
Abstract
Background
Menopause is associated with increased abdominal fat and increased risk of developing diabetes and cardiovascular disease.
Objectives
The present study evaluated the plasma metabolic response in relation to insulin sensitivity after weight loss via diet intervention.
Methods
This work includes two studies; i) Ten women on a 5 weeks Paleolithic-type diet (PD, 30 energy percent (E%) protein, 40 E% fat, 30 E% carbohydrates), ii) 55 women on 6 months of either PD or Nordic Nutrition Recommendations diet (NNR, 15 E% protein, 30 E% fat, and 55 E% carbohydrates). Plasma metabolic profiles were acquired at baseline and post diet using gas chromatography time-of-flight/mass spectrometry and investigated in relation to insulin sensitivity using multivariate bioinformatics.
Results
Both the PD and NNR diet resulted in significant weight loss, reduced waist circumference, improved serum lipid profiles, and improved insulin sensitivity. We detected a baseline metabolic profile that correlated significantly with insulin sensitivity, and of which components increased significantly in the PD group compared to NNR. Specifically, a significant increase in myo-inositol (MI), a second messenger of insulin action, and β-hydroxybutyric acid (β-HB) increased while dihomo-gamma-linoleic acid (DGLA) decreased in PD compared to NNR, which correlated with improved insulin sensitivity. We also detected a significant decrease in tyrosine and tryptophan, potential markers of insulin resistance when elevated in the circulation, with the PD but not the NNR.
Conclusions
Using metabolomics, we detected changes in the plasma metabolite profiles associated with weight loss in postmenopausal women by different diets. The metabolic profiles following 6 months of PD were linked to beneficial effects on insulin sensitivity compared to NNR.
Graphical Abstract

Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
After menopause, the incidence of cardiovascular disease (CVD) increases (Lisabeth et al. 2009). An important mediator of this increase is the redistribution of fat from peripheral to central depots due, at least in part, to a decline in estrogen. Obesity and central fat accumulation (i.e., accumulation of visceral adipose tissue) are strongly linked to an increased risk of type 2 diabetes mellitus (T2DM) and CVD (Rexrode et al. 1998, Peppa et al. 2013). Therefore, effective approaches for reducing weight and tools for identifying potential mediators of beneficial metabolic effects, notably insulin sensitivity, are important in subjects with central obesity.
A Paleolithic-type diet (PD) includes increased proportions of unsaturated fatty acids and a relatively high protein content, with demonstrated beneficial effects on metabolic imbalance, including insulin sensitivity, even when administered ad libitum compared to other types of diets, including the Nordic Nutrition Recommendations (NNR) (Jonsson et al. 2009, 2010; Lindeberg et al. 2007). We have reported that an ad libitum PD can have profound effects on weight loss and metabolic functions in obese postmenopausal women, including decreased ectopic lipid deposition and improved lipid balance and glucose tolerance. The PD was also superior to a diet based on the NNR in terms of weight loss and improvements in body composition (Ryberg et al. 2013, Mellberg et al. Mellberg et al. 2014).
Metabolomics (Fiehn et al. 2000; Kell 2004) studies have shown great promise for discovering pathways linked to disease progression (Wang et al. 2011; Newgard et al. 2009) and for dissecting putative links between food intake and metabolic functions (LeMieux et al. 2013; Brennan, 2013). Simultaneous measurement of multiple analytes (metabolites) has confirmed suggested links between key intermediates in lipid, carbohydrate, and protein metabolism and perturbations in T2DM, CVD, and cancer (Suhre 2014). The aim of the present study was to investigate the plasma metabolic profile in cohorts with diet-induced weight loss in order to find putative predictors and mediators of the outcome after these interventions, notably in relation to insulin sensitivity.
2 Experimental section
2.1 Participants and clinical protocol
The present study comprises two different dietary intervention studies: a 5-week PD pilot study (Ryberg et al. 2013) and a 6-month intervention that employed both a PD and NNR diet (Mellberg et al. Mellberg et al. 2014). The inclusion and exclusion criteria were comparable for the two studies and are presented in detailed elsewhere (Mellberg et al. 2014, Ryberg et al. 2013). Briefly, all study participants were healthy postmenopausal women younger than 70 years of age, non-smokers, and with a body mass index (BMI) between 28 and 40 kg/m2. The studies were approved by the Regional Ethical Review Board at Umeå University, and written informed consent was obtained from all participants.
2.2 Five-week PD pilot study
The study participants were provided a PD ad libitum. The diet consisted of lean meat, poultry, fish, seafood, eggs, vegetables, fruit, berries, nuts, and seeds. All meals were prepared by the food service establishment at Umeå University Hospital. Participants were advised to complement the provided frozen meals with additional food items in concordance with the PD. The provided dietary recommendations aimed for an approximate intake of 30 energy percent (E%) protein, 30 E% carbohydrates, and 40 E% fat, with a high proportion of monounsaturated fatty acids (MUFA) and a low proportion of saturated fatty acids (SFA). The study participants had weekly individual meetings with the study dietician, and food intake was assessed at baseline and after 5 weeks on the PD. A detailed description of the study design, including a detailed dietary intake assessment, was presented previously (Ryberg et al. 2013).
