
Abstract
This paper explores the effect of teenage childbearing on long-term health outcomes and behaviors of mothers using the Midlife Development in the US dataset. Within-family estimations, using samples of siblings, and twin pairs, are employed to overcome the bias generated by unobserved family background and genetic traits. The results suggest no significant effects on health outcomes, and modest effects on health behaviors, including exercise and preventive care. However, accounting for life-cycle effects demonstrates that teenage childbearing has significant effects on both health outcomes and behaviors early in life, but very few significant effects later in life. Moreover, teenage childbearing has a particularly acute effect among minorities. Finally, this paper provides evidence that the effects operate through reduced income and labor force participation, and matching with a lower “quality” spouse.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
Teenage childbearing is a public policy concern, especially in countries with high teen birth rates, such as the United States.Footnote 1 Despite a decline in teen birth rates since 1990s (around 39 in 2009), the rates in the US are still high compared to other developed countries (Kearney and Levine 2012). Among the general public and policy makers, it is widely believed that teenage childbearing is a primary driver of poverty, leading to numerous adverse economic, educational, and health, consequences for mothers and their children.Footnote 2 However, with respect to empirical evidence, there exists several gaps in understanding the links between teenage childbearing and these adverse outcomes.
Early studies document that teen mothers are more likely to have less education, lower earnings, and to be welfare dependent, and are less likely to participate in the labor force. However, more recent and rigorous research does not support that teen childbearing has a causal impact on economic and educational outcomes. (For a survey of the literature, see Kearney and Levine 2012.) Rather than early childbearing causing adverse outcomes, it appears that the socioeconomic background and contextual factors are responsible for early childbearing.Footnote 3 Despite the recent attention in the literature, there are few studies examining the effects of teenage childbearing on health and health behaviors of mothers. In particular, the question of whether there are effects on health has yet to be explored.Footnote 4
The observed relationships between teenage childbearing and adverse health might be the result of underlying differences between teen and non-teen mothers (Kearney and Levine 2012). For instance, women with disadvantaged backgrounds are more likely to be teen mothers and to experience adverse outcomes even without a child as a teen. In order to address the problem of endogeneity of teenage childbearing on various outcomes, previous studies have used within-family estimations using data on pairs of sisters (Geronimus and Korenman 1992; Holmlund 2005), instrumental variables (IV) using twin births and miscarriage as instruments (Klepinger et al. 1999; Bronars and Grogger 1993; Hotz et al. 2005), and propensity score matching (Chevalier and Viitanen 2003). There is a small literature on the causal effects on health behaviors of mothers. Webbink et al. (2008) employ the within-family approach, using a sample of Australian twins and their relatives, and find that teenage childbearing leads to adverse health behaviors. However, Fletcher (2012) shows that teenage childbearing has negligible effects on health behaviors of mothers in the US using both within-family (sibling differences) and IV approaches (miscarriage as the instrument).
This paper estimates the effect of teenage childbearing (before the age of 20) on long-term health and health behaviors of mothers (aged 25–74 in the US in 1995/1996), using a nationally representative sample of twins as well as siblings from the Midlife Development in the United States (MIDUS) dataset.Footnote 5 I employ within-family estimations (fixed-effects (FE) approaches) using samples of siblings, and twin pairs in order to overcome the bias generated by unobserved family background and genetic traits that affect both the probability of becoming a teenage mother and health. More specifically, I compare the long-term health and health behaviors of teenage mothers to that of their (twin) sisters who had their first child after their teens. While within-family estimations eliminate the bias generated by unobserved family factors, this paper overcomes several of the concerns regarding family fixed effects by controlling for early life factors, such as birth weight and age at menarche, and restricting the sample to siblings that exhibit less observable heterogeneity.
