
Abstract
Objective
To explore and understand the experiences of healthcare professionals (HCPs) delivering care in a multidisciplinary care (MDC) clinic for advanced chronic kidney disease (CKD) patients.
Methods
This is a qualitative study based on semi-quantitative questionnaire and semi-structured interviews with thematic analysis and deductive mapping onto the Theoretical Framework of Acceptability. Sixteen HCPs caring for advanced CKD patients in a MDC clinic in a tertiary teaching hospital in Singapore were recruited based on maximum variation sampling procedures.
Results
The majority of the HCPs were supportive of a MDC clinic. There was a positive overall opinion of the programme [median 7.0 of 10.0 (IQR 7.0–8.0)], high satisfaction ratings for interaction with other members of team [6.9 (5.3–8.0)] and time spent with patients [7.0 (5.3–7.0)]. Thematic analysis of the interviews identified the value of MDC clinic in the provision of one-stop care, the improvement in communication and collaboration between HCPs, the facilitation of patient activation to make planned kidney care decisions, and the optimisation of medications. The main challenges were lack of continuity of care, manpower constraints, poor patient navigation between HCPs, poor patient attendance with allied HCPs, and the perception of increased cost and time spent by patients in each MDC clinic visit. The proposed interventions were notification of patients beforehand of the MDC clinic schedule and provision of navigation to patients within the MDC clinic.
Conclusion
A multidisciplinary care clinic for advanced chronic kidney disease patients was viewed positively by the majority of the healthcare professionals, with areas for improvement.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The prevalence of chronic kidney disease (CKD) is high worldwide, ranging from 11 to 13% [1]. In Singapore, the prevalence of CKD was 15.6% in 2007 [2]. This is projected to increase to 24.3% by 2035 [3]. CKD patients are at risk of progression to end stage kidney disease (ESKD), increased cardiovascular events and mortality [4]. Studies have shown that unplanned initiation of renal replacement therapy (RRT) in ESKD patients was associated with poorer survival and longer hospitalisation [5].
In 2018, 1257 patients were initiated on definitive dialysis in Singapore (age-standardised rate 187.0 per 1,00,000 residential population) [6]. The proportion of ESKD patients in Singapore initiated on emergent RRT with a temporary haemodialysis catheter was high (ranging from 64.9 to 98.8%), and this resulted in poorer survival, longer hospitalisations, and more frequent hospital admissions [7,8,9].
Multiple studies on multidisciplinary care (MDC) for advanced CKD patients have reported that MDC clinics improved mortality and hospitalisation rates, slowed renal function decline, reduced the need for temporary catheterisation for dialysis, and reduced healthcare costs [10,11,12,13,14]. The 2012 Kidney Disease Improving Global Outcomes (KDIGO) CKD guideline recommends that people with progressive CKD should be managed in a MDC setting and the multidisciplinary team should include or have access to dietary counselling, education and counselling about renal replacement therapy modalities, transplant options, vascular access surgery, and ethical, psychological, and social care [15]. The primary goals of MDC clinics are to improve morbidity and mortality for CKD patients, and to establish patient-centred goals of care.
Understanding the experiences and perceptions of HCPs in a MDC clinic would help inform the refinement and implementation of similar programmes across different countries and regions. This study aims to understand and explore the experiences of HCPs delivering care to advanced CKD patients within this MDC setting.
Methods
Design
This was a qualitative analysis of interviews with HCPs involved in a MDC clinic for advanced CKD patients. All participants provided written consent to participate in the study and for interviews to be audio-recorded.
