
Abstract
Purpose
To determine the effectiveness of Vacuum-Assisted Closure Device in the postoperative wound care for Fournier's gangrene
Methods
We performed a systematic review in the following databases: Medline (Ovid), EMBASE, and The Cochrane Central Register of Controlled Trials (CENTRAL), from inception to nowadays. We included RCTs and analytical observational studies. Meta-analysis was not possible given the clinical and methodological heterogeneity of the studies.
Results
We included six studies that compared VAC treated patients and a control group. The length of stay of the VAC treated vs. the conventional dressing treated patients was higher for the VAC treated patients in all but one of the included studies. The VAC group had the highest number of surgical debridements requiring anesthesia. The conventionally treated patients had a higher number of daily dressings, and the need for additional dressing changes, without anesthesia. Two studies found significantly higher mean scores for VAS, requiring a higher need for daily analgesics for the control group patients.
Conclusions
VAC therapy is an effective method, but it is not better than conventional dressing treatment. VAC carries fewer dressing changes, less pain, and less need for analgesics, but it comes with a higher need for surgical interventions requiring anesthesia.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Fournier's gangrene (FG) is a rare condition first described in 1883 [1]. It is defined as a necrotizing infection that initially affects the perineal region and rapidly spreads along with the fascial layers to external genitals, perianal, and even abdominal zones. The etiology can be divided into urogenital, anorectal, and cutaneous sources. The most frequently affected patients are diabetic, alcoholic, and immunocompromised male patients [2, 3].
The three main principles accepted for the management of Fournier's Gangrene are initial resuscitation, empirical broad-spectrum antibiotic coverage for Gram-positive, Gram-negative, and anaerobic microorganisms, and early aggressive surgical intervention [3, 4]. To accomplish that, the affected patients need a multidisciplinary management at an intermediate or intensive care unit, from urologists, general surgeons, nutritionists, intensive care specialists, and phycologists. The affected patients might need one or more surgical interventions such as wide excision of dead tissues, urinary or gastrointestinal diversions (colostomy or cystostomy), and reconstructive surgeries. These patients tend to stay for long periods and represent very high costs to health systems [2].
Although Fournier's Gangrene is not a common condition, it still carries a significant morbi-mortality for affected patients [2]. Several options have been proposed in the past: namely honey, hyperbaric oxygenation, grown hormones, growing agents, and vacuum-dressing technologies; however, most of them are not effective for wound closure.
The Vacuum-Assisted Closure System (VAC) is a wound care system that creates a continuous negative pressure at the surgical site [2]. It seals the wounds with a polyurethane foam sponge and an adhesive, connected to a negative pressure pump. It can be repositioned every 48–72 h [1, 2]. This technology has been widely studied for reconstructive purposes: it increases wound vascularization, fibroblast migration, and cell proliferation. These characteristics help for a faster-scaring process, even for complex infected wounds [1, 2]. Following the same mechanism, it also augments the available oxygen, and so it affects the anaerobic bacteria environment, favoring the control of infection [3].
The surgical excision has to be extensive and aggressive for a patient affected by Fournier's Gangrene. Such an extensive wound represents a challenge for nurses, doctors, and finally, surgeons, in charge of the curing interventions and reconstructive surgeries [3]. By increasing the vascular supply and available oxygen, reducing the scaring time, and controlling the infection of even complex wounds, the VAC technology is an efficient and secure therapeutic option for the postoperative wounds of Fournier's Gangrene patients [2]. Some data suggests that the VAC reduces the number of required surgical and curing interventions – for instance, until the granulation tissue is enough for proceeding to the grafting of the wound is ready for a flap coverage-; it also helps with the scaring process after the reconstructive procedure. Besides that, other authors also affirm that the VAC System diminishes the number of analgesics, sedative substances, hospital stay, and, finally, improves the patients' quality of life [2]. That so, our study aims to determine the effectiveness of Vacuum-Assisted Closure Device in the postoperative wound care for Fournier's gangrene.
Methods
We conducted this study according to Cochrane's recommendations and the PRISMA statement.
Eligibility criteria
Study designs
We included analytical observational studies. We could not find any clinical trial.
Participants
Studies including patients with Fournier’s Necrosis who received VAC therapy compared with conventional therapy.
Intervention
Vacuum-Assisted Closure Device.
Comparison
Conventional therapy.
Outcomes
Length of hospital stay, UCI stay duration, mortality, number of surgical debridement and daily dressings, time from initial surgical debridement to wound closure, type of wound closure, costs, pain (analgesic need, Visual Analog Scale).
Timing
None defined.
