
Abstract
Objective
To investigate the efficacy of exercise training on functional capacity and quality of life in chronic kidney disease.
Data sources
SCOPUS, CINAHL, Science Direct, Web of Science, MEDLINE, ProQuest, Physiotherapy Evidence Database (PEDRO), and Google Scholar databases were searched between 2010 and December 2020.
Methods
Randomized controlled trials were included if they involved any types of exercise training (aerobic, resisted and respiratory ex.) conducted with chronic kidney disease patients. Three authors independently screened articles, extracted data, and assessed the methodological quality using PEDro scale, and two authors released any confliction. Modified Sackett Scale was used to determine the level of evidence for each outcome.
Results
Out of 130 papers screened, 13 studies with 619 participants met the inclusion criteria. The frequency of the treatment ranged from three to four sessions per week for a period ranging from 8 to 24 weeks. According to the Pedro scale, the quality of studies ranged from good (three studies) to fair (ten studies). All included studies showed positive effects on the measured outcomes (functional capacity and quality of life in chronic kidney disease).
Conclusion
Exercise programs for chronic kidney disease patients provide beneficial clinical outcomes and optimize functional capacity and quality of life in those patients. Future studies still need to focus on high-quality evidence and studies evaluating the adverse effects of exercise.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Studies of chronic kidney disease (CKD) in several countries have reported that about 12% of the population presents CKD. This rate increases with increasing age [1]. Persons diagnosed with CKD present high morbidity and mortality due to cardiovascular diseases (CVD), low quality of life (QOL), limitation of functional capacity, and metabolic, musculoskeletal disorders [2].
The mortality rate of CKD patients on dialysis is higher than that for individuals in the age-matched population. In Saudi Arabia, the rate of CKD increased in the last three decades due to the rapid changes in lifestyle and high population growth. By the end of 2014, a total of 15,782 dialysis patients were receiving treatment in 187 dialysis centers in the Kingdom of Saudi Arabia, 14,366 of them treated by hemodialysis (HD) and the remaining 1416 by peritoneal dialysis (PD) [3]. The correlation between physical inactivity and poor physical and social outcomes is well established for patients presenting with CKD [4]. Compared with other populations, these patients exhibit reduced physical activity in association with metabolic acidosis, inflammation, and malnutrition, which in turn can induce reduced neuromuscular functioning, reduced exercise tolerance, and reduced cardiorespiratory fitness [5, 6]. Also, we should consider behavioral and pathophysiological factors, such as muscle mass or anemia, and logistical factors, such as time spent on dialysis and traveling to the clinic, as all these factors may contribute to the worsening of physical activity [7].
It is well known that exercise therapy programs lead to an improvement in the functional capacity and life quality of CKD patients due to a positive effect on skeletal and cardiac muscles as well as improved vascular health. Therefore, regular physical activity is strongly recommended for CKD patients [8, 9].
Patients presenting with CKD and their relatives experience different kinds of stress during the duration of their illness and treatment because of the chronicity of the disease and its long-term treatment. Patients report discomfort and disruption in life as they spend hours in dialysis treatments. CKD also stresses the relatives because the treatment is life-time and because of the financial costs of the treatment [10].
Methods
SCOPUS, CINAHL, Science Direct, Web of Science, MEDLINE, ProQuest, Physiotherapy Evidence Database (PEDRO), and Google Scholar were searched without restrictions regarding language or the year of publication. The keywords “exercise training,” “quality of life,” “functional capacity,” and “CKD patient” were used to search from 2010 until December 2020. The screening for eligibility was conducted using the Rayyan QCRI software for systematic reviews [11].
Three independent reviewers (AAI, OWA, and MRA) assessed titles and abstracts of the trials identified by the search against the eligibility criteria (Table 1). All the articles considered potentially eligible were obtained in full text, and additional manual screening of reference lists of the eligible studies was performed. The exclusion criteria for this study included studies based on animal data, studies including subjects who were healthy in experimental settings, and study designs other than RCT such as quasi-experimental, systematic review, case studies, and reports.
