
Abstract
Paget’s disease of bone (PDB) is a metabolic bone disease with distinct geographical and ethnic differences in its pathogenesis. In this study, we aimed to retrospectively analyze the clinical features and the status of diagnosis and treatment of PDB in mainland China to improve the clinician’s understanding of this disease. For this purpose, we conducted a systematic review of 118 articles, including a total of 332 patients with PDB. The results showed that the onset age of PDB in mainland China was 46–60 years. The number of male patients in most age groups was slightly higher than that of female patients, but there was no statistical difference (p > 0.05). The gender ratio (male to female) of PDB in mainland China was significantly different from that in Japan (p < 0.05), but not from that in the USA (p > 0.05). The clinical manifestations of PDB patients in mainland China mainly included ostealgia, bone malformation, hearing loss, and fracture, and bisphosphonate was used as the main treatment drug. These findings were similar to those in Japan, UK, and USA. Total alkaline phosphatase (TALP) level was elevated in about 89.7% of patients, and no correlation between TALP level and ostealgia was observed (p > 0.05). In addition, no difference in TALP level between males and females in each group was observed (p > 0.05).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Paget’s disease of bone (PDB), also called osteitis deformans or scleromalacia, is a progressive monostotic or polyostotic metabolic bone disease characterized by focal abnormal bone remodeling [1]. It was first discovered in 1876 by the British pathologist, Sir James Paget, and named after him [2]. However, the etiology of PDB remains unclear. A previous study reported that in about 14% of patients with a positive family history, the risk of PDB in first-degree relatives of patients was 7–10 higher times than that in general population [3,4,5]. Mutations in sequestosome1 gene (SQSTM1) are likely to be associated with the development of this disease [6]. Other triggers include certain environmental factors, such as deficiency of vitamin D and calcium during childhood [7, 8], zoonotic infection [9], toxic exposure [10], and virus infection [11].
After osteoporosis, PDB is the second most common metabolic bone disease in western countries, with the highest incidence rate in the UK (5.4%), followed by Australia and New Zealand [12,13,14], and the lowest being in Japan (0.00028%) [15]. An epidemiological investigation related to PDB in Japan revealed that the sex ratio (male to female) was 0.86:1, and ostealgia and bone malformation were the most common symptoms [16]. Another study in Hong Kong, including 7 patients with PDB [17], showed that only 1 patient was diagnosed based on clinical manifestations, while the others were diagnosed based on abnormal total alkaline phosphatase (TALP) levels or incidentally by X-ray.
In 2012, a case study of 160 patients with PDB was conducted in China. A sex ratio (male: female) of 3:2 was reported. Bone malformation was found to be the most common clinical manifestation, followed by ostealgia, fracture, and deafness. The most frequently affected bones included the femur, pelvis, skull, vertebra, and tibia [18]. However, this study had certain limitations. First, statistical data of onset age, clinical features, and affected bones were lacking. Second, the status of PDB diagnosis and treatment in China was not systematically reviewed. Third, the correlation between onset age and gender, and the correlation of TALP with gender and ostealgia were not analyzed.
In this review, we summarized the clinical characteristics and the status of diagnosis and treatment of PDB in mainland China over the last 60 years, with an aim to improve the clinician’s understanding of this disease. Furthermore, we statistically analyzed the relationship between age of onset and gender, as well as the correlation of TALP with gender and ostealgia. Clinical department records and comparison of clinical manifestations of PDB between mainland China and western countries and Japan were also included.
2 Materials and methods
2.1 Inclusion criteria
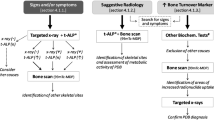
Eligible studies included those in which PDB was diagnosed based on: (1) typical X-ray or Computed Tomography (CT) images, (2) increased TALP levels, (3) abnormal values of radionuclide bone scan (RBS), and (4) pathological alterations. Patients who conform to the first three criteria and/or the last one can be diagnosed as PDB. In addition, case reports, case series, and original articles were also included.
2.2 Exclusion criteria
Studies on Paget’s disease of breast or other parts of the body as well as those including other racial and ethnic groups were excluded. We also excluded narrative reviews, foreign language studies, publications that failed to provide the required statistics, and studies that are not available in full text. For studies published more than once, the most recent one was included.
2.3 Literature search
A comprehensive search of several databases was performed from each database’s earliest inception to May 2018. The databases included China National Knowledge Infrastructure (CNKI), China Biology Medicine disc (CBM), PubMed, Excerpta Medica Database (EMBASE), Cochrane Library, Wanfang Data Knowledge Service Platform (WANFANG), and Weipu Chinese Science and Technology Journal Database (VIP).The following terms were used to conduct the search: Chinese terms for “Paget’s disease of bone, Paget’s disease, deformation osteitis”, English terms for “osteitis deformans (Mesh), Paget’s disease of bone, or Paget disease of bone”, and “China or Chinese (Affiliation)”. Besides database search, we also performed a manual search for the included studies, related comments, and reference lists of systematic reviews.
2.4 Literature selection and data extraction
Two researchers independently imported all relevant articles into the Endnote software and assessed all included studies as described in the inclusion and exclusion criteria. Following de-duplication, titles were independently screened for eligibility, followed by screening of abstracts and then the full-text.
Researchers independently extracted data from the included articles. The following data were abstracted: publication year, province, sex, age, clinical manifestations, commonly involved bones, TALP expression, pathologic findings, diagnostic techniques, treatment options, and medical departments.
2.5 Assessment of study quality
Included studies were all case reports, original articles, and retrospective studies, with a follow-up period ranging from 2 months to 25 years.
