
Abstract
Purpose
Information on access and adherence to positive airway pressure (PAP) treatment is lacking at the regional level in Latin America. This study characterized access and adherence to PAP in patients with moderate-severe obstructive sleep apnea (OSA) in Latin America.
Methods
Cross-sectional study, conducted at 9 sleep centers across Argentina, Brazil, Chile, Colombia, Mexico, and Peru. Adults diagnosed with moderate-severe OSA (apnea-hypopnea index [AHI] ≥ 15/h) in the previous 12–18 months were eligible. Anthropometrics, health coverage, and OSA severity data were collected. Data on access to therapy, barriers to access, adherence, and factors related to non-compliance were obtained via standardized telephone survey.
Results
Eight hundred eighty patients (70% male, 54 ± 13 years, AHI 49 ± 28/h, body mass index 32 ± 7 kg/m2) were included. Four hundred ninety patients (56%) initiated PAP, 70 (14%) discontinued therapy during the first year (mainly due to intolerance), and 420 (48%) were still using PAP when surveyed. Health insurance was private in 36.9% of patients, via the social security system in 31.1%, and via the state in 13.3%, and 18.7% did not have any coverage; 49.5% of patients had to pay all equipment costs. Reasons for not starting PAP were unclear or absent indication (42%), coverage problems (36%), and lack of awareness of OSA burden (14%). Patients with better adherence were older (55.3 ± 13 vs 52 ± 13; p = 0.002) and had more severe OSA (AHI 51.8 ± 27 vs 45.6 ± 27; p = 0.001).
Conclusions
Less than half moderate-severe OSA patients started and continue to use PAP. Unclear or absent medical indication and financial limitations were the most relevant factors limiting access to therapy.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Obstructive sleep apnea (OSA) is a common sleep-related breathing disorder that involves a decrease or complete cessation in airflow despite an ongoing effort to breathe. OSA is characterized by disruption of sleep associated with repetitive narrowing and closure of the upper airway, usually followed by oxygen desaturation, arousals, and sleep fragmentation [1, 2]. Known risk factors for OSA include male sex, older age, overweight, small diameter of the oropharynx, enlargement of pharyngeal soft tissues (tonsils, adenoids, tongue, and palate), high neck circumference, and conditions associated with muscle relaxation or weakness (neuromuscular diseases, drugs, alcohol) [1, 2]. Upper airway collapsibility and anatomy play a central role in the pathogenesis of OSA. Nevertheless, other factors, such as upper airway muscle responsiveness during sleep, the respiratory arousal threshold, and loop gain, may be also involved in OSA pathogenesis for certain patients. [3].
OSA is highly prevalent in the general population [1, 4,5,6], affecting quality of life and increasing cardiovascular and neurocognitive morbidity [1, 2, 7, 8]. Fragmented sleep, excessive daytime sleepiness, cognitive impairment, and increased risk for motor vehicle accidents are also associated with OSA [1, 2]. In addition, OSA significantly increases mortality, and social and health care costs [8, 9]. To our knowledge, only one study has reported on OSA prevalence in Latin America [4]. This study was conducted in Brazil and reported a prevalence for OSA of 32.8%, Although these estimates exceed the historically recognized indexes, they are similar in magnitude to the ones reported in more recent epidemiological studies in other regions of the world [5, 6].
The most effective treatment for moderate to severe OSA is positive airway pressure (PAP). These devices generate positive pressure to prevent the collapse of the airway during sleep in different modalities, continuous PAP (CPAP), automatic adjustment PAP (APAP), and bilevel PAP (BPAP). Interfaces can be nasal (masks or pillows) or oronasal. PAP improves sleep quality and may reduce the health complications associated with untreated OSA, such as subjective and objective sleepiness and accidents [1, 2, 10]. Therapeutic success depends on patient compliance. Some patients do not use PAP for the minimum number of hours required, while others terminate treatment or refuse to even start therapy. PAP compliance rates of between 50 and 80% have been reported [11,12,13]. There are a number of different variables that can interfere with access and adherence to therapy. These include lack of health coverage, patient sociocultural and psychological characteristics, insufficient physician knowledge, lack of access to well-trained professionals, and the influence of early experience with PAP (e.g., clinical improvement, tolerability, adverse events) [11,12,13].
Only a handful of publications have evaluated accessibility and adherence to PAP in Latin America, reporting that between 40 and 60% of patients are not using the device 1 year after diagnosis of OSA [14,15,16]. Several factors that could influence access and adherence to treatment are particularly relevant in most Latin American countries. These include lack of financial coverage by the health system, the inability of a section of the population to meet the high costs of therapies, and sociocultural factors. For countries where these factors are important, there is a lack of multicenter data investigating their effect on access and adherence to PAP.
