
Abstract
Purpose
Physical activity has been associated with several individual dimensions of sleep. However, the association between physical activity and sleep health, a construct that emphasizes the multidimensional nature of sleep, has not been explored. This analysis examined the relationship between physical activity and a composite measure of sleep health.
Methods
A total of 114 adults (66% female, 60.3 ± 9.2 years) were included in the analyses. Participants reported daily light-intensity physical activity (LPA) and moderate- and vigorous-intensity physical activity (MVPA) via diary, while wearing a pedometer (Omron HJ-720ITC) to measure daily steps. Sleep health was measured using the RU_SATED questionnaire, which addresses regularity of sleep patterns, satisfaction with sleep, daytime alertness, and sleep timing, efficiency, and duration. Multiple linear regression, binary logistic regression, and analysis of covariance (ANCOVA) were utilized for analyses.
Results
Mean sleep health score was 9.6 ± 2.4 (0 [poor]–12 [good]). Participants reported 62.9 ± 66.0 and 51.2 ± 51.2 min/day of LPA and MVPA, respectively, and took 5585.5 ± 2806.7 steps/day. Greater MVPA was associated with better sleep health (β = 0.27, P = 0.005) and sleep health scores differed between those reporting < 30 min/day and ≥ 60 min/day of MVPA (P = 0.004). Greater MVPA was associated with higher odds of having good sleep satisfaction (OR = 1.58 [1.14–2.20], P < 0.01), timing (OR = 2.07 [1.24–3.46], P < 0.01), and duration (OR = 1.48 [1.02–2.18], P = 0.04). Pedometer-based physical activity and LPA were not related to sleep health or its individual dimensions.
Conclusions
In middle- to older-aged adults, higher-intensity activity, but not lower-intensity or volume of activity, was associated with greater sleep health. These data suggest that physical activity intensity may be important for sleep health.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Many dimensions of sleep, including duration, timing, regularity, continuity, and satisfaction, have been shown to be important for optimal health and functioning. Sleep health is a construct that emphasizes the multidimensional nature of sleep and can be defined as a pattern of sleep-wakefulness that promotes health and is impacted by environmental, social, and individual factors [1]. Emerging research shows that composite profiles of poor sleep health are associated with metabolic disease, depression, and chronic disease burden [2,3,4], often demonstrating better predictive ability than individual sleep dimensions [5, 6]. As such, identifying behaviors that are associated with better sleep health is an important potential target for future intervention efforts.
Although many daytime behaviors are promoted (e.g., seeking exposure to appropriately timed light) or discouraged (e.g., limiting caffeine intake) to facilitate better sleep, none are recommended as often as physical activity [7, 8]. Physical activity has been consistently shown to be related to individual dimensions of sleep, including longer duration, greater depth, higher efficiency, and better daytime alertness [9,10,11]. However, sleep is a multidimensional behavior and the relationship between physical activity and a composite measure of sleep health remains to be explored.
In the present study, we examined whether physical activity, measured by self-report and objective methods, was related to a composite measure of sleep health. A secondary aim involved exploring whether physical activity was associated with individual components of sleep health. Based on the multiple reports linking physical activity to better sleep, we hypothesized that greater amounts of physical activity would be associated with better sleep health and that those associations would be present across both self-report and objective measurement methods.
Methods
Study population
This sample comprised middle- to older-aged adults recruited for a study on depression, sleep, and cardiometabolic risk [5, 12]. Participants were recruited from four separate studies previously conducted at the University of Pittsburgh between 1982 and 1999. One study (MH024652) examined sleep in adults without personal or first-degree family history of psychiatric disorders, while the other three studies examined sleep in adults with major depressive disorder (MH029618, MH049115, MH041884). Of the 339 participants re-contacted from 2010 to 2014 to participate in the current study, 177 consented. As part of the primary study, consented individuals participated in polysomnographic recording of sleep and assessments of psychiatric disorders and cardiometabolic risk. Details of the primary study are published elsewhere [12]. The University of Pittsburgh Institutional Review Board approved the study and informed consent was collected from all participants before beginning the study.