The quality of the included studies was assessed using the PEDro scale [12]. Three authors (AAI, OWA, MRA) rated the included studies using the PEDro scale, with any conflict being resolved by two authors (HMH and WKA). The following classification was used for rating the methodological quality: a PEDro score of < 4 indicated poor quality, a score of 4–5 indicated fair quality, a score of 6–8 indicated good quality, and a score of 9–10 indicated excellent quality [13]. The methodological quality of the studies was assessed according to the criteria of the PEDro scale 10, which scores 11 items, namely: (1) eligibility criteria, (2) random allocation, (3) hidden allocation, (4) baseline comparability, (5) blind subjects, (6) blind therapists, (7) blind assessors, (8) proper follow-up, (9) intent to treat analysis, (10) group comparisons, and (11) point estimates and variability. Items are scored as present 1 or absent 0, generating a maximum sum of 10 points, and the first item is not counted. For the interpretation of results, we used the Modified Sackett Scale to determine the level of evidence for each outcome [14].
Results
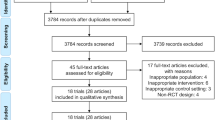
The initial search of all engines resulted in a total of 130 studies: Scopus “27”, Science direct “25”, PEDro “10”, Medline “23”, CINAHL “10”, Web of Science “10”, Google Scholar “5”, and ProQuest “20”. After filtering the articles against the eligibility criteria, 13 trials were included in the review [15,16,17,18,19,20,21,22,23,24,25,26,27]. The selection process of the studies is completely described in the flowchart of Fig. 1. The final included trial had a total of 619 patients presenting with CKD, both sexes included, aged ≤ 80 years old. The characterization of the sample, exercise programs, and the main outcomes are illustrated in Table 2. The studies were arranged in descending order according to the scores in the PEDro score. The quality of the selected studies according to the PEDro scale was fair and good: three studies were of good quality [18, 19, 24] with the level of evidence 1b (Moderate) based on the Modified Sackett Scale, and the other ten studies were fair [15,16,17, 20,21,22,23, 25,26,27] with a level of evidence 2b (Limited). Regarding the intervention in the selected studies (aerobic, resisted, and respiratory exercises) [15,16,17,18,19,20,21,22,23,24,25,26,27], the frequency ranged from 3 to 4 sessions per week for the period ranging from 8 to 24 weeks. The exercise protocol was carried out for HD patients during dialysis in eleven studies [17,18,19,20,21,22,23,24,25,26,27] and for non-dialysis day in one study [15]. Further, in one study, exercise was conducted for a non-dialysis dependent patient presenting with CKD [16] (Table 3).

PRISMA flow diagram of studies through the review [7]
Quality of life was assessed in eleven studies from the included trials [16, 17, 19,20,21,22,23,24,25,26,27] by applying the Short Form Health Survey (SF-36) and the QOL-SF 1.3 questionnaire, both of which measured quality of life in chronic renal patients. Functional capacity was measured in 12 studies from the included trials using the Six-Minute Walk Test [15,16,17,18, 20,21,22,23,24,25,26,27] and the Shuttle Walk Test (ISWT) in one study [19].
Marchesan et al. and Fernandes et al. [18, 24] adopted the same strategy of treatment (aerobic exercise versus control with no exercise). The intervention was done during the dialysis session, and the result showed significant improvement in exercise capacity using the Six-Minute Walk Test (see Table 4), based on the weighted mean difference (95% CI) and the overall effect (Z = 3.59, p = 0.003) of the aerobic exercise vs no exercise on the Six-Minute Walk Test.
Abdelaal and Abdulaziz and Rosa et al. [15, 27] performed the same treatment protocol (aerobic exercise vs resisted exercise). The intervention was conducted during the dialysis session, and the result showed significant improvement in the exercise capacity using the Six-Minute Walk Test (see Table 4). It discussed the weighted mean difference (95% CI) and the overall effect (Z = 9.18, p < 0.001) of the aerobic exercise vs resisted exercise on the Six-Minute Walk Test (Table 5).
