
Abstract
Introduction and objective
Renal colic is one of the most intense pains known to humans. Standard treatment usually consists of nonsteroidal anti-inflammatory drugs and opiates, but they do not always provide optimum efficacy and speed in relieving the pain. For more than 25 years, our hospital has been employing twelfth subcostal nerve block. The objective of the present study was to compare the efficacy of subcostal nerve block with lidocaine versus intramuscular diclofenac in renal colic management.
Methods
Sixty patients of both sexes, above the age of 18 years, and presenting with renal colic were randomly selected for the study. The visual analog scale was applied prior to the treatment and at minutes 1, 3, 5, 30, and 45 after the application of the twelfth nerve block or the intramuscular administration of diclofenac.
Results
A total of 60 patients, 35 women and 25 men, were included in the study. There were statistically significant differences in the mean scores for pain from minute 1 to minute 45. There were no adverse effects.
Conclusions
Twelfth Subcostal nerve block with lidocaine is an efficacious, safe, inexpensive, and very fast-acting medication for pain control related to renal colic. These characteristics make it superior to diclofenac.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Reno-ureteral colic causes one of the most intense pains that a human being can experience and is one of the main reasons for admission to the emergency room. In many cases, the pain is difficult to control and hospitalization for immediate surgical treatment is required [1, 2].
Reno-ureteral colic is generally caused by an obstruction of the renal pelvis or of the ureter by a calculus, with a consequent spasm around the calculus causing distention of the pelvis, renal capsule, and ureter [3,4,5]. The pain is intense, incapacitating, of sudden onset, and localized to the costovertebral angle below the twelfth rib. The radiation of the pain is variable and depends on the site of the obstruction; it may occur on the flank, the inguinal region, the testicles, or the labia majora. If the calculus is located in the ureterovesical junction, it is often associated with symptoms such as dysuria, frequency, vesical tenesmus, and mictional urgency. The most commonly associated gastrointestinal symptoms are nausea and vomiting [6].
According to the evidence-based guidelines of the European Association of Urology (EAU), the standard treatment for reno-ureteral colic is administration of nonsteroidal anti-inflammatory drugs such as diclofenac [7] and indomethacin or opioids such as hydromorphone or pentazocine. However, when resolution of pain is not achieved, surgical management is indicated [8]. Although the analgesic efficacy of these drugs is recognized, on many occasions the effects are slow, and in clinical practice, more rapid action is always desired due to the severity of the pain in this urological emergency [9, 10].
For more than 25 years in our institution, twelfth intercostal nerve block using lidocaine has been performed for the management of reno-ureteral colic. In 1993, Garduño et al. [11] conducted a study that included 240 patients with reno-ureteral colic who were treated with twelfth intercostal nerve block using 2% plain lidocaine; remission of the neurovegetative symptoms was observed in all cases. Aragon, Reyes [12] conducted a similar study of 51 patients; in 90.1% of those patients, the pain was resolved with an average resolution time of 81.6 s and a mean time of analgesia of 7.4 h. However, both of these studies have methodological deficiencies in design in that neither a control group nor random allocation was used.
Due to its demonstrated safety and efficacy, thoracic paravertebral block of the twelfth nerve has been used successfully, even in pregnant patients [13].
The objective of the present study was to compare the efficacy of twelfth intercostal nerve block using 2% lidocaine versus intramuscular diclofenac for the treatment of reno-ureteral colic.
Materials and methods
An open, randomized, longitudinal, comparative, experimental clinical study was conducted in which patients of both sexes who were over 18 years of age and less than 65 years of age who presented with reno-ureteral colic as confirmed by imaging of the calculus by abdominal radiography or by plain tomography were included. Patients with an allergy to lidocaine or to nonsteroidal anti-inflammatory drugs (NSAIDs), as well as those who had a history of urinary lithiasis, who had undergone prior therapy for reno-ureteral colic, who were carriers of a double-J catheter, who might be suffering from chronic renal insufficiency, or who were pregnant, were excluded.
Based upon the formula for independent means, assuming a power of 80% and a significance level of 0.05, we required a sample size of 30 patients per treatment group [14].
Having established the diagnosis of reno-ureteral colic and having determined that the patient met the criteria to enter the protocol, the characteristics of the study were explained to the patient and to his or her responsible family member.
The ethics committee of our hospital considered that due to the severity of the pain and the conditions under which patients typically present with this pathology, informed consent to participation in the study should also be given by the responsible family member. For this reason, a responsible family member of each patient selected for the study gave written informed consent to the patient’s participation in the study according to the principles of the Declaration of Helsinki. The research protocol for this study was approved by the research committee of our institution (registration number DI/14/105/04/047), and it was found to adhere to the rules of good clinical practice.
