
Abstract
Sexuality is an important component in people’s lives, however forgotten in people with intellectual disabilities. Faced with this situation, people with intellectual disabilities tend to be in a situation of vulnerability with greater risk of sexual abuse and altered sexual behavior that give them difficulties to have a lasting relationship. A review of the literature was performed in the databases: Medline, Embase, Lilacs and Scielo. Included studies must mention the perception of people with intellectual disabilities about their sexuality in relation to: education, difficulties, strengths, gender identification, the role of the family and their close circle. 898 articles were reviewed by title and abstract. In total, 38 references were selected for full-text review. Being evident the importance of sexuality in people with intellectual disability, this topic should be addressed from a personal level and their close circle (family and support networks) through sex education about: sexuality, anatomy and functioning of the body, sexual abuse, use of contraceptives, and sentimental relationships. Sexuality in people with intellectual disability should be approached in a multidimensional way. An overarching theme is to teach family and educators not to diminish the value that represents sexuality in people and to assist when needed to address the process of sexual development and sexuality.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
There is a lack of research addressing sexuality in people with intellectual disabilities (ID), as the topic is perceived as a sensitive and somewhat taboo subject for caregivers and even medical staff [1]. Although people with ID have the same sexuality needs as the general population, it is often neglected and poorly understood in the health care field. Some medical staff may have difficulty talking about sexuality with these patients or have fear of perceiving them as sexual beings [2].
Sexual activities and desires are natural aspects of being a human, but for people with ID, the information available on sexuality is usually limited to sexual health education, such as sexual function or contraception. There are barriers that make it difficult to include people with ID in general population studies. Moreover, individuals with ID are susceptible to being perceived as asexual and needing societal protection [3]. This situation ends up isolating them, with a consequent effects in their relationships and results in poor interaction with other people [4]. All of these challenges leads to less opportunities for people with ID to learn about their sexuality or to engage in social activities and sexual experimentation [5].
Young people with ID also seem to have a reduced ability to determine abusive behaviors [6] and a higher risk of being abused compared to the general population [7]. These abuses are usually perpetrated by the people responsible for their care and education [8]. Given the high prevalence of abuse and the benefit that intervention programs can offer in the short and long term, interventions should target this population early [9].
Considering these circumstances, it becomes vital to address sexuality from multiple perspectives: sexual abuse, education, desires, contraceptive use, sexuality differences between males and females as well as between adolescents and adults, gender identity, and sexual orientation. In recent years, there has been some progress in addressing false stereotypes. Despite the existence of studies focusing on sexuality in people with ID, it is necessary to review the literature to gather recent information to understand the problem and develop education that meets the needs of individuals with ID so that they can develop a healthy sexuality.
Methods
A review of the literature was made in 4 databases (PubMed, Embase, Lilacs and Scielo) searching for any information concerning the field of sexuality in individuals with Intellectual Disability (ID).
The search criteria was established in the form of free text and indexed terms. To characterize Intellectual Disability (ID), the free terms: “learning disability”, “mental retardation”, “intellectual disability” were used; and the indexed terms “learning disorders” and “intellectual disability”. To characterize sexuality, the free terms: “sexual behavior”, “sexual function”, “sexual desire”, “sexual education”, “sexuality” and “safe sex” were used; and the indexed terms: “Sexual behavior”, “sexual dysfunction”, “safe sex”, “sex education” and “sex counseling” were used. As a restriction, the search was limited to publications in the last 10 years. A gray literature search was also made in The National Technical Information Service (NTIS) and the European Association for Grey Literature Exploitation (EAGLE), in which relevant information was not found.
The articles had to be original studies, which could provide information about sexuality in people with ID in the following fields: education, support networks, gender identification and attitudes of this population regarding sexuality. The articles were reviewed by title and abstract by two reviewers independently. Selected articles were reviewed in full text to determine whether they contained relevant information in the sexuality of people with ID, as previously described. Duplicate articles were excluded, and studies that were written in a language other than English or Spanish were ignored. The information obtained was subsequently analyzed.
Results
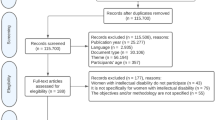
898 references were found, which were reviewed by title and abstract. A total of 75 references were selected for review in full text, of which 37 were excluded since they were not original articles, did not express data of interest, or were references that did not have available full text (poster format or only the abstract). Finally, 38 full-text articles were analyzed for data extraction (see Fig. 1).