2.3 Six-month intervention using a PD and NNR diet
Seventy postmenopausal women were randomized into two groups (Mellberg et al. 2014). One group was instructed to eat a PD ad libitum and the other group to eat an omnivorous diet in concordance with the NNR for 24 months (Becker, 2005). Food intake for the NNR group was ad libitum and recommendations were given for an approximate intake of 15 E% protein, 55 E% carbohydrates, and 30 E% fat (10 E% each of polyunsaturated fatty acids (PUFA), MUFA, and SFA). All participants met in groups for 12 sessions that consisted of cooking lessons, instructions regarding food records, and discussions concerning dietary changes. Plasma samples were collected at baseline and after 6 months of intervention. The largest weight reduction occurred during the first 6 months, suggesting the strongest adherence to the dietary regimens during this time period. A complete description of the study design, including a detailed dietary intake assessment for the entire intervention, was described previously by Mellberg et al. (2014). Briefly, The PD diet included a recommendation for a high intake of MUFAs and PUFAs and relative low intake of carbohydrates. The diet was based on lean meat, fish, eggs, vegetables, fruits, berries and nuts. Additional fat sources were avocado and oils (rapeseed and olive oil) used in food preparation and dressing. Dairy products, cereals, added salt and refined fats and sugar were excluded.
2.4 General measurements for both interventions
Physical examinations were performed at baseline and after 5 weeks in the PD pilot study, and at baseline and after 6 months in the 6-month intervention study. Body composition, including an estimation of total body fat percentage, was measured by dual energy x-ray absorptiometry (DXA) (GE Medical Systems, Lunar Prodigy X-ray Tube Housing Assembly, Brand BX-1L, Model 8743, Madison, WI, USA). Overnight fasting blood samples were drawn from the antecubital vein after a resting period. Aliquots were frozen immediately at −20 °C until being analyzed for fasting plasma glucose (Vitros GLU Slides, Ortho-Clinical Diagnostics J&J) and fasting plasma insulin (Elecsys Insulin kit, Roche Diagnostic Scandinavia AB, Sweden). Insulin sensitivity was calculated using the homeostasis model assessment (HOMA) index with the formula (G0 × I0)/22.5, where G0 is fasting plasma glucose and I0 is fasting plasma insulin. High-sensitivity C-reactive protein (hsCRP) was analyzed by immunoassay (IMMULITE, Diagnostic Products Corporation, USA). A detailed description of the anthropometric measurements, including blood pressure, is found elsewhere (Mellberg et al. 2014, Ryberg et al. 2013). Aliquots for the metabolomics analysis were stored at −80 °C prior to analysis.
2.5 Sample preparation and metabolomics analysis
A run order design was constructed to minimize bias from sample preparation and analysis. Samples from the same participant were prepared and analyzed in close connection to each other, whereas the internal order was randomized. In addition, the sample preparation batches and analytical run order were balanced in relation to the type of diet. Thus, bias interfering with the biological variation of interest was minimized when comparing samples between diet groups or between individuals. From the 5-week PD pilot study, a total of 29 samples were analyzed in duplicate using gas chromatography time-of-flight/mass spectrometry (GC-TOF/MS). Samples from the 6-month intervention study were analyzed in two separate batches in immediate succession. Prior to GC-TOF/MS analysis, MeOH–H2O extraction followed by a two-step derivatization procedure was performed for serum metabolites as described previously (Trygg et al. 2005). The derived samples were injected in splitless mode by a CTC Combi Pal autosampler (CTC Analytics AG, Zwingen, Switzerland) into an Agilent 6890 gas chromatograph equipped with a 10 m × 0.18 mm i.d. fused silica capillary column with a chemically bonded 0.18-μm DB 5-MS stationary phase (J&W Scientific, Folsom, CA). The column effluent was introduced into the ion source of a Pegasus III GC-TOF/MS (Leco Corp., St Joseph, MI).
2.6 Data treatment
Hierarchical multivariate curve resolution (HMCR) (Jonsson et al. 2005) was used to resolve overlapping metabolites/compounds that were not separated by chromatography. For the 5-week PD pilot study, all samples were processed simultaneously, except for the analytical replicates, which were predicted in the existing HMCR model (Jonsson et al. 2006). To remove instrumental biases and concentration variation, the resolved data were normalized using the means of 12 added internal standards that eluted throughout the entire chromatographic range, consisted of: [13C5]-proline, [2H4]-succinic acid, [13C5, 15N]-glutamic acid, [1,2,3-13C3]-myristic acid, [2H7]-cholesterol and [13C4]-disodium - ketoglutarate were purchased from Cambridge Isotope Laboratories (Andover, MA); [13C12]-sucrose, [13C4]- palmitic acid and [2H4]- butanediamine 2HCl were obtained from Campro (Veenendaal, The Netherlands); [13C6]-glucose was purchased from Sigma Aldrich (Steinheim, Germany); [2H6]-salicylic acid was purchased from Icon (Summit, NJ); and NMethyl-N-trimethylsilyltrifluoroacetamide (MSTFA), 1 % trimethylchlorosilane (TMCS) and pyridine (silylation grade) were purchased from Pierce Chemical Co. Stock solutions of the reference compounds and IS were prepared either in Milli-Q water or methanol at the same concentration, 0.5 µg µL−1. The area under the chromatographic peak was calculated for each internal standard using non-noisy and unique mass-channels. A principal component (PC) was then calculated based on the chromatographic peak areas for the internal standards (all variables were scaled to unit variance, non-centered). Finally, the calculated PC score value, which is comparable to the sample mean in this case, was used to normalize the resolved data by dividing each sample by the corresponding score value (Redestig et al. 2009).
