
Abstract
Currently, single fresh frozen plasma (FFP) for clinical use is derived from individual blood donors. The objective of this study is to investigate the differences in single FFP units to make related strategies for improving FFP transfusion efficacy. 120 units of single FFP were selected randomly from Chinese PLA Clinical Blood Transfusion Center in Beijing, China. Single FFP samples were thawed in 37 °C water bath and were assessed immediately for total protein (TP), albumin (Alb), fibrinogen (Fg), factor V (FV), factor VIII (FVIII), antithrombin-III (AT-III) and protein C (PC). Multiple comparisons were employed to analysis the differences. The quality levels of 120 single FFP units showed wider ranges and presented normal distribution. Fg, FV and PC showed larger fluctuation range but TP, Alb, FVIII and AT-III showed smaller. The mean level of TP was 56.07 g/L and FVIII was 0.62 IU/mL. There were no significant differences to genders in single FFP units. FFP from younger people with 18–30 years old showed a trend towards reduced activity of coagulation factors, especially FV and FVIII. TP and Alb levels in FFP with type O were significantly higher than that in non-O type, but FVIII, AT-III and PC levels were lower in type O than that in non-O type. In a word, the whole quality of single FFP units from Chinese regional donors was acceptable, except FVIII. There were great differences of plasma proteins and factors in single FFP units, age and ABO blood type were main influence factors.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Highlights
-
There are considerable differences in clotting factors for fresh frozen plasma in clinical use.
-
It is important for transfusion centers to clarify the individual differences in single fresh frozen plasma.
-
Age and ABO blood type mainly influence the differences.
Introduction
Single fresh frozen plasma (FFP) is prepared from individual blood donor. Clinically, single FFP is considered as a common blood component to correct coagulation disorder or prevent hemorrhage and so on [1,2,3]. However, individual difference and preparation process both influence the quality of single FFP that may affect transfusion efficacy directly. In several national and international guidelines, the contents of FFP are checked by testing Factor VIII (FVIII), which is a representative of the coagulation system, and 0.70 IU/mL is the threshold value [4, 5]. Besides FVIII, other parameters of the coagulation system and the fibrinolytic system should be used to assess the influence of various factors on the quality of single FFP. In China Guideline, there are two quality requirements of plasma proteins or factors in FFP including total protein (TP) ≥ 50 g/L and FVIII ≥ 0.7 IU/mL for single FFP [5]. Moreover, studies showed that the quality of single FFP is related to age and gender of blood donor [6]. Studying the individual difference of single FFP from Chinese donors in specific area, therefore, it can be beneficial to examine the quality of FFP from Chinese population and contributed to recruit donor with higher plasma quality.
In this study, a large number of FFP samples from Chinese regional donors were randomly selected to test plasma proteins or factors level including the central proteins or factors of coagulation system and as the central proteins or factors of anti-coagulation system. The test results were analyzed the quality range, frequency distribution and individual difference including between blood groups, genders and ages to clear out the internal factors affecting FFP quality.
Methods
FFP source
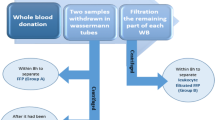
Units of whole blood were collected from Chinese people who came to donate blood in Chinese PLA Clinical Blood Transfusion Center, Chinese PLA General Hospital, Haidian District, Beijing, China. The related information of donor was recorded into blood donation system. Whole blood units were centrifuged at 4000×g for 10 min at 22 ± 2 °C using a centrifuge (Biofuge Primo R, Heraeus, Waltham, MA). The separated liquid plasma with 10 mL were filled into polycarbonate tubes and stored at − 80 °C rapidly as FFP in 6 h after collection. In FFP bank, 120 units of FFP in conservation period from 2016 to 2017 were selected randomly and donor information was extracted subsequently. FFP unit was thawed immediately in a shaking water bath (MultiTemp III, GE Healthcare Europe GmbH, Freiburg, Germany) at 37 °C. After thawed, FFP must be measured for plasma proteins or factors in 1 h.
Plasma proteins assays
Plasma proteins including TP and albumin (Alb) were measured on a fully automatic biochemistry analyzer (cobas c701/702, Roche, Mannheim, Germany) using the colorimetric method with a total protein test kit (Roche, Mannheim, Germany) and albumin test kit (Roche, Mannheim, Germany) respectively.