This multicenter study was designed to investigate accessibility and patient factors associated with adherence to PAP treatment in patients with moderate-severe OSA in Latin America. Specifically, the number of patients who had access to PAP and those who continued using it 12 months after the initial OSA diagnosis were determined along with mean adherence rates. We also identified potential barriers to diagnosis and access to therapy.
Methods
Study design
This multinational, multicenter, retrospective, cross-sectional study was conducted at nine sleep medicine referral centers from 6 Latin American: in Buenos Aires (Argentina), the Hospital de Clínicas of the University of Buenos Aires (center A) and the Hospital Austral of the Universidad Austral (center B); in Sao Paulo (Brazil), the Instituto do Sono (center C); in Santiago (Chile), Clínica Alemana (center D); in Bogotá (Colombia), the Fundación Neumológica Colombiana (center E); in Lima (Peru), the Clínica Anglo-Americana (center F); and in Mexico City, the Instituto Nacional de Enfermedades Respiratorias (center G), the Instituto Nacional de Ciencias Médicas y Nutrición (center H), and the Sleep Clinic of the Universidad Autónoma Metropolitana (center I). A study coordinator was designated at every center. The study protocol was approved by the independent ethics committee at each participating institution. All study procedures were performed in accordance with the ethical standards described in the 1964 Declaration of Helsinki and its later amendments. All patients gave their written informed consent to participate in the study, and confidentiality of their data was guaranteed.
Patients
The population recruited consisted of consecutive male and female adult patients (aged > 18 years) who had undergone a sleep study (polysomnography [PSG] or level 3 respiratory polygraphy [RP]) for suspected OSA, between 12 and 18 months prior to the study survey. Patients with severe cardiovascular, respiratory, neurological, or psychiatric comorbidities were excluded. To be included, patients had to have a diagnosis of moderate to severe OSA (apnea-hypopnea index [AHI] ≥ 15/h) determined by full in-lab PSG or RP in the sleep laboratory or at home. All the diagnostic procedures were performed following the AASM standards [17]. A subsequent supervised CPAP titration was also mandatory [18]. The recruitment goal was 100 patients per center.
OSA diagnosis
Patients underwent a full-night PSG, using a digital system at the sleep laboratory, during the subject’s habitual sleep schedule, or a home-based RP. PSG montage included at least three channels of electroencephalogram (EEG: F4, C4, O2), two channels of electrooculogram, three channels for surface electromyogram (submentonian, anterior tibialis muscle in both legs), electrocardiogram (one channel), airflow detection via thermocouple and nasal pressure, respiratory effort of the thorax and abdomen using piezoelectric sensors or RIP (respiratory inductance plethysmography), microphone for snoring, body position sensor, oxy-hemoglobin saturation (SpO2), and pulse rate.
Respiratory polygraphy studies were performed with portable devices (ApneaLink Plus, ResMed; Stardust 2, Philips) battery operated in a sleep laboratory or in the patient’s home. All patients were trained on the use of the device and were given written instructions on the procedure. All records were downloaded and manually analyzed with specific software.
Expert physicians in every center visually scored all PSGs using standardized criteria [17]. Obstructive sleep apnea was defined if there was a drop in the peak flow signal excursion by ≥ 90% of pre-event baseline with persistent respiratory effort, for ≥ 10 s. Hypopnea was defined as a ≥ 30% drop in flow signal for ≥ 10 s, associated with ≥ 3% desaturation or with an arousal [17]. The severity of OSA was calculated on the basis of the patient’s AHI (number of apneas and hypopneas per hour), and an AHI greater than 15 was classified as moderate-severe [17].
PAP training and titration
The decision to indicate PAP treatment followed the criteria proposed by the regional medical guidelines in accordance with AASM guidelines [1, 19,20,21]. After a moderate to severe OSA was diagnosed, a staff physician interviewed the patient and explained the implications of OSA and the reasons and benefits of PAP treatment. Patients were then scheduled for PAP testing and training (using a CPAP device) and mask fitting in the sleep clinic. Nasal masks were offered in the first order; if oral leak was inevitable or if the patient manifested not feeling comfortable, an oronasal mask was tested. Possible side effects of PAP were explained in detail (rhinitis, nasal congestion or dryness, conjunctival irritation, skin inflammation, or injury). PAP titration was performed through either an in-lab PSG guided (using an APAP device) or with APAP at home [17,18,19]. Objective data from every device was collected after this trial; mean and 95th percentile PAP pressure, effective pressure curve, nightly usage, leak, and residual AHI were evaluated in order to determine the effective pressure for PAP treatment [1, 18]. Titrations were considered optimal when patients used APAP at least 4 h per night, without significant leak (defined as > 24 LPM during ≥ 30% of usage time) and a residual AHI (estimated by the device) ≤ 5/h. Additionally, titrations were considered acceptable if the residual AHI was ≤ 10/h or ≤ 75% of basal AHI in severe OSA patients, with the same criteria for leak and time of use. Titrations that did not meet these criteria were repeated [18].
