
Abstract
Based on analysis of long-running panel surveys in Germany and Australia, we offer a revised assessment of the relationship between subjective well-being (happiness, life satisfaction) and longevity. Most previous research has reported a linear positive relationship; the happier people are, the longer they live (Diener and Chan in Appl Psychol Health Well-Being 3:1–43, 2011. https://doi.org/10.1111/j.1758-0854.2010.01045.x). Results from these two panels indicate that, if a linear model is assumed, the standard positive relationship between life satisfaction and longevity is found. However, an alternative viewpoint merits consideration. It appears that the relationship between happiness and longevity may be non-linear. The evidence is strong that unhappy people die young. Otherwise, across the rest of the distribution, happiness appears to make no difference to longevity. Our findings are consistent using alternative methods of estimation, and are robust with or without controlling for a range of variables known to affect longevity, including socio-economic variables, behavioral choices (e.g. exercise, smoking) and health status.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Do happy people live longer? Most previous papers report a linear positive relationship between longevity and life satisfaction (LS), happiness or other measures of subjective well-being (for a comprehensive recent review see Diener and Chan 2011). However, several studies, notably those based on the longitudinal Terman study of the gifted, conclude that happiness is unrelated to longevity, or even that very happy people may die younger than average (Friedman et al. 1995; Martin et al. 2002; Friedman and Martin 2011).
In this paper we analyse data from two long-running panels in Germany (Frick et al. 2007) and Australia (Watson and Wooden 2004). Our results suggest that the relationship between LS and longevity is probably non-linear. People with low levels of LS die young, but otherwise LS appears to be unrelated to longevity. There is no evidence that high, or even very high LS individuals live longer than people who report average levels.
It should be emphasised that, if we had analysed the panel datasets assuming a linear relationship, as in many previous studies, we would have obtained the standard result that the happier a person is, the longer he or she lives. Our approach departs from the standard approach in two important aspects. First, as mentioned, we allow for the possibility of non-linearity. Second, in respect of panel respondents who have died, we eliminated from consideration their LS in the last 3 years of life. This was because it seems likely, and previous research based on the German panel data has confirmed (Gerstorf et al. 2010), that many people are very unhappy in the last few years of life as their health deteriorates. Of course, some people die suddenly and so presumably retain their normal level of LS until the end. But because those whose health seriously declines also suffer a decline in LS, it may seriously bias results in favour of finding a positive link between LS and longevity if the last few years of life are included. It appears that in most, although not all previous research, they have been included.
1.1 Previous Biomedical and Social Science Research on Happiness and Longevity
There is a vast literature on the correlates and potential causes of longevity; research presumably motivated by a desire in most cultures to lengthen human life. There are two main types of research: biomedical and social science. This paper is in the second category, but it is important to take account of lessons from biomedical research. Biomedical researchers base their human research largely on an animal model of the life cycle (Kaeberlein and Martin 2015). They view aging and dying as developments that start early in life (not just in old age), and they show that the processes of aging, and the shape of survival curves, are the same across most species, including fruit flies, rats, monkeys and humans (Garvrilov and Gavrilov 2006). In humans mortality begins to increase at age 10 and then doubles every decade (Garvrilov and Gavrilov 2006; Kaeberlein and Martin 2015). Twin studies have estimated that approximately 20–30% of the variation in human lifespan is related to genetics, with the rest due to individual behaviours and environmental factors (Hjelmborg et al. 2006).
Numerous biomedical studies have investigated the effects of dietary, hormonal and drug interventions on animal longevity. In some cases, after positive results from animal studies, similar interventions have been initiated with human subjects. A major current trial, conducted by the U.S. National Institutes of Health, involves assessing the effects of the diabetes drug, metformin, on aging; the drug has previously been shown to increase longevity in rats (ClinicalTrials.gov 2015).
A period of peak research activity was at the end of the nineteenth century—the fin de siècle—when the Nobel Prize winning biologist, Elie Metchnikoff, led the movement known as ‘life-extensionism’, partly based on his own cell theory of immunity. There was another upsurge of interest in the inter-War years, when some prominent men were persuaded that having a vasectomy would increase both their potency and life span. The belief was that, since testosterone is an immunosuppressant, reducing the supply would increase longevity. Much was made of limited evidence about the lifespan of eunuchs employed in Asian imperial courts, who were reported to live significantly longer than males who managed to avoid castration (Min et al. 2012). Freud had a vasectomy at 70, but said, “It did nothing for me.” In contrast, the Irish poet, William Butler Yeats, reported that for him the surgery had been a great success.
1.2 Social Science Research
A potential problem in the social science literature is that researchers deploy differing concepts and measures of what, generically, is usually termed subjective well-being (SWB). As previously mentioned, the dependent variable in this paper is life satisfaction (LS). However, other researchers (see below) have employed concepts and measures of positive affect, ‘cheerfulness’ and self-reported happiness.
Like the biomedical literature, the social science literature canvasses a wide range of possible correlates and causes of longevity. Clearly, in order to assess the effects of SWB on longevity, it is desirable to collect longitudinal data in which health and other potential covariates of longevity, as well as SWB, are measured at least once in the years prior to death. All of the studies reviewed here meet these criteria.
One of the first studies of this kind was based on the Dutch Longitudinal Study of the Elderly (Deeg and van Zonneveld 1989). A panel of seniors (N = 3149) was recruited in 1955–57, ranging in age from 65 to over 80 years old. The last follow-up was in 1983, when most had died. Controlling for health at baseline (assessed by physicians) and a standard set of socio-economic characteristics, Deeg and van Zonneveld found a weak but statistically significant association (p < 0.05) between longevity and LS. The relationship was stronger for men than women. It was estimated that, for men aged 70, an increase in satisfaction levels of one standard deviation above the mean extended life by 20 months. It appears that subjects who died in the first few years after baseline measures were taken were included in the study, so it can be inferred that, in some cases, LS measures taken shortly before death were used as explanatory variables; a potential cause of Type 1 error.