2.6 Statistical analysis
Differences between the two independent researchers were settled by consensus. If consensus was not reached, the assessment of a third researcher was decisive. All statistical analyses were performed using SPSS 22.0 software (Statistical Product and Service Solutions, USA).
3 Results
3.1 Study selection
The database search yielded 752 articles, of which 118 studies [19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135] including a total of 332 cases were ultimately selected for this systematic review (Fig. 1),among them, two studies with 10 cases were familial [135, 136].

Flow chart of the literature retrieval and screening process. CNKI, China National Knowledge Infrastructure; CBM, China Biology Medicine disc; EMBASE, Excerpta Medica Database; VIP, Weipu Chinese Science and Technology Journal Database; WANFANG, Wanfang Data Knowledge Service Platform
3.2 PDB-related articles published over the last 60 years in mainland China
An analysis of all statistical results showed that the number of PDB cases increased over the years. 1961–1969: 5 cases, 1980–1989: 17 cases, 1990–1999: 43 cases, 2000–2009: 107 cases, 2010–2018: 160 cases, 1970–1979: no cases reported (Fig. 2).

Number of PDB cases in studies published over the last 60 years in mainland China
3.3 Age and gender ratio of PDB
We analyzed 156 patients whose age could be obtained. Among them, the minimum age was 2 months, the maximum age was 86 years, the mean age was 55.1 ± 7.2 years, and the peak age was 46–60 years. Cases of patients below 30 years of age were rare. Patients in the age groups of 0–15 and 16–30 were not analyzed due to insufficient case numbers. Data of patients in the age groups of 31–45, 46–60, 61–75, and > 75 were compared with chi-square test. No statistical differences between males and females in each age group were observed (p > 0.05; Fig. 3).

Age distribution of 156 PDB patients whose age could be obtained. There was no significant difference in the number of PDB cases between males and females in each age group (p > 0.05)
3.4 Basic clinical features of patients with PDB
This study included 256 clinically affected patients, of which 226 patients (around 88.3%) displayed clinical symptoms of PDB and 30 patients (around 11.7%) visited the hospital due to increased TALP levels or abnormal X-ray scans. No significant difference in clinical manifestations between different genders was reported (p > 0.05; Fig. 4a). From a total of 147 patients with affected bones, 80 were monostotic and 67 were polyostotic cases. The most commonly affected bones in the monostotic cases included the skull, pelvis, tibia, and centrum. The TALP levels of 46 patients were analyzed, and those of 3 patients were in the normal range, while those of 43 patients were increased. The mean TALP level was 1200.8 ± 172.9 U/L. The TALP level in majority of the patients was 10 times higher than the normal upper limit. Related complications, including osteosarcoma, spinal stenosis, and giant-cell tumor were rare (Table 1).

Statistical analysis of the relationship between onset age and gender, and the correlation of TALP with gender and ostealgia. (a) There was no significant difference in clinical manifestations between different genders, as indicated by chi-square test (p = 0.144). (b) There was no significant correlation between TALP level and ostealgia, as indicated by chi-square test (p = 0.288). (c) There was no significant difference in TALP level between males and females, as indicated by chi-square test (p = 0.883). TALP, total alkaline phosphatase
There was an increase in the TALP level of 113 (89.7%) out of 126 patients, whose TALP levels could be obtained. Chi-square test results showed that there was no statistically significant correlation between TALP level and ostealgia (p = 0.288; Fig. 4b). In addition, we also analyzed differences in TALP level between males and females using chi-square test, and results indicated that there were no significant differences (p = 0.883; Fig. 4c).
3.5 Common clinical symptoms of PDB
The most common clinical symptom of PDB included ostealgia, followed by bone malformation. Hearing loss was the least frequently reported symptom. A total of 19 patients suffered fractures (Table 2).
3.6 Distribution of clinical departments
Our study also recorded the clinical departments at which patients with PDB were first diagnosed. Analysis revealed that the most common department was endocrinology, followed by orthopedics, followed by nuclear medicine, and occasionally the emergency department. No department records of 219 cases were obtained (Fig. 5).

Clinical departments at which patients with PDB were first diagnosed. Endo, endocrinology department; Ortho, orthopedic department; NS, neurosurgery department; Stoma, stomatology department; Rheu, rheumatology department; Hema, hematology department; Neuro, neurology department; Neph, nephrology department; NM, nuclear medicine department; EM, emergency department
3.7 Diagnostic methods used for patients with PDB
X-ray scans and evaluation of TALP levels were most commonly applied for diagnosis, and 40.7% of patients were diagnosed by clinical pathology. In addition, CT scan, RBS, and MRI were also used for diagnosis in a fraction of patients (Table 3).
3.8 Treatment methods for patients with PDB
The most frequently used drugs included calcitonin and bisphosphonates. Around 36.4 and 30.6% of patients were found to be administered calcium and vitamin D, respectively, and 27.3% of patients underwent surgery for bone malformation or fractures (Table 4).
In this review, we also analyzed the status of PDB treatment in mainland China over different time periods. Data indicated that etidronate disodium was used as the principal drug before 2000, pamidronate disodium and calcitonin were used from 2000 to 2009, and zoledronate gradually started being used after 2010 (Table 5).
3.9 Clinical manifestations of PDB in different countries
Data on onset age were gathered for middle-aged and elderly PDB patients in various countries. The incidence of the disease among males was higher than that among females in mainland China, the UK and the USA, Japan inversely. The number of monostotic cases was slightly higher in other countries, except the USA, where polyostotic cases were more commonly reported. The commonly involved bones and clinical manifestations were different between countries. The treatments mainly included bisphosphonates and calcitonin. Familial aggregation was rarely reported in mainland China and Japan; however, no data were obtained for the other two countries. The gender ratio of PDB patients was compared between mainland China and Japan using chi-square test, and a significant difference in morbidity between males and females was reported (p < 0.05). However, no significant difference in gender ratio was observed between mainland China and the USA (Table 6).