This paper makes several contributions to the existing literature. First, while a few studies explore the effect of teenage childbearing on health behaviors of mothers, this is the first paper to use within-family estimations to explore the effect of teenage childbearing on health outcomes, including self-reported health, number of chronic conditions, and mental health. Second, this paper adds to the literature investigating the effects of teenage childbearing on health behaviors of mothers. While previous studies generally find insignificant effects on health behaviors, this paper finds several significant impacts on behaviors not previously examined. More importantly, this paper demonstrates significant life-cycle effects. Specifically, accounting for life-cycle effects demonstrates that teenage childbearing has significant effects on both health outcomes and behaviors early in life, but very few significant effects later in life. This paper also provides evidence that teenage childbearing has a particularly acute effect among non-white (minority) mothers. Finally, this paper also uncovers the mechanisms through which teenage childbearing influences health behaviors and outcomes, with primary mechanisms including labor force participation, income, and matching outcomes (spouse’s education and labor force participation).
2 Mechanisms
This section explores various mechanisms linking teenage childbearing and health. These mechanisms may be more relevant or acute for very young mothers, but are also relevant to mothers that are adult teenagers (ages 18 and 19).
The potential effects of teenage childbearing on health begin as early as the time of pregnancy and unfold over the lifetime of the mother. Early childbearing, even with the best possible prenatal care, might result in adverse health repercussions for the mother.Footnote 6 Moreover, younger mothers might devote less resources (e.g., time and money) to prenatal care due to financial or time constraints, lack of information, and various other reasons. Younger mothers might also be reluctant to seek the support of family and friends, perhaps even health professions, due to the real or perceived stigma associated with teenage pregnancy, thereby delaying prenatal care initiation and other preventive behaviors.Footnote 7 Teenage childbearing might also adversely affect mental health as documented by Liao (2003). In contrast, non-teenage mothers are more likely to be married and, more generally, in an environment that facilitates greater resources to health during the mother’s pregnancy.
Perhaps more importantly, the effects of teenage childbearing extend beyond childbearing. Teenage childbearing will likely impinge on the academic performance of the mother, perhaps even precluding maintaining a minimum level of performance, causing her to “drop out” of school.Footnote 8 Because teenage mothers will expect to earn less, and health is a normal good, teenage childbearing will result in reduced demand for health inputs, such as healthcare utilization, nutritious foods, physical activity, and so on. Moreover, because teenage mothers are less likely to be employed and earn less, it is possible that they face a higher effective price of health inputs due to lack of health insurance and tighter borrowing constraints for large health expenditures. The academic disadvantage of teenage mothers might also bear on health more directly, as education might confer a better understanding of the relationship between health behaviors—both positive and negative—and health outcomes. For example, Cutler and Lleras-Muney (2010) find that more educated people are more likely to exercise, seek preventive care, and to control their blood pressure. Moreover, greater education might result in greater efficacy at utilizing health inputs, such as following medical instructions and communicating with health professionals (Grossman 2006, 2003).
Teenage childbearing might also bear on assortative matching outcomes and fertility decisions. In particular, because teenage mothers are often unmarried, teenage mothers might match with lower quality spouses if potential mates have a preference for partners without children. Moreover, to the extent that teenage mothers are less educated and earn less, teenage mothers might also match with partners with less education and income. Because teenage mothers are less likely to continue education and to be employed in high-skilled occupations, they are subsequently less likely to interact with individuals with high education, which tend to have more healthy lifestyles. Finally, teenage childbearing might bear on fertility preferences, or the fertility preferences of their future partners, which in turn affects health through various channels.
Of course, not all of the effects of teenage childbearing are necessarily negative. In particular, parents of teenage mothers might respond by allocating more resources to support both the mother and child. Teenage childbearing might also increase the value of health to the mother, leading to an increase in health inputs or a decrease in risky behavior. Moreover, teenage mothers might be less likely to engage in social activities, which of course have benefits such as reduced stress, but might also be associated with behavior that adversely affects health (e.g., drinking, drug use). Finally, while childbearing might be onerous to the mother in the short run, the child will mature over time and may support the mother later in life. Because teenage childbearing might confer health benefits, the effect of teenage childbearing is an empirical question.