A similar criticism cannot be levelled at findings from the well-known Nun Study in the US. Starting in 1986, the study has followed the lives of 678 nuns belonging to the School Sisters of Notre Dame. Baseline measures of cognitive function were taken soon after the study started, partly by analysing autobiographical essays written by the nuns. The main focus of research was on the precursors of Alzheimer’s disease (National Institute of Aging 1996), but the study also found a significant association (p < 0.001) between longevity and the frequency of ‘positive affect’ expressions in the nuns’ essays (Danner et al. 1991). In the Nun Study the effects of potentially confounding variables were largely eliminated due to the homogeneity of the sample, and it is entirely clear that no positive affect measures were taken in the years immediately preceding death.
In the last two decades longitudinal studies claiming a positive link between measures of SWB and longevity have been reported for samples in Germany (Guven and Saloumidis 2009), Japan (Shirai et al. 2009), Russia (Zhang and Huang 2007) and the U.S. (Ostir et al. 2000; Chida and Steptoe 2008; Xu and Roberts 2010). Scandinavian studies have yielded mixed results, mostly finding a positive relationship (Koivumaa-Honkanen et al. 2001, 2002, 2004; Lyrra et al. 2006), but with one study concluding that only men, but not women, who rate low on LS die young (Koivumaa-Honkanen et al. 2000). The most comprehensive recent review of the literature on SWB, health and longevity concludes with the following ‘take-home message’ (Diener and Chan 2011):
There now are sufficient studies on all-cause mortality and certain diseases to draw relatively strong conclusions. Our overall conclusion is that the evidence for the influence of subjective well-being on health and all-cause mortality is clear and compelling, although there is much more uncertainty about how various types of SWB influence specific diseases, and about the role of the possible mediating processes. The effect sizes for SWB and health are not trivial; they are large when considered in a society-wide perspective. If high SWB adds 4 to 10 years to life compared to low SWB, this is an outcome worthy of national attention.
Impressive as the evidence marshalled by Diener and Chan is, there remain contrary findings. In 2011, the same year as Diener and Chan’s review was published, the final report of the longitudinal Terman Study of the Gifted appeared (Friedman and Martin 2011). The researchers claimed that the personality trait of conscientiousness had a strong effect on the longevity of their intellectually gifted subjects (see also Friedman et al. 1995), but that ‘cheerfulness’ was unrelated to longevity, and in some cases appeared to shorten life. Specifically, they reported that subjects who were reported (by teachers) to be ‘very cheerful’ children took too many risks in later life. They smoked, drank too much, drove too fast, did not comply with health treatments… and so reduced their lifespan (see also McCarron et al. 2003). Somewhat similar results were reported in the longitudinal Grant Study of Harvard graduates (Vaillant 1977). The most successful Harvard men in career terms, and also the longest lived, were those characterised by conscientiousness and perseverance.
Finally, recent evidence from the prospective Million Women Study in the UK was interpreted as showing that self-reported happiness does not affect longevity, because once health was ‘controlled’, the relationship with longevity was no longer statistically significant (Liu et al. 2016).Footnote 1 A questionable assumption here, discussed in the next section, is that health was treated only as a cause of happiness, not also as a potential consequence.
1.3 Our Approach in Analysing the Panel Data
Our approach in analysing the two national panels was driven by awareness of the divergent research findings just reviewed. We initially avoided statistical analysis and began by graphing the ages at which people with high, medium and low levels of LS died. Graphic evidence immediately indicated that, in both countries, people with low levels of LS die young, but there did not appear to be much (if any) difference between medium and high LS groups. Obviously, these simple results could have been misleading, and might have been negated when appropriate statistical analysis was undertaken, with controls in place for other variables besides LS which affect longevity.
However, it is far from straightforward to decide what to include as ‘controls’ in assessing the net effect of LS on longevity. In previous research, depending on data availability, four main sets of ‘control’ variables have been deployed: (1) socio-economic characteristics (2) behavioural choices (e.g. social activities, taking physical exercise, smoking, obesity) (3) personality traits and (4) measures of health (e.g. physician assessments, disability status, physical fitness).
There is a serious danger of ‘over-controlling’, primarily because of possible two-way relationships between LS and some of these variables. Take health. If it is the case that happiness increases longevity, then this must almost certainly be because it improves health (unless we are to believe that happy people stay alive by sheer will power). So it is likely that there is a two-way relationship between health and LS. Good health enhances LS, and high levels of LS may enhance health. Issues of two-way causation are difficult to tackle, even with high quality panel data. That said, it is worth recording that several studies, based on panel data, report significant two-way causation between LS and health (Mathison et al. 2007; Headey and Muffels 2015).
Similar issues arise in relation to socio-economic characteristics and behavioural choices. It is quite likely that happy people, partly as a consequence of being happy, are more successful than unhappy people in their careers and so earn higher incomes (Diener et al. 1999). Happy people may be more likely to get married and stay married (Argyle 2002). Turning to behavioural choices, several studies indicate that LS appears to be a cause as well as a consequence of taking more or less physical exercise, of having better or worse social networks, and of greater or lesser engagement in social activities with family and friends (Lance et al. 1995; Scherpenzeel and Saris 1996; Headey and Muffels 2015). It seems reasonable to suggest that, in some cases, changes in LS might also be both a cause and consequence of smoking, and perhaps of obesity.