4 Discussion
This systematic review aimed to identify the clinical features of PDB in mainland China. Here, we analyzed 118 articles, including a total of 332 patients with PDB, in which 10 cases were familial. Family aggregation was not distinct in mainland China. In Japan, where PDB-related morbidity is low, familial incidence was around 6.3%, which was lesser than that in the USA (12.3%) [3] and the UK (13.8%) [4]. We found that the number of PDB cases significantly increased after 2000. However, whether this was due to increased morbidity or improved diagnosis and treatment remains to be confirmed by more epidemiological data. Our data indicated that PDB incidence is associated with regional disparity in mainland China, which is in accordance with a previous study that reported the prevalence rate of PDB in 17 towns in the UK [13].
The age of patients included in this study ranged from 2 months to 86 years, the peak age being 46–60 years. The rate of incidence appeared to decrease with age, however, it remarkably increased in Japan and other countries with high PDB prevalence. The prevalence rate of PDB in males was found to be slightly higher than that in females in mainland China, which is similar to that in the USA and UK, but not Japan. A statistically significant difference in morbidity between sexes was observed between mainland China and Japan, but not between mainland China and the USA. Meanwhile, no significant differences between sexes in each age group were observed.
Based on the frequency of occurrence, PDB clinical symptoms were roughly similar between mainland China and Japan, USA, and UK. The numbers of monostotic cases were more than those of polyostotic cases in mainland China, and similar results were reported in Japan, but not the USA. In addition, the commonly involved bones were different among various countries. The femur was reported to be the most commonly affected bone in this study, which is consistent with previous studies in Japan [16] and the UK [137]. These data indicate that clinicians should be wary of the possibility of PDB when patients present with fractures at common parts without an apparent cause. Since studies on the occurrence of related complications have seldom been reported, the exact incidence rate of PDB complications remains unknown. In mainland China, PBD has rarely been complicated with osteosarcoma (0.9%), compared with that in Japan (1.8%) [16], as well as spinal stenosis (0.6%) and giant-cell tumor (0.3%),but the occurrence of malignant bone tumors was similar to some regions in the UK [138].
American researchers conducted a systematic review and a meta-analysis of PDB in 2015 [139], and reported that procollagen type 1 amino-terminal propeptide (P1NP) was a valuable indicator for PDB detection and to monitor TALP and bone alkaline phosphatase levels, and urine N-terminal telopeptide was also an essential marker for monitoring disease activity. PDB failed to be diagnosed using bone turnover markers, which are regarded as preferred indexes in primary screening and post-treatment re-examinations. A previous literature study [140] showed that approximately 95% of untreated patients displayed increased TALP levels, which is consistent with our findings. Moreover, two foreign studies [141, 142] showed that most patients with increased TALP presented with ostealgia. In our study, 85 out of 113 (75.2%) PDB patients with elevated TALP levels had ostealgia, indicating an association between the metabolic activity of PDB and ostealgia. Nevertheless, we analyzed the correlation between TALP level and ostealgia as well as TALP levels between males and females, and results showed no significant correlation and differences, respectively.
In mainland China, most PDB patients were diagnosed at the endocrinology and orthopedics department, indicating that this disease may not be well understood by physicians of other departments where PDB patients were diagnosed rarely, which may lead to a missed or delayed diagnosis. Therefore, improving PDB recognition by these physicians is of great importance.
In this study, PDB was diagnosed based on X-ray scans and TALP levels. Additionally, RBS, CT, MRI, and bone pathology tests were also used for diagnosis in a fraction of cases. However, CT and MRI are not recommended as routine examinations in western countries based on their clinical guidelines, in which bone pathology is not put forward, as they may result in wastage of medical resources and increase of financial burden and medical risk in patients. Our findings indicated that in China when considering the diagnosis of PDB, X-ray scans combining with TALP levels should be also preferred as the first-line diagnostic methods. Thus, this may contribute to improving PDB diagnosis efficiency and treatment in terms of saving medical resources and expense of patients.
PDB is a chronic disease, and its development can be controlled by early diagnosis and treatment. Clinical guidelines in western countries [143,144,145] recommend bisphosphonate as the primary drug, with zoledronate being the most effective. In 2017, a cohort study [146] of 107 patients administered zoledronate was conducted, including a 10 year-follow up. P1NP levels were monitored, and low recurrence rates and lasting effects were observed. Moreover, randomized, placebo-controlled clinical trials have demonstrated that bisphosphonates can effectively reduce bone turnover [141, 147, 148], improve ostealgia [147, 149], and promote healing of osteolytic lesions [141] and recovery of bone tissues [141]. Another study showed that bisphosphonates could be used to prevent related complications of PDB [150]; however, this requires further validation [151]. In case of patients presenting with fractures, surgery is a common treatment choice. The percentage of surgeries were found to high according to our study (27.3%), which may be due to lack of knowledge of PDB among Chinese clinicians, leading to non-systematic early diagnosis and medical therapy.
This study had certain limitations. Since PDB is a rare disease, resulting in the lack of extensive epidemiological data, our study included a small sample size. Missing data in the included articles and the quality of literature together may have contributed to possible bias to the interpretation of the clinical features of PDB. However, this is the most detailed systematic analysis and evaluation of the clinical characteristics and the status of diagnosis and treatment of PDB in mainland China among other studies that have been reported so far.
