, Mohapatra D, Behera M, Mishra S (2017) Association between short sleep duration and obesity in medical students. Asian J Pharmaceutl Clin Res 10(1):242–244
Smith CR (2017) Deliberate self-harm and suicide ideology in medical stduents. In: Exploring the Pressures of Medical Education from a Mental Health and Wellness Perspective. IGI Global, USA, p 130
Rotenstein LS, Ramos MA, Torre M, Segal JB, Peluso MJ, Guille C, Sen S, Mata DA (2016) Prevalence of depression, depressive symptoms, and suicidal ideation among medical students: a systematic review and Meta-analysis. JAMA 316(21):2214–2236. https://doi.org/10.1001/jama.2016.17324
Mata DA, Ramos MA, Bansal N, Khan R, Guille C, Di Angelantonio E, Sen S (2015) Prevalence of depression and depressive symptoms among resident physicians: a systematic review and Meta-analysis. JAMA 314(22):2373–2383. https://doi.org/10.1001/jama.2015.15845
Adeosun SO, Asa SO, Babalola OO, Akanmu MA (2008) Effects of night-reading on daytime sleepiness, sleep quality and academic performance of undergraduate pharmacy students in Nigeria. Sleep Biol Rhythms 6(2):91–94. https://doi.org/10.1111/j.1479-8425.2008.00338.x
Ahrberg K, Dresler M, Niedermaier S, Steiger A, Genzel L (2012) The interaction between sleep quality and academic performance. J Psychiatr Res 46(12):1618–1622. https://doi.org/10.1016/j.jpsychires.2012.09.008
Al Sawah M, Ruffin N, Rimawi M, Concerto C, Aguglia E, Chusid E, Infortuna C, Battaglia F (2015) Perceived stress and coffee and energy drink consumption predict poor sleep quality in podiatric medical students a cross-sectional study. J Am Podiatr Med Assoc 105(5):429–434
Asiri AK, Almetrek MA, Alsamghan AS, Mustafa O, Alshehri SF (2018) Impact of twitter and WhatsApp on sleep quality among medical students in King Khalid University, Saudi Arabia. Sleep Hypnosis 20(4):247–252. https://doi.org/10.5350/Sleep.Hypn.2018.20.0158
Brick CA, Seely DL, Palermo TM (2010) Association between sleep hygiene and sleep quality in medical students. Behav Sleep Med 8(2):113–121. https://doi.org/10.1080/15402001003622925
Cai ZZ, Jin M, Zu TT, Yang PP (2016) Study on the relationship between medical Students' worry level, coping style and sleep. In: Wei Z, Guo D (eds) proceedings of the 2016 2nd international conference on education, social science, management and sports, vol 92. Advances in Social Science Education and Humanities Research, pp 99–104
Cates ME, Clark A, Woolley TW, Saunders A (2015) Sleep quality among pharmacy students. Am J Pharm Educ 79(1):09. https://doi.org/10.5688/ajpe79109
Chen B, Liu F, Ding S, Ying X, Wang L, Wen Y (2017) Gender differences in factors associated with smartphone addiction: a cross-sectional study among medical college students. BMC Psychiatry 17(1):341. https://doi.org/10.1186/s12888-017-1503-z
Corrêa CC, Oliveira FK, Pizzamiglio DS, EVP O, SAT W (2017) Sleep quality in medical students: a comparison across the various phases of the medical course. J Bras Pneumol 43(4):285–289. https://doi.org/10.1590/S1806-37562016000000178
Deepali A, Shobha MV, Srinivasa Reddy P (2015) A study of mobile phone usage on sleep and stress among first year medical students. Res J Pharm, Biol Chem Sci 6(5):720–723
Elagra MI, Rayyan MR, Alnemer OA, Alshehri MS, Alsaffar NS, Al-Habib RS, Almosajen ZA (2016) Sleep quality among dental students and its association with academic performance. J Int Soc Prevent Commu Dentistry 6(4):296–301. https://doi.org/10.4103/2231-0762.186788
Eyvazlou M, Zarei E, Rahimi A, Abazari M (2016) Association between overuse of mobile phones on quality of sleep and general health among occupational health and safety students. Chronobiol Int 33(3):293–300. https://doi.org/10.3109/07420528.2015.1135933
Fawzy M, Hamed SA (2017) Prevalence of psychological stress, depression and anxiety among medical students in Egypt. Psychiatry Res 255:186–194. https://doi.org/10.1016/j.psychres.2017.05.027
Fujii H, Miyamoto M, Miyamoto T, Hirata K, Muto T (2009) Relationship between daily meal frequency and subjective sleep quality or daytime sleepiness in Japanese medical students. Dokkyo J Med Sci 36(3):135–142
Genzel L, Ahrberg K, Roselli C, Niedermaier S, Steiger A, Dresler M, Roenneberg T (2013) Sleep timing is more important than sleep length or quality for medical school performance. Chronobiol Int 30(6):766–771. https://doi.org/10.3109/07420528.2012.763132