Flowchart of the search
Sexuality in Adolescents with ID
Seven articles were found that discussed sexuality in adolescents with ID. Castelão et al. (2010) found that initial manifestations of sexual interest in this population do not differ from adolescents without ID. They analyzed behaviors such as flirting, dating and sexual desire [10]. Moreover Akrami and Davudi [11] found that boys with ID had more behavioral problems like public masturbation, and 7.69% of boys with ID had experienced sexual abuse.
On the other hand, Frawley and Wilson (2016) found through qualitative data that young people with ID are aware of rules regarding appropriate sexual behavior. However, they do not know how sexual relations develop, and this situation was associated with limited access of information [12]. Similar results were found by Isler et al. [4], which compared young people between 15 and 20 years of age with mild to moderate ID and students without ID, finding that more than half of the adolescents had not been professionally educated about sexuality and 46.7% had never spoken of sex with their parents. Dekker et al. [13] also found that there was less knowledge among young people with ID regarding the mechanism of sexual intercourse and contraceptive methods, which leaves adolescents with ID with greater risk and vulnerability to unwanted pregnancies and sexually transmitted diseases in comparison with adolescents without ID.
Two articles were found on sex differences. Shandra and Chowdhury [1] conducted a study with 2729 girls between 12 and 24 years old with and without mild ID, finding that women with ID had less knowledge about contraceptive methods and less use of them with their sexual partners than adolescents without ID; additionally, women with ID wanted a pregnancy in the first sexual encounter in a greater proportion than the comparison group. On the other hand, Wilson et al. [14] shows how boys express more masturbatory behaviors than dating rituals or petting. The researchers also explored how sexuality in male adolescents with moderate to profound ID can be constructed, with the study concluding that sexual expressions and desire in people with ID are affected by a “biological urgency” and were more likely to engage in sexual practices affected by environmental factors, resulting in atypical sexual practices [14].
Sexuality in Adults with ID
Six studies were found that discussed sexuality in adults with ID. Chou et al. (2015) looked for differences in sexual attitudes in men and women through interviews, finding differences in both reproductive and sexual behavior, with women having more negative attitudes towards contraceptive methods. In addition, these groups are presented with limited opportunities to develop emotional relationships as well as a healthy sexual identity [15]. Equally, Yau et al. [16] shows how the adult population with ID has the desire to express their sexuality, either through intimate relationships or through the experience of relationships with other people, although they may feel insecure in the latter, especially with long-term relationships.
Bernert and Ogletree (2013) described the most frequent sexual behaviors in women with ID, finding that the majority of women evaluated were not sexually active, and those who were active had heterosexual intercourse exclusively. The study also showed that the main negative perceptions regarding sexuality were related to the fear of first sexual intercourse, as well as fear of negative consequences and perception of absence of pleasure [17]. On the other hand, Van Schrojenstein Lantman-de Valk et al. [18] reported less use of contraceptive methods in women with ID than the general population, of whom only 80% used oral or parenteral pharmacological contraception.
Among other findings, Kijak [19] identified that people with ID have a higher autoerotic behavior compared with the general population. On the other hand, O’Callaghan and Murphy [20] described the knowledge that people with ID have about laws, finding that less than half know about laws against sexual abuse, only half know about the minimum age for consent in a sexual relationship, and only a third know that they have equal freedom to marry.
Sexuality in People with ID with Specific Conditions
Three studies identified specific ID conditions (Autism and Down Syndrome). Barg et al. [22] and Bononi et al. [21] found that sexuality development in people with Down Syndrome was similar to the general population. Additionally, Bononi et al. [21] found a good acceptance of corporeality in individuals with Down Syndrome. On the other hand, Ginevra et al. [23] found that sexual behaviors and knowledge among individuals with Down Syndrome and Autism are different from the general population, demonstrating the importance of different education and training in this population about sexuality.
