
Abstract
Many studies have shown that uric acid was related to hypertension. However, the association dependence on body mass index (BMI) or age was unclear. This study was performed with a group of 4012 Chinese population aged 30 to 92 years old. Subjects were divided into four groups according to the quartiles of uric acid (UA) concentration [First group: ≤ 231 μmol/L (reference), Second group: 231-289 μmol/L, Third group: 289-362 μmol/L, Fourth group: > 362 μmol/L]. Hypertension was defined as newly measured blood pressure ≥ 140/90 mmHg or taking antihypertensive drugs. Stratified analysis based on BMI (< 28 kg/m2 vs ≥ 28 kg/m2) and age (< 60 years old vs ≥ 60 years old) to analyze the association between UA and hypertension. Subjects were 54.50 (45.00, 63.00) years old, and 40.98% were male, 38.33% were hypertension. Adjusted odds ratios (95% confidence intervals) for the association of UA and hypertension were 2.226 (1.662, 2.980), 4.340 (3.253, 5.790), 5.898 (4.434, 7.845) and 6.557 (4.927, 8.727) in the four groups among ≥ 60 years old respectively comparing with first group among < 60 years old. Adjusted odds ratios (95% confidence intervals) for the association between UA and hypertension were 2.170 (1.236, 3.808), 5.260 (3.267, 8.468), 9.056 (5.509, 14.888) and 3.730 (2.529, 5.550) in the four groups among BMI ≥ 28 kg/m2 respectively comparing with first group among BMI < 28 kg/m2. Uric acid was significantly associated with the hypertension. The association was stronger among subjects ≥ 60 years old or BMI ≥ 28 kg/m2.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Highlights
-
Our study was a cross-sectional study.
-
We selected 4012 permanent residents in 24 rural and urban communities as research objects in Hunan Province.
-
The study subjects were divided into four groups according to the quartiles of uric acid.
Introduction
Hypertension is a global health challenge, affecting millions of people around the world [1, 2]. Previous study showed that the incidence of hypertension in the world has reached 26% [3], and in China has reached 29.6% [4]. Hypertension is one of the most important risk factors for cardiovascular disease, stroke and kidney disease, and it is also the main cause of premature death and disability [5,6,7]. As we all know, hypertension is considered to be a multifactorial chronic disease, which may be related to some risk factors [8]. In recent years, accumulated epidemiological and clinical evidence has shown that UA level was related to hypertension [9,10,11]. UA is the ultimate product of purine metabolism which is naturally found in blood in certain amounts [12]. High UA plays an important role in the pathogenesis of cardiovascular, renal disease and metabolic syndrome [13]. Meanwhile, some studies have shown that elevated UA level was related to the occurrence of hypertension [14, 15]. Elevated UA can cause reduced effectiveness of nitric oxide, endothelial dysfunction and renin angiotensin aldosterone system damage, and finally lead to vasoconstriction [16, 17]. However, the association the UA and hypertension dependence on BMI or age was unclear. We conducted a cross-sectional study to determine whether UA was significantly associated with hypertension in a sample of 4012 rural and urban communities population with overall health. In addition, we also tried to analyze the association between UA and hypertension with stratified analysis based on BMI and age.
Materials and methods
Study population and study design
The current study was a cross-sectional study to investigate the prevalence of hypertension among 24 communities in Hunan Province from 2013 to 2014. We selected 6 regions (Changsha, Zhuzhou, Hengyang, Yueyang, Xiangxi, and Yongzhou) from 14 regions in Hunan Province. Then we randomly selected two urban communities and two rural communities from each region that has been selected. The permanent residents of each survey site ≥ 30 years old were included as the targets of the survey. In this study, 5258 people should be surveyed, and 4012 people were actually surveyed, with a response rate of 76.30%. All the respondents have lived in the regions for more than 5 years. By asking about the medical history of hypertension and measuring the blood pressure of the subjects by professionals. Ultimately, a population of 4012 participants (1644 males and 2368 females) were included in our study with 1538 participants (766 males and 772 females) with hypertension. This study was approved by the Institutional Ethics Review Board of the Hunan Provincial People’s Hospital, Changsha, China. Written informed consents were obtained for each subject included in this study.