Frih et al. and Jamshidpour et al. [20, 22] adopted the same strategy of treatment (combined resisted aerobic exercise vs no exercise). The intervention was carried out during the dialysis session, and the result showed significant improvement in the exercise capacity using Six-Minute Walk Test, see Table 4, discussing the weighted mean difference (95% CI) and the overall effect (Z = 6.19, p < 0.001) of the combined resisted aerobic exercise vs no exercise (Table 6).
Discussion
The prevalence of CKD has increased dramatically. CKD has been associated with many complications and a high mortality rate [28]. Functional capacity is often severely impaired in CKD patients because of the disease’s side effects and its complications [29]. Reduction in functional capacity is one of the important complaints of dialysis patients, manifested by decreased exercise tolerance and reduction of daily life activities. Both the HD procedure and uremic myopathy are associated with muscle protein breakdown, affecting peripheral and proximal muscles with a strong impact on overall physical capacity [30].
The outcomes of the included studies showed that exercise training has a positive effect on the functional capacity and quality of life of CKD patients. Intradialytic exercise training has been shown to improve dialysis efficacy by increasing blood flow and perfusion of the muscle tissue and enlarging the surface area, which diffuses greater flux in circulating toxins and urea from the muscle to circulation and removal by dialysis [31, 32]. This is in agreement with Huang et al.’s [33] systematic review that showed that different types of exercise for more than 8 weeks can effectively improve quality of life in CKD patients on dialysis.
The study conducted by Ouzouni et al. [9] established that intra-dialytic resistance training exercise resulted in a significant improvement in physical functioning. It was shown that patients under dialysis can participate safely in a resistance training program and that there is no hemodynamic and musculoskeletal complication as a result of the exercise program. This improvement can be attributed to the functional, morphological, and neural adaptations of the skeletal muscles for resistance training. However, other studies showed a decrease in the walking capacity and have not observed any statistically significant increase in the Six-Minute Walk Test after exercise intervention [34, 35].
Two studies were conducted by Fernandes et al. and Marchesan et al. to analyze the effects of physical training (PT) using aerobic training on the physical fitness of patients undergoing HD, and revealed significant improvement in functional capacity post-treatment in the experimental group using the Six-Minute Walk Test. Further, QoL was measured by Marchesan et al. and improvement was observed in the study group [18, 24].
Studies by Abdelaal and Abdulaziz [15], and Rosa et al. [27] were conducted to analyze the effects of physical training (PT) on the functional capacity of HD patients. They revealed significant improvement in functional capacity post-treatment in the experimental group using the Six-Minute Walk Test; however, QoL measured by Rosa et al. [27] revealed no difference between the study groups. This is in agreement with the study of Headley et al. [36] who showed a significant improvement in the distance measured with the Six-Minute Walk Test after training CKD patients.
One of the explanations for the significant gain in functional capacity was the use of a combined aerobic and strength training program. This suggests that impairment of functional capacity may be decreased by the gain of muscle strength and improved muscle atrophy, and has beneficial effects on overall work performance [37].
The studies carried out by Frih et al. [20] and Jamshidpour et al. [22] using PEDro score 5 assessed the combined resisted aerobic exercise vs. no exercise during the dialysis session and found a significant improvement in the exercise capacity using the Six-Minute Walk Test.
QoL was measured using a short form (SF-36 questionnaire). Frih et al. [20] revealed a significant improvement in the physical and mental components after 4 months of training. On the other hand, Jamshidpour et al. [22] found neither any significant changes in any of the eight generic subscales of HRQoL nor in the exercise training group or controls following an 8-week study, possibly due to the duration of the study and the characteristics of the selected patients. These results are in line with the study by Wu et al. [38], which showed that combined aerobic and resistance exercise had no significant effect on all the domains of QoL, physical or mental. This contradicts the Cochrane systematic review results by Heiwe and Jacobson [39] which concluded that regular exercise can improve QoL in CKD patients.
The only study in our investigation that used home-based versus center-based aerobic exercise in non-dialysis dependent patients with CKD (NDD-CKD) was carried out by Aoike et al. [16] using the Six-Minute Walk Test for measuring functional capacity, and QoL (SF-36) questionnaire for measuring QoL. The results of this study revealed significant improvement in the Six-Minute Walk Test after 12 weeks, and the duration was further increased after 24 weeks in both exercise groups. No changes were found in the control group, and this improvement was maintained after 24 weeks [16]. It was also documented that aerobic exercise training with low-intensity provides efficient influences on QoL, psychological status, and physical performance in CKD patients [40].