Search methods
We conducted a search strategy in MEDLINE (OVID), EMBASE, and the Central Cochrane Controlled Trials Register (CENTRAL) from its inception to nowadays (Appendix 1). We saturated information searching in google scholar, thesis databases, registries of clinical trials, and conferences. There was no language restriction.
Collection of data
We examined the references obtained from databases on a title/abstract level and then, if potentially relevant, retrieved as complete articles. After the title/abstract phase, we reviewed the full text of relevant studies for pre-specified inclusion and exclusion criteria. We collected data using a standardized format, which contains the study design, participants, variables, comparisons, and results. The authors confirmed the entry of the data and verified the information for greater accuracy. Disagreements were resolved by consensus.
Risk of bias assessment
We assessed the risk of bias of the included studies through the STROBE statement.
Analysis of the data and synthesis of the results
Meta-analysis was not possible given the clinical and methodological heterogeneity presented in the studies.
Results
Studies selection
We identified 160 studies through the database search. After excluding duplicates, we included six studies in the qualitative analysis (Fig. 1).

Flowchart of included studies
Characteristics of Included studies
We included six studies in the analysis, including a control group and a VAC group [5,6,7,8,9,10](Table 1). These characteristics included: the specific management given to each of the patient groups, the antibiotic regimen, the first debridement intervention timing, the type of dressings and the frequency of changes, and the indications for new surgical interventions (debridement, urinary or intestinal diversions). On the other hand, we addressed the demographics of the included patients of each of the studies in Table 2.
There were no significant differences among groups regarding age in any of the included studies. Most of them had a higher number of men than women, except for one study, which included more women than men [7]. Most of the studies reported a high percentage of diabetic patients. There were no differences in the number of these patients among groups.
Two of the included studies reviewed the mean delay in the initiation of treatment. They reported no differences among groups. One did not report on mortality, while the other reported higher mortality for the control group, even with no differences in treatment [9].
Only one study mentioned the duration of surgery [6]. Also, two studies compared the Fournier Gangrene Severity Index (FGSI) between both groups at admission [9, 10].
Three studies reported anorectal and urogenital as the leading causes, while others reported unclear causes. Two studies reported no significant differences in etiology [5, 6]. Another study reported a higher percentage of anorectal cases [7].
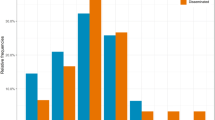
Three studies reported the number of patients with gangrene confined to the perineum (local), and the ones with necrosis extended out of the pelvic region (Disseminated). Only one reported no significant difference in median wound diameter among VAC treated and conventional dressing treated patients [6].
Regarding diversions, only one study reported the need for urinary diversions, which was slightly lower for the control group [8]. Three studies reported an enterostomy need: Ozturk reported no significant differences in both groups [5]. Czymek et al. reported a significantly higher need for an enterostomy in the VAC group [8].
On the other side, two of the included studies reported a polymicrobial infection for most of the included patients [5, 8].
Characteristics of the excluded studies
The articles excluded treated different topics or had a study design that did not accomplish the inclusion criteria.
Outcomes
All of the included studies reported a comparison group. Several different outcomes were analyzed in each of the included studies. Nonetheless, we selected the ones that were most common among studies to review. We described those outcomes in Table 3.
Length of hospital and ICU stay
When comparing the length of stay of the VAC vs. the conventional dressing patients, VAC was significantly longer in two studies [7, 8]. Iacovelli et al. found a longer length of stay for patients with local and disseminated FG in the VAC group. In summary, the VAC group in all had a more extended hospital stay [10].
Only one of the included studies compared the length of stay in the Intensive Care Unit (ICU) for the VAC group vs. the conventional dressing group; they found a significantly longer stay for the VAC group [8].
Number of surgical debridements and changes of dressings
Regarding the number of surgical debridements (the ones requiring anesthesia), the VAC group had the highest number in all the studies. Nonetheless, only two found a significant difference [7, 9].
One of the studies analyzed the number of daily dressings and the need for additional dressing changes without anesthesia. They found a significantly higher for the conventionally treated patients [conventional group 2 (0–3) vs. VAC group 0, and control group 4 (3–5), vs. VAC group 2 (2–3), p < 0.05, respectively] [6].
Mortality
Four studies reported mortality. One of them found no significant difference among groups [6]. Another did not report the difference between groups and only had one death in the intervention group [7]. The other two studies [8, 9] reported significantly higher mortality for the control group. Of notice, most dead patients in the control group of one of these studies died on the third day of hospital stay, while the only dead patient on the VAC group died on the 51st day.
