
Abstract
Objectives
The present study investigated the position and relationship of the maxillary third molars to the maxillary sinus. These molars were detected to have a close relationship with the maxillary sinus based on panoramic images, using cone-beam computed tomography (CBCT).
Methods
This retrospective study evaluated 162 impacted third molars from 100 patients that showed a superimposed relationship between the maxillary sinus and third molars on panoramic images obtained from CBCT. CBCT images were used to assess the horizontal (buccopalatal) and vertical positions of the maxillary sinus relative to the maxillary third molars, proximity of the roots to the sinus, and angulation and depth of the third molars. The associations among the angulation, depth of third molars, and horizontal and vertical positions of the maxillary sinus relative to the third molar findings were examined using Chi square tests.
Results
Based on the winter classification, the most frequent tooth position was vertical (59.9 %), followed by mesioangular (14.2 %), distoangular (9.9 %), and others. Most impacted teeth were at the level between the occlusal and cervical levels of the adjacent second molar. Regarding the relationships of the maxillary third molars with the maxillary sinus examined on CBCT, vertical type III (buccal root related with maxillary sinus) (34 %) and horizontal type 2 (maxillary sinus located between roots) (64.8 %) were seen most frequently.
Conclusions
The relationship between the maxillary sinus and third molar roots should be considered during extraction. When a risk of sinus perforation is predicted in an extraction, a presurgical CBCT examination could be valuable.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Maxillary third molars have a high incidence of impaction [1–4]. These teeth are associated with several conditions, such as orofacial pain, caries of the second molar distal surface, odontogenic tumors, certain types of cysts, pericoronitis, and dental crowding [5, 6].
Removal of a maxillary third molar is a surgical process mainly performed by dental surgeons. This surgical procedure may lead to perforations of the maxillary sinus and displacement of the tooth into the sinus [7, 8]. Some researchers have reported that the frequency of such accidents is high [9, 10]. Thus, an anatomical description and knowledge of the relationship between the maxillary third molar and the maxillary sinus are required for diagnosis of sinus pathologies and planning of proper treatment procedures [7].
Panoramic radiographs are usually used to evaluate the relationship between an impacted maxillary third molar and the maxillary sinus [11]. Although a panoramic radiograph is extremely beneficial to oral surgeons for preoperative control, it can present certain deficiencies, such as distortion and two-dimensional view [7]. It is thus impossible to determine the location of the inferior line of the maxillary sinus relative to the roots. However, computed tomography (CT) can provide three-dimensional (3D) views, and clearly visualize the correct location of the third molar and anatomical structures [12, 13].
Cone-beam computed tomography (CBCT) reduces the radiation dose, offers high resolution, decreases costs, and provides better image quality compared with traditional CT. CBCT can clearly visualize the correct relationships of the third molar with adjacent structures [14].
Many studies have evaluated the position of an impacted mandibular third molar and the anatomic relationship between the third molar and the mandibular canal [4, 15–17]. However, there are limited prevalence studies in the literature on the types of impaction of the maxillary third molar and the anatomic relationship between the third molar and the maxillary sinus [1, 18, 19]. Although a few studies have evaluated this issue using both panoramic radiography and traditional CT [7, 11, 13], no reported studies have analyzed the angulation, position, and impaction of the maxillary third molar and the relationship between the maxillary third molar and the surrounding adjacent structures using CBCT. The aim of the present study was to investigate the position and relationship of maxillary third molars to the maxillary sinus, detected to have a close relationship with the maxillary sinus based on panoramic images (panorex images) obtained from CBCT.
