
Abstract
Twenty-eight pluriparous and non-lactating Santa Inês sheep were synchronized with vaginal sponge and an intramuscular (IM) injection of 37.5 μg of cloprostenol on random days of the estrous cycle (D0); day 6 (D6), at 7:00 am, the devices were removed, and after 24 h (D7), GnRH analog (25 μg of lecirelin) was administrated. Fixed-time artificial insemination (FTAI) with cervical traction by the transcervical route was performed 52 to 58 h after sponge removal. Doppler velocimetry of both uterine arteries was performed on D0, D2, D4, and the morning of D6 (every 48 h), and then every 12 h from D6 to D8 (7:00 a.m. and 7:00 p.m.). We analyzed the peak systolic velocity (PSV), end-diastolic velocity (EVD), time-averaged maximum and mean velocity (TAMAX, TAMEAN), pulsatility index (PI), resistance index (RI), systolic/diastolic ratio (S/D), arterial diameter (AD), and blood flow volume (BFV), with the objective of evaluating the hemodynamic behavior of blood flow velocity parameters of the uterine artery during a short-term progesterone synchronization protocol in ewes. With respect to phases, we noted increases in the means of TAMAX and TAMEAN and decreases of EDV, PI, and RI (P < 0.05). S/D, EDV, TAMEAN, PI, RI, SD, AD, and BFV showed differences between the time of progesterone insertion and the estimated time of ovulation (which was considered the last evaluation) (P < 0.05). The PI and RI values were different when comparing the times of insertion and withdrawal of the progesterone device (PI 2.53–1.54 and RI 0.76–0.68) (P < 0.05). The PI was different with respect to side (P < 0.001), but no side effect was seen in the RI. In conclusion, the two uterine arteries behave differently under the effect of progesterone (intravaginal sponges) and the effect of estradiol during the follicular phase, and estrous phase was responsible for increasing uterine blood flow.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Estrus and ovulation synchronization protocols for ruminants are important to stabilize the timing of reproductive activity in order to improve breeding outcomes and in turn profitability. Decreases in conception rates can result from inappropriate human interference (Russi et al. 2010), pathology of the testis and infertile semen (Pinggera et al. 2008; Arruda et al. 2015), and pathologies of the female genital tract (Marques Júnior et al. 2011). In the latter case, if the cause is identified while planning for selection, some negative consequences can be minimized. In bovines, decisions to discard individuals due to uterus and ovary problems are made using B-mode ultrasound (Lucy 2007). However, this practice is not often applied in small ruminants.
Uterine functionality is highly dependent on adequate vascular perfusion. Vascular disorders are one of the most common causes of subfertility (Ferrusola et al. 2014). Spectral Doppler ultrasonography has become an indispensable tool for the clinical evaluation of female reproductive fertility. In veterinary medicine, there are two types of Doppler ultrasound systems currently in use: continuous wave and pulsed wave (Herzog and Bollwein 2007). They are most useful for estimating blood flow resistance in vessels, and consequently, the hemodynamic viability of organs and structures (Ginther 2014; Beltrame et al. 2017). There is vast information regarding vascular changes in the sheep uterus, which has been generated by different techniques (Saunders et al. 1998; Sprague et al. 2009). However, there are no cutoffs and references to establish normal and pathological findings related to the uterus in ewes.
The early diagnosis of uterine dysfunction triggered by a vascular disorder is crucial for the application of therapeutic strategies to maximize fertility and delay tissue damage in the female reproductive tract. In addition, Doppler ultrasonography is an excellent tool to eliminate females before the reproductive season, since it increases the possibility of identifying reproductive problems (absence, increase, or reduction of blood flow) not diagnosed by conventional ultrasonography.
During a synchronization protocol, differences in vascularization may be due to fluctuations in progesterone (P4) concentrations. At times, an increase in P4 concentration may exert a negative relationship on the size of the dominant follicle. On the other hand, withdrawal of the P4 device promotes follicular growth and subsequent ovulation of a young follicle (Menchaca et al. 2017).