3 Empirical methodology
The within-family estimation uses the following econometric model:
where \(y_{ij}\) is the outcome of individual i in family j, \(T_{ij}\) is a dummy variable indicating whether the individual is a teenage mother, \(\mathbf {X}_{\mathbf {ij}}\) is a vector of control variables, \(f_{j}\) is an unobserved family effect common to all siblings (twins) within the same family, and \(\varepsilon _{ij}\) is a random error term. The family-specific effect (\(f_{j}\)) is removed from Eq. (1) by differencing between siblings, which removes the bias due to unobservable factors common to all siblings such as family endowments (genetic traits for twins). In this within-family specification (or family fixed effects estimation), it is assumed that differences in teenage childbearing within siblings are exogenous, conditional on the control variables.
While the data are discussed in the subsequent section, it should be noted that \(T_{ij}\) is defined as childbearing before the age of 20 in the baseline models. Because the effect of adolescent-teenage childbearing might be more acute than adult-teenage childbearing, the interpretation of \(\beta\) is the average effect of teenage childbearing. The median age of teenage mothers is 18, while the median age of non-teenage mothers is 22. The sensitivity of the results to alternative measures of teenage childbearing is explored in Sect. 6.
It should be noted that the within-family estimator is less biased than the cross-sectional estimator under certain conditions. Recall that the residual of the cross-sectional estimate consists of unobservable components that are directly related to the dependent variable and fertility (endogenous component) and indirectly related to the dependent variable through fertility (exogenous component). The within-family estimator is less biased if the family fixed effect accounts for a larger fraction of the endogenous component than the exogenous component.
While the previous literature points out that the within-family estimator is generally less biased, within-family estimations are potentially biased due to heterogeneity within families. Geronimus and Korenman (1992) acknowledge such heterogeneity in their comparison of sisters for estimating the effects of teenage childbearing on socioeconomics outcomes. Examples of sources of heterogeneity include variations in genetic endowments of siblings and in the way parents treat them (Rosenzweig and Wolpin 1988). Also, Bound and Solon (1999) emphasize that the differences in individual traits between siblings and in their environments over time are potential sources of bias in estimating returns to schooling.
I address the possible bias due to heterogeneity within families by using the within-family approach for samples of not only siblings but also twin pairs.Footnote 9 I also provide several robustness checks: (1) I control for early life factors in the twins sample, more specifically birth weight and age at menarche, (2) I exclude twins with large differences in the timing of their first birth, (3) I exclude twins who separated before 15 years old, and (4) I exclude twins who reported large differences in the way they dressed and had different childhood playmates. While focusing on twins, and excluding twins with observable hetereogeneity, reduces within-family heterogeneity, there is still the possibility of unobservable factors (e.g., motivation, risky behavior) that are correlated with the probability of teenage childbearing and health and health behaviors. To the extent that unobservable factors are positively correlated with teenage childbearing and adverse health outcomes and behavior, the within-family estimator represents an upper bound of the magnitude of the effect of teenage childbearing.
Another well-known concern is that the within-family estimator exacerbates measurement errors by differencing between siblings (twins), which may bias the estimates towards zero (Griliches 1979). In order to deal with measurement error, previous studies on the returns to schooling use various measures of schooling, including a measure of the respondent’s schooling reported by the co-twin (Ashenfelter and Krueger 1994; Ashenfelter and Rouse 1998). I discuss the issue of measurement error in the robustness checks section.
Finally, it should be noted that it is possible that teenage childbearing might impact the health and health behaviors of non-teen mothers. For example, teenage childbearing might result in an intra-household reallocation of resources to the teen mother or her child, at the expense of other siblings. On the other hand, teenage childbearing might result in siblings being less likely to engage in risky behavior or, more generally, to be more risk averse. To the extent that siblings are affected by teenage childbearing, siblings would not provide a valid counterfactual and would lead to a biased estimate.
