
Abstract
Introduction
Endurance races have been associated with a substantial amount of adverse effects which could lead to chronic disease and long-term performance impairment. However, little is known about the holistic metabolic changes occurring within the serum metabolome of athletes after the completion of a marathon.
Objectives
Considering this, the aim of this study was to better characterize the acute metabolic changes induced by a marathon.
Methods
Using an untargeted two dimensional gas chromatography time-of-flight mass spectrometry metabolomics approach, pre- and post-marathon serum samples of 31 athletes were analyzed and compared to identify those metabolites varying the most after the marathon perturbation.
Results
Principle component analysis of the comparative groups indicated natural differentiation due to variation in the total metabolite profiles. Elevated concentrations of carbohydrates, fatty acids, tricarboxylic acid cycle intermediates, ketones and reduced concentrations of amino acids indicated a metabolic shift between various fuel substrate systems. Additionally, elevated odd-chain fatty acids and α-hydroxy acids indicated the utilization of α-oxidation and autophagy as alternative energy-producing mechanisms. Adaptations in gut microbe-associated markers were also observed and correlated with the metabolic flexibility of the athlete.
Conclusion
From these results it is evident that a marathon places immense strain on the energy-producing pathways of the athlete, leading to extensive protein degradation, oxidative stress, mammalian target of rapamycin complex 1 inhibition and autophagy. A better understanding of this metabolic shift could provide new insights for optimizing athletic performance, developing more efficient nutrition regimens and identify strategies to improve recovery.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Although physical activity has been proven to be substantially beneficial to human health (Ojiambo 2013), various negative effects including cardiovascular dysfunction (Webner et al. 2012), muscle damage (Howatson et al. 2010), increased propensity to upper respiratory tract infections (Robson-Ansley et al. 2012) and severe inflammation (Bonasia et al. 2015) have been associated with running extensive distances, such as that of endurance races. Even though these races have become increasingly popular, limited research is based on the elucidation of the effects of these races using a metabolomics approach. Metabolomics is defined as the identification and quantification of the small metabolites (< 1500 Da) present in a biological system in order to determine the physiological effects induced by a specific perturbation (Heaney et al. 2017). Since metabolites are typically the end-products of the genome, transcriptome and proteome, alterations in these are indicative of the overall physiological state of the investigated biological system (Heaney et al. 2017).
Previous metabolomics studies have indicated elevated concentrations of various carbohydrate/glycolysis intermediates, which suggest the utilization of free glucose as the preferred energy source during strenuous physical activity (Lewis et al. 2010; Salway 2012; Waśkiewicz et al. 2012). Furthermore, significant alterations to the tricarboxylic acid (TCA) cycle intermediates were induced by a marathon (Turer et al. 2014) and could be attributed to additional strain placed on the electron transport chain (ETC), causing an imbalanced NADH:NAD+ ratio (Esterhuizen et al. 2017). According to previous work (Stellingwerff 2012), free glucose and other carbohydrate stores can become depleted within approximately 90 min after the start of the race, which most likely lead to the utilization of alternative fuel substrates (lipids and amino acids) for energy production (Waśkiewicz et al. 2012). Increased lipolysis activity results in elevated serum glycerol and free fatty acids (Lewis et al. 2010; Waśkiewicz et al. 2012), the latter of which produce acetyl-CoA via β-oxidation and subsequent energy via the TCA cycle and ETC (Salway 2012). Furthermore, the increased synthesis of acetyl-CoA could also ascribe for the elevated ketone concentrations previously reported (Pechlivanis et al. 2010), as it is a key component of ketogenesis. In the event that the strenuous physical activity continues beyond the capacity of the athlete’s lipid stores, or if the traditional lipid oxidation pathways become saturated (Staron et al. 1989), the athlete’s metabolism shifts towards protein catabolism (resulting in reduced blood amino acid levels) in an attempt to synthesize the energy required to complete the marathon (Lewis et al. 2010). These amino acids are primarily oxidized to pyruvic acid and acetyl-CoA, both of which can serve as TCA cycle influx substrates for energy production (Salway 2012). Additionally, protein degradation has been shown to alter purine catabolism, resulting in elevated adenosine-monophosphate, inosine-monophosphate, hypoxanthine, xanthine, uric acid and allantoin (Turer et al. 2014), the latter of which is a uric acid derivative and a surrogate index of oxidative stress (Lewis et al. 2010).
Although these metabolomics studies provide some clues to the metabolic alterations that occur during strenuous physical activity such as endurance races, very few of these employed an untargeted metabolomics approach. Considering this, an untargeted two-dimensional gas chromatography time-of-flight mass spectrometry (GCxGC-TOFMS) metabolomics approach was used to holistically compare the serum metabolite profiles of 31 recreational marathon athletes before and after the completion of a marathon (42 km), in order to better characterize the acute metabolic changes induced by exercise stress.
2 Materials and methods
2.1 Participants
All participants completed a health and dietary questionnaire (including a menstrual cycle questionnaire for female participants) prior to the marathon in order to assess their eligibility. Individuals with food allergies, cardiovascular complications, musculoskeletal disorders/injuries, or those receiving anti-inflammatory treatment were excluded from the study. Athlete participation in this investigation was completely voluntary, and all the participants gave written and informed consent. A summary of the participant characteristics is presented in Table 1.