The information on each patient was captured in a case report file in which the personal and demographic data of the patient, the patient’s complete clinical history, and the results of his or her physical examination, as well as the results of the laboratory analysis, the images from radiological studies, and the results of the visual analog scale (VAS) for pain measurement were collected.
Patients were admitted consecutively and were randomly assigned to one of the two groups according to a random number table.
Group I
Twelfth intercostal nerve block with 10 cc of 2% lidocaine using the following anatomical references and alignments:
The patient is placed in lateral decubitus position opposite the site of the injection and reclines on a bundle of cloth rolled to the subcostal level to improve the exposure of the tip of the twelfth rib; the ipsilateral arm is positioned with cephalic extension.
The painful point is located by palpating the tip of the twelfth rib. Antisepsis of the area in which the puncture is to be made is performed with povidone-iodine. The needle is inserted at the level of the tip of the twelfth rib in a retroperitoneal direction, previously suctioning to infiltrate 10 mL of 2% lidocaine [11, 12] (Fig. 1).

Sketch of the twelfth intercostal nerve block technique performed at the General Hospital of Mexico
Group II
-
Diclofenac, 75 mg intramuscular single dose.
The intensity of the pain was measured using the visual analog scale (VAS) prior to the administration of the assigned treatment and at 3, 5, 30, and 45 min.
Statistical analysis
Data are presented as the mean ± standard deviation (SD) or in percentages. Exploratory univariate analysis, analysis of normality, and a paired Student’s t test were performed to compare the means of continuous quantitative variables; the Chi-squared test was performed for qualitative variables. A p value <0.05 was taken to indicate statistical significance for all tests. SPSS® version 20 for Windows® statistical software was used (SPSS®, Chicago, IL, USA).
Results
After providing written informed consent, a total of 60 patients (35 females and 25 males) who were diagnosed with reno-ureteral colic were included in the study. The patients were randomly distributed between the two groups; there were 31 patients in the twelfth intercostal nerve block group and 29 patients in the diclofenac group.
Table 1 shows the demographic characteristics of the study population. There were no statistically significant differences between the groups with respect to age, sex, weight, height, or size or laterality of the calculus.
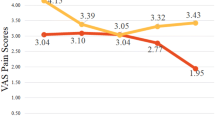
On performing a paired Student’s t test, it was observed that there were statistically significant differences in the VAS from minute 1 through minute 45 (Table 2; Fig. 2).

Comparison of averages of pain index by group
Discussion
Reno-ureteral colic is a medical emergency that must be diagnosed and treated quickly. It is estimated that the probability of presenting reno-ureteral colic at some point in life ranges from 1 to 10% and that the recurrence rate can be as high as 50% [15].
The objective of the treatment is to alleviate the pain and to preserve renal function by ureteral disobstruction. Although in some countries narcotics have traditionally been used to alleviate acute pain related to reno-ureteral colic, more recently the use of NSAIDs has increased significantly [16,17,18,19]. On some occasions, narcotics are still required as a therapy of last resort; however, the latter have undesirable side effects such as somnolence, nausea, vomiting, diaphoresis, and hypotension [20].
Diagnostic and therapeutic use of the thoracic paravertebral block dates from the beginning of the twentieth century [21]; its use for the management of renal colic has been reported in the Soviet medical literature for several decades [22, 23].
There are several reports of the successful management of nephritic colic that is refractory to conventional analgesics using subcutaneous application of lidocaine at the painful point [24]. To date, the exact mechanism of action of infiltration after subcutaneous administration of anesthetic is unknown.
The sensory innervation of the kidney and ureter is provided by nerve fibers of the renal plexus, the testicular (ovarian) plexus, and the hypogastric plexus. The afferent fibers of these nerves enter the spinal cord between T10 and L2. In theory, the blockade of this neurological pathway with lidocaine explains the therapeutic efficacy of this treatment.
Iguchi et al. compared the results of intracutaneous injection of lidocaine into the painful point with those of intravenous administration of butyl scopolamine. They found lower scores on the visual analog scale (VAS) in patients managed with local infiltration in the first thirty minutes and concluded that this technique is simple, safe, and effective for the management of renal colic. However, the process of random allocation used in that study was not specified, nor was how the sample size was calculated or whether an intention-to-treat analysis was performed [14].