Materials and methods
In this study, CBCT images from 100 patients who attended the Department of Oral Diagnosis and Radiology between 2011 and 2013 were used to determine the positions of the maxillary third molars in relation to the maxillary sinus. The CBCT images had been taken to evaluate patients requiring impacted third molar surgery, dental implant surgery, and to examine the maxillary sinus, cysts, trauma, or orthodontic anomalies. Before any CBCT images were obtained, the patients provided informed consent for radiography and examinations according to the principles of the Helsinki Declaration. Only researchers were able to access the acquired data. Owing to the retrospective nature of this study, an exemption in writing was granted by the University of Atatürk Institutional Review Board. The study samples consisted of 162 maxillary third molars that appeared to have a direct relationship with the maxillary sinus on panoramic images of 50-mm thickness generated from CBCT (NewTom FP-DVT 9000; QR, Verona, Italy). The study did not evaluate conventional panoramic radiographs, so that the patients were not exposed to radiation overdoses. The following radiologic parameters were used: 15 mA; 110 kVp; 5.4-s typical X-ray emission time; 36-s scan time; and 17-cm diameter—13-cm height scan volume. The study included CBCT scans with high-resolution images that presented the direct relationship between the maxillary third molar and the maxillary sinus on panorex images. We excluded CBCT scans of patients aged younger than 20 years, with any craniofacial anomaly or syndrome, with any pathological dentoalveolar condition, with poor-quality CBCT images, with incomplete root formation, or missing the adjacent second molar.
The CBCT images were evaluated in all three dimensions by a single examiner in a dark room to determine the relationship of the maxillary third molars to the maxillary sinus in the samples, their levels of depth, and their angulations. The depths of the impacted maxillary third molars were determined according to a modified Archer classification [19] (Fig. 1). In this classification, the depth of the maxillary third molar in relation to the occlusal plane of the adjacent tooth was classified into the following four categories:

Levels of depth of the maxillary third molar with respect to the modified Archer classification on cut panoramic images: a Position A, b Position B, c Position C, d Position D
- Class A:
-
The lowest cusp tubercle of the crown of the maxillary third molar is on a line with the occlusal plane of the second molar.
- Class B:
-
The lowest cusp tubercle of the crown of the maxillary third molar is between the occlusal plane of the second molar and the cervical line.
- Class C:
-
The lowest cusp tubercle of the crown of the maxillary third molar is between the cervical line of the second molar and the mid-third of the root of the second molar.
- Class D:
-
The lowest cusp tubercle of the crown of the maxillary third molar is at or above the apical third of the root of the second molar.
The angulations of the maxillary impacted third molars were documented based on the Winter classification [20] with reference to the position of the long axis of the impacted third molar in relation to the long axis of the second molar (vertical, horizontal, mesioangular, distoangular, buccopalatal, and others) (Fig. 2).

Angulations of the maxillary third molar on panoramic images: a Mesioangular, b Vertical, c Distoangular, d Buccopalatal, e Horizontal, f Inverted
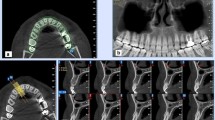
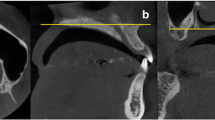
The relationships between the maxillary third molar root apices and the inferior border of the maxillary sinus were evaluated. The vertical relationships between the inferior wall of the maxillary sinus and the maxillary third molar roots were classified into the following five categories using CBCT reformatted cross-section images (Fig. 3):

Vertical relationships between the maxillary third molar and the maxillary sinus on CBCT: a Type I, b Type II, c Type III, d Type IV, e Type V
- Type I:
-
The inferior line of the sinus was observed above the root apices.
- Type II:
-
The inferior wall of the sinus was observed below the root apices.
- Type III:
-
An apical relationship of the buccal root apex was observed over the inferior line of the sinus.
- Type IV:
-
An apical perforation of just the palatal root apex was observed.
- Type V:
-
Apical perforations of the buccal and palatal root apices were observed.
In addition, the horizontal relationships between the inferior wall of the maxillary sinus and the maxillary third molar roots were classified into the following three categories (Fig. 4):

Horizontal relationships between the maxillary third molar and the maxillary sinus on CBCT: a Type 1 (sinus located on the buccal aspect), b Type 2 (sinus located between the roots), c Type 3 (sinus located on the palatal aspect)
- Type 1:
-
The inferior line of the sinus was positioned more toward the buccal aspect than toward the buccal root.