Bearing these issues in mind, we will present results based on two types of model. In our base models only gender and age will be included as ‘controls’ in equations linking LS to longevity. Then, in extended models, we will include ‘controls’ for all categories of variables discussed above. The base models may be regarded as giving upper limit estimates of the effects of LS on longevity, while the extended models give lower limit estimates.
The rest of the paper is as follows. In Sect. 2 we describe the national panels from which data are drawn. Also described are specially constructed measures of ‘quasi-lifetime’ LS, and ‘quasi-lifetime’ measures of other explanatory variables. The point of the quasi-lifetime measures is to enable assessment of long term effects, and to avoid assessing the impact of explanatory variables primarily in the years immediately preceding death.
The main technique of data analysis used in the paper—Cox proportional hazards analysis—is also described in the Methods section. The Results section gives our main results relating to the non-linear relationship between LS and longevity. We also include some sensitivity analyses, using alternative model specifications to assess whether non-linear results are confirmed or falsified. There is also a brief section on an issue, raised by reviewers, of whether the finding that low LS individuals die young could be primarily due to mental illness, rather than low LS. The final section discusses some implications of our results for LS theory.
2 Methods
The methods section is in three parts: data, measures, and techniques of data analysis.
2.1 Data: German and Australian National Panels
Data come from long-running German and Australian national household panel surveys. The German (SOEP) panel began in 1984 in West Germany with a sample of 12,541 respondents (Frick et al. 2007). Interviews have been conducted annually ever since. Everyone in the household aged 16 and over is interviewed. The representativeness of the panel is maintained by interviewing ‘split-offs’ and their new families. So when a young person leaves home (‘splits off’) to marry and set up a new family, the entire new family becomes part of the panel. The sample was extended to East Germany in 1990, shortly after the Berlin Wall came down, and since then has also been boosted by the addition of new immigrant samples, a special sample of the rich, and recruitment of new respondents partly to increase numbers in policy groups (e.g. welfare beneficiaries). There are now over 60,000 respondents on file, including some grandchildren as well as children of the original respondents. The main topics covered in the annual questionnaire are family, income and labor force dynamics. A question on life satisfaction has been included every year.
Clearly, information about the age at which respondents died is crucial for this research. The survey managers in Berlin, like all who run panels, keep a ‘master file’ which records when each respondent entered the panel and when he/she left and why. Most of the information about reasons for leaving is acquired by interviewers when they try to re-contact respondents. Information about deaths comes from relatives and neighbours, and in recent years has been supplemented by official records. The panel started in 1984; since then 4716 respondents are recorded as having died. The data are incomplete, especially for earlier years. It is obvious from the last recorded ages of respondents that some who must have died have not had their year and age of death recorded. It is of course known when these individuals exited the survey. In our analyses they are assumed to be alive in their year of exit, and are treated as right-censored in survival analysis.
The Australian (HILDA) panel began in 2001 with a sample of 13,969 individuals in about 7700 households (Watson and Wooden 2004). Interviews were achieved in 61% of in-scope households. In this panel all household members aged 15 and over are interviewed. Using following rules similar to the German panel, individuals who split off from their original households continue in the panel, and members of their new households join it. In 2015 (the latest available year), interviews were conducted with 17,606 individuals in 9631 households. It may be noted that, as happens in all panels with good retention rates, the sample size is now increasing. That is, the number of individuals added to the panel each year, via split-offs and young people turning 15, exceeds the number who die, cannot be traced, or drop out by refusing an interview. The HILDA panel was supplemented in 2012 with a new sample, including adequate numbers of recent immigrants.
The HILDA survey managers have compiled complete records of respondent deaths. Most information comes from interviewers, as in Germany, but all other cases have been checked using the National Register of Deaths. Since 2001, 1274 respondents are recorded as having died.
2.2 Measures
2.2.1 Life Satisfaction (LS) and ‘Lifetime’ Life Satisfaction (LLS)
In both the German and Australian panels, LS is measured on a 0–10 scale, running from ‘extremely dissatisfied’ to ‘extremely satisfied’ (German mean = 7.31 SD = 1.73; Australian mean = 7.89 SD = 1.47).
In order in order to investigate our central research issue we needed a measure which would enable us to assess how satisfied with life panel members were, on average, over a long period. We needed to measure long-term, or one might say, ‘quasi-lifetime’ LS. Our proxy lifetime measure, for each panel member, is his/her average (mean) LS rating for the years in which the LS question was answered. Panel members were excluded from analysis if they reported fewer than three LS ratings; the median German panel member reported eight times, and the median Australian six times. Further, for reasons already explained, in calculating ‘lifetime LS’ (henceforth LLS), we excluded LS ratings in the last 3 years of life in the case of respondents known to have died.
Individuals were then divided into three groups based on their LLS rating:
-
The top quartile (High LLS)
-
The middle two quartiles (Medium LLS), and
-
The bottom quartile (Low LLS).
2.2.2 Health, Disability and Obesity
In addition to LLS, the other explanatory variables in our models are health, disability and obesity, plus a range of variables described below which are included primarily as ‘controls’.
Clearly, the proximate reason for dying is usually poor health. Hence, if one controls for health measures taken shortly before death, estimates of the effects of LS and other potentially explanatory variables are likely to be biased downwards. However, there is a case for including what are usually referred to as ‘baseline’ measures of health. Ideally, baseline measures should be taken at a certain fixed age (e.g. age 30). This was not feasible for the panel surveys, which respondents join at all ages. As a practical matter, we make use of the first available health measures for each respondent and refer to them as measures of ‘initial health’.
