
Abstract
Background
Normative distribution of serum cystatin C and relationship with sex and age in healthy adult Chinese population is unknown.
Methods
This is a prospective cohort study. Adult subjects (18 years of age and older) who underwent annual health examination at the Health Management Center in Sir Run Run Hospital were eligible. Subjects with major diseases, e.g., hypertension, diabetes, chronic kidney disease, obesity (body mass index ≥ 28 kg/m2) were excluded from the analysis. Multivariate logistic regression analysis was conducted to identify risk factors of elevated cystatin C (> 1.03 mg/L). Data are shown as median and 95% confidence interval (CI).
Results
The final analysis included a total of 10,640 subjects (40 ± 12 years, 52% men). The median serum cystatin C concentration was 0.73 mg/L (95% CI 0.52–1.03 mg/L) in the overall analysis, 0.79 (95% CI 0.59–1.07 mg/L) in men, and 0.67 (95% CI 0.49–0.95 mg/L) in women. In the multivariate regression analysis, elevated cystatin C was independently associated with the male sex (odds ratio 1.94; 95% CI 1.07–3.52), older age (odds ratio 1.04 every year; 95% CI 1.02–1.06), higher body mass index (odds ratio 1.70; 95% CI 1.01–2.83), uric acid (odds ratio 1.00; 95% CI 1.00–1.01), and β2-microglobulin (odds ratio 39.35; 95% CI 22.90–67.64).
Conclusion
The median serum cystatin C concentration was 0.73 (95% CI 0.52–1.03 mg/L) in healthy adult Chinese population, 0.79 (95% CI 0.59–1.07 mg/L) in men, and 0.67 (95% CI 0.49–0.95 mg/L) in women. Elevated cystatin C was associated with the male sex, older age and higher body mass index.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Clinically, renal function is often evaluated with indicators such as serum creatinine, urea and cystatin C. Creatinine and urea easily fluctuate with muscle mass, diet and age; but cystatin C does not, and is less likely to be reabsorbed and catabolized by the tubular epithelial cells [1]. Normal cystatin C ranges have been extensively investigated [2,3,4,5,6,7,8], including those in Chinese population [3, 6], but age- and gender-adjusted reference values and influencing factors of cystatin C in healthy Chinese population were not clearly investigated. Therefore, we conducted this study to propose the reference values of cystatin C in healthy Chinese populations.
Data and methods
Study population
This prospective cohort study was approved by the Ethics Committee of Nanjing Medical University (2018–462), and registered in the US Clinical Trial website (ES-CKD ClinicalTrials.gov number, NCT02841371). Clinical data were collected from 14,736 patients in the Sir Run Run Hospital of Nanjing Medical University from May 1, 2018 to April 1, 2021. The criterion for inclusion was adults having received health examination at the Health Management Center in Sir Run Run Hospital. Excluded were those aged less than 18 years, or with current chronic kidney disease, acute kidney injury, obesity (body mass index, BMI ≥ 28), coronary heart disease, as well as history of hypertension (blood pressure ≥ 140/90 mmHg), diabetes (fasting plasma glucose ≥ 7 mmol/L) and other chronic diseases. Finally, 10,640 healthy participants were included.