4 Data
The data are from the first wave of the MIDUS survey.Footnote 10 The MIDUS is a nationally representative survey of 7108 non-institutionalized English-speaking individuals aged 25–74 in the US in 1995/1996.Footnote 11 The sample of 7108 individuals includes subsamples of 1914 twins and 950 siblings of the respondents. The total number of female siblings in the sample of at least two sisters is 1354 of which 768 are female twins (384 pairs).
MIDUS is a rich dataset, including socioeconomic and demographic characteristics, such as age, race, education, family background, number of children, and age at first birth. The dataset also includes information on health behavior and outcomes, which are discussed below. The sample is restricted to mothers who have a sister (twin) who is also a mother.
The primary independent variable of interest is teenage childbearing, which is a dummy variable indicating whether the women had a child before the age of 20. Other explanatory variables used in the paper are age at survey, race, age at menarche, and birth weight (available only for twins).
Figure 1 describes the distribution of age at first birth for the sample of siblings and twins. Among the sample of twins, about 23 % of mothers had their first birth before the age of 18, 18 % at the age of 18, 25 % at the age of 19, and 33 % at the age of 20 or older. The distribution is similar among the sample of siblings.

Distribution of age at first birth
The outcome variables are grouped into two categories: “health” and “health behaviors.” Following Lundborg (2013), the health outcomes investigated include self-reported health and chronic conditions. Because teenage mothers might experience disapprobation from peers, or even family members, I also investigate the impact on mental health. Self-reported health has been shown to be a strong predictor of mortality and morbidity (Idler and Benyamini (1997) survey the literature), and coded as the response to the question, “how would you rate your health these days?” ranging from 0 (“the worst possible health”) to 10 (“the best possible health”). Chronic conditions and diseases is the number of conditions experienced in the past 12 months. There are 29 chronic conditions, such as asthma, bronchitis, high blood pressure.Footnote 12 Mental health is a dummy variable equal to 1 if the women report excellent mental health, and 0 if otherwise (very good, good, fair, or poor).Footnote 13
Consistent with this paper, Fletcher (2012) finds that teenage childbearing does not significantly affect the following health and health behaviors: smoking, BMI, obesity, marijuana use, and drinking.Footnote 14 This paper also explores the following health behaviors: physical exercise and preventive care utilization. Physical exercise is measured as the number of times per month engaged in vigorous physical activity, while preventive care utilitization is measured as dummy variables indicating whether or not the responded had a blood pressure test and visited a doctor in the past 12 months.Footnote 15 Physical activity has both physical and psychological health benefits, including reduced risk of high blood pressure, colon and breast cancer, heart disease, type 2 diabetes, and reduced symptoms of depression and anxiety (WHO 2009). High blood pressure is another major leading cause of death in the US, particularly for women, and is responsible for approximately 17 % of adult deaths in 2005 (Danaei et al. 2009).
Tables 1 and 2 report summary statistics (sample means, standard deviations, and proportions) for the sample of women that are mothers and have at least one sister in the sample that is also a mother. There are 968 mothers in the cross-section sample (columns 1–2), of which 223 (23.04 %) had their first child before the age of 20. The within-family samples (columns 3–6) include sisters that have differential timing of their first births (teen and non-teen), which is used to identify the effect of teenage childbearing on various outcomes. The identifying sample for siblings consists of 107 teenage mothers and 121 sisters, while the identifying sample for twins consists of 67 teenage mothers and their twin sisters.Footnote 16
Table 1 demonstrates that “teen mothers” share similar personal and family characteristics as their “non-teen mothers” siblings, with of course the exception of age at first birth.Footnote 17 However, teen mothers have mostly worse health outcomes and health behaviors than non-teen mothers. Table 2 demonstrates that teen mothers are less likely to be married and to work for pay, have less education, have less individual and household income, have higher fertility, are more likely to have Medicaid, and are more likely to live with adult children or grandchildren. Moreover, teen mothers have spouses with lower education and income, and that are less likely to work for pay.