Different initial health measures were constructed for the two national panels. One of the main health measures included in the German panel since its inception is ‘disability’. In Germany everyone has an official disability rating based on a medical examination. Of course, most people have a rating of zero. For inclusion in analyses here, we constructed a binary variable, with one denoting disability (any rating above 0) and 0 denoting no disability. A question about disability is also asked in the Australian panel, but ratings are subjective. It is amusing that, despite Australia having a considerably younger population than Germany, four times as many people claim a disability (27.1 vs. 6.8%). So instead of using this measure of disability for Australia, we use a physical functioning index from the well regarded SF-36 Health Survey (Ware et al. 2000). The index is composed of ten items relating to the difficulty subjects report in performing daily tasks (e.g. difficulty in ‘lifting or carrying groceries’; ‘climbing several flights of stairs’).
Also included in analyses of the German (but not Australian) data is a measure of ‘initial obesity’ (1 = obese 0 = not obese).Footnote 2 Obesity has been linked to early death (Kitahara et al. 2014).
2.3 Socio-economic Variables
2.3.1 Age
The role of age in our survival analyses needs to be explained. Age is used as the time duration variable. This may seem unusual, but in fact it is standard in survival analysis to select, as one’s duration measure, a variable (preferably the variable) strongly related to the outcome/the hazard that one is accounting for (Allison 2014).Footnote 3 Survival analysis is a non-linear technique, so one consequence of using age as the duration variable is that hazard ratios are estimated to give the best linear or non-linear fit between age and longevity, net of other variables in the equation.
Other fairly standard socio-economic variables included in our models are gender, partner (marital) status, years of education, income and employment status. It was essential to include employment status because numerous studies, including twin studies, have documented that individuals with a history of unemployment tend to die young (Brenner and Mooney 1983; Voss et al. 2004).
2.4 Behavioural Choices
Four behavioral choices—physical exercise, social participation with friends and family, smoking and church attendance—are included in our analyses. We expected to find a positive association between longevity and exercise (Gremeaux et al. 2012), and also between longevity and social participation (Diener and Chan 2011). Smoking, of course, is known to shorten life. Regular church attendance has been linked to longevity (Strawbridge et al. 1997; Headey et al. 2014).
In both panels respondents are asked about frequency of exercise per week. Respondents’ self-reports were averaged for the years up to and including the current survey year. Social participation is measured in both the German and Australian panels by a question asked on a 5-point scale about frequency of getting together with friends and family.
The smoking history variables are constructed differently for Germany and Australia. The German file includes information about each respondent’s smoking history, including for years before he/she joined the panel. In the Australian file, data on smoking are only available for years in which respondents were already in the panel. So the Australian measure understates years spent smoking.
Church attendance is measured in SOEP on a 1–5 scale running from ‘never’ to ‘at least once a week’. Respondents were grouped into ‘very frequent’ attenders (5 on the scale), ‘moderately frequent’ (points 3–4) and ‘not frequent’ (points 1–2).Footnote 4
The construction of these behavioural choice variables excludes the last 3 years of life for respondents who died during the study period.
2.5 Personality Traits
In principle, it would have been desirable to include personality traits in our models, because (as previously mentioned) the conscientiousness trait has been reported to increase longevity (Friedman and Martin 2011). Unfortunately, the Big Five traits—neuroticism, extroversion, openness, agreeableness and conscientiousness—were not measured in either the German or the Australian panel until 2005 (Costa and McCrae 1991). This meant that, if we had included them in our models, we would have had to exclude all panel members who died before 2005. To do so would have severely reduced the number of deaths included in analyses; by more than half in the German sample and nearly half in the Australian one.
2.6 Data Analysis: Cox Proportional Hazard Estimation
Survival analysis is the usual method of analysing risks in datasets which include numerous right-censored cases; that is, cases to whom the risk event (death) has not happened by the end of the study period. Cox proportional hazard analysis has become the preferred and accepted method of doing survival analysis in social science research, when the main interest is in the covariates of the hazard function and not in the shape of the function, or in making predictions about future survival (Friedman et al. 1995; Allison 2014).
Assuming that time is continuous, we define the survival function as:
where F(t) is the distribution function of the random event, death. The survival function simply states the probability of an individual surviving for longer than time t. Then, letting f(t) = F′(t) be the density function, we define the hazard rate as:
The hazard rate gives the rate at which an individual dies at time t + delta, given that the individual has survived until t.
To account for the effects of covariates, denoted as vector X, the Cox proportional hazard model specifies a hazard function of the form:
where h0(t) is the baseline hazard function and β is a vector of parameters to be estimated.
The key assumption underlying the Cox model is constant proportional hazard over time between any given pair of respondents (Cox 1972). This is a powerful assumption, which allowed Cox to develop a model with two main advantages over previous parametric approaches. First, it is not necessary for the researcher to know and specify the exact distribution of the hazard function. It is not necessary, for example, to know whether the hazard follows an exponential curve, a Weibull distribution, or a Gompertz distribution. Secondly, it allows the researcher, if needed, to include time-varying explanatory variables and not be restricted, as in most parametric analysis, to variables which are deemed to be constant over time.
The key assumption of constant pairwise hazard ratios can be checked, and in practice is often not met. However methodological research, based on large scale simulations, has shown that even substantial violations of the assumption usually make little difference to results of main interest. This is because breaches of the assumption are usually due to omitted explanatory variables (‘unobserved heterogeneity’) rather than due to variables already in one’s model (Wooldridge 2010; Allison 2014). Some of our analyses breached the proportional hazards assumption. It was reassuring, in this context, to find that alternative estimators yielded results very close to the Cox estimates (see below).