2.7 Metabolite identification
All resolved mass spectra profiles were subjected to a spectral database search in NIST MS-Search v. 2.0.38. Match values ranking the spectra were calculated using the dot product of the two spectra (i.e., the resolved spectrum and the database spectrum); higher m/z peaks had more weight than lower m/z peaks because higher m/z values are considered more compound-specific. The match values ranged from 0 to 999, with 999 indicating an identical match. We performed positive identification by combining match values with the retention time index, which was calculated from the analytically characterized alkane series (C10–C40). Only metabolites with match value >700 and retention index difference from the library match <20 units were considered. However a manual inspection were performed on all components prior to assignment to compound class and or identification. Furthermore, all metabolites were classified as amino acids and derivatives, amines, organic acids, carbohydrates, lipids, no class, or unidentified. Assignment to different compound classes was based on criteria set by the Human Metabolome Database (www.HMDB.ca) (Wishart et al. 2007).
2.8 Statistical analysis
The data sets were inspected using principal components analysis (PCA) in order to detect groupings, outliers, and trends, as well as select representative samples for training sets. Additional sample comparison modeling was performed using multivariate regression analysis with orthogonal partial least squares (OPLS). Prior to multivariate analysis, each individual’s baseline sample was subtracted from its post-intervention sample to elucidate the intervention effect on the metabolic profile and minimize the influence from instrumental drift and inter-individual variation. To validate the obtained OPLS models, P values were calculated for the differences between the pre-defined classes. These P values were calculated using analysis of variance (ANOVA) based on the cross-validated OPLS scores (CV-ANOVA). Special consideration was taken to ensure proper cross-validation groups (i.e., to retain the same participant/replicate in the same group, reducing the risk of creating an over-fitted model). The importance of each variable to the multivariate model projection (variable of importance plot, VIP–value) reflects the importance of each metabolite to explaining the response (dietary difference/intervention course). A metabolite was considered to contribute significantly to the metabolite profile if it had a VIP value > 1 and/or a significant P value. All univariate P values were calculated from the Wilcoxon signed-rank test using a 95 % significance level. P values were obtained using univariate t tests, as well as CV-ANOVA and jack knifing-based confidence intervals (Efron et al. 1983) from OPLS models.
3 Results
3.1 Five-week PD pilot study
Ten overweight/obese postmenopausal women (age 52.6 ± 3.8 years, BMI 31.4 ± 2.6 kg/m2, total body fat 39.1 ± 4.5 kg) participated in the 5-week intervention study with a PD. The effects of this intervention on anthropometric data and metabolic function were published elsewhere (Ryberg et al. 2013). Briefly, mean energy intake decreased by 25 % and was associated with a mean weight loss of 4.5 kg. BMI, waist and hip circumference, abdominal sagittal diameter, diastolic blood pressure, fasting serum glucose, and LDL/HDL cholesterol decreased, whereas hepatic insulin sensitivity increased (decreased HOMA values) (Ryberg et al. 2013).
A total of 20 plasma samples were collected and metabolically characterized in duplicate using GC-TOF/MS. One participant (Participant 3) was excluded along with her analytical replicates because of low analytical quality, incomplete chromatographic spectra due to sample contamination. The GC-TOF/MS data collected for the 18 included samples were processed by HMCR, and the analytical replicates were predictively resolved to allow the robustness of the processing to be controlled. A total of 182 putative metabolites were detected in plasma; 79 were successfully identified and/or classified using mass spectral library comparisons (Table 1). The remaining compounds not identified with enough certainty retained information regarding the fragmentation pattern and retention time index, which could be used in further identification attempts. Pearson’s correlation between analytical replicates revealed a >90 % correlation for the resolved metabolites and the internal standards.
3.2 Plasma metabolic profile
We observed a significant difference (P < 0.001) between metabolite profiles in plasma samples collected before and after the intervention. The existing OPLS model had 93 % model sensitivity (% correct prediction) and 100 % model specificity (% correct model classification). The OPLS model revealed a cohesive metabolic response for all participants when comparing their basal samples to those collected after 5 weeks (data not shown). Detailed information regarding identification/classification, related statistics, and responses to the intervention is provided in Table 1.