Setting
The setting was a MDC clinic for adult advanced CKD patients with estimated glomerular filtration rate (eGFR) between 10 and 20 ml/min/1.73 m2 seen in Singapore General Hospital (SGH), a major tertiary hospital in Singapore serving a culturally and ethnically heterogeneous population. In 2019, the Department of Renal Medicine in SGH had managed more than 15,000 patients with 349 new ESKD patients initiated on RRT. A MDC clinic for advanced CKD patients (called Low Clearance Clinic) was set up in SGH in August 2015 and comprised renal physicians, palliative care physicians, nurse clinicians, medical social workers, renal coordinators, transplant coordinators, pharmacists, and dieticians. Advanced CKD patients could be referred by their primary renal physicians to the MDC clinic. The patients’ issues were discussed by the MDC team in weekly multidisciplinary meetings. In the MDC clinic, patients were reviewed by the renal physician at every visit and by the other healthcare professionals (HCPs) on an ‘as-needed’ basis as determined by the MDC team. The palliative care physician alternated with the renal physician to review the patients who chose palliative care. The team also worked in close collaboration with the renal transplant team, vascular surgeons, community patient advocates, and hospices to facilitate care based on patients’ preferred kidney care plan. At the time of the study, the MDC clinic had only been introduced for a subset of advanced CKD patients, but was not routinely implemented for all advanced CKD patients in the hospital.
Participants
The inclusion criteria were: (1) being a HCP, and (2) having experience of working in the MDC clinic. Maximum variation sampling procedures were adopted. Participants were recruited by taking into account profession and working experience so as to ensure representation from all the components of the MDC team. The study sample included renal physicians (consultants and senior residents), palliative care physicians (consultants), nurse clinicians, dieticians, pharmacists, medical social workers, renal coordinators, transplant coordinators and clinic assistants.
Eligible participants were approached by email or face-to-face, and were briefed on the purpose of the study. Written informed consent was obtained from each participant prior to the interview.
Data collection
Qualitative data were gathered through semi-structured interviews and a semi-quantitative questionnaire with HCPs working in the MDC clinic. The participants were interviewed in a confidential setting at their workplace (outside of clinical duties) by a research coordinator (NK, BSc), who remained independent to any health provision services and was not related to nor worked with study participants. The interviewer had prior training in qualitative methodology and was supervised by KG (MSC, PhD), an experienced qualitative researcher. Duration of the interviews ranged from 6 min 15 s to 15 min 26 s.
The interview guide consisted of open-ended questions that explored perceptions, experiences and views on the existing multidisciplinary kidney care pathways for CKD, facilitators and barriers for an effective MDC clinic, and recommendations for refinement of the programme. Questions and prompts were refined iteratively in response to the initial interviews (n = 3(19%)). The final interview guide is shown in Table 1. No repeat interviews were carried out. All interviews were digitally audio-recorded using a handheld recorder (Sony ICD-PX470), stored in MP3 format, and transcribed verbatim. No additional field notes were made. The transcripts were not returned to participants for comment or correction. Feedback on the findings of the study was not sought from the participants. The data were anonymised with code numbers allocated to each participant. The data were stored in Microsoft Word and Microsoft Excel files. Interviews were conducted until thematic saturation was reached, i.e. no new themes in two consecutive interviews.
The structured semi-quantitative questionnaire included questions on their professional role, the impact of LCC on various aspects of their patient care service, and satisfaction level with LCC. These items were rated on a 11-point Likert scale ranging from 0 to 10. On programme impact on HCP and opinion of the programme, 0 represented very negative and 10 represented very positive. On time spent and workload, 0 represented less and 10 represented more. On care provision, 0 represented worse and 10 represented better. On satisfaction level, 0 represented not at all satisfied and 10 represented very satisfied.
Data analysis
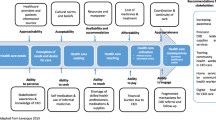
All interviews were recorded, fully transcribed, with the transcript checked against the recording. Thematic analysis that utilised six related steps of: familiarisation, coding, theme development, reviewing themes, defining themes and reporting, was applied [16]. Initial codes and themes identified inductively from the data were then organised into a framework of overarching or higher order themes by two coders (KG, LL). Specialised software was not used. The following strategies were employed to ensure that the analysis was credible and trustworthy: 1. coding was checked and iteratively refined using paired analysis of transcripts by two researchers (LL and KG), and 2. researcher reflexivity was supported by discussing emerging findings at regular meetings with the research group where themes (including illustrative quotes) and overarching framework were reviewed and refined. After inductive coding, the final codes were deductively mapped onto the Theoretical Framework of Acceptability (REF) for the discussion [17]. This framework outlined the 7 key parameters related to acceptability of health interventions based on review of multiple trials. These included affective attitude, perceived effectiveness, intervention coherence, ethicality, burden, self-efficacy, and opportunity costs. The inductive codes were assigned to framework domains by two study team members (KG and KJL)
We followed the recommendations outlined in the Consolidated Criteria for Reporting Qualitative Research (COREQ) to report study findings [18].