Indication of treatment and follow-up
After PAP titration, experts in sleep medicine informed each patient about the results of the studies, evaluated the tolerance to PAP, and reinforced the risks involved and the benefits of PAP treatment. In this medical visit, patients also received a written prescription for PAP, detailing specific settings and mask (according to the data obtained in the titration process) and basic education on the set-up of PAP treatment and its daily use. Thereafter, follow-up was arranged at regular intervals and also according to the specific requirements of the patients. APAP or bilevel positive pressure was indicated in selected cases, when patients presented difficulties in tolerate CPAP or if an effective pressure > 15 cm H2O was required [1, 18].
Data collection
The study coordinator of every center was responsible for data collection and surveys, after a specific and standardized training. Patient demographic and anthropometric data and details of health coverage were collected. OSA severity was determined based on the AHI.
A standardized telephone survey was administered by a group of trained interviewers in each center. This questionnaire has already been validated and applied in a previous study (see Appendix) [22]. Patients were asked if they started PAP treatment (Did you start PAP treatment?), if they were still on PAP (Are you still using PAP?), and how often they used the device (self-reported compliance; How many hours per night and how many nights per week do you use the machine?). Patients who terminated PAP therapy and those who never started treatment were questioned about their reasons for non-adherence, including questions related to therapy access and possible barriers (health coverage, bureaucratic problems, clear medical indication, contradictory indication by another physician, mask or PAP intolerance, patient predisposition, clinical improvement), and about any alternative treatments (e.g., oral appliance, surgery). The occurrence of adverse events was also asked as a potential reason of discontinuation (rhinitis, nasal congestion or dryness, conjunctival irritation, skin inflammation, or injury).
Definitions
Adequate adherence to CPAP was arbitrarily defined as device usage for at least 4 h/night on 5 nights per week, as the patients referred in the survey [1, 2]. Four categories of medical coverage were defined: (a) workers’ health insurance, including all systems with mixed contributions by workers, employers, and/or state; (b) federal health insurance, entirely supported by the government; (c) private health insurance; and (d) no coverage.
Several consensus or clinical practice guidelines recommend starting CPAP treatment for OSA when the AHI is ≥ 15/h, whether or not symptoms or comorbidities are present [1, 19,20,21]. This criterion was taken into consideration when designing the present study. However, other guidelines recommend CPAP treatment when the AHI is ≥ 30/h [2, 22]. Therefore, a post hoc analysis was conducted in the subgroup of patients with an AHI ≥ 30/h.
Statistical analysis
Continuous variables are reported as mean ± standard deviation or median with interquartile range. Continuous variables were analyzed using Student’s t test or Mann-Whitney test depending on their distribution. Dichotomous variables are reported as numbers and percentages. Differences between categorical variables were tested using the χ2 test. All tests were two-tailed, and p values < 0.05 were considered statistically significant. Univariate analyses were used to calculate the unadjusted and adjusted relative hazard ratio (HR) values for predictors of PAP discontinuation. Analyses were carried out using SPSS V.18.0 (Armonk, USA).
Results
Study cohort
A total of 1257 were surveyed and 880 answered the questionnaire (response rate 70%). All centers reached the recruitment goal of 100 patients apart from the one in Lima (Peru) that recruited 80 patients, due to logistical difficulties in the center. Comparing those who completed the interview and those who did not, no statistical differences were found in terms of age (53.8 ± 13.5 years vs 52.4 ± 12.1 years; p = 0.3), gender (males 69.9% vs 71.2; p = 0.2), BMI (32.2 ± 6.7 kg/m2 vs 30.5 ± 6.1 kg/m2; p = 0.08), and AHI (48.6 ± 27.6/h vs 45.2 ± 25.5/h; p = 0.07). We cannot infer whether the non-contacted patients were adherent to PAP treatment or not.
Patient demographic data at baseline are shown in Table 1 and summarized by a study center in Fig. 1. Mean age did not differ between centers, apart from older mean age at center A in Buenos Aires, which predominantly provides care to patients aged > 65 years. More than 80% of patients recruited in Lima, Santiago, and Buenos Aires center B were men, while the proportion of males was about 60% at other centers. With the exception of the sleep unit in Santiago (AHI 34 ± 17/h, body mass index [BMI] 27.5 ± 3.6 kg/m2), the average AHI was > 40/h and the BMI was > 30 kg/m2.