We observed an increase in circulating MUFA and PUFA [e.g., oleic acid (18:1), docosahexadecanoic acid (DHA, 22:6 n-3), palmitoleic acid (16:1), and arachidonic acid (20:4 n-6)], and a decrease in SFA, larger lipids, and sterols [e.g., cholesterol, alpha-tocopherol, glycerophosphocholine (GPC), lauric acid (12:0), and gamma-tocopherol]. However, we noted an increase in palmitic acid (16:0). Two of the most commonly occurring polyols in humans were significantly altered, i.e., myo-inositol (MI) increased and 1,5-anhydroglucitol (1,5-AG) decreased. The circulating concentrations of amino acids decreased in general, especially tryptophan, proline, tyrosine, threonine, and asparagine. In contrast, we detected an increase in diet-related amino acid derivatives, such as methylcysteine and pipecolic acid. The concentrations of branched chain amino acids isoleucine and valine remained unaltered.
3.3 Six-month intervention using a PD and NNR
Participants in both diet groups experienced a significant (P < 0.05) decrease in BMI, waist and hip circumference, and percent body fat after 6 months. The PD group had significantly reduced waist circumference, fasting serum (fs)-insulin, and HOMA index values compared to the NNR group after 6 months of diet (Table 2). Adherence to diets was evaluated, using repeated food records and estimations of nitrogen excretion in the urine, as reported in detail in Mellberg et al. 2014. Briefly, target levels of macronutrient intake were not completely achieved. Protein intake in the PD group was lower than proposed, mirrored by a lack of difference in nitrogen excretion between groups. Furthermore, the NNR group did not reach the target amount of carbohydrate intake.
Only participants with plasma samples available at baseline and after 6 months were included in order to elucidate the metabolic effects and their relationship to changes in insulin sensitivity and body composition. A total of 110 plasma samples (55 subjects sampled before and after dietary intervention) were characterized using GC-TOF/MS. The characteristics of the subjects included in the metabolomic analysis are provided in Table 2. A total of 117 putative metabolites were resolved from the GC-TOF/MS data; 62 of them were identified and/or assigned to a compound class (Table 3).
No significant differences, clusters, or outliers related to the different diets were detected in the metabolite profiles or clinical parameters at baseline based on either PCA or P values (data not shown). Thus, all models investigating intervention effects, not including baseline investigations, were based on delta values, i.e., by subtracting baseline metabolic profiles from the post-intervention metabolic profiles to obtain delta values.
3.4 Baseline metabolic profiles
We identified a plasma metabolic profile at baseline that correlated significantly (P = 0.0045) with insulin resistance (i.e., HOMA index) (Fig. 1). Specifically, ribitol, MI, beta-hydroxybutyric acid (β-HB), glycine, and phosphoric acid correlated negatively with the HOMA index, whereas galactono-1,4-lactone, glucose, dihomo-gamma-linoleic acid (DGLA, 20:3,n-6), palmitoleic acid (16:1), and amino acids valine, cysteine, and isoleucine positively correlated with the HOMA index (i.e., with decreased insulin sensitivity). We did not detect a metabolic profile that significantly correlated with the HOMA index at the remaining time-points.

OPLS loading describes the plasma metabolic profile in relation to the HOMA index in baseline samples from 55 obese/overweight postmenopausal women. Metabolites with positive axis values (w[1]) are associated with low insulin sensitivity (high HOMA values), whereas negative axis values (w[1]) correlate negatively with the HOMA index, i.e., high insulin sensitivity. The multivariate 95 % confidence interval is based on jack-knifing, and the bars are colored according to univariate P values. Dark grey bars differ significantly between diet groups after 6 months of intervention, and light grey bars do not differ significantly between groups after 6 months. Significance is based on a combination of multivariate and univariate significance testing. Table 3 provides a complete description of all metabolites included in the models, classification/identification, abbreviations, and related statistics
3.5 Intervention-related metabolic profiles
Notably, components from the insulin resistance baseline metabolic profile were significantly altered between the diet groups after 6 months. The PD group showed improvements in insulin sensitivity as compared to the NNR group via decreased DGLA (positive correlation with the HOMA index) and an increase in MI and β-HB (negative correlation with the HOMA index).
Comparing the two metabolic profiles, we found a significant difference (P > 0.001) in metabolite profiles between the PD and NNR diet. After 6 months, the PD group exhibited lower relative concentrations of 1,5-AG, DGLA (20:3, n-6), and lauric acid (12:0) and higher concentrations of MI, DHA (22:6, n-3), ascorbic acid, and β-HB than the NNR group (Fig. 2). The observed alterations in MI and 1,5-AG were also seen in the 5-week pilot PD study. Relevant to the aim, we also detected differences in amino acids; the concentrations of glycine, tryptophan, and tyrosine decreased, and the concentration of serine increased in the PD group versus the NNR group.