However, despite the considerable effort to validate this imaging modality in small ruminants, reference values have not yet been established. In a study using pulsed-wave Doppler ultrasonography in Brazil, with respect to the uterus, only the physiological behavior of the Doppler parameters during pregnancy were studied (Beltrame et al. 2017). Corroborating the scarcity of reports, in the ovine species, there is a lack of information about the behavior of hemodynamic indices and parameters of blood flow velocity of the uterine artery during synchronization protocols. This makes it difficult to interpret any values, and their associations with physiological or pathological conditions. Thus, the objective of this study was to evaluate the hemodynamic behavior of blood flow velocity parameters of the uterine artery during a short-term progesterone synchronization protocol in ewes.
Materials and methods
Animals
The experiment was conducted during two periods between September 2016 (n = 14) and March 2017 (n = 14) in Colatina, Brazil (LAT 19°, 40′ 7″ S LON 40°, 53′ 9″ W). Twenty-eight pluriparous and non-lactating Santa Inês ewes, with 4 ± 2 years and average weight of 60 kg, were studied. They were fed Panicum maximum cv. Aruana grass and supplemented with 280 g of concentrate/ewe/day (soybean meal and milled corn, 14.3% crude protein). Water was provided ad libitum. A gynecological exam was performed on all animals before the study. Only animals lacking reproductive abnormalities, as detected by conventional ultrasonography or a clinical exam, were used. The sheep were dewormed and vaccinated and otherwise considered healthy during a general physical examination.
Experimental design
Females were synchronized using a vaginal sponge impregnated with 60 mg of medroxyprogesterone (MAP Progespon®, Intervet, Schering-Plough) and an intramuscular (IM) injection of 37.5 μg of cloprostenol (0.5 ml Prolise®, Tecnopec, Brazil) on random days of the estrous cycle, considered to be day zero (D0).
On day 6 (7:00 am) of the protocol, devices were removed, and after 24 h (D7), a GnRH analog (25 μg lecirelin) was administrated via an IM injection (Gestran Plus®, Tecnopec, Brazil). A transcervical FTAI with cervical traction was performed 52 to 58 h after device removal with cooled semen collected from a fertile male (200 × 106 sperm in 0.25 ml).
Doppler velocimetry of both uterine arteries was performed by transrectal ultrasonography on D0, D2, D4, and the morning of D6 (every 48 h) and every 12 h from D6 to D8 (7:00 a.m. and 7:00 p.m.). This was performed on standing and unsedated animals by a single operator. In order to avoid unnecessary stress, examinations were conducted near the stalls.
Color Doppler ultrasonography
A color Doppler ultrasound (Z6 Vet, Mindray®) device equipped with a multifrequency linear transducer (5–10 MHz) was used for analysis. To obtain transrectal images, we used an adapter/extender with the transducer to facilitate intrarectal guidance and movement. The ultrasonic device was used to detect and display the right and left uterine arteries.
Uterine artery location
The uterine artery was located transrectally, skull laterally to the bladder, using the external iliac artery as a reference point. From this, we lateralized the transducer by viewing the uterine artery in a cross-section and sliding it dorsally to the branch of the iliac artery (Beltrame et al. 2017). Alternatively, we followed the method described for cattle by Ginther et al. (2007), in which the location of the uterine artery is obtained from the abdominal aorta, turning the probe up and monitoring its end portion relative to a branching iliac artery. The angulation of the gate was not used since it was viewed in the uterine artery in cross-section.
Dynamics of the uterine artery indices
As described above, we analyzed parameters of blood flow speed and hemodynamic indices; namely peak systolic velocity (PSV) (cm/s), end-diastolic velocity (EVD) (cm/s), time-averaged maximum and mean velocity (TAMAX, TAMEAN cm/s), pulsatility index (PI), resistance index (RI), and systolic/diastolic ratio (S/D). The blood flow volume (BFV) (ml/min) was determined using the algorithm described by Bollwein et al. (2002). Arterial diameter (AD) (mm) was determined using the free ImageJ® software.