A few points about our data set-up should be mentioned. Individuals were considered to be ‘at risk’ of the hazard occurring (i.e. dying) from the first survey year in which they answered a LS question. They were then considered to ‘exit’ their period of risk when they died, or when they dropped out of the panel survey. In the case of individuals who are still in their national panel, the last available year in which LS was reported is taken as their ‘exit’ year. For individuals who dropped out of the panel some years before they died (a common occurrence), missing data for explanatory variables in the years immediately prior to death were ‘filled in’, using the last available measures for those respondents. For example, if a respondent was married when he or she dropped out of the survey, he or she was classified as married in the years up to death. ‘Filling in’ data in this way is routine in survival analysis; most software packages provide a standard option for doing so.
3 Results
This section first presents our main results showing a non-linear relationship between LS and longevity. Then it will be shown that, if we had adopted the standard approach of assuming a linear relationship, we would have obtained the standard result in the literature. In other words, the data we use appear not to differ in any material way from data analysed in previous studies. The difference in results is primarily due to allowing for a non-linear relationship.
3.1 The Non-linear Relationship Between LS and Longevity
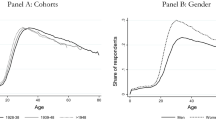
The first clue that the standard result may be incorrect came from straightforward visual evidence depicting the death rates of respondents in the high, medium and low LLS groups. The graphs in Fig. 1 show Kaplan–Meier survival estimates and Nelson-Aalen cumulative hazard estimates for respondents in these three groups. Both these standard techniques provide smoothed curves of survival functions (StataCorp 2017). For the purpose of illustration, the graphs are only drawn for people age 60 years and over, since death rates below the age of 60 are similar across the three LLS groups.

Survival and hazard functions: high, medium and low LLS groups. a Kaplan–Meier survival function, b Nelson–Aalen cumulative hazard, c Kaplan–Meier survival function, d Nelson–Aalen cumulative hazard
These survival and hazard estimates give a first indication that individuals with low LLS die younger than the other two groups. There appears to be almost no difference in longevity between the medium and high LLS groups. Log-rank Chi square tests of the equality of survivor functions confirm that the low LLS group dies significantly younger than the other two groups (p < 0.001).The survival functions of the Medium and High LLS groups are not significantly different from each other, even at the 0.01 level. The pattern of results is much the same for men and women, except that women are at lower risk of dying at all ages. Of course, it remains to be seen whether these initial findings will hold when additional covariates associated with longevity are included.
Our main results are given in Table 1. These are Cox proportional hazard ratios in which the reference group is the Medium LLS group. So the hazard ratios for the low and high LLS groups should be read as being relative to that group. Column (1) of Table 1 gives results for the base model, in which there are controls only for gender and age. The second column gives results for extended model I in which controls have been added for other potential predictors of longevity, but excluding initial health conditions. Column (3) gives results for extended model II in which ‘initial health’ is also controlled.
In both countries base model estimates indicate that the Low LLS group has much higher hazard rates (conditional on gender and age) than the other two groups. In Germany the hazard ratio for the Low LS group is 1.534 (p < 0.001), and in Australia it is 1.537 (p < 0.001). When additional predictors (but not initial health) are included in extended model I, differences between the low LLS and medium LLS groups are somewhat smaller but still statistically significant. In Germany the hazard ratio for the Low LLS group is now estimated at 1.341 (p < 0.001), and in Australia it is 1.307 (p = 0.004). When measures of initial health are also included, the hazard ratio for the Low LLS group in Germany is estimated to be 1.287 (p < 0.001), and in Australia it is also coincidentally 1.287 (p = 0.007). As noted earlier, base model estimates may be viewed as upper limit estimates of the effect of LS on longevity. Extended model estimates probably approach (or conceivably go below) the lower limit, because covariates have been included which may be consequences as well as causes of LS.
A full set of results is shown in the “Appendix”. Smoking has easily the strongest negative effect on longevity, with high hazard ratios for individuals in both countries who smoked for three or more years. Variables positively linked to longevity are having a high income, exercising frequently, and actively participating in social activities (an active social life with family and friends).
3.2 Alternative Estimators
We checked the robustness of our results by using several alternative estimation methods. We estimated parametric survival functions characterised by (a) a Gompertz distribution (b) a Weibull distribution. Also estimated were two discrete-time survival models: a random effects logistic model and a complementary log–log (cloglog) model. Results are reported in Table 2, which shows hazard ratio estimates from extended model II; the model with all available controls in place.
It is clear that all four alternative models produce estimates very close to those of the Cox proportional hazard model. For the German panel, similar hazard ratios and p values were obtained regardless of the estimation method used. Similar results were also obtained for the Australian panel with minor exceptions relating to the High LLS group, for whom hazard ratios were somewhat higher in the discrete time logistic model (1.158, p = 0.058) and the cloglog model (1.152, p = 0.052) than in other models.
3.3 Standard Assumptions Yield Standard Results
We next show that, if the German and Australian data had been analysed using the standard linear approach adopted in most previous studies, the standard results found in the literature would have (apparently) been confirmed. The standard approach simply assumes that a (generalised) linear relationship exists between LLS and longevity. It then follows that, if a positive relationship is found, higher levels of LLS imply longer life.
In Table 3 we report results for extended model II, assuming linearity. In column (1) the measure of LLS excludes the last three years of life for individuals who died during the data period, whereas all years are included in column (2).
These results make it look as if each increment in LLS is associated with an increment in longevity. The evidence in column (1) would usually be interpreted as showing that each one-point increment in LLS lowers the risk of dying in Germany by 7.3% and in Australia by 8.5%. If the last 3 years of life of deceased individuals are included (column 2), the linear results appear stronger still.