There was limited data for NDD-CKD patients, which showed that these patients had better QoL scores than the patients on dialysis, possibly due to less impaired physical capacity and better clinical condition with fewer complications [36, 41, 42]. The findings of our systematic review are in agreement with the meta-analysis of Heiwe and Jacobsen, published in 2011 [39] and updated in 2014 [43]. They found a significant improvement in the various types of exercise for CKD patients, physical fitness, walking capacity, muscular functioning, cardiovascular function, and HRQOL, with stronger evidence for dialysis patients and aerobic exercise programs [43].
Also, our review is in agreement with the systematic review by Barcellos et al. [44] who found significant improvement in physical fitness and QoL after conducting the aerobic exercise in CKD patients under dialysis. These findings indicate that exercise may have multiple benefits for the functional capacity and QoL of non-dialysis dependent CKD patients who make up the largest part of the CKD population, however, there are still relatively few studies of exercise in this group.
Conclusion
Conducting an exercise training program for CKD patients is feasible and effective, as assessed by a statistically and clinically significant improvement in functional capacity, measured by the Six-Minute Walk Test, and QoL, measured by the QOL-SF questionnaire. Future studies are still needed to concentrate on high-quality evidence and to assess the benefits and adverse effects of exercise in patients presenting with CKD. Further, they will also be able to provide more comprehensive evidence for developing exercise programs.
References
Steenbergen K, Mackenzie L (2004) Professional support in rural New South Wales: perceptions of new graduate occupational therapists. Aust J Rural Health 12(4):160–165
Kalantar-Zadeh K, Block G, Humphreys MH, Kopple JD (2003) Reverse epidemiology of cardiovascular risk factors in maintenance dialysis patients. Kidney Int 63(3):793–808
Almutairi FM, Al-Duais MA, Shalaby KA, Sakran MI (2017) Analysis of patients with end-stage renal disease on dialysis in Tabuk City, Saudi Arabia: a single-center, three-year retrospective study. Saudi J Kidney Dis Transpl 28(2):349–354
Johansen KL (2007) Exercise in the end-stage renal disease population. J Am Soc Nephrol 18(6):1845–1854
Kalantar-Zadeh K, Kilpatrick RD, McAllister CJ, Greenland S, Kopple JD (2005) Reverse epidemiology of hypertension and cardiovascular death in the hemodialysis population: the 58th annual fall conference and scientific sessions. Hypertension 45(4):811–817
Zelle DM, Klaassen G, Van Adrichem E, Bakker SJ, Corpeleijn E, Navis G (2017) Physical inactivity: a risk factor and target for intervention in renal care. Nat Rev Nephrol 13(3):152–168
Bauman AE, Reis RS, Sallis JF, Wells JC, Loos RJ, Martin BW et al (2012) Correlates of physical activity: why are some people physically active and others not? Lancet 380(9838):258–271
Suliman M, Stenvinkel P, Qureshi AR, Kalantar-Zadeh K, Barany P, Heimbürger O et al (2006) The reverse epidemiology of plasma total homocysteine as a mortality risk factor is related to the impact of wasting and inflammation. Nephrol Dial Transplantat 22(1):209–217
Ouzouni S, Kouidi E, Sioulis A, Grekas D, Deligiannis A (2009) Effects of intradialytic exercise training on health-related quality of life indices in haemodialysis patients. Clin Rehabil 23(1):53–63
Hawamdeh S, Almari AM, Almutairi AS, Dator WLT (2017) Determinants and prevalence of depression in patients with chronic renal disease, and their caregivers. Int J Nephrol Renovasc Dis 10:183–189
Johnson N, Phillips M (2018) Rayyan for systematic reviews. J Electron Resour Librariansh 30(1):46–48
Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M (2003) Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther 83(8):713–721
Valkenet K, van de Port IG, Dronkers JJ, de Vries WR, Lindeman E, Backx FJ (2011) The effects of preoperative exercise therapy on postoperative outcome: a systematic review. Clin Rehabil 25(2):99–111
Straus SE, Richardson W, Glasziou P, Haynes R (2005) How to practice and teach EBM. Evid Bas Med, 3rd edn. Elservier, pp 13–29
Abdelaal AAM, Abdulaziz EM (2019) Effect of exercise therapy on physical performance and functional balance in patients on maintenance renal hemodialysis: randomized controlled study. J Exerc Rehabil 15(3):472–480
Aoike DT, Baria F, Kamimura MA, Ammirati A, Cuppari L (2018) Home-based versus center-based aerobic exercise on cardiopulmonary performance, physical function, quality of life and quality of sleep of overweight patients with chronic kidney disease. Clin Exp Nephrol 22(1):87–98
de Lima MC, de Cicotoste CL, da Cardoso KS, Forgiarini LA Jr, Monteiro MB, Dias AS (2013) Effect of exercise performed during hemodialysis: strength versus aerobic. Ren Fail 35(5):697–704
Fernandes ADO, Sens YADS, Xavier VB, Miorin LA, Alves VLDS (2019) Functional and respiratory capacity of patients with chronic kidney disease undergoing cycle ergometer training during hemodialysis sessions: a randomized clinical trial. Int J Nephrol 2019:7857824
Figueiredo PHS, Lima MMO, Costa HS, Martins JB, Flecha OD, Gonçalves PF et al (2018) Effects of the inspiratory muscle training and aerobic training on respiratory and functional parameters, inflammatory biomarkers, redox status and quality of life in hemodialysis patients: a randomized clinical trial. PLoS ONE 13(7):e0200727
Frih B, Jaafar H, Mkacher W, Ben Salah Z, Hammami M, Frih A (2017) The effect of interdialytic combined resistance and aerobic exercise training on health related outcomes in chronic hemodialysis patients: the Tunisian randomized controlled study. Front Physiol 8:288
Frih B, Mkacher W, Bouzguenda A, Jaafar H, Alkandari SA, Salah ZB et al (2017) Effects of listening to Holy Qur’an recitation and physical training on dialysis efficacy, functional capacity, and psychosocial outcomes in elderly patients undergoing haemodialysis. Libyan J Med 12(1):1372032
Jamshidpour B, Bahrpeyma F, Khatami M-R (2020) The effect of aerobic and resistance exercise training on the health related quality of life, physical function, and muscle strength among hemodialysis patients with Type 2 diabetes. J Bodyw Mov Ther 24(2):98–103
Lazarus ER (2019) Effectiveness of education and exercise on quality of life among patients undergoing hemodialysis. Clin Epidemiol Glob Health 7(3):402–408
Marchesan M, Nunes VGDS, Rombaldi AJ (2014) Physical training improves physical fitness and the quality of life of patients on hemodialysis. Rev Bras Cineantropom Desempenho Hum 16(3):334–344
Nilsson BB, Bunæs-Næss H, Edvardsen E, Stenehjem A-E (2019) High-intensity interval training in haemodialysis patients: a pilot randomised controlled trial. BMJ Open Sport Exerc Med 5(1):e000617
Pellizzaro CO, Thomé FS, Veronese FV (2013) Effect of peripheral and respiratory muscle training on the functional capacity of hemodialysis patients. Ren fail 35(2):189–197
Rosa CSDC, Nishimoto DY, Souza GDE, Ramirez AP, Carletti CO, Daibem CGL et al (2018) Effect of continuous progressive resistance training during hemodialysis on body composition, physical function and quality of life in end-stage renal disease patients: a randomized controlled trial. Clin Rehabil 32(7):899–908
Matsufuji S, Shoji T, Yano Y, Tsujimoto Y, Kishimoto H, Tabata T et al (2015) Effect of chair stand exercise on activity of daily living: a randomized controlled trial in hemodialysis patients. J Ren Nutr 25(1):17–24