With the exception of BFV, all hemodynamic parameters were calculated automatically by the ultrasound Doppler device, after obtaining at least three systolic peaks in the same speed range. We used a sample volume of 1 mm (gate), transducer frequency of 7.5 MHz, pulse repetition frequency (PRF) of 1.0 KHz, and wall filter (WF) of 171 KHz.
Statistical analysis
Normality was tested using the Kolmogorov–Smirnov test. Arithmetic means and standard errors were calculated for all variables. To determine differences by time, uterus side, and phase (progesteronic (D0 until D6) × estrogenic (D7 and D8)) on estimates of uterine hemodynamics as reflected by the study variables (PSV, EVD, TAMEAN, TAMAX, RI, PI, S/D, AD, BFV), statistical analyses were performed using the MIXED procedure of SAS (SAS Inst., Inc., Cary, NC). A difference was considered significant at P < 0.05. Pearson correlations were used to verify the degree of association between the methods and variables.
Results
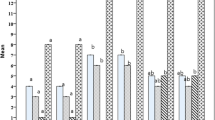
The Doppler parameters and the diameter of the uterine artery showed significant changes during the short-term progesterone synchronization protocol (Fig. 1).

Doppler parameters during a short-term progesterone synchronization protocol. a PSV, peak systolic velocity (cm/s); b EDV, end-diastolic velocity (cm/s); c TAMAX, time-averaged maximum velocity (cm/s); d TAMEAN, time-averaged mean velocity (cm/s); e PI, pulsatility index; f RI, resistance index; g AD, arterial diameter (mm); h BFV, blood flow volume (ml/min). D, day; M, morning; A, afternoon
All variables (PSV, EDV, TAMAX, TAMEAN, PI, RI, SD, AD, and BFV) presented differences (P < 0.05) according to the evaluation day, during the protocol. The variables PSV, TAMAX, TAMEAN, RI, SD, and BFV did not differ between the time of P4 insertion and the estimated time for ovulation (which was considered the last evaluation (P > 0.05), except EDV and AD, which were higher, and PI which presented lower mean in ovulation than at D0 (P > 0.05)). The PI and BFV averages were lower in the evaluation of progesterone device withdrawal (D6M) when compared with the moment of insertion (D0) (PI 2.53–2.08 and BFV 53.38–38.75, respectively for insertion (D0) and withdrawal (D6M) of the P4 device) (P < 0.05) (Fig. 1).
Overall TAMEAN and TAMAX tended to follow the same pattern during the protocol, with a slight decrease after insertion of the sponge to D1 (P > 0.05) and afterward, a gradual increase until D8 (P < 0.05). AD and BFV initially decreased, and then increased (minimum of 2.26 mm and 25.60 ml/min on D1, maximum of 3.04 mm (D8A) and 53.38 ml/min (D0), respectively) (P < 0.05).
Over the two phases, which included the presence of the progesterone device and the estimated period of ovulation (when the estradiol concentration was increasing, after removal of the P4 device), we found evidence of increases (P < 0.05) of the mean values of TAMAX and TAMEAN and decreases (P < 0.05) of EDV, PI, RI, and S/D (Table 1). However, PSV (35.89 ± 1.39), AD (2.76 ± 0.08), and BFV(40.13 ± 6.26) did not show differences (P > 0.05).
Means of the variables with respect to the right and left uterine arteries are presented in Table 2. The PSV (36.95 ± 0.62), EDV (11.98 ± 0.32), TAMAX (16.00 ± 0.47), and TAMEAN (9.42 ± 0.24) were higher in the right side (P < 0.05), while PI (2.06 ± 0.10), RI (0.73 ± 0.02), and AD (2.82 ± 0.04) were higher in the left side (P < 0.05).