Of the 177 enrolled participants, those with significant bipolar or psychotic features (n = 20) were excluded from the analyses. Participants missing diary or sleep health data (n = 37) and covariate data (n = 6) were additionally excluded. As a result, 114 individuals were included in the present report. For analyses involving pedometer physical activity data, 11 additional participants (n = 103) were excluded who failed to provide ≥ 3 days of pedometer data (i.e., considered the minimum acceptable threshold for analysis [13]). No differences in physical activity, sleep health, or covariates were observed between included (n = 114) and excluded (n = 63) participants with the exception of those in the included sample having lower body mass index than the excluded participants (29.4 ± 5.7 vs. 31.9 ± 9.7; P = .04).
Measurement of physical activity
Physical activity was assessed daily with a self-report diary for 5 to 14 days (mean 9.8 ± 1.8 days). At the end of each day, participants were instructed to record their time (in minutes) spent in different intensity categories of physical activity: light (LPA) (i.e., light effort, causes small increases in heart rate like walking at one’s normal pace), medium (i.e., moderate increases in breathing and heart rate like brisk walking or swimming), and heavy (i.e., large increases in breathing and heart rate such as running). Moderate- to vigorous-intensity physical activity (MVPA) was calculated as the sum of medium- and heavy-intensity physical activity. Mean daily LPA and MVPA were used for the analyses.
Physical activity was also objectively assessed each day with a pedometer (HJ-720ITC; Omron Healthcare, Bannockburn, IL) [14, 15]. Participants were instructed to wear the pedometer on the hip of their dominant leg during all waking hours and report times of non-wear in the daily diary. Included participants provided 6.6 ± 0.9 days of pedometer data; mean daily number of steps were retained for the analyses.
Measurement of sleep health
Sleep health was assessed with the 6-item RU_SATED questionnaire [1]. This questionnaire assesses six different sleep health dimensions: regularity (getting in and out of bed at similar times each day), satisfaction (feeling satisfied with one’s sleep), alertness (ability to stay awake during the day without dozing), timing (sleeping between 2:00 a.m. and 4:00 a.m.), efficiency (being awake for less than 30 min each night after trying to fall asleep), and duration (obtaining between 6 and 8 h of sleep per night). Participants indicated how often over the past month they met the criteria for each dimension (0 = rarely/never, 1 = sometimes, 2 = usually/always). Individual items were summed to provide a total score (range 0–12); higher scores indicated better sleep health. A Portuguese language version of the RU_SATED questionnaire has been shown to be psychometrically valid and shows convergent validity with the Pittsburgh Sleep Quality Index, a common measure of sleep quality [16].
Covariates
Indices of mental and physical health were considered as covariates due to their possible relationship with physical activity and/or sleep health. Age, sex, existing cardiovascular disease, depression history, and ability to pay for basic financial needs were self-reported. Due to a limited number of nonwhite participants (< 6%), race was not included as a covariate. As a measure of socioeconomic status, one’s ability to pay for basic financial needs was dichotomized into “not at all” or “somewhat/very hard.” Participant’s height and weight were measured for calculation of body mass index (kg/m2). Existing cardiovascular disease was categorized as a dichotomous variable based on self-report of any of the following conditions: angina, angioplasty, myocardial infarction, bypass surgery, coronary artery disease, heart failure, heart surgery, stroke, or transient ischemic attack. Depression history was also dichotomized and determined by structured clinical interviews performed in earlier research study participation (1982–1999) and the current study; those with a history of major depressive disorder at either time point were considered to have a history of depression. Sleep-disordered breathing was assessed using a single night of polysomnography; the apnea-hypopnea index (AHI), defined as the number of apnea and hypopnea events per hour of sleep, was used as a measure of sleep-disordered breathing severity.
Statistical analysis
Data were analyzed using SAS (v. 9.4; SAS Institute, Cary, NC), with statistical significance set at P ≤ 0.05. Normality distributions of variables were tested via histogram and the Shapiro–Wilk test. The RU_SATED score was skewed; thus, Box–Cox analyses were used to calculate the following transformation to achieve normality: (y2.4 − 1)/2.4 [17]. However, results were similar when using the untransformed and transformed variable; therefore, analyses using the untransformed RU_SATED score are presented.