In conclusion, this study revealed that familial aggregation in PDB was not obvious among patients in mainland China, and sporadic cases were higher. The clinical manifestations of PDB mainly included ostealgia, bone malformation, hearing loss, and fracture, and bisphosphonate was the primary drug used for treatment. These findings were similar to those reported in Japan, UK, and USA.
References
Papapoulos SE. Paget’s disease of bone: clinical, pathogenetic and therapeutic aspects. Baillière’s Clin Endocrinol Metab. 1997;11(1):117–43.
Paget J. On a form of chronic inflammation of bones. (Osteitis deformans). Clin Orthop Related Res. 1966;49(1):37–64.
Siris ES, Ottman R, Flaster E, et al. Familial aggregation of Paget’s disease of bone. J Bone Miner Res. 1991;20(3):541–7.
Sofaer JA, Holloway SM, Emery AE. A family study of Paget’s disease of bone. J Epidemiol Comm Health. 1983;37(3):226–31.
Eekhoff EW, Karperien M, Houtsma D, Zwinderman AH, Dragoiescu C, Kneppers AL, et al. Familial Paget’s disease in the Netherlands: occurrence, identifi cation of new mutations in the sequestosome 1 gene, and their clinical associations. Arthritis Rheum. 2004;50(5):1650–4.
Chung PYJ, Hul WV. Paget’s disease of bone: evidence for complex Pathogenetic interactions. Semin Arthritis Rheum. 2012;41(5):619–41.
Barker DJ, Gardner MJ. Distribution of Paget’s disease in England, Wales and Scotland and a possible relationship with vitamin D deficiency in childhood. British J Preventive Social Med. 1974;28(4):226–32.
Siris ES. Epidemiological aspects of Paget’s disease: family history and relationship to other medical conditions. Semin Arthritis Rheum. 1994;23(4):222–5.
Lopez-Abente G, Morales-Piga A, Elena-Ibanez A, et al. Cattle, pets, and Paget’s disease of bone. Epidemiology. 1997;8(3):247–51.
Lever JH. Paget’s disease of bone in Lancashire and arsenic pesticide in cotton mill wastewater: a speculative hypothesis. Bone. 2002;31(3):434–6.
Siris ES. Seeking the elusive aetiology of Paget’s disease: a progress report. J Bone Miner Res. 1996;11(11):1599–601.
Ralston S, Langston AL, Reid IR. Pathogenesis and management of Paget’s disease of bone. Lancet. 2008;372(9633):155–63.
Barker DJ, Chamberlain AT, Guyer PB, Gardner MJ. Paget’s disease of bone: the Lancashire focus. Br Med J. 1980;280(6222):1105–7.
Cooper C, Harvey NC, Dennison EM, van Staa TP. Update on the epidemiology of Paget’s disease of bone. J Bone Miner Res. 2006;21(S2):3–8.
Takata S, Hashimoto J, Nakatsuka K, Yoshimura N, Yoh K, Ohno I, et al. Guidelines for diagnosis and management of Paget’s disease of bone in Japan. J Bone Miner Metab. 2006;24(5):359–67.
Hashimoto J, Ohno I, Nakatsuka K, Yoshimura N, Takata S, Zamma M, et al. Prevalence and clinical features of Paget’s disease of bone in Japan. J Bone Miner Metab. 2006;24(3):186–90.
Wat WZ, Cheung WS, Lau TW. A case series of Paget’s disease of bone in Chinese. Hong Kong Med J. 2013;19(3):242–8.
Xu ZD,Gao ZH,He Q.Clinical meta analysis of 160 Chinese Paget’s disease. Chinese Integrative Medicine Endocrine and Metabolic Diseases Conference and Diabetes Forum,2012(in Chinese).
Bao YZ, Wu Q, Hu KH, et al. 1 case of left humerus osteitis deformans combining with pathologic fracture and literature review. Int Med Health Guidance News. 2015;21(24):3612–4 (in Chinese).
Chen J, Zhou L, Deng W. 4 cases of Paget’s disease of bone and literature review. Chinese Journal of Osteoporosis and Bone Mineral Research. 2015;8(1):33–8 (in Chinese).
Chen Y, Zhang DY, Li J, et al. 1 case report of Paget’s disease of bone. Clin Misdiag Mistherapy. 2012;25(6):29–30 (in Chinese).
Dai SJ, Yang P, Ye CX, et al. 1 case of skull osteitis deformans. Medical Frontier. 2011;1(20):105 (in Chinese).
Deng HZ, Deng ZJ, Wang AZ, et al. 1 case report of Chinese osteitis deformans. Med Information. 2013;(27):783(in Chinese).
Deng Y, Huo YN. 1 case report of osteitis deformans. Chinese J Osteoporosis Bone Min Res. 2016;9(1):65–7 (in Chinese).00.
Du HQ, Zheng Y, Zhang M, et al. 1 case of Paget’s disease of bone misdiagnosed as hemangioma. Chin J Endocrinol Metab. 2015;31(2):176–8 (in Chinese).
Fan BP, Li LL, Li XL. 1 case report of osteitis deformans. Chin J Osteoporosis Bone Min Res. 2016;9(2):183–5 (in Chinese).
Gao Y. 1 case report of osteitis deformans. Chinese Medical Innovations. 2012;9(1):152 (in Chinese).
Lao YQ, Li QB, Wang MS, et al. 1 case of tibia Paget’s disease of bone. Chin J Joint Surgery(Electronic Edition). 2017;11(1):94–6 (in Chinese).
Li W, Li G. 1 case report and analysis of osteitis deformans. Journal of clinical medical literature(Electronic Edition). 2017;4(48):9465–7 (in Chinese).