Kosmadakis GC, Bevington A, Smith A, Clapp E, Viana J, Bishop N et al (2010) Physical exercise in patients with severe kidney disease. Nephron Clin Pract 115(1):c7–c16
Ikizler TA, Pupim LB, Brouillette JR, Levenhagen DK, Farmer K, Hakim RM et al (2002) Hemodialysis stimulates muscle and whole body protein loss and alters substrate oxidation. Am J Physiol Endocrinol Met 282(1):E107–E116
Brown PDS, Rowed K, Shearer J, MacRae JM, Parker K (2018) Impact of intradialytic exercise intensity on urea clearance in hemodialysis patients. Appl Physiol Nut Metab 43(1):101–104
Sheng K, Zhang P, Chen L, Cheng J, Wu C, Chen J (2014) Intradialytic exercise in hemodialysis patients: a systematic review and meta-analysis. Am J Nephrol 40(5):478–490
Huang M, Lv A, Wang J, Xu N, Ma G, Zhai Z et al (2019) Exercise training and outcomes in hemodialysis patients: systematic review and meta-analysis. Am J Nephrol 50(4):240–254
Cheema B, Abas H, Smith B, O’Sullivan A, Chan M, Patwardhan A et al (2007) Progressive exercise for anabolism in kidney disease (PEAK): a randomized, controlled trial of resistance training during hemodialysis. J Am Soc Nephrol 18(5):1594–1601
DePaul V, Moreland J, Eager T, Clase CM (2002) The effectiveness of aerobic and muscle strength training in patients receiving hemodialysis and EPO: a randomized controlled trial. Am J Kidney Dis 40(6):1219–1229
Headley S, Germain M, Mailloux P, Mulhern J, Ashworth B, Burris J et al (2002) Resistance training improves strength and functional measures in patients with end-stage renal disease. Am J Kidney Dis 40(2):355–364
Kouidi E, Albani M, Natsis K, Megalopoulos A, Gigis P, Guiba-Tziampiri O et al (1998) The effects of exercise training on muscle atrophy in haemodialysis patients. Nephrol Dial Transplant 13(3):685–699
Wu X, Yang L, Wang Y, Wang C, Hu R, Wu Y (2020) Effects of combined aerobic and resistance exercise on renal function in adult patients with chronic kidney disease: a systematic review and meta-analysis. Clin Rehabil 34(7):851–865
Heiwe S, Jacobson SH (2011) Exercise training for adults with chronic kidney disease. Cochrane Database Syst Rev (10):CD003236. https://doi.org/10.1002/14651858.CD003236.pub2
Ibrahim AA, Althomali OW, Hussein HM, Atyia MR, Eldesoky MT, Gamal M, Abdelbasset WK (2021) Physical and psychological response to exercise training in chronic kidney disease patients: a quasi-randomized controlled trial. Med Sci 25(109):547–555
Mustata S, Groeneveld S, Davidson W, Ford G, Kiland K, Manns B (2011) Effects of exercise training on physical impairment, arterial stiffness and health-related quality of life in patients with chronic kidney disease: a pilot study. Int Urol Nephrol 43(4):1133–1141
Perlman RL, Finkelstein FO, Liu L, Roys E, Kiser M, Eisele G et al (2005) Quality of life in chronic kidney disease (CKD): a cross-sectional analysis in the Renal Research Institute-CKD study. Am J Kidney Dis 45(4):658–666
Heiwe S, Jacobson SH (2014) Exercise training in adults with CKD: a systematic review and meta-analysis. Am J Kidney Dis 64(3):383–393
Barcellos FC, Santos IS, Umpierre D, Bohlke M, Hallal PC (2015) Effects of exercise in the whole spectrum of chronic kidney disease: a systematic review. Clin Kidney J 8(6):753–765
Acknowledgements
This research has been funded by Scientific Research Deanship at University of Ha’il—Saudi Arabia, through project number RG-191348.
Funding
University of Ha’il.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ibrahim, A.A., Althomali, O.W., Atyia, M.R. et al. A systematic review of trials investigating the efficacy of exercise training for functional capacity and quality of life in chronic kidney disease patients. Int Urol Nephrol 54, 289–298 (2022). https://doi.org/10.1007/s11255-021-02917-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-021-02917-4