Descriptive statistics [median (IQR), frequencies (%)] were used to summate responses on the structured semi-quantitative questionnaire.
Results
Sixteen HCPs were identified and invited for the study. All 16 agreed to participate, gave informed consent and completed the questionnaire and interview (100% response rate). The sample represented the whole spectrum of HCPs in the MDC clinic at the time of this study and included renal physicians [n = 4 (25%)], palliative care physician [1 (6.3)], nurse clinician [1 (6.3)], renal coordinators [2 (13)], transplant coordinator [1 (6.3)], medical social workers [2 (13)], pharmacists [2 (13)], dieticians [2 (13)] and clinic assistant [1 (6.3)]. Majority [13 (81)] of the participants were female.
Descriptive analyses (median (IQR)) of the semi-quantitative questionnaire indicated that HCPs had a positive overall opinion of the MDC clinic [7.0 of 10.0 (7.0–8.0)], high satisfaction ratings for interaction with other members of the MDC team [6.9 (5.3–8.0)], and time spent with patients [7.0 (5.3–7.0)]. However, they were neutral about improved patient treatment adherence in the MDC clinic compared to usual care [5.5 (5.0–7.0)] (Table 2).
Thematic analysis identified 11 themes that were organised into 3 super-ordinate themes (Table 3): value of MDC clinic; challenges to the implementation and running of the MDC clinic; proposed interventions to overcome the challenges in the implementation of the MDC clinic.
Theme 1: value of multidisciplinary care clinic
The participants readily recognised the multidimensional nature of CKD treatment and patient needs, and thus the importance of adopting a multidisciplinary approach in the provision of healthcare services for CKD patients. They all viewed MDC as adding value to patients who were at the receiving end of care as well as the team of HCPs providing care.
Provision of one-stop care
The structure of the MDC clinic was uniformly seen as one-stop care that led to provision of comprehensive, holistic, coordinated and consolidated care for CKD patients. Participants discussed patients’ convenience as MDC obviated the need for multiple clinic visits and reduced time-burden of care.
Improvement in communication and collaboration between healthcare professionals
The structure of the MDC clinic enabled HCPs to collaborate more closely with one another resulting in more effective communication among HCPs in the team. As a result, HCPs felt better equipped to provide individualised treatment and care. The opportunity to consult with the other members of the team, especially during the multidisciplinary team meetings, was especially beneficial in guiding patient care plans. Resolving discrepancies and collectively agreeing on treatment approaches made work easier and fostered a sense of camaraderie in the team.
Facilitation of patient activation to make planned kidney care decisions
Some opined that MDC facilitated patients’ decision-making related to their long-term kidney care plan. Better patient activation was linked to information consolidation and reinforcement of treatment plans by the various HCPs in the team.
Optimisation of medications
Others commented that the MDC approach made optimisation of medications easier.
Theme 2: challenges to the implementation and running of the multidisciplinary care clinic
Despite all participants voicing positive feedback, they also highlighted some challenges. These were mainly due to logistical disruption related to setting up the new service, and the perception of increased cost and time spent by patients during each MDC clinic visit.
Lack of continuity of care
Participants suggested lack of continuity of care in the MDC clinic had created challenges in patient care. This was related to the rotating assignment of HCPs to the clinic due to manpower and scheduling constraints. Physician participants highlighted the challenges of having to take over the care of patients from their primary referring renal physicians, and to trust that appropriate judgments were made by the previous physician. As the patients were not always seen by the same physician across visits, some also highlighted the limitations in monitoring patient outcomes and building rapport.
Manpower constraints
Differing views regarding HCPs’ workload were expressed. Some reported comparable workload, while others reported increased workload in relation to documentation needs. As a result of the concern of increased workload, some were hesitant to fully endorse expansion of the MDC clinic with current manpower constraints.