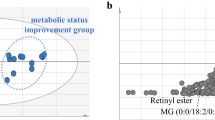
Two separate OPLS models displaying the effects of dietary intervention on plasma metabolite profiles in overweight/obese postmenopausal women after 6 months. a Cross-validated OPLS scores (tcv[1]) describing the metabolic effects recorded for 31 individual participants after a 6-month intervention with a Paleolithic-type diet (PD). One high* and one low** responder to PD are each highlighted in the plot. b OPLS model weights (w[1]) describe the metabolic profile related to the PD. Only identified metabolites with VIP > 1 are presented, and the bars are colored according to univariate P values (dark bars have a significant P value and light bars a non-significant P value). Metabolites with positive axis values increased after 6 months of PD, whereas metabolites with negative axis values decreased. c Cross-validated OPLS scores (tcv[1]) describe the metabolic effects recorded for 24 participants after a 6-month intervention with a diet based on the Nordic Nutrition Recommendations (NNR). d OPLS model weights (w[1]) describe the metabolic profile related to the NNR intervention. Only identified metabolites with VIP > 1 are presented, and the bars are colored according to univariate P values (dark bars have a significant P value and light bars a non-significant P value). Metabolites with positive axis values increased after 6 months of the NNR, whereas those with negative axis values decreased. Table 3 provides a complete description of all metabolites included in the models, classification/identification, and their abbreviation (Color figure online)
When investigating alterations in the diet-specific metabolic profiles, only the PD resulted in a significant change (OPLS CV-ANOVA, P > 0.001) not the NNR diet (OPLS CV-ANOVA, P = 0.09). Diet specific metabolite profiles are plotted in Fig. 3. In terms of unique metabolites, both diets resulted in a significant increase in pantothenic acid (vitamin B5) and a decrease in 1,5-AG, phosphoric acid, MI-1 phosphate, DGLA, and AA (Fig. 3b, d).

An OPLS model comparing the respective effects of dietary intervention with a Paleolithic-type diet (PD) and a diet based on the Nordic Nutrition Recommendations (NNR) on the plasma metabolic profile. a Cross-validated OPLS scores (tcv[1]) describe the 55 participants’ (31 PD, grey bars; 24 NNR, black bars) metabolic responses to 6 months of dietary intervention. One high responder* and one low responder** to the PD are each highlighted in the plot. b OPLS model weights (w[1]) of the discriminating metabolic profile between 6 months of the PD or NNR. The multivariate 95 % confidence interval is based on jack-knifing, and the bars are colored according to univariate P values (dark bars have a significant P value and light bars a non-significant P value). Metabolites with positive axis values decreased in the PD group relative to the NNR group, and those with negative axis values increased in the PD group relative to the NNR group. Table 3 provides complete descriptions of all metabolites included in the models, classification/identification, abbreviations, and related statistics (Color figure online)
In the PD group, but not the NNR group, we observed increases in DHA, MI, β-HB, and oxalic acid. Concomitant decreases in SFA and n6-PUFAs [i.e., lauric acid (LauA, 12:0), palmitic acid (PA, 16:0), stearic acid (SA, 18:0), linoleic acid (18:2, n-6), and glycerophosphocholine (GPC)] were also measured. After 6 months of the PD, we also detected decreases in tyrosine and tryptophan that were not observed in the NNR group (Fig. 3b, d).
3.6 Individual response to the PD
The PD group revealed a robust intervention-related metabolic profile, but with large inter-individual variation after 6 months (Fig. 2a). Based on this finding, we highlighted a high responder (Participant 16) and low responder (Participant 41), which was verified in terms of BMI, percent body fat, and HOMA index compared to the PD group mean. Specifically, the high responder reduced her BMI by 6.5 kg/m2, body fat by 7.9 %, and HOMA index by 3.3 compared to the PD group means of 3 kg/m2, 4.2 %, and 0.4 units, respectively. In contrast, the low responder reduced her BMI by 1.3 kg/m2, percent body fat by 1.4 %, and her HOMA index increased by 5.5 units.
4 Discussion
We detected an intervention-related plasma metabolic profile that differed between the PD and NNR groups. The findings in the PD group were congruent in the 5 weeks and 6 months dietary intervention studies, suggesting that they are robust. Furthermore, we observed a metabolic profile at baseline that correlated significantly with decreased insulin sensitivity (HOMA index) for both diet groups. After 6 months, the components in this metabolic profile differed significantly between the diets and were associated with increased insulin sensitivity in the PD group compared to the NNR group. Specifically, women following the PD had a significant increase in MI and β-HB and reduced DGLA compared to the NNR group. This pattern correlated with improved insulin sensitivity and coincided with significant reductions in waist circumference.
Inositols, with MI as the most abundant stereoisomer, act as second messengers of insulin action and have been identified to play a vital role in activating key enzymes that control the oxidative and non-oxidative metabolism of glucose (Saltiel and Kahn, 2001). Plasma MI comes from different sources, including dietary intake (Clements and Darnell, 1980) and de novo synthesis from glucose-6-phosphate via myo-inositol-1-phosphate. Therefore, predicting where the observed increase in MI originates and whether it reflects intracellular concentrations is difficult. Interestingly, supplementation with MI (Genazzani et al. 2008) and chiro-inositol (CI) (Nestler et al. 1999) has been shown to reduce insulin, glucose, triglycerides, and diastolic blood pressure in young women with polycystic ovarian syndrome, a patient population at risk for developing T2DM (Dunaif, 1997). In addition, improved insulin sensitivity via MI supplementation has been confirmed in patients with gestational diabetes (Corrado et al. 2011). Notably, the menopausal state may influence the effects of MI because estrogen promotes nitric oxide, which in turn inhibits the polyol pathway (Ren and Ceylan-Isik, 2004), and a low-energy diet combined with MI supplementation has been shown to improve insulin sensitivity and blood lipids and reduce diastolic blood pressure in postmenopausal women with metabolic dysregulation (Giordano et al. 2011).