Coagulation factors assays
Fibrinogen (Fg), FACTORV (FV), FVIII were selected as main parameters in coagulation factors. Fg activity were measured on a coagulation analyzer (STA Compact, Diagnostica Stago, Asnieres, France) with the STA Compact using the Clauss clotting method with a fibrinogen kit (STA-fibrinogen 5 kit, Diagnostica Stago). FV and FVIII activity were measured on the IL coagulation system (Instrumentation Laboratory Company, Bedford, MA) using the prothrombin time assay with a FV-deficient plasma kit (Hemosil, IL Company, Bedford, MA), and the activated partial thromboplastin time assay with a FVIII-deficient plasma kit (Hemosil, IL Company, Bedford, MA).
Anti-coagulation factors assays
Antithrombin-III (AT-III) and Protein C (PC) were selected as main parameters in anti-coagulation factors. They were measured on the IL coagulation system (Instrumentation Laboratory Company, Bedford, MA) using automated chromogenic assay with a liquid antithrombin kit (HemosIL, IL Company) and a Protein C kit (HemosIL, IL Company).
Data statistical analysis
For each parameter, the assay was performed in three times and the arithmetic mean and standard deviation (SD) were calculated. Multiple comparisons using SPSS 15.0 were employed to analysis the mean differences between different groups. A P value < 0.05 (2-tailed) was considered statistically significant in the two paired groups.
Results
General characteristics of plasma proteins and factors in 120 single FFP units
Each parameter had a wide range and the frequency results showed they were near normal distribution (Fig. 1). Fg, FV and PC had larger fluctuation range and TP, Alb, FVIII and AT-III had smaller. The main observed parameters in China Guideline were TP with the mean level of 56.07 g/L and FVIII with the mean activity of 0.62 IU/mL (Table 1).

Frequency distribution of plasma proteins and factors in 120 single FFP units
Differences of single FFP units in gender groups
From data analysis, 120 FFP units were from 96 male donors and 24 females donors. No significant differences were found between different gender groups (Fig. 2).

Gender differences of plasma proteins and factors in 120 single FFP units. *P < 0.05
Differences of single FFP units in age groups
There were 42 units from donors with 18–30 years old, 57 units from 31 to 45 years old and 21 units from 46 to 60 years old in 120 single FFP units, respectively. There were significant age differences in certain parameter. In plasma proteins, Alb in FFP from young ages (18–30 years old) were higher than middle ages (31–45 years old) and old ages (46–60 years old) (Fig. 3a). In coagulation factors, however, FV and FVIII in FFP from young ages were lower than middle ages and old ages (Fig. 3b). In anti-coagulation factors, no significant differences were found in different age groups (Fig. 3c).

Age differences of plasma proteins and factors in 120 single FFP units. *P < 0.05
Differences of single FFP units in ABO blood type groups
There were 60 units with type A, 25 units with type B, 15 units with type AB and 20 units with type O in 120 single FFP units, respectively. In plasma proteins, the levels of TP and Alb in FFP with type O were significantly higher than those in other blood types (Fig. 4a). In coagulation factors, Fg in type O was higher than that in type B and AB, but FVIII in type O was lower than that in type B and AB. The levels of FV in type A and O were higher than that in type B and AB (Fig. 4b). In anti-coagulation factors, the activities in type O were significantly lower than that in others, especially AT-III (P < 0.05) (Fig. 4c).

Blood type differences of plasma proteins and factors in 120 single FFP units. *P < 0.05
Discussion
In order to FFP being effective, it is important to define the quality distribution, gender-associated differences, age-associated differences and blood type-associated differences of plasma proteins or factors in single FFP units derived from individual donors. Understanding the individual differences not only examine the quality of single FFP for clinical use regularly but also contribute to recruit preferred donors. Many factors, for instance, ages, genders, races, blood types and so on, were associated with changes in plasma proteins and the activity of proteins involved in the coagulation and anti-coagulation system [6,7,8,9,10,11]. Our study also demonstrated that conclusion and showed similar results.