Comparative patient characteristics of each center: sex (% males), age (years old), body mass index (BMI), apnea-hypopnea index (AHI, ev/h). Study center: Hospital de Clínicas of the University of Buenos Aires (A); Hospital Austral of the Universidad Austral, Buenos Aires (B); Instituto do Sono, Sao Paulo, Brazil (C); Clínica Alemana, Santiago, Chile (D); Fundación Neumológica Colombiana, Bogotá, Colombia (E); Clínica Anglo-Americana, Lima, Peru (F); Instituto Nacional de Enfermedades Respiratorias, Mexico City (G); Instituto Nacional de Ciencias Médicas y Nutrición, Mexico City (H); and Sleep Clinic of the Universidad Autónoma Metropolitana, Mexico City (I)
Study findings
Overall, 36.9% of patients had private health insurance; 31.1% were covered by a social security system and 13.3% by federal health insurance; and 18.7% had no medical insurance coverage. Of the 880 patients enrolled, 490 (55.7%) initiated PAP treatment, 70 of whom (14%) terminated therapy during the first year. Therefore, 420 subjects (47.7%) were still using PAP at the time of the survey. Usage of PAP by study center is shown in Fig. 2. One of the Argentinian centers and the Peruvian sleep lab had the highest proportion of patients treated with PAP, while the Chilean and Brazilian centers had the lowest access rates. A total of 612 patients had an AHI of ≥ 30/h. Of these, 372 (60.8%) started PAP, with 48 (12.9%) terminating therapy, meaning that 324 patients (52.9%) were still under treatment at the time of questioning.

Access, use, and adherence to positive airway pressure (PAP) therapy by study center. Study center: Hospital de Clínicas of the University of Buenos Aires (A); Hospital Austral of the Universidad Austral, Buenos Aires (B); Instituto do Sono, Sao Paulo, Brazil (C); Clínica Alemana, Santiago, Chile (D); Fundación Neumológica Colombiana, Bogotá, Colombia (E); Clínica Anglo-Americana, Lima, Peru (F); Instituto Nacional de Enfermedades Respiratorias, Mexico City (G); Instituto Nacional de Ciencias Médicas y Nutrición, Mexico City (H); and Sleep Clinic of the Universidad Autónoma Metropolitana, Mexico City (I)
As patients reported in the survey, the most common reasons for not starting PAP in the overall population were factors related to the treating physician (unclear or absent indication, contradictions among physicians), followed by limited insurance coverage and patient factors, whereas insurance-related factors were the most common reasons for not starting PAP in the subgroup of patients with an AHI ≥ 30/h (Table 2).
Intolerance to PAP treatment was the main reason for discontinuing therapy, reported by 51/70 patients (10.4% of the study population who started PAP). Other reported reasons for terminating PAP were adverse events and clinical improvement (8/70 patients each; 1.6%). A total of 85% of PAP users stated that they were using their device for ≥ 4 h/night on 5 nights per week.
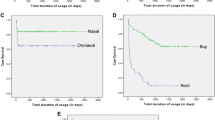
Regarding the characteristics of PAP treatment, CPAP devices were indicated in 80.5% of cases, APAP in 14.8%, and bilevel positive pressure in 4.7%. Nasal masks were indicated in 57.2% of patients, nasal pillows in 6.9%, and oronasal in 35.9%.
Patients using PAP at the time of the survey were significantly older and had a higher AHI than those who did not start or terminated therapy (Table 3). In addition, a higher proportion of PAP users were covered by a social health system (which provide full coverage of treatment) and significantly fewer had a federal insurance (no financial coverage) (Table 3).
Almost two-thirds of patients (60.2%) had full insurance coverage for OSA diagnostic studies, 10.8% had partial insurance coverage, and 28.9% had no coverage. For the PAP device and interface, 36.2% of patients had full coverage, 14.3% had partial coverage, and 49.5% had no insurance coverage and had to pay the full cost themselves. Eighty-three patients (9%) received an alternative treatment for OSA (upper airway surgery in 51 [5.8%], bariatric surgery in 13 [1.4%], an oral appliance in 11 [1.2%], or phoniatrics in 2 [0.2%]).
Discussion
Less than half of the patients with moderate-severe OSA included in our survey were treated with PAP within 1 year after their initial OSA diagnosis. Approximately 44% did not start treatment, and an additional 8% started on PAP but discontinued therapy within 1 year. Rates were similar when the analysis was restricted to patients with an AHI of ≥ 30/h. The number of individuals who opted for an alternative treatment was very low.
Adherence to PAP has been extensively studied, with most research focusing on individuals who start treatment and then discontinue therapy [23,24,25,26]. To our knowledge, only a few studies have investigated whether patients access PAP after a diagnosis of OSA [14,15,16, 27, 28]. A Canadian study in patients with an AHI of > 10/h reported that 31% did not initiate PAP treatment, and an additional 15% started therapy only to discontinue it later [27]. The proportion of patients who did not start PAP was similar in a study from China, and the PAP compliance rate was 51.8% at approximately 4 years after therapy initiation [28].