With physical activity modeled as a continuous variable, multiple linear regression models were used to examine the relationship between physical activity and sleep health. The different physical activity indices (self-reported LPA, MVPA, pedometer physical activity) were examined in separate models following covariate adjustment for age, sex, body mass index, existing cardiovascular disease, depression history, and socioeconomic status. We also evaluated whether sleep health was associated with categorical indices of physical activity to aid interpretation of the data and to observe potential threshold effects. We classified LPA into tertiles for analyses (< 27 min, 27 to < 60 min, ≥ 60 min). Time spent in MVPA was grouped into clinically relevant categories of < 30 min, 30 to < 60 min, and ≥ 60 min [18]. Pedometer physical activity was grouped according to previously established thresholds: inactive (< 5000 steps/day), insufficiently active (5000 to < 7500 steps/day), and active (≥ 7500 steps/day) [19]. Analysis of covariance (ANCOVA) was used to evaluate differences in sleep health across categories of LPA, MVPA, and pedometer physical activity, utilizing the same covariates as previously mentioned. Tukey’s adjustment was used to examine pairwise comparisons if a significant between-group difference was found in each ANCOVA model. Partial eta squares were calculated to evaluate effect size; values of 0.01, 0.06, and 0.14 indicated small, medium, or large effects, respectively [20]. Finally, we evaluated the relationship between physical activity and individual sleep health components with binary logistic regression models. Individual items of the RU_SATED questionnaire were dichotomized into low (i.e., “never/rarely” or “sometimes”) or good (i.e., “usually”) categories. Analyses examined the likelihood of meeting “good” criteria for each sleep health dimension according to physical activity, expressed as odds per 30-min increase in LPA or MVPA and 1000-step increase in pedometer physical activity.
Because the participant sample comprised adults with and without a history of depression, and because depression has been bidirectionally associated with lower physical activity and poor sleep [21,22,23], we also explored depression history as an interaction term in analyses. The physical activity and depression interaction term was not significant in any analyses (P ≥ 0.26 in each model); as a result, the interaction term was not included in any final models. Additionally, to examine whether results were dependent on different sample sizes between the self-reported physical activity (n = 114) and pedometer step analyses (n = 103), we performed sensitivity analyses where the sample size for LPA and MVPA analyses were reduced to n = 103. Lastly, because sleep-disordered breathing may be related to worse sleep health and low physical activity levels, we explored whether adjusting for sleep-disordered breathing severity influenced the results in a subsample who had valid AHI data (MVPA and LPA: n = 110; pedometer steps: n = 100). Because the AHI was skewed, AHI was transformed by natural logarithm values (plus a constant of 1) to achieve normality.
Results
Sample characteristics are displayed in Table 1. Participants were primarily female (65.8%), had a mean age of 60.3 ± 9.2 years, and 57% had a lifetime history of major depressive disorder. Participants reported 62.9 ± 66.0 min/day of LPA. The mean self-reported time spent in MVPA was 51.2 ± 51.2 min/day; 38.6%, 28.9%, and 32.5% of participants reported < 30 min, 30 to < 60 min, or ≥ 60 min of MVPA per day, respectively. Participants took an average of 5585.5 ± 2806.7 steps/day (n = 103); 48.5%, 30.1%, and 21.4% of adults were categorized as being inactive, insufficiently active, and active, respectively. Among those with self-reported and pedometer physical activity data (n = 103), MVPA (min/day) was significantly correlated with pedometer physical activity (steps/day) (r = 0.20, P = 0.04) and LPA (r = 0.29, P = 0.003), but LPA (min/day) was not significantly correlated with pedometer physical activity (r = 0.10, P = 0.31).
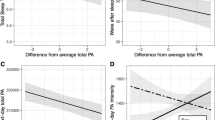
When evaluated as a continuous variable, greater MVPA was significantly associated with better sleep health (β = 0.27, P = 0.005). In contrast, neither LPA (β = 0.07, P = 0.47) nor pedometer physical activity (β = 0.09, P = 0.41) were associated with sleep health. When physical activity was evaluated categorically, we observed a significant difference in sleep health across MVPA categories (F2,105 = 5.49, P = 0.005; Fig. 1a) with a medium effect size (η2 = 0.10). Those who reported ≥ 60 min/day of MVPA had significantly greater sleep health than those who reported < 30 min/day of MVPA (adjusted means ± standard error: 10.3 ± 0.4 vs. 8.6 ± 0.5; P = 0.004). No differences in sleep health were observed across tertiles of LPA (F2,105 = 0.26, P = 0.77, η2 = 0.01; Fig. 1b) or categories of pedometer-based physical activity (F2,94 = 0.58, P = 0.56, η2 = 0.01; Fig. 1c).

