
Abstract
Purpose
This study’s purpose was to examine established cardiovascular risk prediction model scores for their associations with albuminuria and estimated glomerular filtration rate (eGFR) in Korean population.
Methods
We calculated the 10-year atherosclerotic cardiovascular disease (ASCVD) risk estimated score, Korean coronary heart disease risk prediction score (KRS), and the Adult Treatment Panel (ATP) III risk score for 9733 South Koreans, aged 40–79 years, who were not diagnosed with stroke, angina pectoris, or myocardial ischemia using data from the 2011–2013 Korea National Health and Nutrition Examination Survey.
Results
The associations between cardiovascular risk model scores and the urine albumin-to-creatinine ratio (UACR) and eGFR tended to be stronger for the ASCVD risk score than for the other risk scores. The area under the receiver operating characteristic curve for increased albuminuria (UACR ≥ 30 mg/g) and decreased eGFR (<60 mL/min/1.73 m2) was significantly higher for the ASCVD risk score than for the ATP III risk score and the KRS (except for increased albuminuria in women).
Conclusions
The ASCVD risk score had a stronger relationship with and better predicted albuminuria and eGFR than did the KRS and ATP III risk score.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
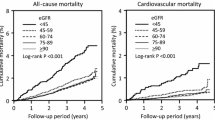
Decreased estimated glomerular filtration rate (eGFR) or increased albuminuria has been associated with a greater risk of cardiovascular mortality [1–3]. A recent meta-analysis suggested that the addition of eGFR and albuminuria to conventional cardiovascular risk factors resulted in improved prediction of cardiovascular risk [4]. Due to the strong associations of eGFR and albuminuria with cardiovascular disease, it may seem intuitive to hypothesize a strong link between cardiovascular risk predicted with these tools and eGFR and albuminuria. In a study of a Chinese population with eGFR > 60 mL/min/1.73 m2 and no cardiovascular disease, an inverse association was found between eGFR and Framingham risk score [5]. Another population-based study revealed a positive association between low-grade albuminuria and Framingham risk score [6], and other studies suggested combination of decreased eGFR and/or increased urine albumin excretion and Framingham risk score for better prevention or detection of cardiovascular disease [7, 8]. However, the relationships between eGFR and albuminuria and other cardiovascular risk estimation methods, such as the 10-year hard atherosclerotic cardiovascular disease (ASCVD) risk estimate [9] and the Korean coronary heart disease risk prediction score (KRS) [10], remain unclear. Thus, this study aimed to assess the associations between albuminuria and eGFR, and cardiovascular disease (CVD), estimated using risk prediction model scores in a representative Korean population.
Materials and methods
Study participants
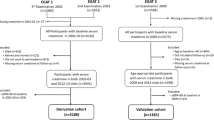
The study participants were from a representative sample of the civilian, non-institutionalized South Korean population included in the Korea National Health and Nutrition Examination Survey (KNHANES) from 2011 to 2013 [11, 12]. Among a total of 24,593 participants, this study included data from 9733 South Korean adults (4254 men and 5479 women), aged 40–79 years, who were not diagnosed with stroke, angina pectoris, or myocardial ischemia, who provided information required for estimating the KRS [10], the Adult Treatment Panel III (ATP III) score [13], and ASCVD risk score [9] and for whom data were available for determining the urine albumin-to-creatinine ratio (UACR) and eGFR.
Measurements and definitions
Demographic variables (age, sex), income level (less than the middle–high level vs. at least the middle–high level), educational level (did not graduate high school vs. graduated high school), medical history (diagnosis and treatment of hypertension, diabetes mellitus, angina pectoris, myocardial ischemia, and stroke), and health behavior-related variables were obtained using data from the survey, which was conducted using a standardized questionnaire via face-to-face interview. Health behavior-related variables included regular exercise at moderate intensity for at least 30 min per day five or more times per week (yes vs. no), alcohol consumption (at least 1 drink per month in the past year; yes vs. no), and smoking status (current smoker, ex-smoker, or non-smoker). Diabetes mellitus was defined as either a high fasting blood glucose level ≥6.99 mmol/L, a diagnosis of diabetes mellitus by a physician, or current treatment for diabetes mellitus [14, 15]. Hypertension was defined as systolic blood pressure ≥140 mmHg, diastolic blood pressure ≥90 mmHg, or use of antihypertensive medications, irrespective of blood pressure.