In this study, it showed that the frequency distribution of plasma proteins or factors in 120 single FFP units was normal distribution meeting distribution requirement of big sample amounts (Table 1; Fig. 1). It was consisntent with other relative studies [12, 13]. Generally speaking, the whole quality of plasma proteins or factors in 120 single FFP units was acceptable. The mean value of TP with 56.07 g/L was above the China Guidelines (50 g/L). However, FVIII with 0.62 IU/mL was slightly blew the China Guidelines (0.7 IU/mL). This phenomenon was possibly attributed to the limitations of regional donor or the sample amount.
For gender, there was no significant differences on the tested parameters in single FFP and it was consistent with previous studies in other countries [6, 14, 15]. It indicated that it was not necessary to discriminate female donors in the view of FFP quality. For age, a significant age influence on coagulation factors can be found (Fig. 2). Younger people showed a trend towards reduced activity, especially FV and FVIII (Fig. 3b). The results were in a agreement with other studies [6, 16]. However, Alb level in young age group was higher than middle age group and older age group. Therefore, FFP from younger donor was not superior to older donor with the purpose of FFP transfusion for coagulant supplement. For ABO blood type, plasma proteins including TP and Alb in type O were significant higher than that in non-O type (Fig. 4a) and FVIII, AT-III and PC levels were lower in type O than in non-O types (Fig. 4b, c). Similar results were found in other countries, such as Canada and Brazil [17, 18]. The impact of ABO blood type on plasma proteins and factors levels was complicated in our study. Generally speaking, FFP with type O was not suggested as the first option to transfuse for factors supplement as compared to other blood types, but it was excellent for plasma proteins supplement. Many previous reports studied the quality of plasma and factors in individuals and our research studied that in single FFP units from individual donors. The similar results indicated that the preparation process of FFP was not able to significantly influence the differences of plasma proteins and factors in single FFP units.
There were limitations in this study, of course, such as the amount of single FFP units and the number of test parameters. In a word, it was suggested, in our this study, that there were significant differences of plasma proteins and factors levels in single FFP units from Chinese regional donors and the main influence factors were age and ABO blood type. Preferred recruitment for blood donor and preferred use in clinical may be available strategies. In order to address the problem of individual differences in single FFP completely, in the field of blood transfusion medicine, pooling plasma had been developed as alternative strategy, such as universal virus-activated plasma which had a uniform level of plasma proteins or factors in each unit [19,20,21]. That will be one of available strategies to achieve plasma precision dose.
Abbreviations
- Alb:
-
Albumin
- AT-III:
-
Antithrombin-III
- FFP:
-
Fresh frozen plasma
- Fg:
-
Fibrinogen
- FV:
-
Factor V
- FVIII:
-
Factor VIII
- PC:
-
Protein C
- TP:
-
Total protein
References
O’Shaughnessy DF, Atterbury C, Bolton Maggs P, Murphy M, Thomas D, Yates S, Williamson LM (2004) Guidelines for the use of fresh-frozen plasma, cryoprecipitate and cryosupernatant. Br J Haematol 126(1):11–28
Puetz J (2013) Fresh frozen plasma: the most commonly prescribed hemostatic agent. J Thromb Haemost 11(10):1794–1799
National Health and Family Planning Commission of the People’s Republic of China (2000) The Technical Criterion of Clinical Blood Transfusion
European Parliament. Commission directive 2004/33/EC. Official Journal of the European Union 2004, 2004
National Health and Family Planning Commission of the People’s Republic of China (2012) Quality requirements for whole blood and blood components
Madla W, Alt T, Jungk H, Bux J (2012) Fresh frozen plasma quality: relation to age and gender of blood donors. Vox Sang 102(2):116–124