There are very few reports on PAP access and adherence in Latin America [14,15,16]. A study from Mexico found that 45% of patients did not start treatment after being diagnosed with OSA [15], while 30% of patients with moderate-severe OSA studied in Chile did not access CPAP treatment [16], and the proportion of patients not starting CPAP in Argentina was similar at 48% [14]. However, direct comparison between these studies is difficult because of the different methodology used. Pooling data from six countries, this study is the first multicenter study in Latin America to study PAP accessibility. Further, the finding that 44% of patients with an indication for PAP do not start therapy is consistent with existing published literature.
Interestingly, our results show that many patients perceived that their physicians were not clear about the PAP indication or they received conflicting advice from different medical professionals about the requirement for PAP. This is similar to previous data showing that 23% patients mentioned a similar issue when discussing barriers to PAP access [14]. The problem might reflect a lack of sleep specialists, and availability of sleep training programs in these countries. Whatever the underlying cause, it is a problem that could easily be solved by increasing knowledge about both diagnostic and therapeutic criteria among general practitioners [15], and has also been previously reported in other high-income countries [29]. Another factor that seems to limit access to treatment was lack of insurance coverage for the PAP device. This statement is supported by the fact that 36% of patients in the study population and 43% in the subgroup of patients with AHI ≥ 30/h reported that they did not initiate PAP treatment due to financial issues (lack of coverage mainly). Further, financial constraints was the most frequently reported reason by patients with severe OSA. The relatively high cost of these therapies may represent an important barrier to access treatment in low-income populations [15, 28]. In our study, approximately half of the sample, including some individuals who had some type of health coverage, had to fully pay the cost of the PAP device. Lack of health coverage in a large proportion of the population and the lack of PAP treatment coverage by some health insurers may lead to disparity in PAP treatment access.
We found that the type of health coverage was associated to the number of patients starting and continuing with CPAP treatment. Individuals with federal health insurance (no financial reimbursement for PAP treatment; lower income population) had a lower rate of PAP adherence. Conversely, patients who were covered by a workers’ health insurance (partial or full financial coverage of PAP treatment) had a much higher rate of PAP adherence. These results are consistent with previous work showing that access to PAP is lower in individuals of low socioeconomic status [30], and with surveys reporting health care disparities affecting access to treatment [15]. Importantly, our study underscores that lack of specific and effective health policies may result in unequal availability and access to health services and OSA diagnosis and treatment [15, 28, 29].
Surprisingly, 15% of patients in our study reported not even starting the process to accessing PAP treatment due to their perception of OSA not being an important heath condition that needed attention or they experienced mild symptoms. These findings are consistent with two previous studies that reported that almost one-third of patients did not initiate PAP treatment because they did not think it was necessary [14, 28]. Interventions targeted at reinforcing education and knowledge about OSA have been shown to be effective at increasing PAP adherence [31,32,33,34]. The proportion of patients in our study who started PAP but terminated therapy during the first year was 8%, similar to other reports [14, 16, 27, 28]. Intolerance was cited by patients as the most common reason for discontinuing treatment.
Of the variables analyzed, only age and AHI were significantly associated with adherence to PAP (BMI and sex had no effect). Currently, available evidence on this topic is contradictory, with some studies reporting an association between age, sex, and adherence [15, 30], and others finding no correlation between these variables [23, 27, 28, 35]. Data on sex and adherence are particularly inconsistent. An association between female gender and better adherence has been reported [26, 35], while other studies did not find any such association [27, 28], and others report better adherence among men [23, 36].
Our study has a number of limitations. For example, we used a telephone survey to assess compliance with PAP therapy rather than objective records of device usage. Self-reported compliance may be overestimated compared to objective measures, and thus, this could have biased our results [37]. Nevertheless, should the patients have overestimated their compliance, true adherence in our sample would have been lower and the access and adherence to treatment would be even lower. The collection of these data only once, over a broad period of time (12 to 18 months after diagnosis), without effective follow-up, may not depict the true story about the use of PAP. Additionally, other factors not considered in the survey could also have affected adherence to treatment and, therefore, our results should be interpreted with caution. On the other hand, we only included patients with an AHI ≥ 15/h, the most common cutoff for recommending the initiation of PAP treatment [1, 19,20,21]. However, other guidelines suggest initiating PAP treatment for patients with severe OSA (AHI ≥ 30/h) [2, 38], which should be taken into consideration when interpreting the study findings. A post hoc analysis found, however, that results in the severe OSA subgroup were consistent with those of the entire population. As this is a multicenter real-life study, there is an unavoidable heterogeneity of recording techniques (from PSG to RP), equipment used, PAP titration modalities (in-lab PSG guided or home titration with APAP), and particular clinical/therapeutic characteristics in every sleep center. All the procedures in the sleep laboratories included in this study were performed following the guidelines from the American Academy of Sleep Medicine. In our study, we also observed some degree of heterogeneity among the different subpopulations. For example, the Peruvian center could not reach the recruitment goal (80/100); patients from the Chilean center had lower AHI and BMI, and three study centers had a higher percentage of men, factors that escape the scope of this study.