2.2 Clinical samples
Blood samples were collected by antecubital fossa venesection of 31 marathon athletes (19 males and 12 females) 24 h before and immediately after completing the Druridge Bay Marathon (Northumberland, UK). Pre-marathon samples were collected the day preceding the race (between 10 am and 6 pm) as a means of reducing additional metabolic changes induced by the venesection stress as well as to limit interference to the athletes’ pre-marathon regimens. The individuals were required to be in a hydrated, yet fasted state (for a minimum of 2 h) at time of baseline sample venesection. The samples were collected in standard 10 mL vacutainer vials, placed on ice and transported to the laboratory (Faculty of Health and Life Sciences, Department of Sport, Exercise and Rehabilitation at the Northumbria University in Newcastle upon Tyne, UK) for immediate processing. Briefly, the blood was allowed to clot for 30 min and centrifuged at 3000×g for 10 min. The supernatant (serum) was then extracted and immediately frozen (− 80 °C) before being transported (on dry ice) to the North-West University, Human Metabolomics: Laboratory of Infectious and Acquired Diseases. These serum samples were stored at − 80 °C until metabolomics analyses commenced.
2.3 Chemicals and reagents
Methoxamine hydrochloride, 3-phenylbutyric acid and bis(trimethylsilyl)-trifluoroacetamide (BSTFA) with 1% trimethylchlorosilane (TMCS) were purchased from Sigma-Aldrich (St. Louis, Missouri, USA) and the pyridine was from Merck (Darmstadt, Germany). The acetonitrile used, was an ultra-pure Burdick and Jackson brand (Honeywell International Inc., Muskegon, Michigan, USA) and hence did not require any further purification.
2.4 Sample extraction and derivatization
A total metabolome extraction was performed on all the collected serum samples, along with appropriate quality control (QC) samples. During this process, 50 µL of internal standard (3-phenylbutyric acid dissolved in a chloroform:methanol:water [1:3:1] solution; 0.45 μg/mL) was added to 50 µL of each serum sample. Hereafter, the samples were placed on ice before 300 µL of acetonitrile was added as a protein precipitation agent. Samples were then subjected to the REAX D-91126 vortex (Heidolph Instruments GmbH & Co.KG, Schwabach, Germany) for 2 min and centrifuged at 3500×g for 10 min at 4 °C. The supernatant of the biphasic solution was then transferred to a clean GC–MS sample vile and dried at 40 °C under a light stream of nitrogen gas for approximately 45 min. Hereafter, 25 µL of methoxamine hydrochloride dissolved in pyridine (15 mg/mL) was added to each sample and incubated at 50 °C for 90 min. Thereafter, 40 µL BSTFA with 1% TMCS was added, followed by derivatization for 60 min at 60 °C. Each derivatized sample was transferred to a new GC–MS vile containing a vile insert, and capped.
2.5 GCxGC-TOFMS analysis and processing
The derivatized samples were placed on a multi-purpose auto-sampler tray (Gerstel GmbH and co. KG, Mülheim van der Ruhr, Germany) in a randomized order, and analyzed using a Pegasus 4D GCxGC-TOFMS system (LECO Africa (Pty) Ltd, Johannesburg, South Africa), fitted with an Agilent 7890A GC and TOFMS (LECO Africa). During analyses, 1 µL of each sample was injected using a 1:3 split ratio. Purified helium was used as a carrier gas and set at a constant flow rate of 1 mL/min, while the injector temperature was set to operate at a constant 270 °C throughout the entire sample analysis. The primary oven was fitted with a Restek Rxi-5MS capillary column (30 m; 0.25 µm diameter and 0.25 µm film thickness) and programmed to start the run at an initial temperature of 70 °C for 2 min, followed by an increase of 4 °C/min until a final temperature of 300 °C was reached and maintained for 2 min. The secondary oven, equipped with a Restek Rxi-17 capillary column (1 m; 0.25 µm diameter and 0.25 µm film thickness), was set at an initial temperature of 85 °C, which was increased by 4.5 °C/min until a final temperature of 300 °C was reached and maintained for 2 min. The thermal modulator was set to pulse streams of cold and hot nitrogen gas every 3 s, for 0.5 s. The detector was set to disregard all mass spectra information for the first 400 s of each run to exclude solvent detection; however, this was still included on the time axis of the primary column to reflect accurate retention times. Additionally, the transfer line and ion source were respectively held at a constant of 270 °C and 220 °C for the entire run, with a detector voltage of 1600 V and filament bias of − 70 eV. Mass spectra were acquired at a rate of 200 ms/s, over a range of 50–800 m/z. The total run time per sample was 111.28 min. Following GCxGC-TOFMS analysis, 838 peaks were identified, which was processed using LECO Corporation’s ChromaTOF software (version 4.32), as described by Luies and Loots (2016).
2.6 Statistical analyses
Prior to statistical analysis, the dataset was normalized in relation to the internal standard and subjected to several “clean-up steps”, including a 50% zero filter, QC drift correction, QC coefficient of variation filter and zero value replacement (Fernandez et al. 2000; Luies and Loots 2016). Hereafter, a natural shifted log transformation was performed to correct for skewed variable distribution, as well as auto scaling to align all variables (Van den Berg et al. 2006) (exclusively during multivariate analysis).
Both multivariate and univariate statistical analyses were performed using MATLAB software (2012), adjusted with the PLS toolbox (2016), to identify the metabolite markers best describing the variation between the comparative groups. Multivariate approaches included principle component analysis (PCA) to determine whether a natural differentiation occurred between the comparative groups, and partial least square-discriminant analysis (PLS-DA) to characterize the group separation (Luies and Loots 2016). The univariate data analyses included a Wilcoxon signed rank test, corrected for multiple testing by the Benjamini–Hochberg procedure, to assess the statistical significance of each compound (Benjamini and Hochberg 1995; Rosner et al. 2006), while an independent effect size calculation (Wilcoxon signed effect size) was used to assess the practical significance of each detected metabolite (Tomczak and Tomczak 2014).