Sex Education in ID Patients
Ten studies were identified that discussed the importance of sex education in this population. Barnard-Brak et al. (2014) identified that between 53 and 56% of people with severe and moderate ID respectively receive sex education. This low prevalence was due to most educators not feeling prepared to manage themes of sexuality with these patients or due to an incorrect perception of mental age versus chronological age [24]. On the other hand, Enow et al. [25] and Calitz [26] mention other problems associated with people with ID, including vulnerability and sexual abuse, where a strong education is fundamental to teach about consent and the necessity of psychological and legal support in subjects who were already victims of abuse.
Moreover, Thompson et al. (2016) and Leuta and Mihoković (2007) identified the topics in which individuals with ID have sufficient and insufficient education. Thompson et al. [27] describes strengths in issues such as body parts and some physiological topics like menstruation. On the other hand Leutar and Mihoković [2] found deficiencies in subjects such as body function during sexual intercourse, contraceptives, and sexually transmitted diseases.
Five authors evaluated the most important aspects to deliver adequate sex education in a population with ID. Schaafsma et al. [28] mentioned that first step should be the identification of the most important problems in the community, followed by evaluation of what activities have been developed in the past and how to involve caregivers and family members. Swango-Wilson [29] also gives some recommendations such as give sex education classes in mixed groups, and discussion about “safe sexuality” and feelings. On the other hand, Löfgren-Mårtenson (2012) describes the subjects in which people with ID are more interested. They found different opinions, with stating that sexual education should focus on the understanding of the sentimental relationship, while others were more concerned about body function. These individual differences demonstrate the importance of anatomical and physiological focused sex education during adolescence and feelings in adulthood [30].
Finally, Hayashi et al. [31] and Murphy et al. (2007) evaluated the effectiveness of educational interventions in their population, with the first study finding positive effects in social integration skills. In contrast, Murphy et al. [32] found no differences after their intervention; however, despite the inconclusive findings, he mentioned the importance of education in people with ID.
Gender Identification and Sexual Orientation in People with ID
Four articles discussed the identification and characterization of gender in patients with ID. Dinwoodie et al. (2016) and Löfgren-Mårtenson (2009) report the challenges in this population with gender identification. Löfgren-Mårtenson (2009) describes the low prevalence in people with ID with identifying homosexual orientation or any other sexual orientation different from heterosexual. Both authors associate this difficulty with support networks, which is fundamental in the gender identification process but is more deficient in this population when compared to people without ID [33, 34]. On the other hand, Rushbrooke et al. [35] found that people with ID are aware of their sexuality in childhood or adolescence and from that moment, begin to develop their identity, though this can change over time.
Likewise, Wilson et al. observed the perception of masculinity among adolescent and adult men with ID, finding a diminished characterization of what may be stereotypically considered as masculinity, given the difficulty that these individuals may have to carry out ‘masculine’ actions, such as sports or having more independent attitudes. However, masculinity is a mutable construct, and a person can manifest more or less “masculine” actions depending on their cultural context and their environment [36].
Network Support and Sexuality in People with ID
Eight articles discussed the importance of support networks in people with ID. Jahoda et al. [37] found some knowledge differences between young people with and without ID since support networks can influence how much information about sexuality they receive, the quality of this information, and accessibility to information sources. Likewise, Healy et al. [38] describes the importance of family in education and reception of information. Other authors identified some difficulties that are present in the support networks of people with ID. Lafferty et al. [40], and Meaney-Tavares and Gavidia-Payne [39] focused on educators and medical staff who care for this population and found a lack of specialized training in communication and delivering interventions for people with ID. McCarthy [41] also found a lack of tools in caregivers to objectively evaluate the quantity and quality of knowledge about sexuality in their patients.
On the other hand, Yıldız and Cavkaytar (2016) and Pownall et al. (2012) described the importance of family support networks, particularly the maternal role in sex education, due to the reliable image that represents the mother in people with ID in the moment they want to talk about their sexuality. Many mothers want to have more information on this topic and want to be educated on how to communicate the information to their children with ID, especially during difficult ages, such as adolescence [9, 42]. Finally, Parchomiuk [43] found communication challenges, specifically the erroneous perception of ‘eternal childhood’ in this population, which diminishes the importance of sexuality.
Discussion
Literature describes different topics of sexuality in people with intellectual disability. Most of the reviewed articles describes the perception that people with ID have of themselves, their knowledge of sexuality, their needs, the risks they could be exposed due to their condition, and the importance of their support network in the accompaniment and learning process about their sexuality.