Closing method
Most of the studies reported the closing method. Two of the studies comparing conventional management vs. VAC therapy found no difference among the closing method (tertiary, or graft/flap use) [5, 6]. In contrast, another found that the graft/flap use was significantly higher in the VAC group [8].
Time from initial surgical debridement to wound closure
Only two studies reported on the time from initial surgical debridement to wound closure. Two of them showed no significant difference between the control group and the VAC group [5, 6]. Iacovelli et al. found a median time longer for VAC therapy in local F (p = 0.01) but no difference in both groups for disseminated type (p = 0.671) [10].
Pain
Regarding pain, we found two studies comparing the Visual Analog Scale referred by patients receiving conventional vs. VAC therapy. Both of them found significantly higher mean scores for the patients in the control group. The first described a mean score of 6.8 [6to7] for controls, vs. 2.4 (2 to 3) for VAC treated patients. They also described a higher need for epidural analgesics for the same group [14 times (14–21) vs. four times (4–6)] [5]. The other study found a mean score of 8 (4–10) for controls, vs. 5 (4–10) for VAC treated patients (p < 0.05). The same study also reported a higher need for daily analgesics for control patients four times (3–5) vs. 2 (2–3), p < 0.05 [6].
Other outcomes
Only two studies compared the FGSI in control, and VAC treated patients at 7 and 14 days after the first debridement surgery. They found a significantly lower score in both measures for VAC treated patients [9, 10].
Ozturk 2009 reported a total cost of US$8800 in the control group and US$8850 in the VAC group, finding no differences in both groups. Also, in this study, they described the physician's opinion. They that VAC treatment was more convenient (92%), more comfortable to use (88%), and the preferred method (92%).
On the other side, Yanaral described the length of the surgical operation. They found 55 min (30–110) for the control group and 48 min (30–98) for the VAC group; no differences between groups. Also, they described that there was more frequent daily dressing (2 for the control group and 0.5 for the VAC group)(p < 0.05).
Risk of bias assessment
We found a low risk of bias in most of the items. Nonetheless, Ozturk et al. had an unclear risk of bias regarding the variables description, statistical methods, bias management, sample size, other analysis, and funding. They did not describe information regarding those items. All studies did not show bias management, other analysis, and sample size information (Table 4).
Discussion
Because of the rapid natural progression of Fournier’s Gangrene, early diagnosis and immediate aggressive, multimodality therapy with surgical debridement and broad-spectrum empiric antibiotics are crucial [11, 12]. Some data suggests that the VAC reduces the number of required surgical and curing interventions—for instance, until the granulation tissue is enough for proceeding to the wound's grafting is ready for flap coverage. It also helps with the scaring process after the reconstructive procedure. Besides that, other sources affirm that the VAC System diminishes the number of analgesics, sedative substances, the hospital stay, and at last, it improves the quality of life of the patient [2].
Previous studies report different lengths of hospitalization for patients with Fournier’s Gangrene Disease, which depends on the initial clinical conditions, such as the diameter of lesions and the related complications during treatment, such as sepsis.
The VAC treatment has previously been proposed as an expediting method for wound healing [13, 14]. Tavusbay et al. reported that VAC treated wounds presented considerable shrinking and acceleration in the granulation tissue development and reduced wound secretion [15]. It would then be thought that the length of hospitalization would be shorter for patients receiving this type of treatment [7, 16,17,18]. However, according to our results, the VAC system does not shorten the time from initial debridement to the wound's closing. It instead represents a more extended hospital say when compared to conventional dressing treatment.
One of the most known adverse effects associated with VAC therapy has been painful. However, the pain appears to be related to the wound's nature rather than VAC itself [19]. These patients have a higher need for anesthetic or epidural analgesia and sedation assisted procedures (for VAC system changing), which are nonpainful. Besides that, just as Ozturk et al. [5] reported previously, we found these patients to have a lower need for an in-bed change of dressings—which is a painful procedure-, compared to conventionally treated patients. This finding explains the lower pain scores and the lower need for analgesics in patients with VAC systems. It also allows for more considerable and more comfortable mobilization. It comes with a lower need for skipped meals that can be related to the effects of strong analgesics [5, 6, 17] That so, authors propose a more comfortable treatment option for patients [7].
The mortality rate associated with Fournier’s Gangrene ranges from 3 to 67% and depends on various factors [8, 20]. Of notice, death is not directly related to the local tissue lesions or defects derived from surgery, but to complications associated with the disease, such as sepsis, coagulopathy, acute renal failure, diabetic ketoacidosis, or multi-organ failure [6, 21,22,23,24]. Our study found significantly higher mortality for the patients receiving conventional treatment than VAC treated ones [8]. Nonetheless, other studies showed no differences in mortality rates among the two groups.