3 Results
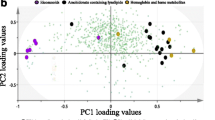
The PCA differentiation between serum metabolite profiles (Fig. 1) of the marathon athletes before and after the completion of the marathon was clearly defined. The total amount of variance explained by the first three principle components (PCs) (R2X cum) was 53%, of which PC1 accounted for 24%, PC2 for 20% and PC3 for 9%. Additionally, the PLS-DA model (results not shown) showed a modelling parameter R2Y (cum) of 48.81% for the total variance of the response Y, and a Q2 (cum) of 83.37%, indicating the cross-validation variation due to the response Y.

Principle component analysis scores plot showing clear differentiation of the serum samples of marathon athletes before (denoted by circles) and after (denoted by squares) the completion of a marathon. The variance accounted for are indicated in parenthesis. PC principle component
Since the aim of this study was to attain a holistic view of the altered human serum metabolome induced by a marathon, compounds with a PCA power value ≥ 0.5 or Wilcoxon p-value ≤ 0.017 (BH-critical value) or an effect size ω-value ≥ 0.3 were considered significant and interpreted based on their associated metabolic/biochemical pathways. This multi-statistical approach yielded an initial list of 78 metabolite markers, of which 70 metabolite markers could be annotated by comparison of their mass spectra and retention times to that of commercially available and in-house libraries developed from previously injected standards (see Table 2).
4 Discussion
The altered metabolite markers listed in Table 2 are indicative of the major metabolic pathways affected by the marathon and are mainly associated with the macro-fuel substrate utilization pathways (carbohydrates, lipids and amino acids) and the regulation thereof (TCA, oxidative phosphorylation [OXPHOS] and gut microbiome). These metabolite pathways, along with the intermittent dietary-associated metabolite markers, are comprehensively discussed below and schematically presented in Fig. 2.

A schematic representation of the altered serum metabolome induced by a marathon. The altered metabolites are either donated as increased (↑) or decreased (↓) relative to the pre-marathon group. FAD flavin adenine dinucleotide, FADH flavin adenine dinucleotide + hydrogen, NAD nicotinamide adenine dinucleotide, NADH nicotinamide adenine dinucleotide + hydrogen, ATP adenosine triphosphate, ADP adenosine diphosphate
Various carbohydrate metabolites were significantly elevated following the marathon and can be ascribed to gluconeogenic influx (MacLaren and Morton 2012) and a reduced insulin secretion (Richter et al. 1992), which is typically induced by an initial depletion of glucose and glycogen stores occurring approximately 90 min after the start of a marathon (exercise intensity dependent) at a VO2max > 75% (Stellingwerff 2012). The reduced insulin concentrations temporarily inactivate insulin-dependent glucose uptake systems (i.e. GLUT 4 transporters and glucokinase) (Salway 2012), preventing glucose absorption into cells. This could ascribe for the post-marathon elevations in serum glucose concentrations and various other associated metabolites, including glucaric acid (Żółtaszek et al. 2008) and mannose (Hu et al. 2016) as well as the elevated concentrations of gluconeogenesis-associated metabolites, i.e. myo-inositol (Eisenberg and Parthasarathy 1987), erythritol (synthesized via erythrose-4-phosphate in pentose phosphate pathway) (Hootman et al. 2017), glycerol and glyceric acid (Salway 2012; Wadman et al. 1976). Furthermore, the elevated concentrations of pyruvic acid observed in the post-marathon samples were anticipated since it is an end-product of the glycolysis pathway which feeds into the TCA cycle for further ATP production (Salway 2012). This is confirmed by the accumulation of various TCA cycle intermediates such as α-ketoglutaric acid, succinic acid, citric acid, fumaric acid and malic acid (Qiang 2015), which also indicate the accumulation of circulating NADH/FADH2 molecules (Esterhuizen et al. 2017) as a result of a saturated ETC activity. It is also important to mention that many of the aforementioned carbohydrate metabolites, along with elevated concentrations of mannose (Hu et al. 2016), sorbose (Guzik and Stachowicz 2016), mannitol (McNutt 2000), tagatofuranose (Kroger et al. 2006), and threonic acid (an ascorbic acid derivative) (Simpson and Ortwerth 2000), are well-known constituents of fruits/fruit juices, vegetables/vegetable juices, peanuts, energy bars, energy drinks and various other ergogenic aids consumed by athletes during the course of a marathon (Jeukendrup 2011; Pfeiffer et al. 2012).