3.4 Sensitivity Analyses Using Cox Proportional Hazard Models
We undertook additional sensitivity analyses to test whether the apparently non-linear relationship between LLS and longevity is sensitive to reasonable variations in the specification of the Cox proportional hazard model.
Could it be the case that our results are due to dividing survey respondents into just three groups: High, Medium and Low LLS? To investigate this possibility, we made alternative cuts, dividing the sample into quintiles, and then into deciles. The upshot was that results were essentially unchanged. The bottom LLS group, however defined, was much shorter-lived than the middle group or groups. There was also no evidence that the top quintile or decile - very happy people—lived longer than average. Table 4 gives a summary of Cox proportional hazard results with respondents in the German and Australian samples divided into quintiles of LLS. Estimates from the extended model II specification indicate that Germans in the lowest LLS quintile were 1.283 times more likely to die than those in the middle quintile (reference group). The hazard ratio of Australians in the lowest LLS quintile was 1.460 times the ratio of the middle quintile.
A second sensitivity test was to see whether results changed if more than just the last 3 years of life were excluded. German research indicates that the decline in LS is mainly in the final 3 years but results are not completely clear (Gerstorf et al. 2010). To explore this possibility, we exclude the last 5 years of life for individuals who died.
The evidence in Table 5 indicates that, even if this longer period is excluded, it is still the case that low LS people die young and high LS people do not live longer than average.
3.4.1 Mental Health
Reviewers suggested to us that the association between low LLS and shorter lifespan may mainly be a reflection of mental ill-health, rather than low LLS. This hypothesis can be checked in the Australian panel but not the German panel, since only the former has included a mental health index—the SF-36 mental health index—since the survey started (Ware et al. 2000). The index is scored 0–100 with a high score indicating good mental health, and a score under 50 potentially indicative of a clinical diagnosis (2000).Footnote 5 Respondents were divided into four groups on the basis of their mean annual scores (excluding the last 3 years of life for those who had died). Individuals who scored under 50, about 10% of the sample, formed the ‘very low mental health’ group. The remaining panel members formed three groups of approximately equal size: low, medium and high mental health.
Table 6 reports Cox proportional hazards estimates for extended model II, but with the addition of mental health as another potential predictor of longevity.
It can be seen that, net of other covariates, hazard ratios for mental health groups are not statistically significant, except for the ‘high’ mental health group, whose hazard ratio is estimated at 0.771 (p = 0.004). Importantly, controlling for mental health did not substantially affect the hazard ratios of LLS groups. The estimated hazard ratio for individuals with low LLS was 1.272 (p = 0.014).
4 Discussion
In summary, results from the German and Australian national panels indicate that the relationship between happiness and longevity is non-linear. People in the bottom quarter of the LS distribution die considerably younger than the rest of the population. This conclusion holds in models controlling only for gender and age—controls that no-one would argue against—and also in models with a larger set of controls. In the latter models, the relationship remains strongly statistically significant in both Germany (p < 0.001) and Australia (p = 0.007). It remains our view, however, that many (perhaps all) of these additional controls could be partly consequences of LS, not just causes. This caveat applies particularly to variables measuring physical exercise, participation in social activities, smoking and perhaps obesity. It also likely that initial health (also included as a control in extended model II) is a consequence as well as a cause of LS.
To recapitulate: the main step we have taken that yields results different from most previous research is to allow for non-linear effects of LS on longevity. A second change from the standard approach—excluding from analysis the final years of life in which LS sharply declines—has made only a small difference.
Our results have an interesting implication for LS theory. Most research treats LS as an outcome, as a goal in life which individuals are assumed to be striving for (King and Scollon 1998). However, an alternative but not mutually exclusive hypothesis is that happiness and positive affect serve an evolutionary purpose (Nesse 2005). From this perspective, positive feelings function to reinforce behaviours which have survival value and competitive value. Negative feelings exist to warn against repetition of behaviours which reduce survival chances and competitive success. LS research in Western countries (the evidence is much less clear for low income countries) has consistently found that most people report positive moods/affects most of the time (Diener et al. 1991, 1999). These feelings probably have survival or competitive value in that they help people to keep on pursuing personal and career goals in a reasonably effective way. The minority who report low levels of LS are less successful in their careers and personal relationships (Nesse 2005; Diener et al. 1999) and, as we have shown, die young.
Veenhoven (2008) has further suggested that chronic unhappiness may lead to early death as a result of over-activation of stress response mechanisms, increasing blood pressure and weakening the immune system. So, in his view, unhappy people may be more vulnerable to disease.
It is accepted that our results are limited to just two Western countries. It may be that the evidence we have brought to bear should not be regarded as overturning what had previously been regarded as a well established finding, based on surveys in many countries. It seems reasonable to suggest, though, that the hypothesis that it is only the unhappy who die young, and that for the rest of the population happiness makes no difference, merits continued investigation.
Notes
Respondents were asked whether they were ‘happy most of the time’ (39%), usually happy (44%) or unhappy (17%).
Data on obesity (body-mass index) were not collected until 2005 in HILDA. Too many deaths would be lost to analysis if obesity were to be included in Australian results.
The alternative would have been to use ‘years’ (1984, 1985…). However, it is clear that death is more likely to be due to the non-linear effects of aging than to the effects of being alive for one more year, then two, then three, and so on.
Church attendance is not included in the Australian results. The relevant question is only asked intermittently in HILDA. Too many deaths would be lost to analysis if the measure were to be included.
The index correlates 0.46 with LS.
References
Allison, P. D. (2014). Event history and survival analysis. Thousand Oaks, CA: Sage.
Argyle, M. (2002). The psychology of happiness. London: Methuen.