Sleep health across different measures of physical activity. Y-axis values for each panel represent mean RU_SATED values following covariate adjustment. a X-axis indicates categories of moderate- to vigorous-intensity physical activity. b X-axis indicates categories of light-intensity physical activity. c X-axis indicates categories of pedometer-assessed steps/day. LPA, light-intensity physical activity; MVPA, moderate- to vigorous-intensity physical activity; PA, physical activity; SE, standard error
Table 2 provides a summary of the analyses examining the association between physical activity indices and individual sleep health dimensions. Greater self-reported MVPA (expressed per 30-min increase in MVPA) was associated with greater odds of reporting good “satisfaction” (odds ratio (OR) = 1.58; 95% confidence interval = 1.14–2.20; P = 0.007), good “timing” (OR = 2.07 (1.24–3.46); P = 0.006), and good “duration” (OR = 1.49 (1.02–2.18); P = 0.04). Self-reported MVPA was not associated with other sleep health dimensions. Neither LPA nor pedometer physical activity was associated with any individual sleep health dimensions.
When all analyses were restricted to a sample size of n = 103, results were unchanged from those observed in the full sample with one exception: greater MVPA was no longer associated with greater odds of reporting good “duration” (OR = 1.34 (0.91, 1.97); P = 0.14). Results were unchanged when AHI was included as an additional covariate in analyses (data not shown).
Discussion
The present study evaluated the association between sleep health and three indices of physical activity: self-reported MVPA, LPA, and objectively measured pedometer steps. We hypothesized that greater levels of physical activity would be associated with better sleep health. Overall, we found that greater levels of self-reported MVPA—but not LPA or pedometer-based physical activity—were associated with better sleep health. Additionally, when exploring the association between MVPA, LPA, and pedometer physical activity with individual sleep health items, we found that higher amounts of MVPA were related to better self-reported sleep satisfaction, sleep timing, and sleep duration. LPA and pedometer physical activity, on the other hand, were not associated with any individual RU_SATED items.
Our primary finding—that MVPA is significantly associated with a composite measure of sleep health—accords with the existing literature, which has consistently observed a relationship between greater physical activity and better sleep. Many of these studies utilized the Pittsburgh Sleep Quality Index, which assesses several different dimensions of sleep that together provide a measure of global sleep quality. In meta-analyses of randomized controlled trials utilizing moderate-intensity exercise interventions, exercise training led to moderate-sized improvements in global PSQI scores compared with non-exercise control conditions [10, 24]. Additionally, Yang and colleagues performed a meta-analysis in which they found that exercise interventions significantly improved global PSQI scores, but not the individual dimensions of sleep duration, sleep disturbance, daytime alertness, or sleep efficiency [11]. These agree with our results utilizing the RU_SATED survey, as we found a global measure of sleep health and some (but not all) individual items to be independently associated with more physical activity.
Our results also suggest a potential dose-response effect, as participants who engaged in ≥ 60 min/day of MVPA had better sleep health than those who reported < 30 min/day of MVPA. The dose-response relationship suggested by the linear regression and ANCOVA analyses is consistent with the limited experimental research on this topic. When evaluating changes in self-reported sleep quality following a 6-month intervention that compared exercise doses equating to 50%, 100%, and 150% of public health guidelines, Kline and colleagues observed greater improvements in sleep quality with increasing exercise dose [25].