Finally, as in all regions of the world, each country has a particular socioeconomic situation that may differ in some way from the neighboring country. In addition, in large countries such as some of those that make up Latin America, there are even socioeconomic differences between different regions within the same country.
According to the United Nations Economic Commission for Latin America and the Caribbean, Latin America is the most unequal region in the world [39]. There are also notably socioeconomic differences between and within countries in this region. Moreover, the sleep centers included in this study were restricted to tertiary care facilities, located in the most important urban centers, and therefore potentially limiting the generalizability of our results to other populations (e.g., rural populations). In our study, we did not formally assess socioeconomic factors (e.g., income, education) associated with PAP access beyond health coverage. Future studies should investigate whether socioeconomic factors including income, education, occupation, and immigration status affect PAP accessibility in Latin America.
The study has also a number of strengths. This is the first multicenter, multinational study on PAP access and adherence in Latin America, including a large population of moderate to severe OSA patients. The follow-up period was at least 1 year, reflecting long-term compliance, with only a small percentage of patients lost to follow-up. The use of telephone interviews gave us the opportunity to contact patients that do not return to the clinic. In addition, the study population included all OSA patients independent of their health coverage status, which allowed us to better evaluate differences in access to treatment.
Conclusions
In a sample of patients from Latin America with moderate to severe OSA, less than half started and continues to use PAP therapy. The most relevant factors limiting access to PAP therapy, referred by patients in a telephonic survey, were unclear or absent medical indication and financial limitations. Regardless of whether other factors not evaluated could also have potentially affected the adherence, these findings may suggest the need for more efficient health policies and advocacy to improve access to diagnosis and treatment of sleep disordered breathing. It is also necessary to improve education in sleep disorders among physicians and to increase awareness among the general population. In this sense, it is likely that the development of regional clinical guidelines can help disseminate knowledge about sleep disorders and unify diagnostic and treatment criteria.
References
Nogueira F, Nigro C, Cambursano H, Borsini E, Silio J, Avila J (2013) Practical guidelines for the diagnosis and treatment of obstructive sleep apnea syndrome. Medicina (B Aires) 73:349–362
Grupo Español de Sueño (2005) Consenso Nacional sobre el síndrome de apneas-hipopneas del sueño. Arch Bronconeumol 41(Supl 4):3–4
Eckert D, White D, Jordan A, Malhotra A, Wellman A (2013) Defining phenotypic causes of obstructive sleep apnea. Identification of novel therapeutic targets. Am J Respir Crit Care 188(8):996–1004
Tufik S, Santos-Silva R, Taddei JA, Bittencourt LRA (2010) Obstructive sleep apnea syndrome in the Sao Paulo epidemiologic sleep study. Sleep Med 11(5):441–446
Heinzer R, Vat S, Marques-Vidal P, Marti-Soler H, Andries D, Tobback N, Mooser V, Preisig M, Malhotra A, Waeber G, Vollenweider P, Tafti M, Haba-Rubio J (2015) Prevalence of sleep-disordered breathing in the general population: the HypnoLaus study. Lancet Respir Med 3:310–318
Arnardottir ES, Bjornsdottir E, Olafsdottir KA, Benediktsdottir B, Gislason T (2016) Obstructive sleep apnoea in the general population: highly prevalent but minimal symptoms. Eur Respir J 47(1):194–202
Marin JM, Carrizo SJ, Vicente E, Agusti AG (2005) Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet 365:1046–1053
Marti S, Sampol G, Muñoz X, Torres F, Roca A, Lloberes P, Sagalés T, Quesadaz P, Morell F (2002) Mortality in severe sleep apnoea/hypopnoea syndrome patients: impact of treatment. Eur Respir J 20:1511–1518
Pelletier-Fleury N, Meslier N, Gagnadoux F, Person C, Rakotonanahary D, Ouksel K, Fleury B, Racineux L (2004) Economic arguments for the immediate management of moderate to severe obstructive sleep apnoea syndrome. Eur Respir J 23:53–60
González Mangado N, Troncoso Acevedo M, Gómez García T (2014) Home ventilation therapy in obstructive sleep apnea-hypopnea syndrome. Arch Bronconeumol 50:528–534
Weaver T, Grunstein R (2008) Adherence to continuous positive airway pressure therapy the challenge to effective treatment. Proc Am Thorac Soc 5:173–178
Sawyer A, Gooneratne N, Marcus C, Ofer D, Richards K, Weaver T (2011) A systematic review of CPAP adherence across age groups: clinical and empiric insights for developing CPAP adherence interventions. Sleep Med Rev 15:343–356