Data collection
Baseline characteristics were obtained by well-trained experimental personnel using a standard questionnaire in a personal interview. Before the survey was performed, all eligible investigators were invited to attend the standard training. After resting for at least 5 min, the blood pressure of the right arm was measured using a standard mercury sphygmomanometer. Those who hid past medical history, yet with positive diagnostic result of hypertension were also set as patients with hypertension. The BMI was calculated by the weight dividing the square of the height (kg/m2). Professionals collected fasting venous blood samples of all participants in the morning. All blood samples were centrifuged and separated on site, and sent to the Central Laboratory of Hunan Provincial People's Hospital for testing. UA, SBP, DBP, ALT, BUN, Cr, TG, TC, HDL-C, LDL-C, ApoA, ApoB, CPR, FBG and Hcy were measured by standard laboratory procedures. All general demographic information and biochemical indicators were collected following standard protocols.
Definitions
Hypertension was defined as systolic blood pressure ≥ 140 mmHg and/or diastolic blood pressure ≥ 90 mmHg [18]. In subgroup analysis, we stratified age (≥ 60 years old and < 60 years old) and BMI (≥ 28 kg/m2 and < 28 kg/m2). Cut-off value of BMI was determined according to the Chinese definition of obesity [19]. The smoking and drinking status were also surveyed. Those who drank regularly for more than 6 months were assigned to the drinking group. Current smokers (at least one per day and consecutive cigarettes for 1 year) and former smokers were divided into current or former smokers group.
Statistical analysis
Categorical variable was expressed as number and percentage. Continuous variable was described using median and interquartile range (IR) for non-normally distributed data. Using non-parametric test for continuous variable and the χ2 test for categorical variable to compare differences between the four groups. Univariate logistic regression was used to analyze the effects of various factors on hypertension. Stratified analysis based on BMI and age to further explore the association between UA and hypertension. SPSS 20.0 software package (SPSS, Chica, Illinois, USA) was used to perform statistical analysis and P value < 0.05 was considered statistically significant.
Results
Basic information
Subjects were 54.50 (45.00, 63.00) years old, and 40.98% were male, 38.33% were hypertension. The median (IR) value of UA was 289 (231, 362) μmol/L. The median (IR) values of UA of each group were 200 (176, 216) μmol/L, 263 (249, 280) μmol/L, 325 (308, 340) μmol/L, 417 (390, 457) μmol/L in the four groups respectively. The median (IR) value of BMI of all participants was 23.13 (20.97, 25.28) kg/m2. There were statistically significant differences in all parameters among four groups, except for age (Table 1).
Except for TC and ApoB, other parameters were related to hypertension. Odds ratio (95% confidence interval) for the association of UA and hypertension was 2.397 (2.096, 2.740) among ≥ 60 years old comparing with among < 60 years old. Odds ratio (95% confidence interval) for the association of UA and hypertension was 2.535 (2.023, 3.177) among BMI ≥ 28 kg/m2 comparing with among BMI < 28 kg/m2 (Table 2).
Association between uric acid and hypertension
Without adjusting any confounding factors, In univariate logistic regression, odds ratios (95% confidence intervals) for the association of UA and hypertension were 1.745 (1.440, 2.114), 2.596 (2.149, 3.135) and 2.514 (2.081, 3.038) in other three groups respectively comparing with first group. After adjusting some confounding factors (age, gender, BMI, drinking history, smoking history, ALT, BUN, Cr, TG, TC, HDL-C, LDL-C, ApoA, ApoB, CPR, FBG, Hcy), Multivariable-adjusted odds ratios (95% confidence intervals) for the association of UA and hypertension were 1.652 (1.337, 2.042), 2.187 (1.761, 2.715) and 1.740 (1.375, 2.201) in other three groups respectively comparing with first group (Table 3).
Stratified analysis
Age
In the total subjects, the research objects of < 60 years accounted for 65.60%. The research objects of 31.16% were hypertension among < 60 years old, while the research objects of 52.03% were hypertension among ≥ 60 years old. Logistic regression showed the odds ratios for the association of UA and hypertension were 1.704, 2.660 and 2.349 in other three groups comparing with first group among < 60 years old. The odds ratios for the association of UA and hypertension were 2.226, 4.340, 5.898 and 6.557 in four groups respectively among ≥ 60 years old comparing with first group among < 60 years old (Fig. 1). Simultaneously, there was an interaction between UA and age (P < 0.001).