- Type 2:
-
The inferior line of the sinus was positioned between the buccal and palatal roots.
- Type 3:
-
The inferior line of the sinus was positioned more toward the palatal aspect than toward the palatal root.
Statistical analysis
The associations among depths, angulations of the maxillary third molars, and the vertical and horizontal relationship findings were analyzed using the Chi square test. Values of p < 0.05 were regarded as statistically significant. All statistical analyses were carried out using PASW Statistics 18.0 (SPSS Inc., Chicago, IL, USA).
Results
Figure 5 shows the ages and sexes of the patients in our study group. Among the 100 patients, 35 were male and 65 were female, giving a ratio of 1:1.9. The age range was 20–65 years (mean age ± SD: 27.6 ± 8.0 years).

Numbers of patients according to sex and five age categories
Based on the winter classification [20], the most frequent tooth position was vertical (59.9 %), followed by mesioangular (14.2 %), distoangular (9.9 %), buccopalatal (8 %), horizontal (4.9 %), and others (3.1 %). There was no significant difference between the right and left sides in the maxillary third molars (p > 0.05).
The relative depths of impaction of the 162 maxillary third molars were classified as A for 61 (37.7 %), B for 31 (19.1 %), C for 49 (30.2 %), and D for 21 (13 %). There was a significant difference between the relative depth of impaction and the angulation of the maxillary third molars (p < 0.05) (Table 1). There was a significant difference between the relative depth of impaction and angulation and age groups, but no significant difference according to sex (p > 0.05).
On the CBCT images, the vertical relationships between the inferior wall of the sinus and the roots of the maxillary molars were classified into five categories. The most common vertical relationship was type III (34 %), followed by type V (33 %), type II (15 %), type I (12 %), and type IV (6 %).
Regarding the horizontal relationships, type 2 (maxillary sinus located between roots) was observed most frequently. Type 2-II was observed most commonly according to both the vertical and horizontal relationships (Table 2). There was a significant difference between the vertical and horizontal relationships. Moreover, there was a significant difference between the depth of the third molar and the vertical relationship, but no significant difference between the winter classification [20] and the vertical relationship. Meanwhile, there was a significant difference between the tooth angulation and the horizontal relationships.
Discussion
Maxillary sinus perforation may occur after the removal of maxillary third molars that are in close proximity to the sinus floor. According to the considerable variety in the relationship of the maxillary sinus to an impacted maxillary third molar, an accurate radiographic diagnosis is essential to evaluate the relationship between these two anatomical structures [12, 13, 18]. Thus, the relationship is most commonly evaluated by panoramic radiography. However, it is difficult to measure the actual proximity of the maxillary third molar to the sinus floor because panoramic radiographs are associated with disadvantages such as superposition of anatomic structures, horizontal and vertical magnification, and lack of cross-sectional information [7, 11, 12]. Kilic et al. [12] reported that the topographic relationships between the roots and the sinus measured using panoramic radiographs were significantly different from those measured on CT images. Lim et al. [19] reported that it is difficult to evaluate the actual proximity of the third molar to the maxillary sinus inferior wall. Therefore, panoramic radiography is not a reliable method to predict the possibility of an oroantral perforation, and CBCT may be a better method to measure the proximity of the roots of the maxillary third molar to the sinus floor [12, 19]. Thus, we examined only CBCT findings to predict the anatomical position of impacted maxillary third molars and the maxillary sinus.
To our knowledge, this is the first study to evaluate the relationship between the maxillary sinus and the maxillary third molar using CBCT. Knowledge of the precise location of the maxillary sinus is very important, because this information provides knowledge on regions where safe and quick removal of bone should be possible [2, 21]. Deeper impaction of the maxillary third molar means that a larger amount of bone removal is required to reach the third molar, and is therefore more likely to give rise to damage to the sinus floor during operative procedures [19]. In our study, the level of impaction was assessed according to the level of the cemento-enamel junction of the third molar relative to the alveolar bone height, and not according to the relationship to the occlusal surface of the adjacent second molar. This assessment is more objective, because it excludes any normally erupting third molars. Bouquet et al. [7] reported that the impaction levels of maxillary third molars were submucosal and intraosseous. Lim et al. [19] described that the depth of impaction of maxillary third molars serves as a better indication of the possibility of oroantral perforation, and that traditional radiographs are not reliable for predicting this possibility.