Blood pressure was measured, and body mass index (BMI) was calculated as weight (kg)/height (m)2 and measured according to standard procedures. Antecubital venous blood samples and random urine samples were obtained from each subject after overnight fasting. The levels of serum total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), glucose, and creatinine and urine creatinine and albumin concentration were measured using an automatic analyzer (Automatic Chemistry Analyzer 7600, Hitachi, Japan and Cobas 8000 C702, Roche, Germany). The UACR was calculated as the urine albumin-to-urine creatinine ratio (mg/g). eGFR was computed using the serum creatinine-based Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation [16]. Categories for albuminuria and eGFR were, respectively, defined as UACR < 30, 30–300 (moderately increased albuminuria), and ≥300 mg/g (severely increased albuminuria), and eGFR ≥ 60, 30–60 (mild to severely decreased eGFR), and <30 mL/min/1.73 m2 (severely decreased eGFR) [1, 17].
The KRS, which provides an absolute 10-year risk of coronary heart disease and includes age, blood pressure, TC, HDL-C, diabetes, and smoking as components [10], the ATP III assessment, which uses a modified Framingham risk model for predicting an individual’s risk for developing CVD over the next 10 years and includes age, TC, HDL-C, systolic blood pressure, and smoking as components [13], and the ASCVD risk score, which assesses the risk of developing the first ASCVD event (a non-fatal myocardial infarction or coronary heart disease death, or fatal or non-fatal stroke) within a 10-year period and includes age, TC, HDL-C, systolic blood pressure, smoking, and diabetes as components [9], were calculated.
Statistical analyses
All the analyses were conducted separately for each sex. Comparisons of the relationships of the three CVD risk scores with the demographics and health behaviors for individuals categorized by albuminuria and eGFR were made using the test for linear trend using Chi-squared test or one-way analysis of variance. A natural logarithmic transformation was performed to normalize the distribution of UACR values. Spearman’s correlations were performed to assess the relationships between kidney function and CVD risk scores. Linear regression analyses were conducted to determine the association of a 1-standard deviation (SD) change in each CVD risk score (independent variable) with UACR and eGFR (dependent variable) as a continuous variable after adjusting for demographics, BMI, and health behaviors. Multinomial logistic regression analyses were applied to determine the associations of a 1-SD change in each CVD risk score as an independent variable with categorized UACR and eGFR as dependent variables after adjusting for demographics, BMI, and health behaviors. Receiver operating characteristic (ROC) curve analyses were used to determine sensitivity, specificity, and area under the curve (AUC) of the CVD risk scores for predicting UACR ≥ 30 mg/g and eGFR < 60 mL/min/1.73 m2. A pairwise comparison of two independent ROC curves was conducted using the Z statistic. Data were analyzed using the IBM Statistical Package for the Social Sciences (SPSS) software version 21.0.0.0 (IBM Corp., Armonk, NY, USA) and MedCalc statistical software version 15.6.1 (MedCalc Software bvba, Ostend, Belgium; https://www.medcalc.org; 2015). A two-sided P < 0.05 was considered statistically significant.
Results
In Korean men, 8.0 % had moderately increased albuminuria, 1.7 % had severely increased albuminuria, 4.5 % had mild to severely decreased eGFR, and 0.2 % had severely decreased eGFR, while in Korean women, those rates were 7.7, 1.1, 2.7, and 0.9 %, respectively. CVD risk scores, age, and prevalence of hypertension and diabetes mellitus tended to increase when individual had increased albuminuria and decreased eGFR in both sexes (Table 1). The relationships between CVD risk scores and kidney function were presented using Spearman correlations and multiple linear regression analyses in Table 2. All correlations between CVD risk scores and kidney function were significant. Even after adjusting for demographics, BMI, and health behaviors, 1-SD increase in CVD risk scores was associated with increase in UACR and decrease in eGFR. The regression coefficient was greater for the ASCVD risk score than it was for the other CVD risk scores. In the multinomial logistic regression analyses between CVD risk scores and categorized UACR and eGFR, the odds ratios were generally higher for the ASCVD risk score than it was for the other CVD risk scores. As compared with the association in individuals with UACR < 30 mg/g and eGFR ≥ 60 mL/min/1.73 m2, a 1-SD increase in the ASCVD risk score was associated with moderately or severely increased albuminuria (odds ratio 1.85 and 2.59 for men and 1.42 and 1.70 for women) and mild to severely decreased eGFR (odds ratio 2.25 for men and 1.88 for women) (Table 3). In the comparison of the ROC curve analyses, the ASCVD risk score better predicted increased albuminuria (UACR ≥ 30 mg/g) and decreased eGFR (eGFR < 60 mL/min/1.73 m2) as compared to the ATP III risk score and the KRS (except for increased albuminuria in women, P < 0.05). The cutoff values of CVD risk scores for increased albuminuria and decreased eGFR were consistently higher in men as compared in women (Table 4).