Li X, Zhao Y, Wang YP, et al. 1 case of thoracic spinal stenosis caused by Paget’s disease. Chin J Bone and Joint Surgery. 2010;3(2):172–5 (in Chinese).
Liu CD, Zhang XG, Sun XP. 1 case of multiple scleromalacia. Guangdong Med J. 2011;32(19) cover 3(in Chinese).
Liu XY, Li XY, Deng XH, et al. 1 case of osteitis deformans combining with hypocalcemia and hypophosphatemia. Chin J Osteoporosis Bone Min Res. 2017;10(3):284–9 (in Chinese).
Long HQ, Li GS, Li HM, et al. Diagosis and treatment report of multiple-level osteitis deformans of lumbar vertebra. Chin J Surg. 2010;48(21):1677–8 (in Chinese).
Lv S, Wang XL, Zhao Y. 1 case of osteitis deformans. Chin J Med Device. 2012;25(9):35 (in Chinese).
Ma JT, Zhang L, Yu M, et al. 1 case of pathologic femoral shaft fracture caused by osteitis deformans. Chin J Surg Integrated Traditional Western Med. 2013;19(4):465–6 (in Chinese).
Ming K. 1 case of osteitis deformans diagnosed by 64 slice spiral CT. J Pract Med Techniques. 2010;17(6):548 (in Chinese).
Shi XT, Li HW, Qu Z, et al. 1 case of pathologic left femoral shaft fracture caused by osteitis deformans and literature review. Chin J Lab Diagnosis. 2018;22(1):190–1 (in Chinese).
Wan Q, Zhang XD, Cheng YF, et al. 1 case of osteitis deformans of whole skull. Chin J Neurosurg. 2014;30(7):689 (in Chinese).
Wang LN, Jia MF, Li T. Et al. 1 case of Paget’s disease of bone and literature review. Chin J Hematol. 2014;35(6):561–2 (in Chinese).
Wen HJ, Yang YM. Analysis of an atypical osteitis deformans. Chinese Journal of Misdiagnostics. 2011;11(15):3698 (in Chinese).
Wu RZ. 2 cases of polyostotic osteitis deformans. Sichuan Medical Journal. 2010;31(2):270 (in Chinese).
Wu W, Yao XX, Yang NJ, et al. A case report of osteitis deformans of mandibular symphysis and literature review. J Jilin Med College. 2015;36(3):187–8 (in Chinese).
Xiao TY, Wang R, Sun J, et al. 1 case of Paget’s disease of jaw. J Oral Sci Res. 2015;31(1):90–1 (in Chinese).
Xu ZD, Gao ZH, He Q, et al. Clinical analysis of 4 cases of Paget’s disease of bone. National Medical Journal of China. 2011;91(36):2582–4 (in Chinese).
Yu XX. 1 case analysis of osteitis deformans of rib. Chronic Pathematology Journal. 2010;12(1):68 (in Chinese).
Yue YH,Lin Y,Cao Y, et al. 2 cases of Paget’s disease of bone misdiagnosed as metastatic tumor of bone and literature review. Jiangsu Med J. 2017;(2): 80–3 (in Chinese).
Zhang F. 1 case of skull Paget’s disease of bone and literature review. Chin J Coal Industry Med. 2013;16(3):513–4 (in Chinese).
Zhang S, Luo J. 2 cases of skull osteitis deformans. Guangdong Med J. 2013, 2913;34(19) (in Chinese).
Zheng JL, Hu YS. 1 case of bilateral tibia osteitis deformans combining with venous thrombosis of the lower limbs. J Clin Orthopaedics. 2010;13(6):718 (in Chinese).
Zheng Y, Du HQ, Zhang ZL. Analysis of clinical diagnosis and treatment of 6 osteitis deformans. Chin J Endocrinol Metab. 2015;31(2):139–42 (in Chinese).
Zeng YF. Analysis of treatment of atypical osteitis deformans. For All Health. 2012;6(23):39–40 (in Chinese).
Wang YJ. Imaging manifestation of 4 case of osteitis deformans. J Chin Physician. 2011;13(6):826–8 (in Chinese).
Wang DW,Wang RF. Imageology study of Paget’s disease of bone with 11 case reports. Radiologic Practice. 2011;(6): 641–4(in Chinese).
Li J. Imaging diagnostic analysis of osteitis deformans. J Clin Med Literature. 2014;1(7):292 (in Chinese).
Liu YK, Chen W, Guo HL, et al. Imaging diagnosis of osteitis deformans. J Pract Radiol. 2012;28(11):1745–9 (in Chinese).
Bao CH, Zhang ZL. Analysis clinical diagnosis and treatment of 8 osteitis deformans. Shanghai Med J. 2012;35(6):139–42 (in Chinese).
A Si Ka Er·Mai Mai Ti Ming, Tian H, Yu CH. 1 case of osteitis deformans. J Xinjiang Med Univ. 2000 (02):170(in Chinese).
Fang D, Zhang DS. 1 case report of jaw osteitis deformans. Shandong Medical Journal. 2005;45(33):74–5 (in Chinese).
Gong CJ, Wang A, Xi Y, Xue S. 1 case of osteitis deformans. Chin J Neurosurg. 2000;16(3):142 (in Chinese).
He D, Ping FY, Xu X, et al. Diagnosis and treatment of jaw Paget’s disease. Preventive Medicine. 2004;16(10):63–4 (in Chinese).
He W, Liu W, Chen WM. 1 case report of jaw symmetric multiple osteitis deformans and literature review. J Clin Stomatol. 2008;24(11):682–3 (in Chinese).