In general, Doppler parameters and the diameter of the uterine artery showed significant correlations, with the exception of AD, PSV, and BFV with PI, RI, and S/D (Table 3). The parameter BFV showed highly significant coefficients (P < 0.001), positive low to medium magnitudes with PSV, EDV, TAMAX, TAMEAN, and AD; PI, RI, S/D, and AD had negative correlation coefficients of low to medium magnitudes with EDV, TAMAX, and TAMEAN (with the exception of EDV and AD, which were not significant); and PI, RI, and S/D presented high and positive mutual pairwise correlations (P < 0.001).
Discussion
Uterine arteries are the vessels most frequently used to determine Doppler parameters in gynecology (Panarace et al. 2006; Petridis et al. 2017; Beltrame et al. 2017). The blood flow indices and Doppler parameters in the present study are the first measures of hemodynamic changes in the uterine vasculature during a short-term progesterone synchronization protocol in ewes. We have thus provided reference values for changes in uterine blood flow during short-term progesterone synchronization protocols in sheep (Table 1).
We found differences in EDV, TAMAX, TAMEAN, PI, RI, and S/D according to the phase of the protocol. These differences may be due to progesterone and estradiol (E2) changes. Both RI and PI increased when blood perfusion decreased, and it decreased when blood perfusion was increasing (Petridis et al. 2017). In a synchronization protocol, there are times when serum P4 concentrations have a negative relationship with the size of the dominant follicle, and when higher progesterone levels cause regression of the dominant follicle (with the presence of an internal device). On the other hand, device withdrawal promotes follicular growth and thus allows for the ovulation of a young follicle (Menchaca et al. 2017).
In lactating Holstein cows, Rawy et al. (2018) showed that PI and RI values decreased while TAMAX, BFV, and diameter of uterine arteries increased in response to E2 administration. These events were associated with an increase in blood flow, as evidenced by the corresponding increase in blood flow velocity. Although this is the first description of a hemodynamic pattern during a short-term progesterone-duration synchronization protocol, given the existence of the two phases in the protocol (P4 × E2), our results suggest different physiological behaviors and different values of some variables (Fig. 1). With respect to BFV, although there were no differences in relation to the phases, differences were identified with respect to the evaluated time points (Fig. 1). In bitches, ovulation and the early luteal phase are characterized by high blood flow velocities and low PI and RI values (Köster et al. 2001). We found similar patterns in the ewes (Fig. 1).
A study of cows during the estrous cycle showed that uterine blood flow had a characteristic pattern. Although several factors are known to be involved in the regulation of uterine blood flow, estradiol appears to be responsible for vasodilation (Mattioli et al. 2001; Rawy et al. 2018). Our results show a similar pattern in ewes, with decreases in RI and PI. In contrast, progesterone appears to exhibit a negative effect on uterine perfusion (Fig. 1).
Except for BFV and S/D, all other variables differed according to the evaluated side. This is in contrast to results described for cattle by Rawy et al. (2018), who did not identify differences in hemodynamic variables, but it emphasizes that sheep mostly present multiple ovulations, and, in this case, different ovarian performance can explain uterine changes and these results (Table 2).
In humans, Doppler ultrasonography provides several parameters that can be used as indicators of uterine efficiency (Idowu et al. 2017). Esmaeillou et al. (2015) and Alcazar (1998) suggested a cutoff value of 0.45 for the RI. Achiron et al. (1993), in a postpartum and postabortal bleeding study, showed 100% specificity and 60% sensitivity, using an RI cutoff level of < 0.35.
Doppler ultrasonography could be an alternative to invasive procedures. This imaging modality has improved the diagnosis of male and female reproductive tract disorders in animals and humans (Ferreira et al. 2007; Blanco et al. 2011; Ortiz-Rodriguez et al. 2017). The existence of a pattern of behavior may help in the early identification of any change in the uterus. Vascular perfusion is critical for the correct diagnosis of various uterus and ovary pathologies and the prompt implementation of appropriate treatment. Related to the uterus, our results suggest hemodynamic values that can be used to guide decisions.