Discussion
In this representative Korean population, KRS, ATP III risk score, and ASCVD risk score were associated with increased albuminuria and decreased eGFR. In the comparison of the three CVD risk scores for determining these relationships, the ASCVD risk score tended to have a stronger association than did the KRS and ATP III risk score. As compared to the ATP III risk score, the KRS was a better predictor of increased albuminuria in both sexes and of decreased eGFR in women. Although the present findings replicated those from previous studies with respect to the relationship between the Framingham risk score and eGFR and albuminuria in a Chinese population [5] and in a Korean population [6], the current study additionally evaluated the relative performance of CVD risk scores on those associations. As a result, the strength of the associations appeared to be greatest for the ASCVD risk score, followed by the KRS and the ATP III risk score.
The link between albuminuria and eGFR and CVD risk score suggests a common pathway, such as insulin resistance, endothelial dysfunction, vascular inflammation, or atherosclerosis [18]. However, the difference in the associations may be explained by the differences in individual components included in the CVD risk scores and the relative weight of the coefficient given to each component in those risk scores. The lower associations with the ATP III risk score may be related to the exclusion of diabetes mellitus from the components.
The associations between increased albuminuria and/or decreased eGFR and CVD event development were well demonstrated. Excretion of albumin in the urine was a continuous risk factor for CVD events, without a lower limit [17, 19], and the relationship between urinary albumin and cardiovascular mortality was monotonic in meta-analyses [2]. With respect to the association between eGFR and cardiovascular mortality, cardiovascular mortality gradually increased as eGFR decreased from 60 mL/min/1.73 m2 to lower levels [2]. As compared to women, the association of eGFR and UACR with the risk of cardiovascular mortality at all levels of eGFR and UACR was higher in men [1]. In the current data, the cutoff scores of CVD risk for predicting increased albuminuria and decreased eGFR in men were consistently higher than those in women. The current findings support previous results showing sex differences in the associations of eGFR and UACR with cardiovascular events.
Several limitations of the current study need to be noted. Although the area under the ROC curve analysis is commonly used for discrimination purposes, it has limitations, such as lower sensitivity, in assessing the impact of adding new predictors to a score and evaluating the differences in probabilities between models [20]. Although eGFR assessed using the CKD-EPI equation has been shown to be a more accurate estimate than the Modification of Diet in Renal Disease (MDRD) study equation, the precision for determining eGFR using the CKD-EPI equation remains limited [16]. The measurement of urinary albumin using random urine also has potential problems with respect to the accuracy of reflecting proteinuria quantification [21–23]. In addition, individuals taking medications that may influence eGFR, albuminuria, and CVD risk scores were not taken into account in the analyses. Although ASCVD risk score was better for discrimination of increased albuminuria and decreased eGFR than KRS in this study, a recent study suggested inadequate performance of ASCVD risk score for predicting atherosclerotic cardiovascular disease events in Korean population [24]. To compare the prognostic ability of these prediction models for development of decreased eGFR and albuminuria, long-term prospective studies are needed.
In summary, this study compared the relationships of CVD prediction models, such as the KRS, the ATP III risk score, and the ASCVD risk score, with eGFR and albuminuria in a representative Korean population. The ASCVD risk score had the strongest relationship and best discrimination for predicting increased albuminuria and decreased eGFR compared to the KRS and ATP III risk score. Therefore, ASCVD risk score may be a more sensitive assessment tool for identifying individuals with higher risk of chronic kidney disease than KRS and ATP III risk score in Korean population. To the best of our knowledge, there is no established prospective study for the association between cardiovascular risk and chronic kidney disease in Korean population, and then, current findings confirm previous knowledge in Korean population using several CVD risk scores.