The reduction in intracellular glucose due to the aforementioned cellular uptake inhibition is known to activate lipolysis of free and adipose tissue-bound triacylglycerol (TAG) (MacLaren and Morton 2012) as alternative fuel substrates. This is substantiated by the elevated concentrations of serum glycerol, monopalmitin and various free fatty acids (lauric acid, palmitic acid, palmitoleic acid, 11-eicosenoic acid, 11,14-eicosadienoic acid, myristoleic acid, α-linolenic acid, 5-dodecenoic acid, linoleic acid and oleic acid) (Kujala et al. 2013; Lewis et al. 2010; Peake et al. 2014; Waśkiewicz et al. 2012). Additionally, accumulated 3-hydroxy acids (β-hydroxyhexanoic acid) and 3-keto acids (β-hydroxy-α,β-didehydrosebacic acid) are indications of a saturated β-oxidation pathway, ascribed to the inhibition of the rate-limiting enzyme, β-hydroxyacyl dehydrogenase, which is pursued by 3-ketoacyl-CoA thiolase. This saturated β-oxidation pathway results in the catabolism of the accumulated fatty acids via α-oxidation (Roe and Ding 2001), thus substantiating the elevated concentrations of α-hydroxyoctanoic acid (C8; an α-oxidation intermediate) and the odd-chain fatty acids (OCFA; tridecanoic acid [C13], pentadecanoic acid [C15], heptadecanoic acid [C17] and 10-heptadecenoic acid [C17:1]) detected in the post-marathon serum. It should, however, be mentioned that these OCFA may also arise from elevated dietary intake (Jenkins et al. 2017) and/or autophagy of various cellular constituents during extensive energy-requiring states (Singh and Cuervo 2011). Nevertheless, irrespective of their origins, these OCFAs are ultimately catabolized to propionyl-CoA (Pfeuffer and Jaudszus 2016), hence the elevated β-hydroxypropionic acid observed in the post-marathon serum. The elevated concentrations of β-hydroxybutyric acid and acetoacetic acid are anticipated, as these are alternative fuel substrates for the brain (Cahill and Vech 2003) and skeletal muscles (Holloszy and Coyle 1984) in hypoglycemic states, and could also be an indication of an imbalanced redox state (Esterhuizen et al. 2017; Salway 2012). Furthermore, the post-marathon elevations of malonic acid typically indicate the accumulation of malonyl-CoA, which is a long-chain fatty acid (LCFA) transport inhibitor (Salway 2012) and could therefore be an additional reason for the increased cytosolic LCFAs (palmitic acid, palmitoleic acid, 11-eicosenoic acid, 11,14-eicosadienoic acid, myristoleic acid, α-linolenic acid, linoleic acid and oleic acid).
Most amino acids are catabolized into TCA cycle substrates via propionyl-CoA, succinyl-CoA, pyruvic acid or acetyl-CoA, depending on the specific amino acid (Salway 2012). Reduced concentrations of amino acids (serine, glycine, alanine, aspartic acid, phenylalanine, tyrosine, threonine and methionine) and altered amino acid-associated metabolite concentrations [dimethylglycine (Holm et al. 2003), pyroglutamic acid (Kumar and Bachhawat 2012), indole-3-acetic acid (Salway 2012) and glutaric acid (Peake 2016)] were detected in the post-marathon serum, which indicate amino acid catabolism during the marathon. Furthermore, elevated concentrations of α-hydroxybutyric acid (an intermediate in the threonine/methionine pathway), further supports the aforementioned NADH:NAD+ imbalance, ketoacidosis, reduced insulin secretion and impaired glucose absorption (Gall et al. 2010). Additionally, elevated p-hydroxyphenylacetic acid and p-hydroxyphenyllactic acid could be indicative of mild liver injury/damage (Ghoraba et al. 2014; Liebich and Pickert 1985), which concur with previous findings (Jastrzebski et al. 2015; Lippi et al. 2011).
In accordance with previous findings (Pechlivanis et al. 2010), reduced serum concentrations of the branched-chain amino acids (BCAAs) isoleucine (0.05 vs 0.02 µg/mL, p = 0.018), valine and leucine were detected in the post-marathon samples, while their catabolism intermediates i.e. α-ketoisovaleric acid, β-hydroxyisobutyric acid (valine metabolites) and α-ethylhyrdracrylic acid (allo-isoleucine metabolism) (Wendel et al. 1989), were significantly elevated. Allo-isoleucine catabolism intermediates may serve as alternative substrates in the valine catabolism pathway (Ryan 2015), however, since the valine catabolism intermediates remained elevated in the post-marathon serum it can be deduced that allo-isoleucine is instead catabolized to α-ethylhydracrylic acid (Korman et al. 2005) via α-keto-β-methylvaleric acid (explaining its reduced concentrations post-marathon) with the subsequent production of FADH2 (Korman et al. 2005). The elevated concentrations of β-hydroxyisovaleric acid detected post-marathon is typically associated with ketone rich environments (as observed in the current investigation), resulting from increased leucine catabolism and the subsequent production of isovaleryl-CoA`23 (Mock et al. 2011). This metabolite is also a well-known constituent of athlete supplementation (Brioche et al. 2016) and could be elevated due to dietary ingestion during the marathon. Furthermore, reduced concentrations of these BCAAs, in particular leucine, results in mammalian target of rapamycin complex 1 (mTOR1) inhibition (Laplante and Sabatini 2009), which in turn activates various catabolic processes such as autophagy (of organelle and plasma membrane constituents) to release additional embedded fuel substrates (Singh and Cuervo 2011). mTOR1 inhibition can also be induced by other factors including elevated 5′-AMP-activated protein kinase during energy deprivation, reduced oxygen levels, reduced essential amino acids and inflammation (Laplante and Sabatini 2009), all of which are associated with endurance races and evidently occur in the marathon athletes investigated in this study. Considering that autophagy contributes to elevated amounts of cellular debris, the aforementioned accumulation of fatty acids (especially the OCFAs) in the post-marathon serum may also be explained by the autophagosomal degradation of phospholipids, sphingolipids (Kishimoto et al. 1973; Maes et al. 1996) and phytosphingosines (Kitamura et al. 2017; Kondo et al. 2014) found in cell and organelle membranes. Additionally, the elevated concentrations of squalene and 5-pregnene-3β,20α-diol in the post-marathon serum suggest cholesterol degradation (Charlton-Menys and Durrington 2007; Salway 2012), further supporting the activation of autophagy as the latter is a common constituent in cell membranes (Salway 2012). Elevated 5-pregnene-3β,20α-diol (also known as 20α-dihydropregnenolone) post-marathon also indicates steroid metabolism activation via cholesterol catabolism as it is produced by the reduction of pregnenolone via 20-hydroxysteroid dehydrogenase (Ebner et al. 2006). Pregnenolone is a precursor for the production of aldosterone and cortisol, the latter of which stimulates lipolysis, gluconeogenesis and protein catabolism (Salway 2012).