Other less commonly used therapies include intranasal fentanyl [25], tamsulosin [26], desmopressin [27, 28], combination of propofol and ketamine [29], and transcutaneous electrical nerve stimulation (TENS) [30]
Lee et al. [31] reported the efficacy of acupuncture in the management of this urological emergency; those results support endogenous opioid release in the central nervous system and spinal cord as a therapeutic mechanism.
Anesthetic infiltration into the “painful point” is often used in cases of myofascial pain syndrome and chronic visceral pain, with effective and immediate results [32, 33]. The “painful points” (trigger points) are small circumscribed areas on the surface of the body that present focal hyperirritability, thereby inducing referred pain from the affected area, and these points have been described in various parts of the body [34]. In the case of reno-ureteral colic, referred pain usually manifests in the ipsilateral lumbar region, specifically at the tip of the twelfth rib.
In this study, infiltration of 2% lidocaine was used for the twelfth intercostal nerve block and compared to the effects of intramuscular diclofenac. Nerve block was found to be a fast, effective, and safe treatment. Furthermore, this technique is simple and easily reproducible; in our hospital, it has been performed for several years by residents in other specialties including medical–surgical emergencies, general surgery, and internal medicine.
A strength of this study is that a direct comparison (face-to-face) was made between the twelfth intercostal nerve block patients and the diclofenac patients. Diclofenac is recommended in the European guidelines for the management of renal colic. However, a weakness of the study is that due to the characteristics of the route of administration of the drugs, blinding was not possible.
Conclusions
Twelfth intercostal nerve block with 2% lidocaine is an effective, safe, and fast-acting pain control treatment for reno-ureteral colic. In this study, it was demonstrated to be significantly superior to intramuscular diclofenac.
References
Esquena S, Millan Rodriguez F, Sanchez-Martin FM, Rousaud Baron F, Marchant F, Villavicencio Mavrich H (2006) Renal colic: revision of literature and scientific evidence. Actas Urol Esp 30(3):268–280
Leveridge M, D’Arcy FT, O’Kane D, Ischia JJ, Webb DR, Bolton DM et al (2016) Renal colic: current protocols for emergency presentations. Eur J Emerg Med 23(1):2–7
Shokeir AA (2002) Renal colic: new concepts related to pathophysiology, diagnosis and treatment. Curr Opin Urol 12(4):263–269
Pedersen KV, Drewes AM, Frimodt-Moller PC, Osther PJ (2010) Visceral pain originating from the upper urinary tract. Urol Res 38(5):345–355
Burnstock G (2009) Purinergic mechanosensory transduction and visceral pain. Mol Pain 5:69
Bultitude M, Rees J (2012) Management of renal colic. BMJ 345:e5499
Knoedler JJ, Lieske JC (2016) Non-steroidal anti-inflammatory drugs for renal colic. Lancet 387(10032):1971–1972
Türk C, Petřík A, Sarica K, Seitz C, Skolarikos A, Straub M, Knoll T (2012) EAU guidelines on diagnosis and conservative management of urolithiasis. Eur Urol 69(3):468–474
Davenport K, Timoney AG, Keeley FX (2005) Conventional and alternative methods for providing analgesia in renal colic. BJU Int 95(3):297–300
Sivrikaya A, Celik OF, Sivrikaya N, Ozgur GK (2003) The effect of diclofenac sodium and papaverine on isolated human ureteric smooth muscle. Int Urol Nephrol 35(4):479–483
Garduño AL, García IC, González RR (1993) Bloqueo del duodécimonervio intercostal como tratamiento del cólico renoureteral. Rev Mex Urol. 53(4):74–79
Aragon TA, Reyes VF, Herrera G, Manjarrez EG, Gutierrez PC (1994) Eficacia del bloqueo subcostal como tratamiento del cólico nefritico. Rev Mex Urol. 54(5):91–98
Nikiforov S, Cronin AJ, Murray WB, Hall VE (2001) Subcutaneous paravertebral block for renal colic. Anesthesiology 94(3):531–532
Iguchi M, Katoh Y, Koike H, Hayashi T, Nakamura M (2002) Randomized trial of trigger point injection for renal colic. Int J Urol 9(9):475–479
Shokeir AA (2001) Renal colic: pathophysiology, diagnosis and treatment. Eur Urol 39(3):241–249