Methods
Data were collected from May 2018 to April 2021, involving age, sex, BMI, blood pressure, previous history, serum creatinine, cystatin C, urea, β2 microglobulin, uric acid (UA), fasting plasma glucose (FPG), and urine protein. Among them, the biochemical values were tested from blood samples and morning urine. Creatinine was determined by the Roche sarcosine oxidase method, and the variation coefficient of creatinine was 3.5% (normal reference range 57–97 μmol/L for males, 41–73 μmol/L for females). Serum creatinine was assayed by IDMS-traceable calibration for the standard reference material (SRM 967) in our study. Serum cystatin C was examined with particle enhanced turbidimetric immunoassay, and calibrated according to the international certified reference material ERM-DA471 with a variation coefficient of 7.5% (normal reference range is 0.59–1.03 mg/L). β2 microglobulin was determined by Roche Particle enhanced turbidimetric immunoassay with a variation coefficient of 6.71% (normal reference range 1.0–2.3 mg/L); uric acid by Roche colorimetry with a variation coefficient of 3% (normal reference range 208–428 μmol/L for males, 155–357 μmol/L for females); urea by Roche colorimetry with a variation coefficient of 2.67% (normal reference range 3.1–8.0 mmol/L for males, 2.6–7.5 mmol/L for females); glucose by hexokinase method with a variation coefficient of 2.2% (normal reference range 3.9–6.1 mmol/L). All biochemical indexes were tested using Roche Cobas c701 automatic biochemical analyzer. CKD was diagnosed with reference to the Natural Kidney Foundation Kidney-Disease Outcome Quality Initiative (NKF-K/DOQI) Guidelines: clinical evidence of kidney injury and/or GFR < 60 ml/min/1.73m2 lasting > 3 months.
Statistical analysis
Data statistics and graphics were processed by Office Excel 2019 and SPSS 22.0. Continuous variables were represented by mean ± standard deviation or median, and t test was used to analyze normal distribution data. The 2.5th percentile (P2.5) and 97.5th percentile (P97.5) were used to reflect the 95% reference range for non-normal distribution data. Age-creatinine and age-cystatin C levels line charts were drawn to display the trends and differences between P2.5, median and P97.5 values in different groups. Multivariate logistic regression analysis was adopted to observe the effects of gender and age on, creatinine and cystatin C levels in healthy participants. Statistical significance was considered at p < 0.05.
Results
Study population characteristics
A total of 14,736 participants were recruited, with 8570 males (58%) and 6,209 females (42%), and a mean age of 42 ± 13 years (Table 1). This cohort included 7,110 young (18–39 years) participants (48.25%), 6995 middle-aged (40–64 years) participants (47.47%), and 631 elderly (65 years or more) (4.28%). The mean value of the creatinine was 66 ± 16 μmol/L, and that of the cystatin C was 0.76 ± 0.14 mg/L. After removing patients of obesity (n = 1903), hypertension (n = 2424), diabetes (n = 918), CKD and acute renal injury (n = 111), 10,640 healthy participants were included. Among them were 5482 males and 5158 females, with a mean age of 40 ± 12 years (Table 1). In terms of age, 5852 participants were young, 4468 were middle-aged, and 320 were elderly. All data did not conform to a normal distribution.
Confidence intervals of cystatin C in the healthy population
The 95% confidence interval of cystatin C was 0.52–1.03 mg/L in the entire healthy population, 0.59–1.07 mg/L in men, and 0.49–0.95 mg/L in women (Table 2). Cystatin C in men was higher than that in women, and increased with age.
Multivariate logistic regression analysis in the healthy population
The variables were assigned according to Online supplementary Table S1. As shown by the multivariate logistic regression analysis, higher serum urea, uric acid, and β2-microglobulin were risk factors for elevated serum creatinine after adjustment for age, sex, BMI, blood pressure, diabetes and urine protein + (Online supplementary Table S2). Age, sex, BMI, blood pressure, fasting glucose and urine protein + were not associated with elevated serum creatinine. In addition, the risk of elevated cystatin C (> 1.03 mg/L) in men was 1.94 times (95% CI 1.07–3.52) that in women and the risk of cystatin C increased by 4% (95% CI 2%-6%) every year with age. Higher BMI (odds ratio 1.70; 95% CI 1.01–2.83), uric acid (odds ratio 1.00; 95% CI 1.00–1.01), and β2-microglobulin (odds ratio 39.35; 95% CI 22.90–67.64) were risk factors for elevated serum cystatin C after adjustment for BMI, blood pressure, diabetes and urine protein + (Online supplementary Table S3). Blood pressure, fasting glucose, urea and urine protein were not associated with elevated serum cystatin C.