One key finding was that the importance of sexual expression is underestimated in this population (in men, women, adolescents, and adults), but sexual expression is necessary to allow them to develop fulfilling relationships with others. Winges-Yanez [44] explains this phenomenon from the perspective of caregivers who may tend to see people with ID as asexual individuals given their condition.
There is a need for people with ID to express their sexuality, but it is also evident that this population is more vulnerable to risk, associated with sexual abuse as well as sexually transmitted diseases or unwanted pregnancies due to less knowledge and less use of contraceptive methods [11, 25, 26]. This situation must be addressed in different ways, with education being the main method to teach about consent, rights, and legal mechanisms that protect them from abuse and the importance of reporting abuses to prevent re-occurrence [45].
It was also found that people with ID have less access to information. Anatomy and physiology in intercourse as well as contraceptive methods were some of the most requested topics for sexual health education. However, it is interesting to note that other learning needs were omitted in sex education classes, such as how to begin a sentimental relationship and how to have a long-term relationship, which further demonstrates the limitations in information and education that they receive [2, 30].
Finally, support networks were found to be important, and the role of parents in the process of accompanying and delivering information to their children with ID during adolescence, when physical changes and sexual thoughts emerge, was highlighted. There is a definite need to educate parents, so that they do not make the mistake of ignoring the sexuality of their children, and to help them communicate the information necessary for their children to be safe [9, 42].
Possible Implications
People with intellectual disability need support to have healthy relationships. This review provides the information necessary to raise awareness and concern about sexuality in people with ID. Parents, caregivers, educators, and medical staff should be educated about sexuality in this population. Sex education in early ages should be reinforced. Sex education for this population should be given by professional sex educators and should also focus on neglected topics such as consent, protection laws, and romance. Medical staff should have the right materials to provide information effectively. There is a lack of information on how to discuss issues surrounding romantic relationships with people with ID. We hope that this study will encourage others to conduct further research in this area.
Conclusion and Limitations
The results of this review demonstrate the challenges that people with ID face and identify important sexual education topics for people with ID. The review also highlights that these issues should not be ignored by relatives and caregivers given the role that the support network plays in the education and accompaniment of the person with ID, to help them have a healthy and satisfying sex life. Although the attitudes of family and medical staff towards the topics of sexuality in people with ID may have been changed, the biggest challenge in this population remains the lack of accessibility of information, and not the personal limitations of people with ID (Table 1).
Some limitations of this study deserve attention. As a review, this article does not give original research findings and was intended to describe the results from other authors. Additionally, we did not intend to conduct a meta-analysis, and so the chosen studies could be heterogeneous. Some key strengths of this paper include that it is comprehensive review with the latest information and that the article selection was conducted using a specific methodology, enabling readers to reproduce our efforts and delve deeper into the subject if they desire.
References
Shandra, C.L., Chowdhury, A.R.: The first sexual experience among adolescent girls with and without disabilities. J. Youth Adolesc. 41(4), 515–532 (2012)
Leutar, Z., Mihoković, M.: Level of knowledge about sexuality of people with mental disabilities. Sex. Disabil. 25(3), 93–109 (2007)