5 Empirical findings
Table 3 presents the estimates of the effects of teenage childbearing on health and health behaviors. Panels A and B report the results of ordinary least squares (OLS) estimation for the “cross-section” samples and FE estimation for the samples of siblings and twins where at least one of the siblings (twins) is a teenage mother. Standard errors are adjusted for clustering within families. The cross-section estimations control for age and race. For within-family estimations, the siblings sample (Panel A) controls for age, while age and race difference out in the twins sample (Panel B). The last rows of Panels A and B in Table 3 report the p value of F-tests for testing the null hypothesis that all family fixed effects are equal to 0. The null hypothesis is rejected in all estimations (except “doctor visit”), suggesting the presence of unobservable genetic and background factors.
5.1 Health
The OLS estimates reported in Table 3 suggest significant and negative associations between teenage childbearing and health for all health outcomes: teenage mothers report worse health, have more chronic conditions, and are less likely to report better mental health than their sisters (twins). However, the effects of teenage childbearing on health disappear once I control for family fixed effects (within-family estimations).
While the within-family estimations are statistically insignificant, some of the results do not warrant ruling out impacts that are potentially non-trivial in size. Using 95 % confidence intervals, the upper bound of the effect on self-reported health using siblings (twins) is \(-0.598\) (\(-0.807\)), which corresponds to 0.33 (0.42) standard deviations. Similarly, the upper bound effect on the number of chronic conditions is 0.17 (0.26) chronic conditions, which corresponds to 0.06 (0.09) standard deviations. Finally, the upper bound effect on the probability of reporting excellent mental health is 14 (19) percentage points.
5.2 Health behaviors
The OLS estimates reported in Table 3 suggest significant and negative associations between teenage childbearing and exercise and some preventive care behaviors (doctor visit). Controlling for family fixed effects results in significant effects on some preventive care behaviors (exercise and blood pressure test), but no significant effects on doctor visits.
The within-family estimates suggest that using the sample of siblings (twins) teenage childbearing reduces vigorous physical activity by 1 (1) activity per month, which corresponds to 0.16 (0.25) standard deviations. Similarly teenage childbearing reduces the probability of a blood pressure test by 10 (12) percentage points. While the doctor visit estimate is statistically insignificant, the upper bound, using a 95 % CI, is approximately 23 percentage points. In sum, the effect of teenage childbearing on health behaviors is statistically and economically significant for exercise and blood pressure test, and we cannot rule out the potential of economically significant effects for doctor visits.
5.3 Inference over multiple outcomes
The concern of incorrect inference (increase in Type I error) due to using multiple outcome variables is addressed by re-estimating the effects on overall indices. In order to improve the statistical power, I construct overall indices of health and health behavior using all of the outcomes.Footnote 18 The overall indices are obtained by using the principle components analysis (PCA) to determine the weights of standardized health and health behavior outcomes in the indices.Footnote 19
The last columns of Table 3 present the effects of teenage childbearing on the overall indices of health and health behavior. The coefficient estimates in the cross-section estimations suggest significant and negative associations between teenage childbearing and health and health behavior. However, the within-family estimates in Table 3 suggest no significant effects of teenage childbearing on health. On the other hand, the within-family estimates for health behavior index in Table 3 are negative and significant, indicating a negative effect of teenage childbearing on health behavior.
5.4 Life-cycle and heterogeneous effects
Section 2 highlights that the effect of teenage childbearing unfolds over the lifetime of the mother. The effects include both “short-run” effects, such as pregnancy complications and depression, and “long-run” effects, such as lower expected lifetime earnings and assortative mating outcomes, which in turn affect health. Because many of the short-run effects are not expected to directly bear on long-run health, and short-run constraints might be less binding over time, we might expect that teenage childbearing might have acute short-run effects and little or no effect later in life. For example, teenage mothers are less likely to be affected by social stigma later in life, and might re-enroll in schooling after the child reaches a certain age.