Nogueira JF, Borsini E, Nigro C (2016) Estrategias para mejorar la adaptación al tratamiento con CPAP en pacientes con SAHOS. Rev Am Med Resp 4:365–377
Facundo N, De Luca M, Simonelli G, Vera D, Vera S, Rey R (2017) ¿Qué pasa con los pacientes luego de que se les diagnostica Apneas del Sueño? Rev Am Med Resp 2:41–47
Torre Bouscoulet L, López Escárcega E, Castorena Maldonado A, Vázquez García JC, Meza Vargas MS, Pérez-Padilla R (2007) Continuous positive airway pressure used by adults with obstructive sleep apneas after prescription in a public referral hospital in Mexico City. Arch Bronconeumol 43(1):16–21
Santín K, Jorquera J, Jordán J, Bajut F, Masalán P, Mesa T, Kuester G, Godoy J (2007) Uso de CPAP nasal en el largo plazo en síndrome de apnea-hipopnea del sueño. Rev Méd Chile 135:855–861
Berry RB, Brooks R, Gamaldo CE, Harding SM, Marcus CL, Vaughn BV, Tangredi MM (2012) The AASM manual for the scoring of sleep and associated events: rules, terminology and technical specifications, version 2.0. In: www.aasm.org/clinical-resources/scoring-manual. Accessed 24 July 2015
Morgenthaler TI, Aurora RN, Brown T, Zak R, Alessi C, Boehlecke B, Chesson AL, Friedman L, Kapur V, Maganti R, Owens J, Pancer J, Swick TJ (2008) Standards of Practice Committee of the AASM. Practice parameters for the use of autotitrating continuous positive airway pressure devices for titrating pressures and treating adult patients with obstructive sleep apnea syndrome: an update for 2007. Sleep 31(1):141–147
Epstein L, Kristo D, Strollo P, Friedman N, Malhotra A, Patil SP, Ramar K, Rogers R, Schwab R, Weaver E, Weinstein M (2009) Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med 5:263–276
Recomendações para o Diagnóstico e Tratamento da Síndrome da Apneia Obstrutiva do Sono no Adulto. Associação Brasileira do Sono. 2015. In: http://www.absono.com.br/absono. Accessed 24 July 2015
Detección, diagnóstico y tratamiento del síndrome de apnea obstructiva del sueño en el adulto en los tres niveles de atención. Guía de práctica clínica. Secretaría de Salud de México. In: http://www.imss.gob.mx/sites/all/statics/guiasclinicas/385GER.pdf . Accessed 24 July 2015
Nogueira JF, Simonelli G, Giovini V, Angellotti F, Borsini E, Ernst G, Nigro C (2018) Access to CPAP treatment in patients with moderate to severe sleep apnea in a Latin American City. Sleep Sci 11(3):174–182
McArdle N, Devereux G, Heidarnejad H, Engleman HM, Mackay TW, Douglas NJ (1999) Long-term use of CPAP therapy for sleep apnea/hypopnea syndrome. Am J Respir Crit Care Med 159:1108–1114
Meslier N, Lebrun T, Grillier-Lanoir V, Rolland N, Henderick C, Sailly J, Racineux J (1998) A French survey of 3,225 patients treated with CPAP for obstructive sleep apnoea: benefits, tolerance, compliance and quality of life. Eur Respir J 12:185–192
Pépin JL, Krieger J, Rodenstein D, Cornette A, Sforza E, Delguste P, Deschaux C, Grillier V, Lévy P (1999) Effective compliance during the first 3 months of continuous positive airway pressure: a European prospective study of 121 patients. Am J Respir Crit Care Med 160:1124–1129
Sin D, Mayers I, Godfrey C, Man W, Pawluk L (2002) Long-term compliance rates to continuous positive airway pressure in obstructive sleep apnea. A population-Based Study. Chest 121:430–435
Wolkove N, Baltzan M, Kamel H, Dabrusin R, Palayew M (2008) Long-term compliance with continuous positive airway pressure in patients with obstructive sleep apnea. Can Respir J 15(7):365–369
Wang Y, Gao W, Sun M, Chen B (2012) Adherence to CPAP in patients with obstructive sleep apnea in a Chinese population. Respir Care 57(2):238–243
Terán Santos J, Fernández García C, Cordero Guevara J (2000) Continuous positive airway pressure for obstructive sleep apnea syndrome: the current state of diagnostic resources and therapy in Spain. Arch Bronconeumol 36:494–499
Simon-Tuval T, Reuveni H, Greenberg-Dotan S, Oksenberg A, Tal A, Tarasiuk A (2009) Low socioeconomic status is a risk factor for CPAP acceptance among adult OSAS patients requiring treatment. Sleep 32(4):545–552
Meurice JC, Ingrand P, Portier F, Arnulf I, Rakotonanahari D, Fournier E, Philip-Joet F, Veale D (2007) A multicentre trial of education strategies at CPAP induction in the treatment of severe sleep apnoea-hypopnoea syndrome. Sleep Med 8:37–42
Haniffa M, Lasserson TJ, Smith I (2004) Interventions to improve compliance with continuous positive airway pressure for obstructive sleep apnoea. Cochrane Database Syst Rev 4:CD003531. https://doi.org/10.1002/14651858.CD003531.pub2
Dourado Rueda A, Santos-Silva R, Togeiro S, Tufik S, Azeredo Bittencourt L (2009) Improving CPAP compliance by a basic educational program with nurse support for obstructive sleep apnea syndrome patients. Sleep Sci 2(1):8–13