Giri P, Baviskar M, Phalke D (2013) Study of sleep habits and sleep problems among medical students of Pravara institute of medical sciences Loni, Western Maharashtra, India. Annals Med Health Sci Res 3(1):51–54. https://doi.org/10.4103/2141-9248.109488
Goel N, Malhotra V, Tripathi Y (2016) Sleep habits among first year medical students. J Evol Med Dent Sci 5(38):2276–2278. https://doi.org/10.14260/jemds/2016/529
Hasan EM, Ziaeddin TS, Saeed MMS, Hossein F, Mohammad N, Mehrnoosh D, Sedighe F (2017) Studying the relationship between university Students' anxiety and depression with religious orientation, quality of sleep and emotional cognitive adjustment. Neuroquantology 15(4):69–75. https://doi.org/10.14704/nq.2017.15.4.1155
Israel M, Patil U, Shinde S, Ruikar VM (2016) Obesity in medical students and its correlation with sleep patterns and sleep duration. Indian J Physiol Pharmacol 60(1):38–44
James B, Omoaregba J, Igberase O (2011) Prevalence and correlates of poor sleep quality among medical students at a Nigerian university. Annals Niger Med 5(1):1–5. https://doi.org/10.4103/0331-3131.84218
Kang JH, Chen SC (2009) Effects of an irregular bedtime schedule on sleep quality, daytime sleepiness, and fatigue among university students in Taiwan. BMC Public Health 9:248. https://doi.org/10.1186/1471-2458-9-248
Karaman HIO, Tanriverdi G, Degirmenci Y (2012) Subjective sleep quality in premenstrual syndrome. Gynecol Endocrinol 28(8):661–664. https://doi.org/10.3109/09513590.2011.650769
Kumar A, Vandana AAN (2016) Analgesics self-medication and its association with sleep quality among medical undergraduates. J Clin Diagn Res 10(12):FC7–FC11. https://doi.org/10.7860/jcdr/2016/22504.8953
Lei J, Jin H, Shen S, Li Z, Gu G (2015) Influence of clinical practice on nursing students' mental and immune-endocrine functions. Int J Nurs Pract 21(4):392–400. https://doi.org/10.1111/ijn.12272
Liu Y, Liu L, Yang Y, He Y, Zhang Y, Wang M, Chen S, Yao S (2014) A school-based study of irritable bowel syndrome in medical students in Beijing, China: prevalence and some related factors. Gastroenterol Res Pract 2014:124261. https://doi.org/10.1155/2014/124261
Mansouri A, Mokhayeri Y, Tavakol Z (2016) Sleep onset latency in students living in dormitories at Tehran University of Medical Sciences : a survival analysis. Res J Pharm, Biol Chem Sci 7(2):2127–2135
Medeiros ALD, Mendes DBF, Lima PF, Araujo JF (2001) The relationships between sleep–wake cycle and academic performance in medical students. Biol Rhythm Res 32(2):263–270. https://doi.org/10.1076/brhm.32.2.263.1359
Mirghani HO, Mohammed OS, Almurtadha YM, Ahmed MS (2015) Good sleep quality is associated with better academic performance among Sudanese medical students. BMC Res Notes 8:706–706. https://doi.org/10.1186/s13104-015-1712-9
Modna Y, Scott B (2017) The role of circadian rhythms among medical students in time management organization and academic achievement. In: Hajek P, Vit O, Basova P et al. (eds) CBU international conference proceedings 2017: innovations in science and education, vol 5. CBU International Conference Proceedings. pp 983-987. Doi:https://doi.org/10.12955/cbup.v5.1056
Mohammadbeigi A, Absari R, Valizadeh F, Saadati M, Sharifimoghadam S, Ahmadi A, Mokhtari M, Ansari H (2016) Sleep quality in medical students; the impact of over-use of Mobile cell-phone and social networks. J Res Health Sci 16(1):46–50
Mokros L, Witusik A, Michalska J, Lezak W, Panek M, Nowakowska-Domagala K, Antczak A, Pietras T (2017) Sleep quality, chronotype, temperament and bipolar features as predictors of depressive symptoms among medical students. Chronobiol Int 34(6):708–720. https://doi.org/10.1080/07420528.2017.1316730
Najafi Kalyani M, Jamshidi N, Salami J, Pourjam E (2017) Investigation of the relationship between psychological variables and sleep quality in students of medical sciences. Depress Res Treat 2017. https://doi.org/10.1155/2017/7143547
Pagnin D, de Queiroz V, Carvalho YTMS, Dutra ASS, Amaral MB, Queiroz TT (2014) The relation between burnout and sleep disorders in medical students. Acad Psychiatry 38(4):438–444. https://doi.org/10.1007/s40596-014-0093-z
Peng H, Zhang H (2004) Sleep quality of medical students and the related factors. Chin J Clin Rehabilitation 8(33):7574–7576