Brenner, M. H., & Mooney, A. (1983). Unemployment and health in the context of economic change. Social Science and Medicine, 17, 1125–1138.
Chida, Y., & Steptoe, A. (2008). Positive psychological well-being and mortality: A quantitative review of prospective observational studies. Psychosomatic Medicine, 70, 741–756.
ClinicalTrials.gov. (2015). Metformin longevity study (MLES). ClinicalTrials.gov Identifier: NCT02432287.
Costa, P. T., & McCrae, R. R. (1991). Revised NEO personality inventory (NEO PI-R) and NEO five-factor inventory (NEO-FFI): Professional manual. Odessa, FL: PAR.
Cox, D. R. (1972). Regression models and life-tables. Journal of the Royal Statistical Society, Series B, 34(2), 187–220.
Danner, D. D., Snowdon, D. A., & Friesen, W. V. (1991). Positive emotions in early life and longevity: Findings from the nun study. Journal of Personality and Social Psychology, 80, 804–813.
Deeg, D., & van Zonneveld, R. J. (1989). Does happiness lengthen life? In R. Veenhoven (Ed.), How harmful is happiness?. Rotterdam: Erasmus University Press.
Diener, E., & Chan, M. Y. (2011). Happy people live longer: Subjective well-being contributes to health and longevity. Applied Psychology: Health and Well-Being, 3, 1–43. https://doi.org/10.1111/j.1758-0854.2010.01045.x.
Diener, E., Sandvik, E., & Pavot, W. (1991). Happiness is the frequency, not the intensity, of positive affect versus negative affect. In F. Strack, M. Argyle, & N. Schwarz (Eds.), Subjective well-being (pp. 119–140). Oxford: Pergamon.
Diener, E., Suh, E. M., Lucas, R. E., & Smith, H. L. (1999). Subjective well-being: Three decades of progress. Psychological Bulletin, 25, 276–302.
Frick, J. R., Schupp, J., & Wagner, G. G. (2007). Enhancing the power of the German Socio-Economic Panel Study (SOEP) evolution, scope and enhancements. Schmollers Jahrbuch, 127, 139–169.
Friedman, H. S., & Martin, L. R. (2011). The longevity project. Melbourne: Angus and Robertson.
Friedman, H. S., Tucker, J. S., Schwartz, J. E., Martin, L. R., Tomlinson-Keasey, C., Winegard, D. L., et al. (1995). Childhood conscientiousness and longevity: Health behaviors and cause of death. Journal of Personality and Social Psychology, 68, 696–703.
Garvrilov, L. A., & Gavrilov, N. S. (2006). Reliability theory of aging and longevity. In E. J. Masoro & S. N. Austad (Eds.), Handbook of the biology of aging (pp. 3–42). San Diego, CA: Academic Press.
Gerstorf, D., Ram, N., Estabrook, R., Schupp, J., Wagner, G. G., & Linden-berger, U. (2010). Life satisfaction shows terminal decline in old age: Longitudinal evidence from the German Socioeconomic Panel Study. Developmental Psychology, 44, 1148–1159. https://doi.org/10.1037/0012-1649.44.4.1148.
Gremeaux, V., Gayda, M., Lepers, R., Sosner, P., Juneau, M., & Nigam, A. (2012). Exercise and longevity. Maturitas, 73, 312–317.
Guven, C., & Saloumidis, R. (2009). Why is the world getting older? The influence of happiness on mortality. SOEPpapers, 198, DIW Berlin, The German Socio-Economic Panel (SOEP).
Headey, B. W., Hoehne, G., & Wagner, G. G. (2014). Does religion make you healthier and longer lived? Evidence for Germany, Social Indicators Research, 119, 1135–1361.
Headey, B. W., & Muffels, R. J. A. (2015). Towards a theory of medium term life satisfaction: Two-way causation partly explains persistent satisfaction or dissatisfaction. Social Indicators Research. https://doi.org/10.1007/s11205-015-1146-8.
Hjelmborg, J., Iachine, I., Skytthe, A., Vaupel, J. W., McCue, M., Koskenvuo, M., et al. (2006). Genetic influence on human lifespan and longevity. Human Genetics, 119(3), 312–321. https://doi.org/10.1007/s00439-006-0144-y).
Kaeberlein, M., & Martin, G. (2015). Handbook of the biology of aging (8th ed.). San Diego: Academic Press.
King, L. A., & Scollon, C. N. (1998). What makes a life good? Journal of Personality and Social Psychology, 75, 156–165.
Kitahara, C. M., Flint, A. J., de Gonzalez, A. B., Bernstein, L., Brotzman, M., MacInnis, R. J., et al. (2014). Association between Class III obesity (BMI of 4059 kg/m) and mortality: A pooled analysis of 20 prospective studies. PLOS Medicine. https://doi.org/10.1371/journal.pmed.1001673.
Koivumaa-Honkanen, H., Honkanen, R., Koskenvuo, M., Viinamki, H., & Kaprio, J. (2002). Life dissatisfaction as a predictor of fatal injury in a 20-year follow-up. Acta Psychiatrica Scandinavica, 105, 444–450.
Koivumaa-Honkanen, H., Honkanen, R., Viinamaki, H., Heikkila, K., Kaprio, J., & Koskenvuo, M. (2000). Self-reported life satisfaction and 20-year mortality in healthy Finnish adults. American Journal of Epidemiology, 152, 983–991.
Koivumaa-Honkanen, H., Honkanen, R., Viinamaki, H., Heikkila, K., Kaprio, J., & Koskenvuo, M. (2001). Life satisfaction and suicide: A 20-year follow-up study. American Journal of Psychiatry, 158, 433–439.