Hu ZY, Yang YL, Huang ZX. Analysis of 1 case of right tibia osteitis deformans. Chin J Misdiagnostics. 2008;8(16):3996 (in Chinese).
Huang G, Zhao JG, Wang XM, et al. 1 case of persistent dizziness caused by Paget’s disease of bone. J Chin Phys. 2009;11(10):1440 (in Chinese).
Li P, Wang QX, Li H, et al. Imaging manifestations and clinical pathology of osteitis deformans(attaching 2 case reports). Modern Med Imagel. 2005;14(1):7–9 (in Chinese).
Li CP, Qiu L. 1 case of osteitis deformans and literature review. J Inner Mongolia Med Univ. 2006;28(5):446–8 (in Chinese).
Li JF. 1 case of osteitis deformans combining with skull cyst. Chin J Diff Complicated Cases. 2008;7(2):76 (in Chinese).
Li N, Chen Y, Jia SQ. 1 case of skull osteitis deformans combining with brain glioma. J Clin Radiol. 2003;22(3):257 (in Chinese).
Li SZ, Kuang FY, Wu ZJ. 1 case of osteitis deformans. J Clin Res. 2001;18(3):239 (in Chinese).
Liu FX. 2 cases of osteitis deformans. Acta Academiae Medicinae Weifang. 2007; 29(4):cover 3,I(in Chinese).
Liu FX, Yu MX, Cao J. 3 case reports of osteitis deformans and literature review. Chin J Misdiagnostics. 2008;8(22):5504–5 (in Chinese).
Liu YH, LBE G. 1 case of misdiagnosed chronically Paget’s disease. Clin Misdiagnosis Mistherapy. 2005;18(10):716 (in Chinese).
Liu YZ, Shi CR, Zhou XF, et al. 1 case of osteitis deformans. Modern Med Imagel. 2005;14(6):285 (in Chinese).
Meng XB, Liu ZL, Li SB, et al. Analysis of 1 case of misdiagnosed Paget’s disease of bone. Chin foreign Health Abstr. 2011;8(43):219 (in Chinese).
Shao QT, Chang XM. 1 case of pelvis osteitis deformans. Heilongjiang Med Pharmacy. 2001;24(5):102 (in Chinese).
Song L. 1 case report of rib osteitis deformans combining with multilocular bone cyst. J Trad Chin Orthopedics Traumatol. 2001;13(12):62 (in Chinese).
Sun BJ. 1 case of osteitis deformans combining with fracture. J Clin Surg. 2004;12(12):728 (in Chinese).
Sun W, Li ZR, Wang BL. 1 case of varus deformity of bilateral femur caused by Paget’s disease. Chin J Misdiagnostics. 2007;7(16):3939–40 (in Chinese).
Wang SY, Li XH. 1 case of whole-body bone imaging of osteitis deformans and literature review. J Pract Med Imaging. 2008;9(4):247–8 (in Chinese).
Wang WG, Liang CH, Zeng H, et al. Imaging characteristics and pathological correlative study of Paget’s disease of early and middle term(attaching 1 case report and literature review). J Pract Med Imaging. 2001;2(4):232–4 (in Chinese).
Wang XL, Yang G, Lu JM, et al. Clinical analysis of Paget’s disease(osteitis deformans). Chin J Endocrinol Metab, 2008;24(4):412–4 (in Chinese).
Wang X, Liu JJ, Fu MH, et al. 1 case of monostotic osteitis deformans. Chin J Med Imaging. 2006;14(5):398–400 (in Chinese).
Wang Y, Xu XM. X-ray analysis of a case of osteitis deformans. J Med Radiol Technol. 2003;(6):45 (in Chinese).
Wu QB, Xu SW, Xu K, et al. 1 case report of multiple symmetric osteitis deformans. J Pract Orthopaedics. 2005;11(6, 559) (in Chinese).
Xie YP, Yang ZJ, Lu Y. Radionuclide bone imaging of a case of osteitis deformans. Int J Radiation Med Nuclear Med. 2008;32(4):217 (in Chinese).
Xu G, Bai L, Sun Y. 1 case of skull osteitis deformans ensuing malignant fibrous histiocytoma. Chin J Med Imaging Technol. 2009;25(8):1354 (in Chinese).
Yan TQ, Guo W, Shen DH. Osteitis deformans. Chin J Orthopaedics. 2002;22(2):100–2 (in Chinese).
Yang J, Xu HQ. 1 case report of osteitis deformans predominated by cardiac failure. Zhejiang Practical Medicine. 2000;5(5):64 (in Chinese).
Yang QS, Song SQ. 1 case report of osteitis deformans invading skull and femur. Chin Modern Med. 2005;3(10):84 (in Chinese).
Yang S, Wan GH, Gong SZ, et al. 1 case of Paget’s disease. Chin New Med. 2003;2(5):78–9 (in Chinese).
Yin MG, Liu HQ, He LQ. 1 case of right mid-femur amputation caused by right tibia osteitis deformans. Hebei Med J. 2004;26(1):121 (in Chinese).
Yu XT, Song XF. 1 case report of osteitis deformans diagnosed by CT scan. Chin Imaging J Integrated Traditional Western Med. 2004;2(2):121 (in Chinese).
Zhang LL, Cui SM, Liu ML, et al. 1 case of Paget’s disease. Chin J Med Imaging. 2001;9(6):473–4 (in Chinese).
Zhang ZH, Wang Y, Chen WJ, et al. 1 case report of osteitis deformans combining with vacuole turcica. J Pract Radiol. 2006;22(10):1213 (in Chinese).
Zheng J. 1 case of osteitis deformans diagnosed by X-ray plain film. Chin J Med Imaging Technol. 2009;25(6):948 (in Chinese).