Obayashi et al. [13] reported that the vertical positions of the maxillary third molars were well correlated between panoramic and CT image evaluations. These results are consistent with the report by Kurihara et al. [22], who reported on tooth inclination by panoramic radiography. De Carvalho et al. [18] reported that the relative depths of maxillary third molars are important for the prediction of difficulty in surgical removal. However, they did not prove that angulation was a significant factor in the removal of maxillary third molars. These reports are in accordance with our results.
In our study, tooth angulation was evaluated on panoramic images. The most common angulation was the vertical position (59.9 %), followed by the mesioangular position (14.2 %). These findings are in accordance with several previous studies reporting that the vertical angulation type was observed most frequently (range 45.3–95 %) [1, 7, 8, 12, 13, 18, 19, 21]. However, they disagree with Kruger et al. [3], who found that mesioangular impaction was the most frequently observed position of impaction. This discrepancy may be partly explained by differences in sample sizes, races, and radiographic techniques.
Knowledge of the topography and relationship between the root apex and the inferior wall of the maxillary sinus are crucial for diagnosing and treating a sinus pathosis as well as for removing a maxillary third molar. Based on the appearance in panoramic radiography, and consistent with the results of Bouquet et al. [7], Obayashi et al. [13] reported that CT images are more successful than panoramic radiographs for evaluating the root apex of the maxillary third molar relative to the floor of the maxillary sinus. In our study, we investigated the vertical and horizontal relationships between the inferior wall of the maxillary sinus and the maxillary third molars. Until now, these classifications have not been described in any reports. In panoramic radiographs, third molar roots presenting as vertical type II appeared to penetrate the maxillary sinus, although there was no relationship between the roots and the maxillary sinus. In addition, the horizontal relationship may provide oral surgeons with information regarding the surgical approach for maxillary third molars. We described the five vertical relationships and three horizontal relationships seen most frequently in vertical relationships by which the tooth roots had contact with the sinus floor (types III, V, and IV at 34, 33, and 6 %, respectively). However, in contrast to our findings, Kilic et al. [12] reported that in the most frequent vertical relationship, the roots had no contact with the sinus floor. This discrepancy may be partly explained by differences in sample sizes, radiographic interpretations, and radiographic techniques.
The relationship between the maxillary sinus and the third molar roots should be considered during extraction. When a risk of sinus perforation is predicted in an extraction, a presurgical CBCT examination could be valuable.
References
Hashemipour MA, Tahmasbi-Arashlow M, Fahimi-Hanzaei F. Incidence of impacted mandibular and maxillary third molars: a radiographic study in a Southeast Iran population. Med Oral Patol Oral Cir Bucal. 2013;18:e140–5.
Iwai T, Chikumaru H, Shibasaki M, Tohnai I. Safe method of extraction to prevent a deeply-impacted maxillary third molar being displaced into the maxillary sinus. Br J Oral Maxillofac Surg. 2013;51:e75–6.
Kruger E, Thomson WM, Konthasinghe P. Third molar outcomes from age 18 to 26: findings from a population-based New Zealand longitudinal study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;92:150–5.
Nakayama K, Nonoyama M, Takaki Y, Kagawa T, Yuasa K, Izumi K, et al. Assessment of the relationship between impacted mandibular third molars and inferior alveolar nerve with dental 3-dimensional computed tomography. J Oral Maxillofac Surg. 2009;67:2587–91.
Lysell L, Rohlin M. A study of indications used for removal of the mandibular third molar. Int J Oral Maxillofac Surg. 1988;17:161–4.
Brauer HU. Unusual complications associated with third molar surgery: a systematic review. Quintessence Int. 2009;40:565–72.