The association between UA and hypertension after age stratification (< 60 years old, ≥ 60 years old)
BMI
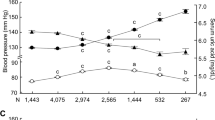
In the total participants, the subjects of BMI < 28 kg/m2 had 3669. The subjects of 36.39% were hypertension among BMI < 28 kg/m2, while sujects of 59.18% were hypertension among BMI ≥ 28 kg/m2. Logistic regression showed the odds ratios for the association of UA and hypertension were 1.659, 2.442 and 2.514 in other three groups comparing with first group among BMI < 28 kg/m2. The odds ratios for the association of UA and hypertension were 2.170, 5.260, 5.260 and 3.730 in four groups respectively among BMI ≥ 28 kg/m2 comparing with first group among BMI < 28 kg/m2 (Fig. 2). Simultaneously, there was an interaction between UA and BMI (P < 0.001).

The association between UA and hypertension after BMI stratification (< 28 kg/m2, ≥ 28 kg/m2)
Discussion
Few studies have explored the association between the UA and hypertension in the Chinese southern rural and urban communities population. Therefore, in this study, our purpose was to investigate whether the level of UA was related to hypertension in the Chinese southern population from Hunan. Simultaneously, our research also showed that UA was associated with hypertension. The association was stronger among subjects ≥ 60 years old or BMI ≥ 28 kg/m2. To our knowledge, this was the first study to report the association between UA and hypertension in the Chinese rural and urban communities population based BMI and age stratification. Among subjects ≥ 60 years old or BMI ≥ 28 kg/m2, the effect of UA on hypertension was stronger, and the odds ratio for the association of UA and hypertension was greater. There was an interaction between UA and age, there was also an interaction between UA and BMI. Age and BMI may exaggerate the effect of UA on hypertension.
Previous studies have suggested that UA was associated with hypertension. The result of Kuriyama et al. showd that high uric acid (UA) level was associated with the new development of hypertension among Japanese [20]. A cohort study conducted in the United States reported that 956 people developed hypertension during the 10-years follow-up period. As the UA quartile increased, the relative risk of hypertension (95% confidence interval (CI) was dose-dependent increase (P-trend < 0.05 in all models) [21]. In a cross-sectional study of 85,286 Japanese workers, it was found that hyperuricemia was significantly associated with hypertension in different gender, which existed between men with SUA ≥ 5.3 mg/dL and women with SUA ≥ 4.3 mg/dL after adjusting for age (years), BMI, dyslipidemia (yes), diabetes (yes), and alcohol consumption (nondaily drinker), smoking (nonsmoker) and estimated glomerular filtration rate (mL/min/1.73 square meters) [22]. The review of Johnson et al. supported that UA may play a causative role in the development of hypertension, vascular disease, and kidney disease [23]. Our study also showed that UA was significantly associated with hypertension in Chinese southern rural and urban communities population, which was consistent with the results of other studies based population of different countries.
UA is produced mainly in the liver and intestines because of the high activity of xanthine oxidase (XO) in these tissues. Xanthine oxidase (XO) is an enzyme that converts hypoxanthine to xanthine and xanthine to UA [24, 25], however, oxygen free radical produced by xanthine oxidase is one of the pathogenesis of hypertension [26]. Hypoxanthine is a precursor of UA which is metabolized by XO in vascular endothelium to UA, in which reactive oxygen generated during this process inactivates NO in vascular endothelium, resulting in endothelial dysfunction [27, 28]. In addition, there are some hypotheses that UA deposits on the walls of blood vessels with activating the renin-angiotensin system, inhibiting the release of carbon monoxide and increasing inflammation, as a result, the blood vessels contract later, which leads to hypertension [29, 30]. UA can stimulate a variety of factors into vascular smooth muscle cells, causing smooth muscle cell proliferation, resulting in secondary arteriosclerosis [31]. The above are about the mechanisms that UA may affect hypertension, which provides experimental evidence for the association between UA and hypertension.
In our study, the correlation between UA and hypertension in the four groups of subjects ≥ 60 years old was stronger than that of the four groups of subjects < 60 years old respectively. Age may exaggerate the effect of UA on hypertension. The study of Norvik et al. found that an increase in the baseline level of UA can independently predict the increase in blood pressure and fasting blood glucose in overweight subjects (BMI ≥ 25 kg/m2), but it can not predict the increase in blood pressure and fasting blood glucose in normal-weight subjects [32]. The division of BMI in our study was based on Chinese definition of obesity. The association between UA and hypertension based on BMI and age among Chinese southern rural and urban communities population needs more researches to explore and confirm.