Furthermore, a significant decrease in α-aminomalonic acid concentrations was observed in the post-marathon serum samples. Although the precise origin of this metabolite is unknown, it has been associated with abnormal protein oxidation, macrophage accumulation, non-essential amino acid oxidation via reactive oxygen species and pulmonary arterial hypertension (Bujak et al. 2016).
The microbiome plays a crucial role in many essential metabolic processes required during strenuous exercise, including the regulation of energy metabolism, oxidative stress and inflammatory response pathways (Mach and Fuster-Botella 2017). To this end, various microbial-associated metabolites (i.e. tagatofuranose, talofuranose, ethyl-α-d-glucopyranoside, arabitol, indole-3-propionic acid and d-rhamnose) were significantly altered in the post-marathon samples. Most of these metabolites are synthesized from host carbohydrate intermediates, either via catabolism or fermentation processes [arabitol: a sugar alcohol produced from arabinose/glucose (Kumdam et al. 2014); and ethyl-α-d-glucopyranoside: an ethnolysis product from glucose (Hu et al. 2013)]. Indole-3-propionic acid is the deamination product of tryptophan, produced by gut microbes (e.g. Clostridium sporogenes) (Wikoff et al. 2009) and further supports the notion of reduced amino acids. The reduced concentrations of d-rhamnose, a component of most Gram-positive bacterial cell walls (Mistou et al. 2016), contradict the above-mentioned microbial product elevations. Since the particular nature of this reduction following completion of the marathon is unclear, it warrants future investigation.
In addition to these endogenously and microbially produced metabolites, elevated concentrations of ibuprofen were also observed post-marathon. Ibuprofen is a well-known non-steroidal, anti-inflammatory drug (Nieman et al. 2006) commonly used by athletes for preventing muscle damage/soreness and inflammation and was most likely consumed by some athletes prior to/during the marathon (Mcanulty et al. 2007).
5 Conclusion
The results of this metabolomics investigation suggest that the body utilizes various fuel substrate pathways to comply with the high energy demands required during the marathon, including catabolism of carbohydrates, lipids (β-oxidation and α-oxidation) and amino acids, as well as the activation of ketogenesis and autophagy via mTOR1 inhibition. Considering the results of the current investigation and previous literature, the possible cascade of events contributing to this metabolic “snapshot” could be summarized as follows: (a) A proposed initial reduction in carbohydrate catabolism and glucose uptake via insulin-dependent transporters lead to glycolysis dysregulation, ketogenesis activation and increased serum glucose. (b) A metabolic shift towards fatty acid utilization (from either endogenous or dietary TAGs) is induced, which (c) overwhelms/saturates the β-oxidation pathway, resulting in the α-oxidation of fatty acids. (d) Amino acids (from either endogenous or dietary protein catabolism) are also used as alternative fuel substrates, resulting in (e) mTOR1 inhibition and autophagy as the body desperately tries to generate the necessary fuel substrates to comply with the energy demand. (f) Lastly, various metabolic processes are activated to reduce oxidative stress and regulate/correct the redox imbalance.
Possible limitations of this study include human genotype/phenotype variation (an inevitable confounder) and the uncontrolled dietary intake of the athletes during the marathon. However, convincing athletes to deviate from their individualized supplementation protocols would be extremely difficult, if not impossible. Validation using a larger sample cohort could further substantiate the current findings. Nonetheless, these findings indicate the extensive metabolic changes induced by the marathon perturbation. Possible future prospects could be to investigate the effects of supplementing with amino acids, pre- and/or pro-biotics, and β-hydroxyisovaleric acid as a means of improving aerobic exercise performance, reduce skeletal muscle/liver damage, and enhance recovery.
Data availability
The current analysis is part of a larger study consisting of multiple aims which are being drafted into various manuscripts. Considering this, the datasets generated from this investigation are not publically available, but can be acquired from the corresponding author on reasonable request. The authors declare that all the results included within this study have been presented clearly, honestly and without fabrication, falsification, or inappropriate data manipulation.
References
Benjamini, Y., & Hochberg, Y. (1995). Controlling the false discovery rate: A practical and powerful approach to multiple testing. Journal of the Royal Statistical Society, 57, 289–300.
Bonasia, D. E., Rosso, F., Cottino, U., & Rossi, R. (2015). Exercise-induced leg pain. Asia-Pacific Journal of Sports Medicine, Arthroscopy, Rehabilitation and Technology, 2, 73–84.
Brioche, T., Pagano, A. F., Py, G., & Chopard, A. (2016). Muscle wasting and aging: Experimental models, fatty infiltrations, and prevention. Molecular Aspects of Medicine, 50, 56–87.
Bujak, R., Mateo, J., Blanco, I., Izquierdo-Garcia, J. L., Dudzik, D., Markuszewski, M. J., et al. (2016). New biochemical insights into the mechanisms of pulmonary arterial hypertension in humans. PLoS ONE, 11, 1–14.
Cahill, G. F., & Vech, R. L. (2003). Ketoacids? Good medicine? American Clinical and Climatological Association, 114, 149–163.
Charlton-Menys, V., & Durrington, P. N. (2007). Human cholesterol metabolism and therapeutic molecules. Experimental Physiology, 93, 27–42.