Poor patient navigation between healthcare professionals
Participants commented that the navigation of patients between HCP groups within the MDC clinic was challenging. HCPs themselves had to signpost and guide patients to the other healthcare providers. Patients’ unfamiliarity with the new process and apprehension to consult with allied HCPs made coordination and flow across the MDC team challenging.
Poor patient attendance with allied healthcare professionals
Participants highlighted that some patients did not see the necessity of attending their appointments with some allied HCPs.
Perception of increased cost and time spent by patients during each MDC clinic visit
Participants expressed conflicting views in relation to costs and time spent by patients. Even though time was saved when the patients were able to consult different HCPs in a single MDC clinic compared to having different appointment dates for different HCPs, participants noticed that it was more time-intensive at each MDC appointment. They commented that some patients did not agree to consult some of the HCPs because of concerns about a longer visit duration. Some also brought up concerns about patients’ perception of increased financial costs in MDC clinic.
Theme 3: proposed interventions to overcome the challenges in the implementation of the multidisciplinary care clinic
Participants made the following suggestions to overcome some of the challenges discussed above.
Notification of patients beforehand of the MDC clinic schedule
As the MDC approach was novel and many patients were unprepared for the longer clinic visit duration arising from the need to see different HCP groups, the main suggestion for improvement was related to providing prior explanation and pre-empting patients on the clinic schedule.
Provision of navigation to patients within MDC clinic
Better navigation to patients during clinic sessions to ensure better patient flow between members of the MDC team with reasonable waiting times was also highlighted.
Theoretical framework of acceptability
We further mapped our study findings on the 7 component constructs of the theoretical framework of acceptability. Taken together, the programme was shown to have good acceptability. The identified themes were linked to the components of affective attitude, ethicality, perceived effectiveness, intervention coherence and burden (Table 4). The participants’ ‘affective attitudes’ were generally positive as they were supportive of the MDC clinic from the outset and as the programme was rolled out. They discussed its value for patients and providers, detailing how this model of care provided convenience and improved collaboration between HCPs. Their accounts also echoed its ‘ethicality’ as the programme was aligned with the value of holistic care. Its ‘perceived effectiveness’ was evident mainly in terms of facilitation of patient decision-making and optimisation of medications, yet on the other hand, from the results of the questionnaire, participants were unsure if the MDC clinic would result in patients being more compliant to their management compared to usual care. Their accounts on ‘intervention coherence’ suggest that while the movement of patients between the HCPs was clear to the providers, this might not be the case for patients, which might have contributed to them missing out seeing some of the designated HCPs. This was seen as a remediable issue by including pre-clinic notification for patients to prepare them for the clinic flow and navigation services that could support the running of the clinic. The main ‘burden’ of the MDC clinic was increased workload and manpower constraints and this resulted in some hesitation in recommending the MDC clinic concept to their colleagues. The other 2 components (self-efficacy and opportunity costs) were not explored in this study.
Discussion
This study has provided insights to the understanding of HCPs’ perceptions on acceptability, value and challenges of MDC for advanced CKD patients. The majority of the participants were supportive of the MDC clinic. This echoes a previous mailed survey study among Canadian renal physicians in which the majority of the physicians strongly agreed that MDC was superior compared to care provided by a renal physician alone [19]. This study highlights the support of MDC from HCPs and its value in enhancing the work of HCPs to support advanced CKD patients in their journey, albeit with the burden of increased workload and unfamiliar work processes. It gives strength to the argument that MDC may be the preferred model of care among HCPs if the challenges can be overcome.
The participants perceived care in the MDC clinic as convenient and comprehensive for advanced CKD patients and as being valuable in facilitating kidney care planning. A Belgian study on professionals’ perceptions of integrated palliative care in chronic heart failure and chronic obstructive pulmonary disease reported a similar holistic approach in facilitating integrated care [20]. Another value of the MDC clinic highlighted by participants was an improvement in communication among healthcare groups. Communication among HCPs is crucial in the management of complex advanced CKD patients and the MDC clinic provides an avenue for the healthcare groups to communicate with one another efficiently. A Netherlands study on diabetes care also reported similar perceptions of multidisciplinary collaboration, direct communication lines, and short physical distances to other professionals as care facilitators [21].