Our research has many advantages. Firstly, this study was an observational study that included inevitable potential confusion, so we used strict statistical adjustment to minimize confusion to analyze the association between UA and hypertension by multivariate logistic regression. Secondly, this study was the first to analyze the association between the two based on BMI and age stratification among Chinese southern population from Hunan. On the other hand, there are limitations in this study. Firstly, our study was a cross-sectional study, it cannot get the causal association between UA and hypertension. Secondly, unknown confounding factors may affect the real association between the two.
Conclusions
Uric acid was significantly associated with the hypertension. The association was stronger among subjects ≥ 60 years old or BMI ≥ 28 kg/m2.
Abbreviations
- UA:
-
Uric acid
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- ALT:
-
Alanine aminotransferase
- BUN:
-
Blood urea nitrogen
- Cr:
-
Creatinine
- TG:
-
Triglyceride
- TC:
-
Total cholesterol
- HDL-C:
-
High density lipoprotein cholesterol
- LDL-C:
-
Low density lipoprotein cholesterol
- ApoA:
-
Apolipoprotein A
- ApoB:
-
Apolipoprotein B
- CPR:
-
C-reactive protein
- FBG:
-
Fasting blood glucose
- Hcy:
-
Homocysteine
References
Organization WH (2014) Global Status Report on non-communicable diseases.
Organization WH (2013) A global brief on hypertension: silent killer, global public health crisis.
Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J (2005) Global burden of hypertension: analysis of worldwide data. Lancet 365(9455):217–223
Wang J, Zhang L, Wang F, Liu L, Wang H (2014) Prevalence, awareness, treatment, and control of hypertension in China: results from a national survey. Am J Hypertens 27(11):1355–1361
Lawes CM, Vander Hoorn S, Rodgers A (2008) International society of hypertension. Global burden of blood-pressure-related disease, 2001. Lancet 371(9623):1513–1518
Imano H, Kitamura A, Sato S, Kiyama M, Ohira T, Yamagishi K, Noda H, Tanigawa T, Iso H, Shimamoto T (2009) Trends for blood pressure and its contribution to stroke incidence in the middle-aged Japanese population: the circulatory risk in communities study (CIRCS). Stroke 40(5):1571–1577
Okumura N, Kondo T, Matsushita K, Osugi S, Shimokata K, Matsudaira K, Yamashita K, Maeda K, Murohara T (2014) Associations of proteinuria and the estimated glomerular fifiltration rate with incident hypertension in young to middle-aged Japanese males. Prev Med 60:48–54
Fields LE, Burt VL, Cutler JA, Hughes J, Roccella EJ, Sorlie P (2004) The burden of adult hypertension in the United States 1999 to 2000: a rising tide. Hypertension 44(4):398–404
Forman JP, Choi H, Curhan GC (2007) Plasma uric acid level and risk for incident hypertension among men. J Am Soc Nephrol 18(1):287–292
Mehta T, Nuccio E, McFann K, Madero M, Sarnak MJ, Jalal D (2015) Association of uric acid with vascular stiffness in the Framingham heart study. Am J Hypertens 28(7):877–883
Cannon PJ, Stason WB, Demartini FE, Sommers SC, Laragh JH (1966) Hyperuricemia in primary and renal hypertension. N Engl J Med 275(9):457–464
Glantzounis GK, Tsimoyiannis EC, Kappas AM, Galaris DA (2005) Uric acid and oxidative stress. Curr Pharm Des 11(32):4145–4151
Kanbay M, Jensen T, Solak Y, Le M, Roncal-Jimenez C, Rivard C, Lanaspa MA, Nakagawa T, Johnson RJ (2016) Uric acid in metabolic syndrome: from an innocent bystander to a central player. Eur J Intern Med 29:3–8
Forman JP, Choi H, Curhan GC (2009) Uric acid and insulin sensitivity and risk of incident hypertension. Arch Intern Med 169(2):155–162
Mellen PB, Bleyer AJ, Erlinger TP, Evans GW, Nieto FJ, Wagenknecht LE, Wofford MR (2006) Serum uric acid predicts incident hypertension in a biethnic cohort: the atherosclerosis risk in communities study. Hypertension 48(6):1037–1042
Mazzali M, Hughes J, Kim YG, Jefferson JA, Kang DH, Gordon KL, Lan HY, Kivlighn S, Johnson RJ (2001) Elevated uric acid increases blood pressure in the rat by a novel crystal-independent mechanism. Hypertension 38(5):1101–1106