Zhou H, Xie YC, Li KS. 1 case of osteitis deformans. Med Pharmacy Yunnan. 2001;22(5):430 (in Chinese).
Zhuo QJ, Wang RM, Su XF, et al. 1 case of osteitis deformans combining with skin mycosis fungoides. Chin J Endocrinol Metab. 2008;24(4):453–4 (in Chinese).
Liu HG, Cao QX, Lu MH. Osteitis deformans diagnosed by CT scan. J Pract Radiol. 2002;18(1):63–4 (in Chinese).
Qin QY, Li HF. Craniofacial osteitis deformans diagnosed by CT scan. J Pract Med Techniques. 2001;8(4):250–1 (in Chinese).
Sun DH, Lu HQ, Zhang RL. Value of X-ray in diagnosing osteitis deformans(attaching 20 cases analysis). J Med Imaging. 2000;10(2):105–6 (in Chinese).
Zhang JX, Liu JC, Yan D, et al. Clinical and imaging manifestation of osteitis deformans. Chin J Osteoporosis Bone Min Res. 2008;1(1):34–8 (in Chinese).
Yang J, Xu SD, Bai JJ, et al. Clinical,CT and X-ray manifestation of extensive lesion of skull(attaching 7 case reports). J Med Imaging. 2009;19(8):1031–3 (in Chinese).
Yang BT, Wang ZC, Xian JF, et al. Osteitis deformans diagnosed by HRCT. J Clin Radiol. 2001;20(4):321–2 (in Chinese).
Wei JJ, Sun Y, Guo BC, et al. 3 cases of Paget’s disease. J Rare Uncommon Dis. 2001;8(3):60–1 (in Chinese).
Wang J, Shi H, Chang JP, et al. Observation and nursing of treating 7 case of osteitis deformans with Pamidronate. Chin J Pract Nursing. 2005;21(22):8–9 (in Chinese).
Zhang ZL, Meng XW, Xing XP, et al. Prospective observation of treating osteitis deformans with pamidronate. Nat Med J China. 2003;83(19):1653–6 (in Chinese).
Fu AL, Zhao MF. 1 case of cancerated osteitis deformans. Henan J Oncol. 1996;(4):296(in Chinese).
Lin SP. 1 case of osteitis deformans. Modern Med Imagel. 1997;6(5):240 (in Chinese).
Liu FC, Li QY. 1 case of osteitis deformans combining with polycentric giant cell tumor of bone. China J Orthopaedics Traumatol. 1995;8(5):8 (in Chinese).
Liu LS, Liang P. 1 case of osteitis deformans. J Pract Med Techniques. 1997;4(5):394 (in Chinese).
Mi XY. 1 case report of osteitis deformans of lower jawbone. Med J Liaoning. 1990;4(2):93 (in Chinese).
Shao YP. 1 case report of osteitis deformans. J Med Theory Pract. 1991;4(1):38–9 (in Chinese).
Shen CW,Zhang HS, Jin XL. 1 case report of cancerated osteitis deformans. Acta Universitatis Medicinalis Secondae Shanghai. 1996;(6): 407–9(in Chinese).
Shen Y. 1 case of scleromalacia combining with hyperuricemia. J Med Theory Pract. 1998;11(2):89 (in Chinese).
Shi ZC, Su RG. Treatment of 2 cases of osteitis deformans. Chin J Clin Med. 1999;6(3):296 (in Chinese).
Sun T, Wu JM, Xiu SY. 1 case of osteitis deformans misdiagnosed as thoracic spinal tuberculosis. Qingdao Med J. 1997;29(12):18–9 (in Chinese).
Wu ZQ, Huang SZ. 1 case report of osteitis deformans. J Fuzhou Gen Hospital. 1999;6(3):46 (in Chinese).
Yan LF, Peng YZ. 2 case reports of osteitis deformans. J Med Radiol Technol. 1998; (2): 67–8(in Chinese).
Zhang RX, Zhao ZY, Chen BS, et al. Onset,diagnosis and treatment of osteitis deformans. J Traditional Chin Orthopedics Traumatol. 1997;9(4):23–4 (in Chinese).
Zhang SP, Zhang SD, Liu LP. Skull Paget’s disease diagnosed by CT scan(attaching 2 casereports). J Pract Med Imaging. 1997;1(2):52–3 (in Chinese).
Zhao XM. 1 case report of 22-year dynamic observation of osteitis deformans the whole course of disease by X-ray. J Pract Radiol. 1999;15(10):637 (in Chinese).
Cui JG, Li CM. X-ray analysis of 3 cases of osteitis deformans. Med Pharmacy Yunnan. 1997;(3):71(in Chinese).
Li AG, Niu BH. Clinical pathologic analysis of 4 cases of osteitis deformans. J Henan Univ (Med Sci). 1999;18(2):44–51 (in Chinese).
Meng XW, Xing XP, Liu HC, et al. Diagnosis and treatment of osteitis deformans. Chin J Endocrinol Metab. 1993;9(1):27–9 (in Chinese).
Cao QL, Shen W. 1 case report of lower jawbone osteitis deformans. J Modern Stomatol. 1989;(3):155(in Chinese).
Dong GH, Dong X. Pointing therapy of 1 case of osteitis deformans combining with paralysis. Shandong Medical Journal. 1983;(5):33(in Chinese).
Wang LC, Liu RS. 1 case of osteitis deformans.Henan Medicine. 1981;(4):57 (in Chinese).
Wang ZA, Wang MQ. 1 case report of scleromalacia. Chongqing Med. 1989;18(8):42 (in Chinese).
Xu QR, Lu JM. 1 case of osteitis deformans. J Shandong Med College. 1987;(9):46(in Chinese).