We measured significant decreases in tyrosine and tryptophan in the PD groups. Both tyrosine and tryptophan are included in the metabolic signature that is reported to be a strong predictor of insulin resistance (Newgard et al. 2009). The underlying mechanism may be the disruption of insulin signaling in skeletal muscle (Newgard et al. 2009, Wang et al. 2011a, b). Therefore, a decrease in these circulating amino acids may be beneficial for preventing T2DM. We did not find a significant correlation between tyrosine and tryptophan and the HOMA index at baseline, possibly due to the relatively well-preserved insulin sensitivity in this study group.
As no major difference was found in protein intake between the groups, based on urine nitrogen measurements, fat composition is the key difference between the PD and NNR. The PD contains greater percentages of MUFA and PUFA than the NNR. We detected significant decreases in SFA and n6-PUFA and significant increases in MUFA and n-3 PUFA after 6 months of the PD compared to the NNR. Importantly, the n-6 PUFA DGLA, which was closely linked to insulin resistance at baseline, decreased significantly more in the PD group. DGLA has anti-proliferative and inflammatory properties through its conversion to prostaglandin (PG)H1, which is further converted to PGE1. Via this conversion, DGLA has been reported to have anti-inflammatory effects in diabetic humans (Kapoor and Huang, 2006). Because DGLA correlates with insulin resistance (i.e., via the HOMA index), diets, such as the PD, that reduce DGLA and increase MI and β-HB are expected to have beneficial effects on insulin sensitivity. As each lipid subtype has its own unique biochemical properties, including different n-6 and n-3 PUFAs (Russo, 2009, Virtanen et al. 2014), further research should focus on specific lipids and whether they are key mediators of improved insulin sensitivity and protect against CVD.
In addition to the mentioned alterations in MI, we observed an intervention-related effect of another common polyol, 1,5-AG. The intervention effects of PD on 1,5-AG (and MI) observed during the 5-week PD pilot study were verified in the long-term study; 1,5-AG decreased in both diet groups but significantly more in the PD group. 1,5-AG is generated from glycogen via 1,5-anhydrofrucotose by an NADPH-dependent reductase (Sakuma et al. 1998) and can act as a powerful insulin secretagogue in pancreatic β-cells (Yamanouchi et al. 2003). 1,5-AG has also been suggested as a marker for postprandial glycemic variability in hyperglycemic individuals (Yamanouchi et al. 1996). Therefore, the detected decrease in circulating 1,5-AG may be a consequence of a negative energy balance (which was more profound in the carbohydrate-restricted PD group), as these individuals may deplete their glycogen storage to a greater extent. Additional investigations regarding the use of 1,5-AG as a marker of postprandial glycemic variability during negative energy balance, particularly during carbohydrate restriction, are of interest.
Traditionally, nutritional recommendations to improve health have focused mainly on the whole population. However, there is major variability in individual adaptive and functional mechanisms of metabolic homeostasis. As highlighted by our results, metabolomics, if combined with suitable bioinformatics, has the potential to objectively capture the complexity of human nutritional status on both the individual and population level. This approach is a step towards assessing personalized dietary recommendations to improve health (McNiven et al. 2011, Zeisel et al. 2005). Studies of intervention effects could include normalizing the metabolic profile for each individual to baseline levels in order to more sensitively elucidate the true intervention-related metabolic effects apart from individual variability, such as improved insulin sensitivity, in a population prior to disease onset, e.g., T2DM.
Weight loss occurred in both diet groups, despite the ad libitum conditions. Contributing factors to this may include inadequate reports of energy intake, increased physical activity energy expenditure when the volunteers were not using the accelerometers, the increased thermogenic effects of protein and other uncertainties regarding the measurement of all energy components. A major strength of this study is the validation of our findings in two independent studies. However, the study also has some limitations. First, since T2DM was an exclusion criterion, all of the included women were insulin-sensitive, which decreases the possibility of identifying effects related to improved metabolic regulation. Second, we did not include the lipidome in the analysis, which may be of future interest in relation to improvements in insulin sensitivity via lifestyle interventions.
In conclusion, we found distinct differences in the metabolite profiles of our diet study groups, which were associated with a more pronounced improvement in body composition and insulin sensitivity in the PD group. These results highlight metabolites of interest for monitoring mechanisms related to improved insulin sensitivity after weight loss in postmenopausal women. Additional studies are warranted regarding the effects of lifestyle interventions on intermediary metabolism in participants with more pronounced metabolic dysfunction, including T2DM.
References
Becker, W. (2005). New Nordic nutrition recommendations 2004. Physical activity as important as good nourishing food. Lakartidningen, 102, 2757-8–2760-2.
Brennan, L. (2013). Metabolomics in nutrition research: Current status and perspectives. Biochemical Society Transactions, 41, 670–673.