Three of the six individual indices of the RU_SATED sleep health score were related to MVPA. Specifically, greater MVPA was associated with greater odds of having good sleep satisfaction, timing, and duration. This is valuable as it elucidates which individual domains may be driving the positive association between physical activity and sleep health. Sleep satisfaction (i.e., sleep quality) has been frequently reported to be positively impacted by MVPA and exercise [9]. Our finding that greater MVPA was associated with obtaining “good” sleep duration (6–8 h) in the full sample is consistent with prior research, as well. Experimental research indicates that acute and chronic exercise has beneficial effects on increasing sleep duration [9, 26, 27], while epidemiologic research has found that MVPA is associated with lower odds of short (< 6 h) or long (> 8 h) sleep duration [28]. Greater amounts of physical activity have been shown to be associated with longer sleep duration on the following night, as well [29]. We also found that greater amounts of MVPA were associated with a greater likelihood of “good” sleep timing (i.e., usually sleeping between 2:00 and 4:00 a.m.). Other cross-sectional studies have found similar results [30, 31]. For instance, Shechter and St-Onge, after adjusting for sleep duration, found that delayed bedtimes and waketimes were associated with less MVPA [31]. In contrast to these associations, no relationships were found between MVPA and other sleep health dimensions, including sleep efficiency, sleep regularity, and daytime alertness. These results conflict with previous studies that have indicated beneficial effects of exercise and MVPA on objectively assessed sleep efficiency and reductions in daytime sleepiness [9]. Although little research has examined the association between MVPA and sleep regularity, secondary analyses of randomized controlled trials have found that exercise interventions lead to decreased night-to-night variability of sleep efficiency and wake after sleep onset [32, 33], as well as self-rated time to fall asleep [34]. These conflicting results could be due to the differences in the measurement of alertness, efficiency, and regularity between previous studies (i.e., actigraphy, Pittsburgh Sleep Quality Index subscale) compared with the single-item categorical indices used in the RU_SATED questionnaire.
Although MVPA was associated with sleep health, neither LPA nor pedometer-assessed physical activity was associated with the individual sleep health dimensions or the composite measure of sleep health. This finding could reflect that the intensity of physical activity may be an important factor in the positive relationship between physical activity and sleep health. LPA is, by definition, lower-intensity activity. Because pedometers are unable to assess intensity and are primarily used to quantify total physical activity volume [35], they could be objectively measuring the accumulation of lower-intensity physical activity and not purposeful higher-intensity activity like exercise. Previous studies have indicated that incidental lower-intensity activities may not be as beneficial to sleep as purposeful exercise [36,37,38]. In a sample of midlife women, Kline and colleagues found that higher levels of sport and exercise participation were associated with multiple self-reported and objectively measured indices of better sleep; however, no associations were found between sleep and participation in active living, caregiving, or household activities [36]. Similar findings were found in an acute exercise study by Wang and Youngstedt, where older participants completed either low- or moderate-intensity exercise of the same duration; only moderate-intensity activity elicited significant reductions in wake after sleep onset and nighttime awakenings relative to a non-exercise condition [37]. Lastly, Chen and colleagues explored the association between baseline walking characteristics and sleep quality measured 2 years later [38]. They found that slower self-reported walking speed was the only predictor of worse sleep following adjustment for walking duration and frequency [38]. Overall, these studies corroborate our finding that lower-intensity physical activity, as captured by the self-reported LPA or pedometer-based physical activity, may not be as strongly associated with better sleep.
This study is the first to directly examine the association between physical activity and a composite measure of sleep health. Additionally, we utilized both subjective and objective measures of physical activity and included multiple covariates which could have confounded the relationship between physical activity and sleep health. Despite these strengths, this study has limitations. One limitation is the measurement of physical activity and sleep. LPA, MVPA, and the RU_SATED questionnaire were based on self-report. This could elicit measurement bias as the significant relationship between MVPA and sleep health could be due to the shared construct of the measures. However, this chance of bias may be reduced since LPA, a self-reported measure, was not found to be significantly related to sleep health. MVPA could have been under- or overestimated due to its self-report nature [39], while pedometers are unable to capture physical activity modalities outside of walking/running such as swimming or resistance training. In addition, our self-reported physical activity data do not provide information on the timing or types of activities undertaken. Due to evidence that exercise timing may impact circadian timing [40] and that different modes of exercise could impact sleep differently [26], future research should assess these variables. Out of 339 individuals eligible for enrollment, only 177 consented to participate in the study; this could potentially indicate a sampling bias in which those who decided to participate had better sleep health than those who declined participation. Additionally, there is a potential bias in the subjective measurement of sleep health since the concordance between the self-reported sleep health dimensions in RU_SATED and their objective measures is unknown. However, Brindle and colleagues found that childhood trauma was related to both subjectively and objectively derived sleep health, which suggests compatibility between different derivations of sleep health [5]. A prior study also demonstrated that the SATED questionnaire (identical to RU_SATED aside from the regularity domain) has stronger linear relationships with self-rated health status than sleep duration alone, which provides support for its validity [2]. Additionally, recent papers have operationalized sleep health with a variety of objective and self-reported sleep indices [3, 5, 6].