In conclusion, the two uterine arteries behave differently under the effect of progesterone (intravaginal sponges) and the effect of estradiol during the follicular phase, and the estrous phase was responsible for increasing uterine blood flow. Thus, even though our results suggest a pattern during a normal short-term progesterone synchronization protocol, more studies of uterine hemodynamic patterns are needed to better determine the indexes and changes that might indicate pathological situations, and other potential Doppler applications, to assure their reliability for use as part of regular gynecological veterinary evaluation.
References
Achiron, R., Goldenberg, M., Lipitz., Mashiach, S., 1993. Transvaginal duplex Doppler ultrasonography in bleeding patients suspected of having residual trophoblastic tissue. Obstetrics and Gynecology. 81, 507–511.
Alcazar, J.L., 1998. Transvaginal ultrasonography combined with color velocity imaging and pulsed Doppler to detect residual trophoblastic tissue. Ultrasound in Obstetrics and Gynecology. 11, 54–58.
Arruda, R.P., Celeghini, E.C.C., Garcia, A.R., Carli dos Santos, G., Leite, T.C., Oliveira, L.Z., et al., 2015. Bull sperm morphology: interpretation and impact on fertility. Revista Brasileira de Reprodução Animal. 39 (1), 47–60.
Beltrame, R.T., Covre, C., Littig, L.B., Martins, A.B., Quirino, C.R., Junior, A.B., et al., 2017. Transrectal Doppler sonography of uterine blood flow in ewes during pregnancy. Theriogenology 91, 55–61.
Blanco, P. G, Rodríguez, R., Rube, A., Arias, D.O., Tórtora, M., Díaz, J.D., et al., 2011. Doppler ultrasonographic assessment of maternal and fetal blood flow in abnormal canine pregnancy. Animal Reproduction Science 126, 130–135.
Bollwein, H., Baumgartner, U., Stolla, R., 2002 Transrectal Doppler sonography of uterine blood flow in cows during pregnancy. Theriogenology 57 (8), 2053–2061.
Esmaeillou, H., Jamal, A., Eslamian, L., Marsousi, V., Sarvi, F., Kokab, A., 2015. Accurate Detection of Retained Products of Conceptions after First- and Second- trimester Abortion by Color Doppler. Journal of Medical Ultrasound. 23, 34–38.
Ferreira, A.M., Pires, C.R., Moron, A.F., Araujo Júnior, E., Traina, E., Mattar, R., 2007. Doppler assessment of uterine blood flow in recurrent pregnancy loss. International Journal of Gynecology. Obstet. 98, 115–119.
Ferrusola, C.O., Gracia-Calvo, L.A., Ezquerra, J., Peña, F.J., 2014 Use of Colour and Spectral Doppler Ultrasonography in Stallion Andrology. Reproduction in Domestic Animals. 49 (4), 88–96.
Ginther, O.J., 2014. How ultrasound technologies have expanded and revolutionized research in reproduction in large animals. Theriogenology 81, 112–125.
Ginther, O.J., Gastal, E.L., Gastal, M.O., Utt, M.D., Beg, M.A., 2007. Luteal blood flow and progesterone production in mares. Animal Reproduction Science. 99. 213–220.
Herzog, K., Bollwein, H., 2007. Application of Doppler ultrasonography in cattle reproduction. Reproduction in Domestic Anim. 42 (Suppl 2), 51–58.
Idowu, B.M., Ibitoye, B.O., Adetiloye, V.A., 2017. Uterine Artery Doppler Velocimetry of Uterine Leiomyomas in Nigerian Women. Rev. Bras. Ginecol. Obstet. 39, 464–470.
Köster, K., Poulsen, C.N., Günzel-Apel, A.R., 2001. A Doppler ultrasonographic study of cyclic changes of ovarian perfusion in the Beagle bitch. Reproduction 122, 453–461.
Lucy, M.C., 2007. The bovine dominant ovarian follicle . J.Anim. Sci. 85, E89–E99.
Marques Júnior, A.P., Martins, T.M. Borges Á.M., 2011. Diagnosis and treatment of uterine infection in cows. Rev. Bras. Reprod. Anim. 35 (2), 293–298.