Clements, R. S., & Darnell, B. (1980). Myoinositol content of common foods—development of a high-myo-inositol diet. American Journal of Clinical Nutrition, 33, 1954–1967.
Corrado, F., D’Anna, R., Di Vieste, G., Giordano, D., Pintaudi, B., Santamaria, A., & Di Benedetto, A. (2011). The effect of myoinositol supplementation on insulin resistance in patients with gestational diabetes. Diabetic Medicine, 28(8), 972–975.
Dunaif, A. (1997). Insulin resistance and the polycystic ovary syndrome: Mechanism and implications for pathogenesis. Endocrine Reviews, 18, 774–800.
EFRON, B. A. G., G. 1983. A Leisurely Look at the Bootstrap, the Jack-knife, and Cross-validation. The American Statistician. http://www.jstor.org/stable/2685844: American Statistical Association.
Fiehn, O., Kopka, J., Dormann, P., Altmann, T., Trethewey, R. N., & Willmitzer, L. (2000). Metabolite profiling for plant functional genomics. Nature Biotechnology, 18, 1157–1161.
Genazzani, A. D., Lanzoni, C., Ricchieri, F., & Jasonni, V. M. (2008). Myo-inositol administration positively affects hyperinsulinemia and hormonal parameters in overweight patients with polycystic ovary syndrome. Gynecological Endocrinology, 24, 139–144.
Giordano, D., Corrado, F., Santamaria, A., Quattrone, S., Pintaudi, B., di Benedetto, A., & D’Anna, R. (2011). Effects of myo-inositol supplementation in postmenopausal women with metabolic syndrome: A perspective, randomized, placebo-controlled study. Menopause-the Journal of the North American Menopause Society, 18, 102–104.
Jönsson, T., Granfeldt, Y., Ahrén, B., Branell, U. C., Pålsson, G., Hansson, A., et al. (2009). Beneficial effects of a Paleolithic diet on cardiovascular risk factors in type 2 diabetes: A randomized cross-over pilot study. Cardiovasc Diabetol, 8(35), 1–14.
Jönsson, T., Granfeldt, Y., Erlanson-Albertsson, C., Ahrén, B., & Lindeberg, S. (2010). A paleolithic diet is more satiating per calorie than a mediterranean-like diet in individuals with ischemic heart disease. Nutrition & metabolism, 7(1), 1.
Jonsson, P., Johansson, A. I., Gullberg, J., Trygg, J., Grung, B., Marklund, S., et al. (2005). High-throughput data analysis for detecting and identifying differences between samples in GC/MS-based metabolomic analyses. Analytical Chemistry, 77(17), 5635–5642.
Jonsson, P., Johansson, E. S., Wuolikainen, A., Lindberg, J., Schuppe-Koistinen, I., Kusano, M., et al. (2006). Predictive metabolite profiling applying hierarchical multivariate curve resolution to GC-MS datas - A potential tool for multi-parametric diagnosis. Journal of Proteome Research, 5, 1407–1414.
Kapoor, R., & Huang, Y.-S. (2006). Gamma linolenic acid: An antiinflammatory omega-6 fatty acid. Current Pharmaceutical Biotechnology, 7, 531–534.
Kell, D. B. (2004). Metabolomics and systems biology: Making sense of the soup. Current Opinion in Microbiology, 7, 296–307.
Lemieux, M., Al-Jawadi, A., Wang, S., & Moustaid-Moussa, N. (2013). Metabolic Profiling in Nutrition and Metabolic Disorders. Advances in Nutrition, 4, 548–550.
Lindeberg, S., Jonsson, T., Granfeldt, Y., Borgstrand, E., Soffman, J., Sjostrom, K., & Ahren, B. (2007). A Palaeolithic diet improves glucose tolerance more than a Mediterranean-like diet in individuals with ischaemic heart disease. Diabetologia, 50, 1795–1807.
Lisabeth, L. D., Beiser, A. S., Brown, D. L., Murabito, J. M., Kelly-Hayes, M., & Wolf, P. A. (2009). Age at natural menopause and risk of ischemic stroke The Framingham Heart Study. Stroke, 40, 1044–1049.
McNiven, E. M. S., German, J. B., & Slupsky, C. M. (2011). Analytical metabolomics: Nutritional opportunities for personalized health. Journal of Nutritional Biochemistry, 22, 995–1002.
Mellberg, C., Sandberg, S., Ryberg, M., Eriksson, M., Brage, S., Larsson, C., et al. (2014). Long-term effects of a Palaeolithic-type diet in obese postmenopausal women: A 2-year randomized trial. European Journal of Clinical Nutrition, 68, 350–357.
Nestler, J. E., Jakubowicz, D. J., Reamer, P., Gunn, R. D., & Allan, G. (1999). Ovulatory and metabolic effects of D-chiro-inositol in the polycystic ovary syndrome. New England Journal of Medicine, 340, 1314–1320.
Newgard, C. B., An, J., Bain, J. R., Muehlbauer, M. J., Stevens, R. D., Lien, L. F., et al. (2009). A branched-chain amino acid-related metabolic signature that differentiates obese and lean humans and contributes to insulin resistance. Cell Metabolism, 9(4), 311–326.