Ebner, M. J., Corol, D. I., Havlikova, H., Honour, J. W., & Fry, J. P. (2006). Identification of neuroactive steroids and their precursors and metabolites in adult male rat brain. Endocrinology, 147, 179–190.
Eigenvector Reserch. (2016). PLS_Toolbox 8.2.1 (Version 8.2.1). Manson: Eigenvector Reserch Inc.
Eisenberg, F., & Parthasarathy, R. (1987) Measurement of biosynthesis of myo-inositol from glucose 6-phosphate. Methods in Enzymology, 141, 127–143.
Esterhuizen, K., van der Westhuizen, F. H., & Louw, R. (2017). Metabolomics of mitochondrial disease. Mitochondrion, 35, 97–110.
Fernandez, J. A. M., Vida, C. B., & Glahn, V. P. (2000). Zero replacement in compositional data sets. In H. A. L. Kiers, J.-P. Rasson, P. J. F. Groenen & M. Schader (Eds.), Data analysis, classification, and related methods (pp. 155–160). Berlin: Springer.
Gall, W. E., Beebe, K., Lawton, K. A., Adam, K. P., Mitchell, M. W., Nakhle, P. J., et al. (2010). Alpha-hydroxybutyrate is an early biomarker of insulin resistance and glucose intolerance in a nondiabetic population. PLoS ONE, 5, e10883.
Ghoraba, D. A., Mohamed, M. M., & Zaki, O. K. (2014). Screening of diseases associated with abnormal metabolites for evaluation of HPLC in organic aciduria profiling. Egyptian Journal of Medical Human Genetics, 15, 69–78.
Guzik, G. P., & Stachowicz, W. (2016). Study on radiation-induced radicals giving rise to stable EPR signal suitable for the detection of irradiation in L-sorbose-containing fruits. Nukleonika, 61, 461–465.
Heaney, L. M., Deighton, K., & Suzuki, T. (2017) Non-targeted metabolomics in sport and exercise science. Journal of Sports Sciences. https://doi.org/10.1080/02640414.2017.1305122
Holloszy, J. O., & Coyle, E. F. (1984). Adaptations of skeletal muscle to endurance exercise and their metabolic consequences. Journal of Applied Physiology, 56, 831–838.
Holm, P. l. I., Ueland, P. M., Kvalheim, G., & Lien, E. A. (2003). Determination of choline, betaine, and dimethylglycine in plasma by a high-throughput method based on normal-phase chromatography–tandem mass spectrometry. Clinical Chemistry, 49, 286–294.
Hootman, K. C., Trezzi, J. P., Kraemer, L., Burwell, L. S., Dong, X., Guertin, K. A., et al. (2017) Erythritol is a pentose-phosphate pathway metabolite and associated with adiposity gain in young adults. Proceedings of the National Academy of Sciences, 114, 4233–4240.
Howatson, G., McHugh, M. P., Hill, J. A., Brouner, J., Jewell, A. P., van Someren, K. A., et al. (2010). Influence of tart cherry juice on indices of recovery following marathon running. Scandinavian Journal of Medicine and Science in Sports, 20, 843–852.
Hu, X., Shi, Y., Zhang, P., Miao, M., Zhang, T., & Jiang, B. (2016). D-Mannose: Properties, production, and applications: An overview. Comprehensive Reviews in Food Science and Food Safety, 15, 773–785.
Hu, X., Wu, L., Wang, Y., Song, Y., Mourant, D., Gunawan, R., et al. (2013). Acid-catalyzed conversion of mono- and poly-sugars into platform chemicals: Effects of molecular structure of sugar substrate. Bioresource Technology, 133, 469–474.
Jastrzebski, Z., Zychowska, M., Radziminski, L., Konieczna, A., & Kortas, J. (2015). Damage to liver and skeletal muscles in marathon runners during a 100 km run with regard to age and running speed. Journal of Human Kinetics, 45, 93–102.
Jenkins, B. J., Seyssel, K., Chiu, S., Pan, P. H., Lin, S. Y., Stanley, E., et al. (2017). Odd chain fatty acids; new insights of the relationship between the gut microbiota, dietary intake, biosynthesis and glucose intolerance. Scientific Reports, 7, 1–8.
Jeukendrup, A. E. (2011). Nutrition for endurance sports: Marathon, triathlon, and road cycling. Journal of Sport Science, 29, 91–99.
Kishimoto, Y., Williams, M., Moser, H. W., Hignite, C., & Biemann, K. (1973). Branched-chain and odd-numbered fatty acids and aldehydes in the nervous system of a patient with deranged vitamin B12 metabolism. Journal of Lipid Research, 14, 69–77.
Kitamura, T., Seki, N., & Kihara, A. (2017). Phytosphingosine degradation pathway includes fatty acid α-oxidation reactions in the endoplasmic reticulum. Proceedings of the National Academy of Science, 114, 1–8.
Kondo, N., Ohno, Y., Yamagata, M., Obara, T., Seki, N., Kitamura, T., et al. (2014). Identification of the phytosphingosine metabolic pathway leading to odd-numbered fatty acids. Nature Communications, 5338, 1–11.
Korman, S. H., Andresen, B. S., Zeharia, A., Gutman, A., Boneh, A., & Pitt, J. J. (2005). 2-Ethylhydracrylic aciduria in short/branched-chain acyl-CoA dehydrogenase deficiency: Application to diagnosis and implications for the R-pathway of isoleucine oxidation. Clinical Chemistry, 51, 610–617.