Bouquet A, Coudert JL, Bourgeois D, Mazoyer JF, Bossard D. Contributions of reformatted computed tomography and panoramic radiography in the localization of third molars relative to the maxillary sinus. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;98:342–7.
Selvi F, Cakarer S, Keskin C, Ozyuvaci H. Delayed removal of a maxillary third molar accidentally displaced into the infratemporal fossa. J Craniofac Surg. 2011;22:1391–3.
Killey H, Kay L. Possible sequelae when a tooth or root is dislodged into the maxillary sinus. Br Dent J. 1964;116:73.
Hirata Y, Kino K, Nagaoka S, Miyamoto R, Yoshimasu H, Amagasa T. A clinical investigation of oro-maxillary sinus-perforation due to tooth extraction. Kokubyo Gakkai Zasshi. 2001;68:249–53.
Jung YH, Nah KS, Cho BH. Correlation of panoramic radiographs and cone beam computed tomography in the assessment of a superimposed relationship between the mandibular canal and impacted third molars. Imaging Sci Dent. 2012;42:121–7.
Kilic C, Kamburoglu K, Yuksel SP, Ozen T. An assessment of the relationship between the maxillary sinus floor and the maxillary posterior teeth root tips using dental cone-beam computerized tomography. Eur J Dent. 2010;4:462–7.
Obayashi N, Ariji Y, Goto M, Izumi M, Naitoh M, Kurita K, et al. CT analyses of the location of the maxillary third molar in relation to panoramic radiographic appearance. Oral Radiol. 2009;25:108–17.
Nakagawa Y, Ishii H, Nomura Y, Watanabe NY, Hoshiba D, Kobayashi K, et al. Third molar position: reliability of panoramic radiography. J Oral Maxillofac Surg. 2007;65:1303–8.
Şekerci AE, Şişman Y. Comparison between panoramic radiography and cone-beam computed tomography findings for assessment of the relationship between impacted mandibular third molars and the mandibular canal. Oral Radiol. 2014;30:170–8.
Hazza’a AM, Albashaireh Z, Bataineh AB. The relationship of the inferior dental canal to the roots of impacted mandibular third molars in a Jordanian population. J Contemp Dent Pract. 2006;7:71–8.
de Melo Albert DG, Gomes ACA, do Egito Vasconcelos BC, de E Silva ED, Holanda GZ. Comparison of orthopantomographs and conventional tomography images for assessing the relationship between impacted lower third molars and the mandibular canal. J Oral Maxillofac Surg. 2006;64:1030–7.
de Carvalho RWF, de Araújo Filho RCA, do Egito Vasconcelos BC. Assessment of factors associated with surgical difficulty during removal of impacted maxillary third molars. J Oral Maxillofac Surg. 2013;71:839–45.
Lim AAT, Wong CW, Allen JC. Maxillary third molar: patterns of impaction and their relation to oroantral perforation. J Oral Maxillofac Surg. 2012;70:1035–9.
Winter G. Principles of exodontias as applied to the impacted third molars: a complete treatise on the operative technic with clinical diagnoses and radiographic interpretations. 1st ed. St. Louis: American Medical Books; 1926. p. 21–58.
Ventä I, Turtola L, Ylipaavalniemi P. Radiographic follow-up of impacted third molars from age 20 to 32 years. Int J Oral Maxillofac Surg. 2001;30:54–7.
Kurihara N, Sasano T, Iikubo M, Kobayashi A, Shimeno Y, Abue M, et al. A diagnostic study on the criteria for extraction of third molars. Part 2: temporal change in third molar positions for the past 21 years (in Japanese). Jpn J Oral Diag Oral Med. 2003;16:32–40.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Omer Demirtas and Abubekir Harorli declare that they have no conflict of interest.
Human rights statements and informed consent
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions. Informed consent was obtained from all patients for being included in the study.
Rights and permissions
About this article

Cite this article
Demirtas, O., Harorli, A. Evaluation of the maxillary third molar position and its relationship with the maxillary sinus: a CBCT study. Oral Radiol 32, 173–179 (2016). https://doi.org/10.1007/s11282-015-0228-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11282-015-0228-2