One of the main reasons to criticize VAC therapy has been its cost [19]. Some studies affirm that the suction unit is expensive, but it can be used for a long time [5]. Philbeck et al. even determined lower costs when treating VAC patients than conventional methods [25]. Ozturk et al. [5] reported that conventional methods and VAC treatment methods showed equivalent effects in wound healing and represented similar costs. One of the included studies of our review also described almost similar costs for patients receiving conventional and VAC therapy ($8800 and $8850, respectively) [5]. Nevertheless, considering the already mentioned longer hospitalization associated with VAC therapy, one should consider these costs too before considering one option of the other as the most convenient.
The already mentioned findings, along with the effectiveness demonstrated for VAC treatment, may explain why, in some studies, it is proposed as the preferred method by physicians. One of the included studies [5] described the physicians’ opinion on both options – VAC vs. conventional treatment. 50% of the physicians said that the time to change the dressings was the same for both treatments. 92% of them considered that the VAC treatment was the most convenient option, 88% said it was the easiest method to use, and 92% chose it as the preferred method.
Strengths and limitations
Most of the studies measured different outcomes, or the used measurement method was different among them. Given the clinical and methodological heterogeneity presented in the included studies, a meta-analysis was not possible.
Conclusions
According to our results, VAC therapy is an effective method, but it is not better than conventional dressing treatment. Specifically, VAC carries fewer dressing changes, less pain, and less need for analgesics, but it comes with a higher need for surgical interventions requiring anesthesia. Also, VAC therapy does not shorten the time from initial debridement to the closing of the wound. It instead represents a more extended hospital say when compared to conventional dressing treatment.
It may be a valid option, convenient for both patients and treating physicians; however, we need more well-design studies to confirm these findings.
References
Tucci G, Amabile D, Cadeddu F, Milito G (2009) Fournier’s gangrene wound therapy: our experience using VAC device. Langenbeck’s Arch Surg 394(4):759–760
Flores Cortés M, López Bernal F, Valera Sánchez Z, Prendes Sillero E, Pareja CF (2011) Utilización del sistema de presión negativa VAC en la gangrena perineal: Presentación de un caso. Cir Esp 89(10):682–683
Tiong WHC, O’Sullivan B, Ismael T (2009) Managing extensive Fournier’s gangrene secondary to bilateral, inguinal hernias. J Plast Reconstr Aesthetic Surg 62(11):533–535
Atakan IH, Kaplan M, Kaya E, Aktoz T, Inci O (2002) A life-threatening infection: Fournier’s gangrene. Int Urol Nephrol 34(3):387–92. Doi: https://doi.org/10.1023/A:1024427418743. Accessed 26 Oct 2020
Ozturk E, Ozguc H, Yilmazlar T (2009) The use of vacuum assisted closure therapy in the management of Fournier’s gangrene. Am J Surg 197(5):660–665
Yanaral F, Balci C, Ozgor F, Simsek A, Onuk O, Aydin M et al (2017) Comparison of conventional dressings and vacuum-assisted closure in the wound therapy of Fournier’s gangrene. Arch Ital di Urol e Androl 89(3):208–211
Yücel M, Özpek A, Başak F, Kılıç A, Ünal E, Yüksekdağ S et al (2017) Fournier gangreni: 25 hastanın geriye dönük analizi. Ulus Travma ve Acil Cerrahi Derg 23(5):400–404
Czymek R, Schmidt A, Eckmann C, Bouchard R, Wulff B, Laubert T et al (2009) Fournier’s gangrene: vacuum-assisted closure versus conventional dressings. Am J Surg 197(2):168–176
Xu XP, Cai XH, Zhang L, Li XH, Liu ZH, Pan Y et al (2015) Clinical efficacy of vacuumsealing drainage in treatment of fournier’s gangrene. World Chin J Digestol 23:348–352
Iacovelli V, Cipriani C, Sandri M, Filippone R, Ferracci A, Micali S et al (2020) The role of vacuum-assisted closure (VAC) therapy in the management of FOURNIER’S gangrene: a retrospective multi-institutional cohort study. World J Urol. https://doi.org/10.1007/s00345-020-03170-7
Wagner S, Greco F, Hoda MR, Kawan F, Heynemann H, Fornara P (2011) Is intensive multimodality therapy the best treatment for fournier gangrene? Evaluation of clinical outcome and survival rate of 41 patients. Surg Infect (Larchmt) 12(5):379–383