Suris, J.C., Resnick, M.D., Cassuto, N., Blum, R.W.: Sexual behavior of adolescents with chronic disease and disability. Sex. Disabil. 19(2), 124–131 (1996)
Isler, A., Tas, F., Beytut, D., Conk, Z.: Sexuality in adolescents with intellectual disabilities. Sex. Disabil. 27(1), 27–34 (2009)
Chen, C.J.: From the perspective of philosophy of life care for sexuality education for persons with disabilities. J Sex Med. 8, 283 (2011)
Wang, B., Li, B.-H., Hu, J.-M.: Evaluation on social function in cases involving sexual assault of patients with mental retardation. Fa Yi Xue Za Zhi 23(2), 110–113 (2007)
Conod, L., Servais, L.: Sexual life in subjects with intellectual disability. Salud Publica Mex. 50 Suppl 2, s230–s238 (2008)
Martinello, E.: Reviewing strategies for risk reduction of sexual abuse of children with intellectual disabilities: a focus on early intervention. Sex. Disabil. 32(2), 167–174 (2014)
Pownall, J.D., Jahoda, A., Hastings, R.P.: Sexuality and sex education of adolescents with intellectual disability: mothers’ attitudes, experiences, and support needs. Intellect. Dev. Disabil. 50(2), 140–154 (2012)
Castelão, T., Campos, T., Torres, V.: A new perspective of sexual orientation for adolescents that have mental retardation. Sexologies 19, S116–S117 (2010)
Akrami, L., Davudi, M.: Comparison of behavioral and sexual problems between intellectually disabled and normal adolescent boys during puberty in Yazd, Iran. Iran. J. Psychiatry Behav. Sci. 8(2), 68–74 (2014)
Frawley, P., Wilson, N.J.: Young people with intellectual disability talking about sexuality education and information. Sex. Disabil. 34(4), 469–484 (2016)
Dekker, A., Safi, M., van der Zon-van Welzenis, E.I., Echteld, M.A., Evenhuis, H.M.: Sexuality and contraception in young people with mild intellectual disability; a qualitative study on the basis of 28 interviews. Ned. Tijdschr. Geneeskd. 158, A8010 (2014)
Wilson, N.J., Parmenter, T.R., Stancliffe, R.J., Shuttleworth, R.P.: Conditionally sexual: men and teenage boys with moderate to profound intellectual disability. Sex. Disabil. 29(3), 275–289 (2011)
Chou, Y.-C., Lu, Z.-Y.J., Pu, C.-Y.: Attitudes toward male and female sexuality among men and women with intellectual disabilities. Women Health 55(6), 663–678 (2015)
Yau, M.K.-S., Ng, G.S.-M., Lau, D.Y.-K., Chan, K.S., Chan, J.S.-K.: Exploring sexuality and sexual concerns of adult persons with intellectual disability in a cultural context. Br. J. Dev. Disabil. 55(2), 97–108 (2009)
Bernert, D.J., Ogletree, R.J.: Women with intellectual disabilities talk about their perceptions of sex. J. Intellect. Disabil. Res. 57(3), 240–249 (2013)
van Schrojenstein Lantman-de Valk, H.M.J., Rook, F., Maaskant, M.A.: The use of contraception by women with intellectual disabilities. J. Intellect. Disabil. Res. 55(4), 434–440 (2011)
Kijak, R.: The sexuality of adults with intellectual disability in Poland. Sex. Disabil. 31(2), 109–123 (2013)
O’Callaghan, A.C., Murphy, G.H.: Sexual relationships in adults with intellectual disabilities: understanding the law. J. Intellect. Disabil. Res. 51(Pt 3), 197–206 (2007)
Bononi, B.M., Sant’Anna, M.J.C., de Oliveira, A.C.V., Renattini, T.S., Pinto, C.F., Passarelli, M.L., et al.: Sexuality and persons with Down syndrome. A study from Brazil. Int. J. Adolesc. Med. Health 21(3), 319–326 (2009)
Barg, E., Bury, M., Marczyk, T., Palac, K., Wirth, M.: Psychosexual problem in young people with Down syndrome in parents’ opinions—personal experience. Pediatr. Endocrinol. Diabetes Metab. 14(4), 225–230 (2008)
Ginevra, M.C., Nota, L., Stokes, M.A.: The differential effects of Autism and Down’s syndrome on sexual behavior. Autism Res. 9(1), 131–140 (2016)
Barnard-Brak, L., Schmidt, M., Chesnut, S., Wei, T., Richman, D.: Predictors of access to sex education for children with intellectual disabilities in public schools. Intellect. Dev. Disabil. 52(2), 85–97 (2014)
Enow, H., Nagalingam, P., Singh, R., Thalitaya, M.D.: Need for a comprehensive sex and relationship education programme for adults with learning disability. Psychiatr Danub. 27(Suppl 1), S465–S467 (2015)
Calitz, F.J.W.: Psycho-legal challenges facing the mentally retarded rape victim. S. Afr. J. Psychiatry 17(3), 66–72 (2011)