In conclusion, we found an association between self-reported MVPA and a composite measure of sleep health as well as the individual components of sleep satisfaction, sleep timing, and sleep duration. In contrast, no association was observed between LPA and pedometer-assessed physical activity with sleep health. Future studies should include accelerometer-based measurement of physical activity or questionnaires focused on mode of activity to examine whether objectively assessed physical activity intensity or type is associated with sleep health. Additionally, this analysis was in a sample with relatively good sleep health; as a result, it is important to explore the strength of association between physical activity and sleep health and the use of MVPA as a potential therapy among those with poor sleep health.
References
Buysse DJ (2014) Sleep health: can we define it? Does it matter? Sleep 37(1):9–17. https://doi.org/10.5665/sleep.3298
Dalmases M, Benitez ID, Mas A, Garcia-Codina O, Medina-Bustos A, Escarrabill J, Salto E, Buysse DJ, Roure N, Sanchez-de-la-Torre M, Rue M, Barbe F, de Batlle J (2018) Assessing sleep health in a European population: results of the Catalan health survey 2015. PLoS One 13(4):e0194495. https://doi.org/10.1371/journal.pone.0194495
Furihata R, Hall MH, Stone KL, Ancoli-Israel S, Smagula SF, Cauley JA, Kaneita Y, Uchiyama M, Buysse DJ (2017) An aggregate measure of sleep health is associated with prevalent and incident clinically significant depression symptoms among community-dwelling older women. Sleep 40 (3):zsw075. https://doi.org/10.1093/sleep/zsw075
Jennings JR, Muldoon MF, Hall M, Buysse DJ, Manuck SB (2007) Self-reported sleep quality is associated with the metabolic syndrome. Sleep 30(2):219–223. https://doi.org/10.1093/sleep/30.2.219
Brindle RC, Cribbet MR, Samuelsson LB, Gao C, Frank E, Krafty RT, Thayer JF, Buysse DJ, Hall MH (2018) The relationship between childhood trauma and poor sleep health in adulthood. Psychosom Med 80(2):200–207. https://doi.org/10.1097/psy.0000000000000542
Wallace ML, Stone K, Smagula SF, Hall MH, Simsek B, Kado DM, Redline S, Vo TN, Buysse DJ (2018) Which sleep health characteristics predict all-cause mortality in older men? An application of flexible multivariable approaches. Sleep 41 (1):zsx189. https://doi.org/10.1093/sleep/zsx189
Irish LA, Kline CE, Gunn HE, Buysse DJ, Hall MH (2015) The role of sleep hygiene in promoting public health: a review of empirical evidence. Sleep Med Rev 22:23–36. https://doi.org/10.1016/j.smrv.2014.10.001
King AC, Oman RF, Brassington GS, Bliwise DL, Haskell WL (1997) Moderate-intensity exercise and self-rated quality of sleep in older adults. A randomized controlled trial. JAMA 277(1):32–37. https://doi.org/10.1001/jama.1997.03540250040029
Kredlow MA, Capozzoli MC, Hearon BA, Calkins AW, Otto MW (2015) The effects of physical activity on sleep: a meta-analytic review. J Behav Med 38(3):427–449. https://doi.org/10.1007/s10865-015-9617-6
Rubio-Arias JA, Marin-Cascales E, Ramos-Campo DJ, Hernandez AV, Perez-Lopez FR (2017) Effect of exercise on sleep quality and insomnia in middle-aged women: a systematic review and meta-analysis of randomized controlled trials. Maturitas 100:49–56. https://doi.org/10.1016/j.maturitas.2017.04.003
Yang PY, Ho KH, Chen HC, Chien MY (2012) Exercise training improves sleep quality in middle-aged and older adults with sleep problems: a systematic review. J Physiother 58 (3):157–163. https://doi.org/10.1016/s1836-9553(12)70106-6
Hall MH, Mulukutla S, Kline CE, Samuelsson LB, Taylor BJ, Thayer JF, Krafty RT, Frank E, Kupfer DJ (2017) Objective sleep duration is prospectively associated with endothelial health. Sleep 40 (1):zsw003. https://doi.org/10.1093/sleep/zsw003
Jake-Schoffman DE, Silfee VJ, Sreedhara M, Rosal MC, May CN, Lopez-Cepero A, Lemon SC, Haughton CF (in press) Reporting of physical activity device measurement and analysis protocols in lifestyle interventions. Am J Lifestyle Med. https://doi.org/10.1177/1559827619862179