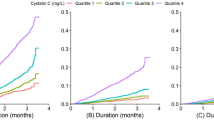
Distribution of creatinine and cystatin C in subgroups of age and sex
Four figures illustrated the distributions of serum creatinine and cystatin C in subgroups of age and sex (Online supplementary Figs S1–S4). The level of serum creatinine increased in the elderly, and the level of serum cystatin C increased with age in all age subgroups, especially in those of females.
Discussion
In 2017, 697.5 million cases of various stages of CKD were recorded, with a global prevalence of 9.1% (8.5–9.8) [9], and 10.8% in China, the most inflicted country [10]. The elderly patients aged over 65 years accounted for 53.07% of the CKD population [11]. To control this disease, efficient diagnostic indexes are of utmost importance.
In the present study, we found that the cystatin C level in males exceeded that in females by an average of 0.12 mg/L (Table 2), and was positively associated with age (+0.05 mg/L for every 10 years). The normal cystatin C level was significantly higher in the elderly than in the young. These findings are similar to the data in previous studies, including those in Chinese [3, 6], Japanese [2] and American [4]. A study has suggested that cystatin C is not associated with sex [8].
Cystatin C is constantly and independently produced by the glomerular base membrane of nuclear cells, reabsorbed and fully metabolized by proximal convoluted tubules; therefore, its level remains stable, despite changes in muscle content and protein intake [12, 13], age and sex [14]. Cystatin C concentration is independent on race or genetic ancestry, which is a major advantage that needs to be emphasized [15]. Studies have shown that cystatin C is affected by age, sex, BMI, smoking status, C-reflection protein, hypertension, and other factors [16,17,18]. Our study showed a sex-related difference in cystatin C in the healthy subjects. Cystatin C in men was higher than that in women, and increased with age.
Our data in healthy participants showed that cystatin C was associated with BMI after full adjustment, similar to the findings in previous studies [19, 20]. In our study, higher BMI, uric acid, and β2-microglobulin were risk factors for elevated serum cystatin C after full adjustment.
Through this prospective analysis with a big Chinese cohort, we obtained a new normal range of cystatin C, with its P2.5 and P97.5 as reference values.
This study also has limitations. First, it was a single-center prospective cohort study, and suspected cases were not followed up. Second, our data only include qualitative examination of urine protein, not quantitative examination.
In conclusion, our study provides age-adjusted reference values of cystatin C in a Chinese population. Creatinine and cystatin C increase with uric acid and β-microglobulin. Male is a risk factor for elevated cystatin C, but not for elevated serum creatinine. Cystatin C is associated with higher BMI.
Data availability
All data generated or analyzed during this study are included in this article and its online supplementary material files. Further enquiries can be directed to the corresponding author.
References
Stevens LA, Coresh J, Greene T, Levey AS (2006) Assessing kidney function–measured and estimated glomerular filtration rate. N Engl J Med 354(23):2473–2483
Ichihara K, Saito K, Itoh Y (2007) Sources of variation and reference intervals for serum cystatin C in a healthy Japanese adult population. Clin Chem Lab Med 45(9):1232–1236
Li DD, Zou MN, Hu X, Zhang M, Jia CY, Tao CM, Wang LL, Ying BW (2012) Reference intervals and factors contributing to serum cystatin C levels in a Chinese population. J Clin Lab Anal 26(2):49–54
Juraschek SP, Coresh J, Inker LA, Levey AS, Köttgen A, Foster MC, Astor BC, Eckfeldt JH, Selvin E (2013) Comparison of serum concentrations of β-trace protein, β2-microglobulin, cystatin C, and creatinine in the US population. Clin J Am Soc Nephrol 8(4):584–592
Odden MC, Tager IB, Gansevoort RT, Bakker SJ, Katz R, Fried LF, Newman AB, Canada RB, Harris T, Sarnak MJ, Siscovick D, Shlipak MG (2010) Age and cystatin C in healthy adults: a collaborative study. Nephrol Dial Transplant 25(2):463–469