Thompson, V.R., Stancliffe, R.J., Wilson, N.J., Broom, A.: The content, usefulness and usability of sexual knowledge assessment tools for people with intellectual disability. Sex. Disabil. 34(4), 495–512 (2016)
Schaafsma, D., Stoffelen, J.M.T., Kok, G., Curfs, L.M.G.: Exploring the development of existing sex education programmes for people with intellectual disabilities: an intervention mapping approach. J. Appl. Res. Intellect. Disabil. 26(2), 157–166 (2013)
Swango-Wilson, A.: Meaningful sex education programs for individuals with intellectual/developmental disabilities. Sex. Disabil. 29(2), 113–118 (2011)
Löfgren-Mårtenson, L.: “I want to do it right!” A pilot study of Swedish sex education and young people with intellectual disabilities. Sex. Disabil. 30(2), 209–225 (2012)
Hayashi, M., Arakida, M., Ohashi, K.: The effectiveness of a sex education program facilitating social skills for people with intellectual disability in Japan. J. Intellect. Dev. Disabil. 36(1), 11–19 (2011)
Murphy, G., Powell, S., Guzman, A.-M., Hays, S.-J.: Cognitive-behavioural treatment for men with intellectual disabilities and sexually abusive behaviour: a pilot study. J. Intellect. Disabil. Res. 51(Pt 11), 902–912 (2007)
Dinwoodie, R., Greenhill, B., Cookson, A.: “Them two things are what collide together”: understanding the sexual identity experiences of lesbian, gay, bisexual and trans people labelled with intellectual disability. J. Appl. Res. Intellect. Disabil. (2016). doi:10.1111/jar.12252
Löfgren-Mårtenson, L.: The invisibility of young homosexual women and men with intellectual disabilities. Sex. Disabil. 27(1), 21–26 (2009)
Rushbrooke, E., Murray, C., Townsend, S.: The experiences of intimate relationships by people with intellectual disabilities: a qualitative study. J. Appl. Res. Intellect. Disabil. 27(6), 531–541 (2014)
Wilson, N.J., Parmenter, T.R., Stancliffe, R.J., Shuttleworth, R.P.: From diminished men to conditionally masculine: sexuality and Australian men and adolescent boys with intellectual disability. Cult. Health Sex. 15(6), 738–751 (2013)
Pownall, J.D., Jahoda, A., Hastings, R., Kerr, L.: Sexual understanding and development of young people with intellectual disabilities: mothers’ perspectives of within-family context. Am. J. Intellect. Dev. Disabil. 116(3), 205–219 (2011)
Healy, E., McGuire, B.E., Evans, D.S., Carley, S.N.: Sexuality and personal relationships for people with an intellectual disability. Part I: service-user perspectives. J. Intellect. Disabil. Res. 53(11), 905–912 (2009)
Meaney-Tavares, R., Gavidia-Payne, S.: Staff characteristics and attitudes towards the sexuality of people with intellectual disability. J. Intellect. Dev. Disabil. 37(3), 269–273 (2012)
Lafferty, A., McConkey, R., Simpson, A.: Reducing the barriers to relationships and sexuality education for persons with intellectual disabilities. J. Intellect. Disabil. 16(1), 29–43 (2012)
McCarthy, M.: Prescribing contraception to women with intellectual disabilities: general practitioners’ attitudes and practices. Sex. Disabil. 29(4), 339–349 (2011)
Yıldız, G., Cavkaytar, A.: Effectiveness of a sexual education program for mothers of young adults with intellectual disabilities on mothers’ attitudes toward sexual education and the perception of social support. Sex Disabil. 35(1), 3–19 (2017)
Parchomiuk, M.: Specialists and sexuality of individuals with disability. Sex. Disabil. 30(4), 407–419 (2012)
Winges-Yanez, N.: Why all the talk about sex? An authoethnography identifying the troubling discourse of sexuality and intellectual disability. Sex. Disabil. 32(1), 107–116 (2014)
Wacker, J., Macy, R., Barger, E., Parish, S.: Sexual assault prevention for women with intellectual disabilities: a critical review of the evidence. Intellect. Dev. Disabil. 47(4), 249–262 (2009)
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Rights and permissions
About this article

Cite this article
Medina-Rico, M., López-Ramos, H. & Quiñonez, A. Sexuality in People with Intellectual Disability: Review of Literature. Sex Disabil 36, 231–248 (2018). https://doi.org/10.1007/s11195-017-9508-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11195-017-9508-6