Balleisen L, Assmann G, Bailey J, Epping PH, Schulte H, van de Loo J (1985) Epidemiological study on factor VII, factor VIII and fibrinogen in an industrial population—II. Baseline data on the relation to blood pressure, blood glucose, uric acid, and lipid fractions. Thromb Haemost 54(3):721–723
Balleisen L, Bailey J, Epping PH, Schulte H, van de Loo J (1985) Epidemiological study on factor VII, factor VIII and fibrinogen in an industrial population: I. Baseline data on the relation to age, gender, body-weight, smoking, alcohol, pill-using, and menopause. Thromb Haemost 54(2):475–479
Folsom AR, Conlan MG, Davis CE, Wu KK (1992) Relations between hemostasis variables and cardiovascular risk factors in middle-aged adults. Atherosclerosis Risk in Communities (ARIC) Study Investigators. Ann Epidemiol 2(4):481–494
Lowe GD, Rumley A, Woodward M, Morrison CE, Philippou H, Lane DA, Tunstall-Pedoe H (1997) Epidemiology of coagulation factors, inhibitors and activation markers: the Third Glasgow MONICA Survey. I. Illustrative reference ranges by age, sex and hormone use. Br J Haematol 97(4):775–784
Mari D, Coppola R, Provenzano R (2008) Hemostasis factors and aging. Exp Gerontol 43(2):66–73
Wang Z, Liu H, Dou M, Du X, Hu J, Su N, Wang Y, Zhang R, Li C.The quality changes in fresh frozen plasma of the blood donors at high altitude. PLoS ONE 2017 12(4):e0176390
Wang ZK, Dou MM, Du X, Ma L, Sun P, Cao HJ et al (2017) Influences of ABO blood group, age and gender on plasma coagulation factor VIII, fibrinogen, von Willebrand factor and ADAMTS13 levels in a Chinese population. PeerJ 5:e3156
Favaloro EJ, Soltani S, Mc Donald J, Grezchnik E, Easton L, Favaloro JW (2005) Reassessment of ABO blood group, sex, and age on laboratory parameters used to diagnose von Willebrand disorder. Am J Clin Pathol 124(6):910–917
Kadir RA, Economides DL, Sabin CA, Owens D, Lee CA (1999) Variations in coagulation factors in women: effects of age, ethnicity, menstrual cycle and combined oral contraceptive. Thromb Haemost 1999 82(5):1456–1461
Hamilton PJ, Allardyce M, Ogston D, Dawson AA, Douglas AS (1974) The effect of age upon the coagulation system. J Clin Pathol 27:980–982
Albánez S, Ogiwara K, Michels A, Hopman W, Grabell J, James P, Lillicrap D (2016) Aging and ABO blood type influence von Willebrand factor and factor VIII levels through interrelated mechanisms. J Thromb Haemost 14(5):953–963
Rios DRA, Fernandes AP, Figueiredo RC, Guimaraes DAM, Ferreira CN, Silva E, Carvalho ACS, Gomes MG, Dusse KB (2012) LMS. Relationship between ABO blood groups and von Willebrand factor, ADAMTS13 and factor VIII in patients undergoing hemodialysis. J Thromb Thrombolysis 33:416–421
Solheim BG, Chetty R, Flesland O (2008) Indications for use and cost-effectiveness of pathogen-reduced ABO-universal plasma. Curr Opin Hematol 15(6):612–617
Heger A, Brandstätter H, Prager B, Brainovic J, Cortes R, Römisch J (2015) Universal pooled plasma (Uniplas(®)) does not induce complement-mediated hemolysis of human red blood cells in vitro. Transfus Apher Sci 52(1):128–135
Wang S, Zhou W, Zhuang Y, Zhang D, Li H, Wang D (2012) Study on preparation of universal plasma in Chinese Han population. Transfus Apher Sci 47(2):167–170
Acknowledgements
We thank experimental supports of Fengyan Fan, Liping Sun, Dongqing Zhang from Department of Blood Transfusion, Chinese PLA General Hospital and Ping Di from Department of Clinical Laboratory, Chinese PLA General Hospital.
Funding
This study was supported by the CAMS Innovation Fund for Medical Sciences (CIFMS, No. 2017-I2M-3-021), the Sichuan Provincial Science and Technology Project (No. 2017JY0064), and the Military Major Special Project (AWS11J007-08).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors have disclosed no conflicts of interest.
Ethical approval
The Institutional Ethics Committee of CPGH approved this study.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Zhu, L., Li, C. & Wang, D. Individual differences of plasma proteins and factors in fresh frozen plasma from Chinese regional blood donors. J Thromb Thrombolysis 47, 420–426 (2019). https://doi.org/10.1007/s11239-018-1789-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11239-018-1789-9