Kroger, M., Meister, K., & Kava, R. (2006). Low-calorie sweeteners and other sugar substitutes: A review of the safety issues. Comprehensive Reviews in Food Science and Food Safety, 5, 35–47.
Kujala, U. M., Mäkinen, V.-P., Heinonen, I., Soininen, P., Kangas, A. J., Leskinen, T. H., et al. (2013). Long-term leisure-time physical activity and serum metabolome. Circulation, 127, 340–348.
Kumar, A., & Bachhawat, A. K. (2012). Pyroglutamic acid: Throwing light on a lightly studied metabolite. Current Science, 102, 288–297.
Kumdam, H., Murthy, S. N., & Gummadi, S. N. (2014). Arabitol production by microbial fermentation—biosynthesis and future applications. International Journal of Sciences and Applied Research, 1, 1–12.
Laplante, M., & Sabatini, D. M. (2009). mTOR signaling at a glance. Journal of Cell Science, 122, 3589–3594.
Lewis, G. D., Farrell, L., Wood, M. J., Martinovic, M., Arany, Z., Rowe, G. C., et al. (2010). Metabolic signatures of exercise in human plasma. Science Translational Medicine, 2, 33–37.
Liebich, H. M., & Pickert, A. (1985). Gas chromatographic profiling of phenolic acids in urine of patients with cirrhosis of the liver. Journal of Chromatography, 338, 25–32.
Lippi, G., Schena, F., Montagnana, M., Salvagno, G. L., Banfi, G., & Guidi, G. C. (2011). Significant variation of traditional markers of liver injury after a half-marathon run. European Journal of Internal Medicine, 22, E36–E38.
Luies, L., & Loots, D. T. (2016). Tuberculosis metabolomics reveals adaptations of man and microbe in order to outcompete and survive. Metabolomics, 12, 1–9.
Mach, N., & Fuster-Botella, D. (2017). Endurance exercise and gut microbiota: A review. Journal of Sport and Health Science, 6, 179–197.
MacLaren, D., & Morton, J. (2012). Biochemistry for sport and exercise metabolism (1 ed.). West Sussex: Wiley
Maes, M., Smith, R., Christophe, A., Cosyns, P., Desnyder, R., & Meltzer, H. (1996). Fatty acid composition in major depression: Decreased w3 fractions in cholesteryl esters and increased C20:4w6/C20:5w3 ratio in cholesteryl esters and phospholipids. Journal of Affective Disorders, 38, 35–46.
MATLAB. (2012). MATLAB and Statistics toolbox (Version 2012b). Natick: The MathWorks Inc.
Mcanulty, S. R., Owens, J. T., Mcanulty, L. S., Nieman, D. C., Morrow, J. D., Dumke, C. L., & Milne, G. L. (2007). Ibuprofen use during extreme exercise: Effects on oxidative stress and PGE2. Medicine and Science in Sports and Exercise, 39, 1075–1079.
McNutt, K. (2000). What clients need to know about sugar replacers. Journal of the American Dietetic Association, 100, 466–469.
Mistou, M. Y., Sutcliffe, I. C., & van Sorge, N. M. (2016). Bacterial glycobiology: Rhamnose-containing cell wall polysaccharides in Gram-positive bacteria. FEMS Microbiol Review, 40, 464–479.
Mock, D. M., Stratton, S. L., Horvath, T. D., Bogusiewicz, A., Matthews, N. I., Henrich, C. L., et al. (2011). Brain, behavior, and immunity urinary excretion of 3-hydroxyisovaleric acid and 3-hydroxyisovaleryl carnitine increases in response to a leucine challenge in marginally biotin-deficient humans. Journal of Nutrition, 141, 1925–1930.
Nieman, D. C., Henson, D. A., Dumke, C. L., Oley, K., McAnulty, S. R., Davis, J. M., et al. (2006). Ibuprofen use, endotoxemia, inflammation, and plasma cytokines during ultramarathon competition. Brain, Behavior, and Immunity, 20, 578–584.
Ojiambo, R. M. (2013). Physical activity and well-being: A review of the health benefits of physical activity on health outcomes. Journal of Applied Medical Sciences, 2, 69–78.
Peake, J. M., Tan, S. J., Markworth, J. F., Broadbent, J. A., Skinner, T. L., & Cameron-Smith, D. (2014). Metabolic and hormonal responses to isoenergetic high-intensity interval exercise and continuous moderate-intensity exercise. American Journal of Pathology, 307, 539–552.
Peake, R. W. A. (2016). Seizures, dystonia, and spasms in a 14-year-old child. Clinical Chemistry, 62, 1159–1168.
Pechlivanis, A., Kostidis, S., Saraslanidis, P., Petridou, A., Tsalis, G., Mougios, V., et al. (2010). H NMR-based metabonomic investigation of the effect of two different exercise sessions on the metabolic fingerprint of human urine. Journal of Proteome Research, 9, 6405–6416.
Pfeiffer, B., Stellingwerff, T., Hodgson, A. B., Randell, R., Pottgen, K., Res, P., et al. (2012). Nutritional intake and gastrointestinal problems during competitive endurance events. Medicine and Science in Sports and Exercise, 44, 344–351.
Pfeuffer, M., & Jaudszus, A. (2016). Pentadecanoic and heptadecanoic acids: Multifaceted odd-chain fatty acids. Advances in Nutrition, 7, 730–734.
Qiang, F. (2015). Effect of malate-oligosaccharide solution on antioxidant capacity of endurance athletes. The Open Biomedical Engineering Journal, 9, 326–329.
Richter, E. A., Turcotte, L., Hespel, P., & Kiens, B. (1992). Metabolic responses to exercise: Effects of endurance training and implications for diabetes. Diabetes Care, 15, 1767–1776.