Afshar K, Jafari S, Marks AJ, Eftekhari A, MacNeily AE (2015) Nonsteroidal anti-inflammatory drugs (NSAIDs) and non-opioids for acute renal colic. Cochrane Database Syst Rev 2015(6):CD006027
Pathan SA, Mitra B, Straney LD, Afzal MS, Anjum S, Shukla D et al (2016) Delivering safe and effective analgesia for management of renal colic in the emergency department: a double-blind, multigroup, randomised controlled trial. Lancet 387(10032):1999–2007
KandaSwamy GV, Dhanasekaran AK, Elangovan A, John B, Viswaroop B, Vedanayagam KS (2015) Randomized double blinded placebo controlled trial comparing diclofenac and piroxicam in management of acute renal colic and its clinical implications. Urol J 12(2):2069–2073
Kaynar M, Koyuncu F, Buldu I, Tekinarslan E, Tepeler A, Karatag T et al (2015) Comparison of the efficacy of diclofenac, acupuncture, and acetaminophen in the treatment of renal colic. Am J Emerg Med 33(6):749–753
Firouzian A, Alipour A, Rashidian-Dezfouli H, Zamani-Kiasari A, Gholipour-Baradari A, Emami-Zeydi A et al (2016) Does lidocaine as an adjuvant to morphine improve pain relief in patients presenting to the ED with acute renal colic? A double-blind randomized controlled trial. Am J Emerg Med 34(3):443–448
Hura G, Knapik P, Sorek-Kubicka G, Maciejewski D (2005) Thoracic paravertebral blockade–history or present time? Wiad Lek 58(3–4):208–211
Rossikhin VV (1978) Effectiveness of M.N. Astvatsaturov’s block in renal colic. Klin Khir 2:74–75
Puterman NS (1973) Treatment of the renal colic. Vestn Khir Im I I Grek 110(3):113–114
Eken C, Durmaz D, Erol B (2009) Successful treatment of a persistent renal colic with trigger point injection. Am J Emerg Med 27(2):252-e3
Belkouch A, Zidouh S, Rafai M, Chouaib N, Sirbou R, Elbouti A et al (2015) Does intranasal fentanyl provide efficient analgesia for renal colic in adults? Pan Afr Med J 20:407
Benitez Camps M, Cerain Herrero MJ, de Miguel Llorente N, Martorell Sole E, Flores Mateo G, Pedro Pijoan AM et al (2015) Tamsulosin efficacy and safety for conservative management of renal colic: systematic review and meta-analysis of randomized controlled trials. Med Clin 145(6):239–247
el-Sherif AE, Salem M, Yahia H, al-Sharkawy WA, al-Sayrafi M (1995) Treatment of renal colic by desmopressin intranasal spray and diclofenac sodium. J Urol 153(5):1395–1398
Pricop C, Branisteanu DD, Orsolya M, Puia D, Matei A, Checherita IA (2016) Sublingual desmopressin is efficient and safe in the therapy of lithiasic renal colic. Int Urol Nephrol 48(2):183–189
Faridaalaee G, Mohammadi N, Merghati SZ, Keyghobadi Khajeh F, Naghipour B, Pouraghaei M et al (2016) Intravenous morphine vs intravenous ketofol for treating renal colic; a randomized controlled trial. Emergency. 4(4):202–206
Mora B, Giorni E, Dobrovits M, Barker R, Lang T, Gore C et al (2006) Transcutaneous electrical nerve stimulation: an effective treatment for pain caused by renal colic in emergency care. J Urol 175(5):1737–1741 (discussion 41)
Lee YH, Lee WC, Chen MT, Huang JK, Chung C, Chang LS (1992) Acupuncture in the treatment of renal colic. J Urol 147(1):16–18
Melzack R, Stillwell DM, Fox EJ (1977) Trigger points and acupuncture points for pain: correlations and implications. Pain 3(1):3–23
Fine PG, Milano R, Hare BD (1988) The effects of myofascial trigger point injections are naloxone reversible. Pain 32(1):15–20
Wyant GM (1979) Chronic pain syndromes and their treatment. II. Trigger points. Can Anaesth Soc J 6(3):216–219
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Ethical approval and informed consent
The research protocol for this study was approved by the research committee of our institution (Registration Number DI/14/105/04/047), and it was found to adhere to the rules of good clinical practice.
Rights and permissions
About this article

Cite this article
Maldonado-Avila, M., Del Rosario-Santiago, M., Rosas-Nava, J.E. et al. Treatment of reno-ureteral colic by twelfth intercostal nerve block with lidocaine versus intramuscular diclofenac. Int Urol Nephrol 49, 413–417 (2017). https://doi.org/10.1007/s11255-016-1479-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-016-1479-5