Koivumaa-Honkanen, H., Koskenvuo, M., Honkanen, R. J., Viinamki, H., Heikkild, K., & Kaprio, J. (2004). Life dissatisfaction and subsequent work disability in an 11-year follow-up. Psychological Medicine, 34, 221–228.
Lance, C. E., Mallard, A. G., & Michalos, A. C. (1995). Tests of the causal directions of global-life facet satisfaction relationships. Social Indicators Research, 34, 69–92.
Liu, B., Floud, S., Pirie, K., Green, J., Peto, R., Beral, V., et al. (2016). Does happiness itself directly affect mortality? The prospective UK Million Women Study. The Lancet, 387(1002), 874–881.
Lyrra, T., Tormakangas, T. M., Read, S., Rantanen, T., & Berg, S. (2006). Satisfaction with present life predicts survival in octogenarians. Journals of Gerontology Series B, Psychological Sciences and Social Sciences, 61, 319–326.
Martin, L. R., Friedman, H. S., Tucker, J. S., Tomlinson-Keasey, C., Criqui, M. H., & Schwartz, J. E. (2002). A life course perspective on childhood cheerfulness and its relation to mortality risk. Personality and Social Psychology Bulletin, 28, 1155–1165.
Mathison, L., Andersen, M. H., Veenstra, M., Wahl, A. K., Hanestad, B. R., & Fosse, E. (2007). Quality of life can both influence and be an outcome of general health perceptions after heart surgery. Health and Quality of Life Outcomes, 5, 27. https://doi.org/10.1186/1477-7525-5-27.
McCarron, P., Gunnell, D., Harrison, G. L., Okasha, M., & Davey Smith, G. (2003). Temperament in young adulthood and later mortality: Prospective observational study. Journal of Epidemiology and Community Health, 57, 888–892.
Min, J.-M., Lee, C.-K., & Park, H.-N. (2012). The lifespan of Korean eunuchs. Current Biology, 22, 792–793.
National Institute on Aging. (1996). Landmark study links cognitive ability of youth with Alzheimer’s disease risk later in life. U.S. Department of Health and Human Services. Accessed Sept 5, 2017, from archive.hhs.gov/news/press/1996pres/960220b.html.
Nesse, R. M. (2005). Natural selection and the elusiveness of happiness. In F. A. Huppert, N. Baylis, & B. Keverne (Eds.), The science of well-being (pp. 3–34). Oxford: Oxford University Press.
Ostir, C. V., Markides, K. S., Black, S. A., & Goodwin, J. S. (2000). Emotional wellbeing predicts subsequent functional independence and survival. Journal of the American Geriatrics Society, 48, 473–478.
Scherpenzeel, A., & Saris, W. E. (1996). Causal direction in a model of life satisfaction: The top-down/bottom-up controversy. Social Indicators Research, 38, 161–180.
Shirai, K., Iso, H., Ohira, T., Ikeda, A., Noda, H., Honjo, K., et al. (2009). Perceived level of life enjoyment and risks of cardiovascular disease incidence and mortality: The Japan public health center-based study. Circulation, 120, 956–963.
StataCorp. (2017). Structural equation modelling reference manual, release 14. College Station, TX: Stata Press.
Strawbridge, W. J., Cohen, R. D., Shema, S. J., & Kaplan, G. A. (1997). Frequent attendance at religious services and mortality over 28 years. American Journal of Public Health, 87, 957–961.
Vaillant, G. E. (1977). Adaptation to life. Boston: Little, Brown.
Veenhoven, R. (2008). Healthy happiness: Effects of happiness on physical health and the consequences for preventive health care. Journal of Happiness Studies, 9, 449–469.
Voss, M., Nylen, L., Floderus, B., Diderichsen, F., & Terry, P. D. (2004). Unemployment and early cause-specific mortality: A study based on the Swedish Twin Registry. American Journal of Public Health, 94, 2155–2161.
Ware, J. E., Snow, K., & Kosinski, M. (2000). SF-36 Health Survey: Manual and interpretation guide. Lincoln, Rhode Island: QualityMetric Inc.
Watson, N., & Wooden, M. (2004). Assessing the quality of the HILDA Survey Wave 2 data. Melbourne: Melbourne Institute of Applied Economic and Social Research.
Wooldridge, J. M. (2010). Econometric analysis of cross-section and panel data (2nd ed.). Cambridge, MA: MIT Press.
Xu, J., & Roberts, R. E. (2010). The power of positive emotions, it’s a matter of life or death: Subjective well-being and longevity over 28 years in a general population. Health Psychology, 29, 919.
Zhang, X., & Huang, S.-S. (2007). The micro-consequences of macro-level social transition: How did Russians survive in the 1990s? Social Indicators Research, 82, 337–360.
Acknowledgements
The German panel data used in this publication were made available to us by the German Socio-Economic Panel Study (SOEP) at the German Institute for Economic Research (DIW), Berlin. The Australian panel data came from the Household, Income and Labour Dynamics in Australia (HILDA) Survey. The HILDA Project was initiated and is funded by the Australian Government Department of Social Services (DSS) and is managed by the Melbourne Institute of Applied Economic and Social Research (Melbourne Institute). The findings and views reported in this paper, however, are those of the authors and should not be attributed to DIW, DSS or the Melbourne Institute.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
See Table 7.
Rights and permissions
About this article

Cite this article
Headey, B., Yong, J. Happiness and Longevity: Unhappy People Die Young, Otherwise Happiness Probably Makes No Difference. Soc Indic Res 142, 713–732 (2019). https://doi.org/10.1007/s11205-018-1923-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11205-018-1923-2