Despite the HCPs’ support of the programme, challenges remained. Manpower adequacy was one concern, similar to the concern in another MDC qualitative study [22]. This finding contributed to a review of our MDC clinic processes to trim down its time demands. Another concern was lack of continuity of care. This arose mainly from the initial framework of referral to the MDC clinic, where patients would be referred by their primary renal physicians to be followed up by a few renal physicians assigned to run the MDC clinic. Following the findings of this study, our MDC clinic was subsequently expanded to involve all the renal physicians within the hospital, to allow patients’ usual renal physician to continue care for them with the support of the MDC team. To address the concern of poor patient attendance with allied healthcare and poor navigation during the session, the MDC team modified the clinic workflow such that the first HCP reviewing the patients on that visit day would inform the patients of their scheduled reviews with subsequent HCPs and their room locations for that visit.
There were several limitations in our study. This study was conducted in one of the hospitals in Singapore. It was unclear if variations of healthcare practices in other hospitals in Singapore or in other regions had an influence on the perceptions of healthcare providers practising elsewhere. There was no validated satisfaction questionnaire for healthcare professionals that was deemed suitable, hence items in the semi-quantitative questionnaire were developed solely for this study. Even though we had included representatives from all the healthcare groups and conducted interviews until thematic saturation was achieved, it was still possible that some perceptions about the MDC clinic might not have been described. There were changes to the work processes of the MDC clinic after this study which would not be accounted for by this study and might change the participants’ perception of this MDC clinic.
Further research is needed on the patients’ perceptions and patient-reported outcomes of the MDC clinic, the comparison of efficiencies of different MDC clinic compositions and structures, and the cost-effectiveness of a MDC clinic in the different healthcare systems.
In conclusion, the MDC clinic was viewed positively by the majority of the participating HCPs, with identification of potential areas for further improvement and proposed interventions to increase acceptability among HCPs and improve patient care.
References
Hill NR, Fatoba ST, Oke JL, Hirst JA, O’Callaghan CA, Lasserson DS, Hobbs FD (2016) Global prevalence of chronic kidney disease: a systematic review and meta-analysis. PLoS ONE 11(7):e0158765
Sabanayagam C, Lim SC, Wong TY, Lee J, Shankar A, Tai ES (2010) Ethnic disparities in prevalence and impact of risk factors of chronic kidney disease. Nephrol Dial Transpl 25(8):2564–2570
Wong LY, Liew AST, Weng WT, Lim CK, Vathsala A, Toh MPHS (2018) Projecting the Burden of Chronic Kidney Disease in a Developed Country and Its Implications on Public Health. Int J Nephrol 4(2018):5196285
Keith DS, Nichols GA, Gullion CM, Brown JB, Smith DH (2004) Longitudinal follow-up and outcomes among a population with chronic kidney disease in a large managed care organization. Arch Intern Med 164(6):659–663
Metcalfe W, Khan IH, Prescott GJ, Simpson K, MacLeod AM (2000) Can we improve early mortality in patients receiving renal replacement therapy? Kidney Int 57(6):2539–2545
Singapore Renal Registry Annual Report (2018). Ministry of Health Singapore National Registry of Diseases Office. https://www.nrdo.gov.sg/publications/kidney-failure. Accessed 18 June 2020
Teo BW, Ma V, Xu H, Li J, Lee EJ (2010) Nephrology Clinical Research Group. Profile of hospitalisation and death in the first year after diagnosis of end-stage renal disease in a multi-ethnic Asian population. Ann Acad Med Singapore 39(2):79–87
Roy D, Chowdhury AR, Pande S, Kam JW (2017) Evaluation of unplanned dialysis as a predictor of mortality in elderly dialysis patients: a retrospective data analysis. BMC Nephrol 18(1):364