Zhou YN,Sun XR,Zhu XX. Osteitis deformans(Paget’s disease) of short tubular bone. Journal of Xinjiang Medical University.1982;(Z1):194(in Chinese).
Zhu B, He ZL, Liu HB, et al. 1 case report of pathological spondylolisthesis caused by osteitis deformans resulting in spinal stenosis. Railway Med J. 1983;11(3):191 (in Chinese).
Zheng ZM, Zhang XZ, Luo SX, et al. Osteitis deformans(Paget’s disease)—X-ray analysis of 10 cases. Acta Academiae Medicinae Sinicae. 1982;4(4):11,216–9 (in Chinese).
Cao LB. 2 cases of osteitis deformans(Paget’s disease). Shandong Med. 1964;(5):10(in Chinese).
Wu EH,Wang XS. Osteitis deformans(attaching 3 case reports). Tianjin Med J. 1961;(7):443–4,461(in Chinese).
Liu Z. 1 case of osteitis deformans. Chin J Anatomy Clin. 1998;3(1):12 (in Chinese).
Tang ZX, Yang ZY, Liu FJ, et al. 7 cases of hereditary osteitis deformans in a family. Chin J Endocrinol Metab. 1999;15(6):372 (in Chinese).
Davie M, Davies M, Francis R, et al. Paget's disease of bone: a review of 889 patients. Bone. 1999;24(suppl 2):S11–2.
van Staa TP, Selby P, Leufkens G, et al. Incidence and natural history of Paget’s disease of bone in England and Wales. J Bone Miner Res. 2002;17(3):465–71.
Nofal AAA, Altayar O, Benkhadra K, et al. Bone turnover markers in Paget’s disease of the bone: A Systematic review and meta-analysis. Osteoporosis Int. 2015;26(7):1875–91.
Alvarez L, Peris P, Pons F, Guañabens N, Herranz R, Monegal A, et al. Relationship between biochemical markers of bone turnover and bone scintigraphic indices in assessment of Paget's disease activity. Arthritis Rheum. 1997;40(3):461–8.
Reid IR, Nicholson GC, Weinstein RS, et al. Biochemical and radiologic improvement in Paget’s disease of bone treated with alendronate: a randomized, placebo-controlled trial. Am J Med. 1996;101(4):341–8.
Langston AL, Campbell MK, Fraser WD, et al. Randomized trial of intensive bisphosphonate treatment versus symptomatic management in Paget’s disease of bone. J Bone Min Res. 2010;25(1):20–31.
Singer FR, Hosking DJ, Lyles K, et al. Paget’s disease of bone: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2014;99(12):4408–22.
Muschitz C, Feichtinger X, Haschka J, Kocijan R. Diagnosis and treatment of Paget’s disease of bone:a clinical practice guideline. Wien Med Wochenschr. 2016;167(1–2):18–24.
Ralston S, Corral-Gudino L, Cooper C, et al. Diagnosis and Management of Paget’s disease of bone in adults: a clinical guideline. J Bone Miner Res. 2019;34(4):1–26.
Cundy T, Maslowski K, Grey A, Reid IR. Durability of response to Zoledronate treatment and competing mortality in Paget’s disease of bone. J Bone Miner Res. 2017;32(4):753–6.
Altman RD, Johnston CC, Khairi MRA, et al. Influence of disodium Etidronate on clinical and laboratory manifestations of Paget’s disease of bone (Osteitis Deformans). N Engl J Med. 1973;289(26):1379–84.
Fraser WD, Stamp TC, Creek RA, Sawyer JP, Picot C. A double-blind, multicentre, placebo-controlled study of tiludronate in Paget’s disease of bone. Postgrad Med J. 1997;73(862):496–502.
Ralston SH, Boyce BF, Cowan RA, Fogelman I, Smith ML, Jenkins A, et al. The effect of one alpha hydroxyvitamin D3 on the mineralisation defect in disodium etidronate treated Paget’s disease-a double-blind randomized study. J Bone Miner Res. 1987;2(1):5–12.
Lyles KW, Siris ES, Singer FR, Meunier PJ. A clinical approach to diagnosis and Management of Paget's disease of bone. J Bone Miner Res. 2001;16(8):1379–87.
Selby PL, Davie MWJ, Ralston SH, et al. Guidelines on the Management of Paget’s disease of bone. Bone. 2002;31(3):366–73.
Sun YF, Wang YC, Wang LC, et al. Analysis of mutation of SQSTM1 and TNFRSF11A gene in a family of Paget’s disease. J Shandong Univ (Health Sci). 2012;50(12):107–13 (in Chinese).
Acknowledgements
This work was supported by grants from the National Nature Science Foundation of China [grant numbers 81471091 and 81870622], the Hunan Nature Science Foundation [grant number 2018JJ2574] and Bethune Charitable Foundation, BCF [grant numer G-X-2019-1107-3].
Author information
Authors and Affiliations
Contributions
The study conception and design were performed by Sheng Zhifeng and Ou Yangna. Material preparation was performed by Fu Shanjiang, Wang Qinyi, Ding Na and Liu Shuying. Data collection and analysis were performed by Wang Qinyi,Fu Shanjiang,Chen Rong,Wen Zhangxin and Fu Sang. The first draft of the manuscript was written by Wang Qinyi and Fu Shanjiang. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Wang, QY., Fu, SJ., Ding, N. et al. Clinical features, diagnosis and treatment of Paget’s disease of bone in mainland China: A systematic review. Rev Endocr Metab Disord 21, 645–655 (2020). https://doi.org/10.1007/s11154-020-09544-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11154-020-09544-x