Selvi I, Aykac A, Baran O, Burlukkara S, Ozok U, Sunay MM (2019) A different perspective for morbidity related to Fournier’s gangrene: which scoring system is more reliable to predict requirement of skin graft and flaps in survivors of Fournier’s gangrene? Int Urol Nephrol 51(8):1303–11. Available from: https://springerlink.bibliotecabuap.elogim.com/article/https://doi.org/10.1007/s11255-019-02188-0. Accessed 26 Oct 2020
Morykwas MJ, Argenta LC, Shelton-Brown EI et al (1997) Vacuum-Assisted Closure: a new method for wound control and treatment: animal studies and basic foundation. Ann Plast Surg 38:553–562
Argenta LC, Morykwas MJ (1997) Vacuum-assisted closure: a new method Surg, for wound control and treatment: clinical experience. Ann Plast 38:563–576
Tavusbay C, Kar H, Cin N, Kamer E, Aksut H, Karahalli O et al (2013) The use of vacuum-assisted wound closure system for management of difficult wounds. Biomed Res 24(3):329–336
Morpurgo EGSS (2002) Fournier’s gangrene. Surg Clin North Am 82:1213–1224
Oguz A, Gümüs M, Turkoglu A, Bozdaǧ Z, Ülger BV, Agaçayak E et al (2015) Fournier’s gangrene: a summary of 10 years of clinical experience. Int Surg 100(5):934–941
Cuccia G, Mucciardi G, Morgia G, Stagno D’Alcontres F, Galì A, Cotrufo S et al (2009) Vacuum-assisted closure for the treatment of Fournier’s gangrene. Urol Int 82(4):426–431
Lambert KV, Hayes P, Mc Carthy M (2005) Vacuum Assisted Closure: a review of development and current applications. Eur J Vasc Endovasc Surg 29:21
Ersay A, Yilmaz G, Akgun YCY (2007) Factors affecting mortality of Fournier’s gangrene: review of 70 patients. ANZ J Surg 77(1–2):43
Laor E, Palmer LS, Tolia BM et al (1995) Outcome prediction in patients with Fournier’s gangrene. J Urol 154:89–92
Slater DN, Smith GTMK (1982) Diabetes mellitus with ketoacidosis presenting as Fournier’s gangrene. R Soc Med 75:531–532
Lamb RC, Juler GL (1983) Fournier’s gangrene of the scrotum. A poorly defined syndrome or a misnomer? Arch Surg. 118:38–40
Scott SD, Dawes RFH, Tate JJT et al (1988) The practical management of –20, Fournier’s gangrene. Ann R Coll Surg Engl. 70:16
Philbeck TE Jr, Whittington KT, Millsap MH et al (1999) The clinical and cost effectiveness of externally applied negative pressure wound therapy in the treatment of wounds in home healthcare medicare patients. Ostomy Wound Manag 45:41–50
Funding
None.
Author information
Authors and Affiliations
Contributions
Research conception and design: DF-B, HAG-P. Data acquisition: DF-B, HAG-P. Statistical analysis: DF-B, HAG-P. Data analysis and interpretation: DF-B, HAG-P. Drafting of the manuscript: DF-B, HAG-P. Critical revision of the manuscript: DF-B, HAG-P. Administrative, technical, or material support: DF-B, HAG-P. Approval of the final manuscript: DF-B, HAG-P.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare we had no conflict of interest and no funding.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendices
Appendix 1 Search strategies
Medline through ovid
(Exp Fournier Gangrene or (Gangrene adj2 Fournier*).mp or (Fournier* adj2 disease).mp) AND (exp Negative-Pressure Wound Therapy or (Negative-Pressure Wound Therap*).mp or (Topical Negative-Pressure Therap*).mp or (Negative-Pressure Dressing*).mp or (Vacuum-Assisted Closure*).mp).
Central through ovid
(Exp Fournier Gangrene or (Gangrene adj2 Fournier*).mp or (Fournier* adj2 disease).mp) AND (exp Negative-Pressure Wound Therapy or (Negative-Pressure Wound Therap*).mp or (Topical Negative-Pressure Therap*).mp or (Negative-Pressure Dressing*).mp or (Vacuum-Assisted Closure*).mp).
Embase through scopus
TITLE-ABS-KEY(“Fournier Gangrene” or “Fournier* disease”) AND TITLE-ABS-KEY(“Negative-Pressure Wound Therap*” or “Topical Negative-Pressure Therap*” or “Negative-Pressure Dressing*” or “Vacuum-Assisted Closure*”).
Rights and permissions
About this article

Cite this article
Franco-Buenaventura, D., García-Perdomo, H.A. Vacuum-assisted closure device in the postoperative wound care for Fournier's gangrene: a systematic review. Int Urol Nephrol 53, 641–653 (2021). https://doi.org/10.1007/s11255-020-02705-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-020-02705-6