Mattioli, M., Barboni, B., Turriani, M., Galeati, G., Zannoni, A., Castellani, G., et al., 2001. Follicle activation involves vascular endothelial growth factor production and increased blood vessel extension. Biol. Reprod. 65, 1014–1019.
Menchaca, A., Santos Neto, P.C., Cuadro, F., 2017. Estrous synchronization treatments in sheep: Brief update. Rev. Bras. Reprod. Anim. 41 (1), 340–344.
Ortiz-Rodriguez, J.M., Lopez, L.A., Muñoz, P.M., Alvarez, M., Phillips, G.G., Anel, L., et al., 2017. Pulse Doppler ultrasound as a tool for the diagnosis of chronic testicular dysfunction in stallions. Plos One. 12(5),1–21.
Panarace, M., Garnil, C., Marfil, M., Jauregui, G., Lagioia, J., Luther, E., et al., 2006. Transrectal Doppler sonography for evaluation of uterine blood flow throughout pregnancy in 13 cows. Theriogenology 66 (9), 2113–2119.
Petridis, I.G., Barbagianni, M.S., Ioannidi, K.S., Samaras, E., Fthenakis, G.C., Vloumidi, E.I., 2017. Doppler ultrasonographic examination in sheep. Small Ruminant Res. 152, 22–32.
Pinggera, G.M., Mitterberger, M., Bartsch, G., Strasser, H., Gradl, J., Aigner, F., et al., 2008. Assessment of the intra- testicular resistive index by colour Doppler ultrasonography measurements as a predictor of spermato- genesis. BJU Int. 101(6), 722–726.
Rawy, M., Mido, S., El-Sheikh Ali, H., Derar, D., Megahed, G., Kitahara, G., et al. 2018. Effect of exogenous estradiol Benzoate on uterine blood flow in postpartum dairy cows. Anim. Reprod. Sci. 192, 136–145.
Russi, L.S., Costa-e-Silva, E.V., Zúccari, C.E.S.N., Recalde, C.S., 2010. Human resources in artificial insemination of beef cattle: profile of managers and inseminators. Rev. Bras. Zootecn. 39(7), 1464–1470.
Saunders, H.S., Burns, P.N., Needleman, L,. Liu, J.B., Boston, R. Wortman, J.A., Chan, L., 1998. Hemodynamic factors affecting uterine artery Doppler waveform pulsatility in sheep. J Ultrasound Med. 17, 357–68.
Sprague, B.J., Phernetton, T. M., Magness, R. R., & Chesler, N. C. (2009). The effects of the ovarian cycle and pregnancy on uterine vascular impedance and uterine artery mechanics. European journal of obstetrics, gynecology, and reproductive biology, 144 Suppl 1(Suppl 1), S170–S178. doi:https://doi.org/10.1016/j.ejogrb.2009.02.041
Acknowledgments
This study was conducted as a requirement of junior scientific initiation (Federal Institute of Espírito Santo - IFES), scientific initiation, and graduation work for the Veterinary course at the Centro Universitário do Espírito Santo (UNESC).
Funding
We had financial support (TO 913/2015) and a scholarship financed by Fundação de Amparo a Pesquisa e Inovação do Espírito Santo (FAPES). Joao Vitor Pagoto Careta has a scholarship financed by FAPES, which is gratefully acknowledged.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Statement of animal rights
This study was approved by the institute’s ethics committee (Protocol No. CEUA/IFES – ES 23147.000841-2016-23).
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Highlights
• The Doppler parameters and the diameter of the uterine artery showed significant changes during a short synchronization protocol
• Differences were found between the means of the Doppler parameters in relation to the phase of the protocol (progesterone × estradiol)
• Doppler parameters and the diameter of the uterine artery showed significant correlations
Rights and permissions
About this article

Cite this article
Beltrame, R.T., Morais Junior, N.N., Careta, J.V.P. et al. Uterine hemodynamics during a short-term progesterone synchronization protocol in ewes. Trop Anim Health Prod 52, 503–509 (2020). https://doi.org/10.1007/s11250-019-02035-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11250-019-02035-5