Hasson RE, Haller J, Pober DM, Staudenmayer J, Freedson PS (2009) Validity of the Omron HJ-112 pedometer during treadmill walking. Med Sci Sports Exerc 41(4):805–809. https://doi.org/10.1249/MSS.0b013e31818d9fc2
Smith KA, Egercic L, Bramble A, Secich JJ (2017) Reliability and validity of the Omron HJ-720 ITC pedometer when worn at four different locations on the body. Cogent Med 4(1):1311461. https://doi.org/10.1080/2331205X.2017.1311461
Becker NB, Martins RIS, de Neves JS, Chiodelli R, Rieber MS (2018) Sleep health assessment: a scale validation. Psychiatry Res 259:51–55. https://doi.org/10.1016/j.psychres.2017.10.014
Ishak NAM, Ahmad S (2018) Estimating optimal parameter of Box-Cox transformation in multiple regression with non-normal data. In: Regional conference on science, technology and social sciences (RCSTSS 2016). Singapore: Springer, pp 1039–1046. https://doi.org/10.1007/978-981-13-0074-5_102
Piercy KL, Troiano RP, Ballard RM, Carlson SA, Fulton JE, Galuska DA, George SM, Olson RD (2018) The physical activity guidelines for Americans. JAMA 320(19):2020–2028. https://doi.org/10.1001/jama.2018.14854
Tudor-Locke C, Craig CL, Thyfault JP, Spence JC (2013) A step-defined sedentary lifestyle index: < 5000 steps/day. Appl Physiol Nutr Metab 38(2):100–114. https://doi.org/10.1139/apnm-2012-0235
Richardson JT (2011) Eta squared and partial eta squared as measures of effect size in educational research. Educ Res Rev 6(2):135–147. https://doi.org/10.1016/j.edurev.2010.12.001
Achttien R, van Lieshout J, Wensing M, van der Sanden MN, Staal JB (2019) Symptoms of depression are associated with physical inactivity but not modified by gender or the presence of a cardiovascular disease; a cross-sectional study. BMC Cardiovasc Disord 19(1):95. https://doi.org/10.1186/s12872-019-1065-8
Fluetsch N, Levy C, Tallon L (2019) The relationship of physical activity to mental health: a 2015 behavioral risk factor surveillance system data analysis. J Affect Disord 253:96–101. https://doi.org/10.1016/j.jad.2019.04.086
Zhai L, Zhang H, Zhang D (2015) Sleep duration and depression among adults: a meta-analysis of prospective studies. Depress Anxiety 32(9):664–670. https://doi.org/10.1002/da.22386
Banno M, Harada Y, Taniguchi M, Tobita R, Tsujimoto H, Tsujimoto Y, Kataoka Y, Noda A (2018) Exercise can improve sleep quality: a systematic review and meta-analysis. PeerJ 6:e5172. https://doi.org/10.7717/peerj.5172
Kline CE, Sui X, Hall MH, Youngstedt SD, Blair SN, Earnest CP, Church TS (2012) Dose-response effects of exercise training on the subjective sleep quality of postmenopausal women: exploratory analyses of a randomised controlled trial. BMJ Open 2(4):e001044. https://doi.org/10.1136/bmjopen-2012-001044
Passos GS, Poyares D, Santana MG, Garbuio SA, Tufik S, de Mello MT (2010) Effect of acute physical exercise on patients with chronic primary insomnia. J Clin Sleep Med 6(3):270–275
Richards KC, Lambert C, Beck CK, Bliwise DL, Evans WJ, Kalra GK, Kleban MH, Lorenz R, Rose K, Gooneratne NS, Sullivan DH (2011) Strength training, walking, and social activity improve sleep in nursing home and assisted living residents: randomized controlled trial. J Am Geriatr Soc 59(2):214–223. https://doi.org/10.1111/j.1532-5415.2010.03246.x
Reis C, Dias S, Rodrigues AM, Sousa RD, Gregorio MJ, Branco J, Canhao H, Paiva T (2018) Sleep duration, lifestyles and chronic diseases: a cross-sectional population-based study. Sleep Sci 11(4):217–230. https://doi.org/10.5935/1984-0063.20180036
Best JR, Falck RS, Landry GJ, Liu-Ambrose T (2019) Analysis of dynamic, bidirectional associations in older adult physical activity and sleep quality. J Sleep Res 28(4):e12769. https://doi.org/10.1111/jsr.12769