References
Komenda P, Rigatto C, Tangri N (2014) Estimated glomerular filtration rate and albuminuria: diagnosis, staging, and prognosis. Curr Opin Nephrol Hypertens 23:251–257
Chronic Kidney Disease Prognosis Consortium, Matsushita K, van der Velde M et al (2010) Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet 375:2073–2081
van der Velde M, Matsushita K, Coresh J et al (2011) Lower estimated glomerular filtration rate and higher albuminuria are associated with all-cause and cardiovascular mortality. A collaborative meta-analysis of high-risk population cohorts. Kidney Int 79:1341–1352
Matsushita K, Coresh J, Sang Y, CKD Prognosis Consortium et al (2015) Estimated glomerular filtration rate and albuminuria for prediction of cardiovascular outcomes: a collaborative meta-analysis of individual participant data. Lancet Diabetes Endocrinol 3:514–525
Jin B, Bai X, Han L, Liu J, Zhang W, Chen X (2014) Association between kidney function and Framingham global cardiovascular disease risk score: a Chinese longitudinal study. PLoS One 9:e86082
Hong JW, Ku CR, Noh JH, Ko KS, Rhee BD, Kim DJ (2015) Association between low-grade albuminuria and cardiovascular risk in Korean adults: the 2011–2012 Korea National Health and Nutrition Examination Survey. PLoS One 10:e0118866
Asselbergs FW, Hillege HL, van Gilst WH (2004) Framingham score and microalbuminuria: combined future targets for primary prevention? Kidney Int Suppl 92:S111–S114
Chang A, Kramer H (2011) Should eGFR and albuminuria be added to the Framingham risk score? Chronic kidney disease and cardiovascular disease risk prediction. Nephron Clin Pract 119:c171–c177
Stone NJ, Robinson JG, Lichtenstein AH, American College of Cardiology/American Heart Association Task Force on Practice Guidelines et al (2014) 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 129:S1–S45
Jee SH, Jang Y, Oh DJ et al (2014) A coronary heart disease prediction model: the Korean Heart Study. BMJ Open 4:e005025-2014-005025
Korea Centers for Disease Control and Prevention, Ministry of Health and Welfare. Korea health statistics 2010-2012: The Fifth Korea National Health and Nutrition Examination Survey (KNHANES V) [internet]. 2013. https://knhanes.cdc.go.kr/knhanes/index.do
Korea Centers for Disease Control and Prevention, Ministry of Health and Welfare. Korea health statistics 2013: The Sixth Korea National Health and Nutrition Examination Survey (KNHANES VI-1) [internet]. 2014. https://knhanes.cdc.go.kr/knhanes/index.do
Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (2001) Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III). JAMA 285:2486–2497
Korea Centers for Disease Control and Prevention. Guidelines for using the Fifth National Health and Nutrition Examination Survey (KNHANES V-1), 2010 In Osong, Chungcheong Buk-Do, Republic of Korea, Korea Centers for Disease Control and Prevention. 2011
Korea Centers for Disease Control and Prevention. Guidelines for using the third year, Fourth National Health and Nutrition Examination Survey (KNHANES IV), 2009 In, Osong, Chungcheong Buk-Do, Republic of Korea, Korea Centers for Disease Control and Prevention. 2010
Levey AS, Stevens LA, Schmid CH, CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) (2009) A new equation to estimate glomerular filtration rate. Ann Intern Med 150:604–612
Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group (2013) KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl 13:1–150
Ruggenenti P, Remuzzi G (2006) Time to abandon microalbuminuria? Kidney Int 70:1214–1222
Hillege HL, Fidler V, Diercks GF, Prevention of Renal and Vascular End Stage Disease (PREVEND) Study Group et al (2002) Urinary albumin excretion predicts cardiovascular and noncardiovascular mortality in general population. Circulation 106:1777–1782
Cook NR (2008) Statistical evaluation of prognostic versus diagnostic models: beyond the ROC curve. Clin Chem 54:17–23
KDOQI (2007) KDOQI clinical practice guidelines and clinical practice recommendations for diabetes and chronic kidney disease. Am J Kidney Dis 49:S12–S154
Lamb EJ, MacKenzie F, Stevens PE (2009) How should proteinuria be detected and measured? Ann Clin Biochem 46:205–217
Viswanathan G, Upadhyay A (2011) Assessment of proteinuria. Adv Chronic Kidney Dis 18:243–248
Jung KJ, Jang Y, Oh DJ et al (2015) The ACC/AHA 2013 pooled cohort equations compared to a Korean Risk Prediction Model for atherosclerotic cardiovascular disease. Atherosclerosis 242:367–375
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
K. Lee declares that she has no conflict of interest. J. Kim declares that he has no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The KNHANES was conducted with ethical approval from the Institutional Review Board of the Korea Center for Disease Control and Prevention (Nos: 2012-01EXP-01-2C, 2013-07CON-03-4C).
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Lee, K., Kim, J. Estimated glomerular filtration rate and albuminuria in Korean population evaluated for cardiovascular risk. Int Urol Nephrol 48, 759–764 (2016). https://doi.org/10.1007/s11255-016-1244-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-016-1244-9