He M, Ke PF, Chen WY, Lin HB, Wang YX, Wan ZM, Wu XZ, Zhuang JH, Huang XZ (2017) Clinical correlates and reference intervals for cystatin C in a Han population from Southeast China. clin lab 63(3):607–615
Hannemann A, Friedrich N, Dittmann K, Spielhagen C, Wallaschofski H, Völzke H, Rettig R, Endlich K, Lendeckel U, Stracke S, Nauck M (2011) Age- and sex-specific reference limits for creatinine, cystatin C and the estimated glomerular filtration rate. Clin Chem Lab Med 50(5):919–926
Weinert LS, Prates AB, do Amaral FB, Vaccaro MZ, Camargo JL, Silveiro SP (2010) Gender does not influence cystatin C concentrations in healthy volunteers. Clin Chem Lab Med 48(3):405–408
GBD Chronic Kidney Disease Collaboration (2020) Global, regional, and national burden of chronic kidney disease, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 395(10225):709–733
Zhang L, Wang F, Wang L et al (2012) Prevalence of chronic kidney disease in China: a cross-sectional survey. Lancet 379(9818):815–822
Liu BC, Wu XC, Wang YL et al (2008) Investigation of the prevalence of CKD in 13383 Chinese hospitalised adult patients. Clin Chim Acta 387(1/2):128–132
Schacffner ES, Ebert N, Delanaye P et al (2012) Two novel equations to estimate kidney function in persons aged 70years or older. Ann Intern Med 157(7):471–481
Alshaer IM, Kilbrride HS, Stevens PE et al (2014) External validation of the Berlin equations for estimation of GFR in the elderly. Am J Kidney Dis 63(5):862–865
Schwartz GJ, Schneider MF, Maier PS et al (2012) Improved equations estimating GFR in children with chronic kidney disease using an immunonephelometric determination of cystatin C. Kidney Int 82(4):445–453
Hsu CY, Yang W, Parikh RV, CRIC Study Investigators et al (2021) Race, genetic ancestry, and estimating kidney function in CKD. N Engl J Med 385(19):1750–1760
Wei L, Ye X, Pei X et al (2014) Reference intervals for serum cystatin C and factors influencing cystatin C levels other than renal function in the elderly. PLoS One 9(1):e86066
Pei X, Bao L, Xu Z et al (2013) Diagnostic value of cystatin C and glomerular filtration rate formulae in Chinese nonelderly and elderly populations. J Nephrol 26(3):476–484
Knight EL, Verhave JC, Spieglman D et al (2004) Factors influencing serum cystatin C levels other than renal function and the impact on renal function measurement. Kidney Int 65(4):1416–1421
Mathisen UD, Melsom T, Ingebretsen OC et al (2011) Estimated GFR associates with cardiovascular risk factors independently of measured GFR. J Am Soc Nephrol 22(5):927–937
Liu X, Foster MC, Tighiouart H, Anderson AH, Beck GJ, Contreras G, CRIC (Chronic Renal Insufficiency Cohort) Study Investigators et al (2016) Non-GFR determinants of low-molecular-weight serum protein filtration markers in CKD. Am J Kidney Dis 68(6):892–900
Funding
This work was supported by grants from Guiding Project of Jiangsu Commission of Health (Z201842), Chinese Society of Nephrology (14050430580) and High-level Talents of the Fifteenth “Six Talents Peaks” in Jiangsu Province (WSN-113). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
XD: contributed to the study conception and design. Methods preparation and data collection were performed by MJ and YF. Analysis was performed by XW. The first draft of the manuscript was written by MJ and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to declare.
Ethical approval
This study was approved by the Institutional Review Boards of Nanjing Medical University (IRB no.2018-462). All procedures involving human participants were in accordance with the ethical standards of the institutional and national research committee, and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. All participants in this manuscript provided their written informed consent in this study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ji, M., Fu, Y., Wan, X. et al. Age-adjusted reference values and influencing factors of cystatin C in healthy Chinese population. Int Urol Nephrol 55, 1641–1644 (2023). https://doi.org/10.1007/s11255-023-03497-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-023-03497-1