Haraszti RA, Purebl G, Salavecz G, Poole L, Dockray S, Steptoe A (2014) Morningness-eveningness interferes with perceived health, physical activity, diet and stress levels in working women: a cross-sectional study. Chronobiol Int 31(7):829–837. https://doi.org/10.3109/07420528.2014.911188
Shechter A, St-Onge MP (2014) Delayed sleep timing is associated with low levels of free-living physical activity in normal sleeping adults. Sleep Med 15(12):1586–1589. https://doi.org/10.1016/j.sleep.2014.07.010
Baron KG, Reid KJ, Malkani RG, Kang J, Zee PC (2017) Sleep variability among older adults with insomnia: associations with sleep quality and cardiometabolic disease risk. Behav Sleep Med 15(2):144–157. https://doi.org/10.1080/15402002.2015.1120200
Breneman CB, Kline CE, West DS, Sui X, Porter RR, Bowyer KP, Custer S, Wang X (2019) The effect of moderate-intensity exercise on nightly variability in objectively measured sleep parameters among older women. Behav Sleep Med 17(4):459–469. https://doi.org/10.1080/15402002.2017.1395337
Buman MP, Hekler EB, Bliwise DL, King AC (2011) Exercise effects on night-to-night fluctuations in self-rated sleep among older adults with sleep complaints. J Sleep Res 20(1 Pt 1):28–37. https://doi.org/10.1111/j.1365-2869.2010.00866.x
Tudor-Locke C, Williams JE, Reis JP, Pluto D (2002) Utility of pedometers for assessing physical activity: convergent validity. Sports Med 32(12):795–808. https://doi.org/10.2165/00007256-200232120-00004
Kline CE, Irish LA, Krafty RT, Sternfeld B, Kravitz HM, Buysse DJ, Bromberger JT, Dugan SA, Hall MH (2013) Consistently high sports/exercise activity is associated with better sleep quality, continuity and depth in midlife women: the SWAN sleep study. Sleep 36(9):1279–1288. https://doi.org/10.5665/sleep.2946
Wang X, Youngstedt SD (2014) Sleep quality improved following a single session of moderate-intensity aerobic exercise in older women: results from a pilot study. J Sport Health Sci 3(4):338–342. https://doi.org/10.1016/j.jshs.2013.11.004
Chen LJ, Fox KR, Sun WJ, Tsai PS, Ku PW, Chu D (2018) Associations between walking parameters and subsequent sleep difficulty in older adults: a 2-year follow-up study. J Sport Health Sci 7(1):95–101. https://doi.org/10.1016/j.jshs.2017.01.007
Sallis JF, Saelens BE (2000) Assessment of physical activity by self-report: status, limitations, and future directions. Res Q Exerc Sport 71(2):1–14. https://doi.org/10.1080/02701367.2000.11082780
Youngstedt SD, Elliott JA, Kripke DF (2019) Human circadian phase-response curves for exercise. J Physiol 597(8):2253–2268. https://doi.org/10.1113/jp276943
Acknowledgments
The authors are grateful to all study staff and participants that made this dataset a reality for secondary analyses such as these.
Funding
This study was funded by National Institutes of Health (NIH) grant R01HL104607 (PI: Hall). Additional investigator support was provided by NIH grants K23HL118318 (PI: Kline) and R01GM113243 (PI: Krafty).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
DJB, RTK, MHH, and CEK have received grant support independent from this project from the NIH. DJB has served as a paid consultant for Weight Watchers, Bayer, and Emmi Solutions; received fees for educational products and programs sponsored by the American Academy of Physician Assistants, CME Institute, and Eisai; received licensing fees for the Pittsburgh Sleep Quality Index, copyrighted to the University of Pittsburgh, and the Consensus Sleep Diary, licensed to Ryerson University. RCB and JFT declare that they have no conflict of interest.
Ethical approval
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kubala, A.G., Buysse, D.J., Brindle, R.C. et al. The association between physical activity and a composite measure of sleep health. Sleep Breath 24, 1207–1214 (2020). https://doi.org/10.1007/s11325-019-02007-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11325-019-02007-x