Yap HY, Pang SC, Tan CS, Tan YL, Goh N, Achudan S, Lee KG, Tan RY, Choong LH, Chong TT (2018) Catheter-related complications and survival among incident hemodialysis patients in Singapore. J Vasc Access 19(6):602–608
Wei SY, Chang YY, Mau LW, Lin MY, Chiu HC, Tsai JC, Huang CJ, Chen HC, Hwang SJ (2010) Chronic kidney disease care program improves quality of pre-end-stage renal disease care and reduces medical costs. Nephrology 15:108–115
Curtis BM, Ravani P, Malberti F, Kennett F, Taylor PA, Djurdjev O, Levin A (2005) The short- and long-term impact of multidisciplinary clinics in addition to standard nephrology care on patient outcomes. Nephrol Dial Transpl 20:147–154
Chen PM, Lai TS, Chen PY, Lai CF, Yang SY, Wu V, Chiang CK, Kao TW, Huang JW, Chiang WC, Lin SL, Hung KY, Chen YM, Chu TS, Wu MS, Wu KD, Tsai TJ (2015) Multidisciplinary care program for advanced chronic kidney disease: reduces renal replacement and medical costs. Am J Med 128:68–76
Wang SM, Hsiao LC, Ting IW, Yu TM, Liang CC, Kuo HL, Chang CT, Liu JH, Chou CY, Huang CC (2015) Multidisciplinary care in patients with chronic kidney disease: a systematic review and meta-analysis. Eur J Intern Med 26(8):640–645
Shi Y, Xiong J, Chen Y, Deng J, Peng H, Zhao J, He J (2018) The effectiveness of multidisciplinary care models for patients with chronic kidney disease: a systematic review and meta-analysis. Int Urol Nephrol 50(2):301–312
Kdigo C (2013) Chapter 5: referral to specialists and models of care. Kidney Int Suppl 3(1):112–119. https://doi.org/10.1038/kisup.2012.68
Braun V, Clarke V (2006) Using thematic analysis in psychology. Qual Res Psychol 3:77–101
Sekhon M, Cartwright M, Francis JJ (2017) Acceptability of healthcare interventions: an overview of reviews and development of a theoretical framework. BMC Health Services Res 17(1):88
Tong A, Sainsbury P, Craig J (2007) Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care 19:349–357
Mendelssohn DC, Toffelmire EB, Levin A (2006) Attitudes of Canadian Nephrologists Toward Multidisciplinary Team-Based CKD Clinic Care. Am J Kidney Dis 47(2):277–284
Sioutal N, Clement P, Aertgeerts B, Beek K, Menten J (2018) Professionals’ perceptions and current practices of integrated palliative care in chronic heart failure and chronic obstructive pulmonary disease: a qualitative study in Belgium. BMC Palliative Care 17:103
Raaijmaker LG, Hamers FJ, Martens MK, Bagchus C, de Vries NK, Kremers SP (2013) Perceived facilitators and barriers in diabetes care: a qualitative study among health care professionals in the Netherlands. BMC Family Pract 14:114
Hofstede SN, Marang-van de Mheen PJ, Wentink MM, Stiggelbout AM, Vleggeert-Lankamp CL, Vliet Vlieland TP, van Bodegom-Vos L (2013) Barriers and facilitators to implement shared decision making in multidisciplinary sciatica care: a qualitative study. Implement Sci 8:95
Acknowledgements
The authors would like to acknowledge the Singapore General Hospital Low Clearance Clinic team and the Health Service Research Unit for their assistance and support in this study. This work was supported by Singhealth Foundation Research Grant 2016 (SHF/HSRHO006/2016).
Funding
This work was supported by Singhealth Foundation Research Grant 2016 (SHF/HSRHO006/2016).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by JLK, NK, LYL and KG. The first draft of the manuscript was written by JLK and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that they have no conflict of interest.
Ethics approval
The research was approved by the Singhealth Centralised Institutional Review Board (CIRB) (reference number 2016/2921).
Informed consent
All participants provided written consent to participate in the study and for interviews to be audio-recorded.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kwek, J.L., Griva, K., Kaur, N. et al. Healthcare professionals’ perceptions of the role of a multidisciplinary approach in improving the care of patients with advanced chronic kidney disease. Int Urol Nephrol 52, 2357–2365 (2020). https://doi.org/10.1007/s11255-020-02571-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-020-02571-2