Peppa, M., Koliaki, C., Papaefstathiou, A., Garoflos, E., Katsilambros, N., Raptis, S. A., et al. (2013). Body composition determinants of metabolic phenotypes of obesity in nonobese and obese postmenopausal women. Obesity, 21, 1807–1814.
Redestig, H., Fukushima, A., Stenlund, H., Moritz, T., Arita, M., Saito, K., & Kusano, M. (2009). Compensation for systematic cross-contribution improves normalization of mass spectrometry based metabolomics data. Analytical Chemistry, 81, 7974–7980.
Ren, J., & Ceylan-Isik, A. F. (2004). Diabetic cardiomyopathy—Do women differ from men? Endocrine, 25, 73–83.
Rexrode, K. M., Carey, V. J., Hennekens, C. H., Walters, E. E., Colditz, G. A., Stampfer, M. J., et al. (1998). Abdominal adiposity and coronary heart disease in women. Jama-Journal of the American Medical Association, 280, 1843–1848.
Russo, G. L. (2009). Dietary n-6 and n-3 polyunsaturated fatty acids: From biochemistry to clinical implications in cardiovascular prevention. Biochemical Pharmacology, 77, 937–946.
Ryberg, M., Sandberg, S., Mellberg, C., Stegle, O., Lindahl, B., Larsson, C., et al. (2013). A Palaeolithic-type diet causes strong tissue-specific effects on ectopic fat deposition in obese postmenopausal women. Journal of Internal Medicine, 274, 67–76.
Sakuma, M., Kametani, S., & Akanuma, H. (1998). Purification and some properties of a hepatic NADPH-dependent reductase that specifically acts on 1,5-anhydro-D-fructose. Journal of Biochemistry, 123, 189–193.
Saltiel, A. R., & Kahn, C. R. (2001). Insulin signalling and the regulation of glucose and lipid metabolism. Nature, 414, 799–806.
Suhre, K. (2014). Metabolic profiling in diabetes. Journal of Endocrinology, 221, R75–R85.
Trygg, J., Gullberg, J., Johansson, A. I., Jonsson, P., Antti, H., Marklund, S. L., & Moritz, T. (2005). Extraction and GC/MS analysis of the human blood plasma metabolome. Analytical Chemistry, 77, 8086–8094.
Virtanen, J. K., Mursu, J., Voutilainen, S., Uusitupa, M., & Tuomainen, T.-P. (2014). Serum omega-3 polyunsaturated fatty acids and risk of incident type 2 diabetes in men: The Kuopio Ischemic Heart Disease Risk Factor study. Diabetes Care, 37, 189–196.
Wang, T. J., Larson, M. G., Vasan, R. S., Cheng, S., Rhee, E. P., McCabe, E., et al. (2011). Metabolite profiles and the risk of developing diabetes. Nature Medicine, 17, 448–453.
Wishart, D. S., Tzur, D., Knox, C., Eisner, R., Guo, A. C., Young, N., et al. (2007). HMDB: The human metabolome database. Nucleic Acids Research, 35, D521–D526.
Yamanouchi, T., Inoue, T., Ichiyanagi, K., Sakai, T., & Ogata, N. (2003). 1,5-Anhydroglucitol stimulates insulin release in insulinoma cell lines. Biochimica Et Biophysica Acta-General Subjects, 1623, 82–87.
Yamanouchi, T., Ogata, N., Tagaya, T., Kawasaki, T., Sekino, N., Funato, H., et al. (1996). Clinical usefulness of serum 1,5-anhydroglucitol in monitoring glycaemic control. Lancet, 347, 1514–1518.
Zeisel, S. H., Freake, H. C., Bauman, D. E., Bier, D. M., Burrin, D. G., German, J. B., et al. (2005). The nutritional phenotype in the age of metabolomics. Journal of Nutrition, 135, 1613–1616.
Acknowledgments
We are grateful to all of the women who participated in this study. Krister Lundgren and Inga-Britt Carlsson assisted during the GC-TOF/MS analysis, and Inger Arnesjö made important contributions during the dietary intervention studies. This work was supported by grants from the Swedish Research Council (VR), the Swedish Council for Working Life and Social Research, the Swedish Strategic Research Foundation (SSF), Wallenberg Consortium North (WCN), the Kempe Foundation, the Swedish Heart and Lung Foundation, the Medical Faculty at Umeå University, and the Västerbotten County Council.
Financial support
This study was supported by grants from The Swedish Council for Working Life and Social Research (2006-0699 and 2010-0398), the Swedish Research Council (K2011-12237-15-6), the Swedish Heart and Lung Foundation, the Swedish Diabetes Foundation, King Gustaf V and Drottning Victorias Foundation, the County Council of Västerbotten, and Umeå University, Sweden.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflicts of interest.
Additional information
Henrik Antti and Tommy Olsson have shared senior authorship.
Rights and permissions
About this article

Cite this article
Chorell, E., Ryberg, M., Larsson, C. et al. Plasma metabolomic response to postmenopausal weight loss induced by different diets. Metabolomics 12, 85 (2016). https://doi.org/10.1007/s11306-016-1013-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11306-016-1013-x