Mazzali M, Kanbay M, Segal MS, Shafiu M, Jalal D, Feig DI, Johnson RJ (2010) Uric acid and hypertension: cause or effect? Rheumatol Rep 12(2):108–117
Ma L, Li L, Tang Z (2017) Epidemiological characteristics of hyperhomocysteinemia and H-type hypertension in the elderly in Beijing. China Clin Exp Hypertens 39(7):640–644
Shu L, Zheng PF, Zhang XY, Si CJ, Yu XL, Gao W, Zhang L, Liao D (2015) Association between dietary patterns and the indicators of obesity among Chinese: a cross-sectional study. Nutrients 7(9):7995–8009
Kuriyama S, Maruyama Y, Nishio S, Takahashi Y, Kidoguchi S, Kobayashi C, Takahashi D, Sugano N, Hosoya T, Yokoo T (2015) Serum uric acid and the incidence of CKD and hypertension. Clin Exp Nephrol 19(6):1127–1134
Shankar A, Klein R, Klein BE, Nieto FJ (2006) The association between serum uric acid level and long-term incidence of hypertension: population-based cohort study. J Hum Hypertens 20(12):937–945
Yokokawa H, Fukuda H, Suzuki A, Fujibayashi K, Naito T, Uehara Y, Nakayama A, Matsuo H, Sanada H, Jose PA, Miwa Y, Hisaoka T, Isonuma H (2016) Association between serum uric acid levels/hyperuricemia and hypertension among 85,286 japanese workers. J Clin Hypertens (Greenwich) 18(1):53–59
Johnson RJ, Kang DH, Feig D, Kivlighn S, Kanellis J, Watanabe S, Tuttle KR, Rodriguez-Iturbe B, Herrera-Acosta J, Mazzali M (2003) Is there a pathogenetic role for uric acid in hypertension and cardiovascular and renal disease? Hypertension 41(6):1183–1190
Williams AW, Wilson DM (1990) Uric acid metabolism in humans. Semin Nephrol 10(1):9–14
Menenakos E, Doulami G, Tzanetakou IP, Natoudi M, Kokoroskos N, Almpanopoulos K, Leandros E, Zografos G, Theodorou D (2015) The use of serum uric acid concentration as an indicator of laparoscopic sleeve gastrectomy success. Int Surg 100(1):173–179
Khosla UM, Zharikov S, Finch JL, Nakagawa T, Roncal C, Mu W, Krotova K, Block ER, Prabhakar S, Johnson RJ (2005) Hyperuricemia induces endothelial dysfunction. kidney Int 67(5):1739–1742
Battelli MG, Polito L, Bolognesi A (2014) Xanthine oxidoreductase in atherosclerosis pathogenesis: not only oxidative stress. Atherosclerosis 237(2):562–567
Neogi T, George J, Rekhraj S, Struthers AD, Choi H, Terkeltaub RA (2012) Are either or both hyperuricemia and xanthine oxidase directly toxic to the vasculature? A critical appraisal. Arthritis Rheum 64(2):327–338
Johnson RJ, Sanchez-Lozada LG, Mazzali M, Feig DI, Kanbay M, Sautin YY (2013) What are the key arguments against uric acid as a true risk factor for hypertension? Hypertension 61(5):948–951
Bjornstad P, Paul WR, Sirota JC, Snell-Bergeon JK, McFann K, Rewers M, Rivard CJ, Jalal D, Chonchol MB, Johnson RJ, Maahs DM (2014) Serum uric acid and hypertension in adults: a paradoxical relationship in type 1 diabetes. J Clin Hypertens (Greenwich) 16(4):283–288
Kang DH, Park SK, Lee IK, Johnson RJ (2005) Uric acid-induced C-reactive protein expression: implication on cell proliferation and nitric oxide production of human vascular cells. J Am Soc Nephrol 16(12):3553–3562
Norvik JV, Storhaug HM, Ytrehus K, Jenssen TG, Zykova SN, Eriksen BO, Solbu MD (2016) Overweight modifies the longitudinal association between uric acid and some components of the metabolic syndrome: the tromso study. BMC Cardiovasc Disord 16:85
Acknowledgements
This study was sponsored by grants from the National Natural Science Foundation of China (Nos. 81202281, 81773530).We wish to thank the participants of this study and support staff who make the study possible. We would like to express our gratitude to the personnel of Laboratory Department in Hunan Provincial People's Hospital for their substantial assistance.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflicts of interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Niu, X., Chen, J., Wang, J. et al. Association between the uric acid and hypertension in community-based Chinese population: stratified analysis based on body mass index and age. J Thromb Thrombolysis 51, 1113–1119 (2021). https://doi.org/10.1007/s11239-020-02256-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11239-020-02256-8