Robson-Ansley, P., Howatson, G., Tallent, J., Mitcheson, K., Walshe, I., Toms, C., et al. (2012). Prevalence of allergy and upper respiratory tract symptoms in runners of the London marathon. Medicine & Science in Sports & Exercise, 44, 999–1004.
Roe, C. R., & Ding, J. (2001). Mitochondrial fatty acid oxidation disorders. In The online metabolic and molecular bases of inherited disease. New York: The McGraw-Hill Companies.
Rosner, B., Glynn, R. J., & Lee, M.-L. T. (2006). The Wilcoxon signed rank test for paired comparisons of clustered data. Biometrics, 62, 185–192.
Ryan, R. O. (2015). Metabolic annotation of 2-ethylhydracrylic acid. Clinical Chimica Acta, 448, 91–97.
Salway, J. G. (2012). Medical biochemistry at a glance (3rd ed.). Oxford: Wiley.
Simpson, G. L. W., & Ortwerth, B. J. (2000). The non-oxidative degradation of ascorbic acid at physiological conditions. Biochimica et Biophysica Acta, 1501, 12–24.
Singh, R., & Cuervo, A. M. (2011). Autophagy in the cellular energetic balance. Cellular Metababolism, 13, 495–504.
Staron, R. S., Hikida, R. S., Murray, T. F., Hagerman, F. C., & Hagerman, M. T. (1989). Lipid depletion and repletion in skeletal muscle following a marathon. Journal of the Neurological Sciences, 94, 29–40.
Stellingwerff, T. (2012). Case study: Nutrition and training periodization in three elite marathon runners. International Journal of Sport Nutrition and Exercise Metablism, 22, 392–400.
Tomczak, M., & Tomczak, E. (2014). The need to report effect size estimates revisited: An overview of some recommended measures of effect size. Trends in Sport Science, 1, 19–25.
Turer, A. T., Lewis, G. D., O’Sullivan, J. F., Elmariah, S., Mega, J. L., Addo, T. A., et al. (2014). Increases in myocardial workload induced by rapid atrial pacing trigger alterations in global metabolism. PLoS ONE, 9, 1–9.
Van den Berg, R. A., Hoefsloot, H. C., Westerhuis, J. A., Smilde, A. K., & van der Werf, M. J. (2006). Centering, scaling, and transformations: Improving the biological information content of metabolomics data. BMC Genomics, 7, 142.
Wadman, S. K., Duran, M., Ketting, D., Bruinvis, L., De Bree, P. K., Kamerling, J. P., et al. (1976). D-Glyceric acidemia in a patient with chronic metabolic acidosis. Clinica Chimica Acta, 71, 477–484.
Waśkiewicz, Z., Klapcinska, B., Sadowska-Krepa, E., Czuba, M., Kempa, K., Kimsa, E., et al. (2012). Acute metabolic responses to a 24-h ultra-marathon race in male amateur runners. European Journal of Applied Physiology, 112, 1679–1688.
Webner, D., DuPrey, K. M., Drezner, J. A., Cronholm, P., & Roberts, W. O. (2012). Sudden cardiac arrest and death in United States marathons. Medicine and Science in Sports and Exercise, 44, 1843–1845.
Wendel, U., Langenbeck, U., & Seakins, J. W. T. (1989). Interrelation between the metabolism of LIsoleucine and L-allo-isoleucine in patients with maple syrup urine disease. Pediatric Research, 25, 11–15.
Wikoff, W. R., Anfora, A., Liu, T. J., Schultz, P. G., Lesley, S. A., Peters, E. C., & Siuzdak, G. (2009). Metabolomics analysis reveals large effects of gut microflora on mammalian blood metabolites. Proceedings of the National Academy of Sciences, 106, 3698–3703.
Żółtaszek, R., Hanausek, M., Kiliańska, Z. M., & Walaszek, Z. (2008). The biological role of D-glucaric acid and its derivatives: Potential use in medicine. Postepy Gigieny i Medycyny Doswiadczalnej, 62, 451–462.
Acknowledgements
The authors would like to thank Dr. Mari van Reenen for assistance with statistical analysis, Mrs. Derylize Beukes-Maasdorp for sample analysis and Prof. Nico L. Smit for initiating the collaboration.
Funding
The authors have no specific funding to report.
Author information
Authors and Affiliations
Contributions
The concept and study were designed by DTL, ZS, GH, TC, KMK and EJS; samples were acquired from the Northumbria University in collaboration with GH, TC, KMK and EMS. ZS was responsible for manuscript drafting, data analysis and interpretation, the latter of which was assisted by DTL, LL and LJM. LL, LJM and DTL were involved in repeated manuscript reviewing, of which LL was greatly involved with structural (format) editing. All of the authors revised and approved the final version of this manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that there are no conflicts of interest, and that this manuscript, and the work described therein, is unpublished and has not been submitted for publication elsewhere.
Ethical approval
Ethical approval for this investigation, conducted according to the Declaration of Helsinki and International Conference on Harmonization Guidelines, was obtained from the Research Ethics Committee of the Faculty of Health and Life Sciences at the Northumbria University in Newcastle upon Tyne, UK (Reference Number: HLSTC120716).
Informed consent
Informed consent was obtained from all individuals included in the study.
Rights and permissions
About this article

Cite this article
Stander, Z., Luies, L., Mienie, L.J. et al. The altered human serum metabolome induced by a marathon. Metabolomics 14, 150 (2018). https://doi.org/10.1007/s11306-018-1447-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11306-018-1447-4