Purim KS, Guimarães AT, Titski AC, Leite N (2016) Sleep deprivation and drowsiness of medical residents and medical students. Revista do Colegio Brasileiro de Cirurgioes 43(6):438–444. https://doi.org/10.1590/0100-69912016006005
Qaiser DH, Albanyan OA (2018) Sleeping disturbances/disorders in medical students of king Saud bin Abdulaziz University for Health Sciences, Riyadh. J Pioneer Medic Sci 8(1):9–13
Randjelović P, Stojiljković N, Radulović N, Ilić I, Stojanović N, Ilić S (2018) The association of smartphone usage with subjective sleep quality and daytime sleepiness among medical students. Biol Rhythm Res. https://doi.org/10.1080/0929101620181499374
Rasekhi S, Ashouri FP, Pirouzan A (2016) Effects of sleep quality on the academic performance of undergraduate medical students. Health Scope 5(3):e31641. https://doi.org/10.17795/jhealthscope-31641
Rique GLN, Fernandes Filho GMC, Ferreira ADC, de Sousa-Muñoz RL (2014) Relationship between chronotype and quality of sleep in medical students at the Federal University of Paraiba, Brazil. Sleep Sci 7(2):96–102. https://doi.org/10.1016/j.slsci.2014.09.004
Sahin EM, Ozturk L, Oyekcin DG, Uludag A (2016) Effects of sleep hygiene education on subjective sleep quality and academic performance. J Clin Analytic Med 7(3):304–308. https://doi.org/10.4328/jcam.2728
Sahraian A, Javadpour A (2010) Sleep disruption and its correlation to psychological distress among medical students. Shiraz E Medical Journal 11(1):12–17
Saygın M, Öztürk Ö, Gonca T, Has M, Hayri UB, Kurt Y, Yağlı MA, Çalışkan S, Akkaya A, Öztürk M (2016) Investigation of sleep quality and sleep disorders in students of medicine. Turkish Thoracic Journal 17(4):132–140. https://doi.org/10.5578/ttj.30513
Serra-Negra JM, Scarpelli AC, Tirsa-Costa D, Guimaraes FH, Pordeus IA, Paiva SM (2014) Sleep bruxism, awake bruxism and sleep quality among Brazilian dental students: a cross-sectional study. Braz Dent J 25(3):241–247
Shad R, Thawani R, Goel A (2015) Burnout and sleep quality: a cross-sectional questionnaire-based study of medical and non-medical students in India. Cureus 7(10):e361. https://doi.org/10.7759/cureus.361
Siddiqui AF, Al-Musa H, Al-Amri H, Al-Qahtani A, Al-Shahrani M, Al-Qahtani M (2016) Sleep patterns and predictors of poor sleep quality among medical students in King Khalid University, Saudi Arabia. Malay J Med Sci 23(6):94–102. https://doi.org/10.21315/mjms2016.23.6.10
Surani AA, Zahid S, Surani A, Ali S, Mubeen M, Khan RH (2015) Sleep quality among medical students of Karachi, Pakistan. J Pak Med Assoc 65(4):380–382
Vardar E, Vardar SA, Molla T, Kaynak C, Ersoz E (2008) Psychological symptoms and sleep quality in young subjects with different circadian preferences. Biol Rhythm Res 39(6):493–500. https://doi.org/10.1080/09291010701736884
Wang L, Qin P, Zhao YS, Duan SY, Zhang Q, Liu Y, Hu YL, Sun J (2016) Prevalence and risk factors of poor sleep quality among Inner Mongolia Medical University students: a cross-sectional survey. Psychiatry Res 244:243–248. https://doi.org/10.1016/j.psychres.2016.04.011
Yazdi Z, Loukzadeh Z, Moghaddam P, Jalilolghadr S (2016) Sleep hygiene practices and their relation to sleep quality in medical students of Qazvin University of Medical Sciences. J Caring Sci 5(2):153–160. https://doi.org/10.15171/jcs.2016.016
Zarghami M, Khalilian A, Setareh J, Salehpour G (2015) The impact of using cell phones after light-out on sleep quality, headache, tiredness, and distractibility among students of a University in North of Iran. Iran J Psychiatry Behavioral Sci 9(4):e2010. https://doi.org/10.17795/ijpbs-2010
Funding
The study was supported by the National Science and Technology Major Project for investigational new drug (2018ZX09201-014), and the University of Macau (MYRG2019-00066-FHS).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants performed by any of the author.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 36 kb)
Rights and permissions
About this article

Cite this article
Rao, WW., Li, W., Qi, H. et al. Sleep quality in medical students: a comprehensive meta-analysis of observational studies. Sleep Breath 24, 1151–1165 (2020). https://doi.org/10.1007/s11325-020-02020-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11325-020-02020-5