Deng T, Wang Y, Sun M, Chen B (2013) Stage-matched intervention for adherence to CPAP in patients with obstructive sleep apnea: a randomized controlled trial. Sleep Breath 17:791–801
Amfilochiou A, Tsara V, Kolilekas L, Gizopoulou E, Maniou C, Bouros D, Polychronopoulos V (2009) Determinants of continuous positive airway pressure compliance in a group of Greek patients with obstructive sleep apnea. Eur J Intern Med 6:645–650
Pelletier-Fleury N, Rakotonanahary D, Fleury B (2001) The age and other factors in the evaluation of compliance with nasal continuous positive airway pressure for obstructive sleep apnea syndrome. A Cox’s proportional hazard analysis. Sleep Med 2(3):225–232
Kribbs NB, Pack AI, Kline LR, Smith PL, Schwartz AR, Schubert NM, Redline S, Henry JN, Getsy JE, Dinges DF (1993) Objective measurement of patterns of nasal CPAP use by patients with obstructive sleep apnea. Am Rev Respir Dis 147:887–895
Arcos J, López V, Musetti A, Mamchur M, Gutiérrez M, Otaño N et al (2012) Trastornos respiratorios del sueño: Guías clínicas para el diagnóstico y tratamiento. Rev Méd Urug 28:274–308
Economic Commission for Latin America and the Caribbean (ECLAC), United Nations, Social Panorama of Latin America, 2016 (LC/PUB.2017/12-P), Santiago, 2017. In https://repositorio.cepal.org/bitstream/handle/11362/41599/4/S1700566_en.pdf. Accessed 10 May 2019
Acknowledgments
The authors want to acknowledge Victoria Santiago-Ayala, Yoaly Arana Lechuga, Javier Velázquez Moctezuma, Carolina Silva, Andrea Esguerra, Ricardo Silvestre Bello Carrera, and Rocío López Acuña for their invaluable contribution to the development of this research project. The material has been reviewed by the Walter Reed Army Institute of Research. There is no objection to its presentation and/or publication. The opinions or assertions contained herein are the private views of the author, and are not to be construed as official, or as reflecting true views of the Department of the Army or the Department of Defense. The investigators have adhered to the policies for protection of human subjects as prescribed in AR 70–25. English language editing assistance was provided by Nicola Ryan, independent medical writer, funded by ResMed.
Funding
ResMed provided financial support to cover the costs of the surveyors, data entry, and English language editing support. ResMed did not participate in the design of the study, nor in the collection and analysis of the data. Lía Bittencourt received a grant from Associação Fundo de Incentivo a Pesquisa (AFIP) and Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Grant number: 309336/2017-1.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Juan Facundo Nogueira has received financial support from ResMed, destinated to cover the cost of study procedures. Dalva Poyares has received financial support from ResMed, destinated to cover the cost of study procedures. Guido Simonelli declares that he has no conflict of interest. Sebastián Leiva declares that he has no conflict of interest. José Luis Carrillo-Alduenda has received financial support from ResMed, destinated to cover the cost of study procedures. María Angélica Bazurto has received financial support from ResMed, destinated to cover the cost of study procedures. Guadalupe Terán has received financial support from ResMed, destinated to cover the cost of study procedures. Matilde Valencia-Flores has received financial support from ResMed, destinated to cover the cost of study procedures. Leonardo Serra has received financial support from ResMed, destinated to cover the cost of study procedures. Jorge Rey de Castro has received financial support from ResMed, destinated to cover the cost of study procedures. Victoria Santiago-Ayala declares that she has no conflict of interest. Daniel Pérez-Chada has received financial support from ResMed, destinated to cover the cost of study procedures. María Eugenia Franchi declares that she has no conflict of interest. Ligia Lucchesi declares that she has no conflict of interest. Sergio Tufik declares that he has no conflict of interest. Lia Bittencourt has received financial support from ResMed, destinated to cover the cost of study procedures and received a grant from Associação Fundo de Incentivo a Pesquisa (AFIP) and Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Grant number: 309336/2017-1.
Ethical approval
This study has been approved by the Ethics committee of the participating institutions (Approval Certificate: 2014-195). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 24 kb)
Rights and permissions
About this article

Cite this article
Nogueira, J.F., Poyares, D., Simonelli, G. et al. Accessibility and adherence to positive airway pressure treatment in patients with obstructive sleep apnea: a multicenter study in Latin America. Sleep Breath 24, 455–464 (2020). https://doi.org/10.1007/s11325-019-01881-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11325-019-01881-9