The effects of teenage childbearing, especially in the short-run, might also be mitigated by higher socioeconomic status. For example, minorities and, in general, disadvantaged groups might face even more acute discrimination as a result of teenage childbearing. Moreover, low-income households might not be able to afford high-quality prenatal care and mothers might be required to work after childbearing. On the other hand, high-income households might be able to afford high-quality prenatal care, as well as childcare and private schooling to accommodate the mother.
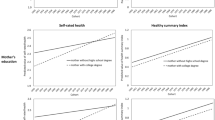
To account for life-cycle effects and heterogeneous effects, teenage childbearing is interacted with (i) dummy variables indicating whether the respondent is aged 25–34 and 35–45 at the time of the survey, (ii) a dummy variable indicating whether the mother is non-white, and (iii) a categorical variable of parental education ranging from 1 to 4.Footnote 20
Table 4 presents estimations using within-family variation for siblings and twins samples (odd and even columns, respectively) for health and health behaviors (Panel A and Panel B, respectively). Panel A and Panel B demonstrates mostly consistent evidence that the effect of teenage childbearing is most pronounced early in the lifecycle (25–34). Specifically, compared to teen mothers older than 46, teen mothers at the ages of 25–34 (35–45) have 1.4 (1.7) more chronic conditions and are 37 (20) percentage points less likely to report better mental health. Similarly, teen mothers engage in 5 (3) less vigorous physical activities per month than teen mothers older than 46, and are around 29 (26) percentage points less likely to visit a doctor. Moreover, the overall indices confirm this pattern.Footnote 21
The analysis of life-cycle effects has important policy implications, and provides a possible explanation why studies typically do not find significant adverse effects of teenage childbearing (Kearney and Levine 2012). With respect to the studies investigating the effect of teenage childbearing over the life cycle, Fletcher (2012) and Webbink et al. (2008) investigate the effect of teenage childbearing using subsamples of females according to age, and do not find evidence of life-cycle effects.Footnote 22 This study demonstrates that, using the entire sample of mothers (ages 25 and older), teenage childbearing has mostly insignificant and typically small effects on health and health behaviors. Accounting for life-cycle effects, however, results in several economically significant effects for women younger than 45, and especially women younger than 35, but very few effects for women over 45. This is indeed as expected for many of the health outcomes and behaviors. For example, accounting for life-cycle effects implies that teenage childbearing significantly affects mental health for women younger than 45, and especially women younger than 35, which is expected as the psychological effects of teenage pregnancy and the stigma associated with teenage childbearing are likely mostly worn off later in life. Similarly, teenage mothers are plausibly more time constrained, at least before the child reaches adulthood, and are therefore less likely to exercise and to visit the doctor.Footnote 23 However, after a certain age, teenage mothers are no less time constrained, and therefore exercise and visit the doctor as much as non-teenage mothers.
Table 4 also suggests that non-whites experience consistently greater adverse effects of teenage childbearing on health outcomes (Panel A). Specifically, teenage childbearing reduces self-reported health by nearly 3 additional points for non-whites, and results in around 2.5 additional chronic conditions for non-whites.Footnote 24 The overall index is also consistent with a greater impact of teenage childbearing for non-whites. However, non-whites do not experience significantly different effects on health behaviors. One tentative conclusion is therefore that non-whites experience greater adverse effects of teenage childbearing, despite the fact that they do behave differently as a consequence of teenage childbearing. Because non-whites experience greater adverse effects of teenage childbearing on self-reported health and chronic conditions, but not mental health, another tentative conclusion is that the reason they experience acute effects is due to tighter financial or time constraints, rather than an inability to cope with the psychological effects of teenage childbearing.
Table 4 provides some evidence that the effect of teenage childbearing on health behavior is particularly acute among mothers with less educated parents (Panel B). Specifically, the effect of teenage childbearing on preventive care (blood pressure test and doctor visit) is decreasing in parental education. There are multiple possible interpretations for this finding. First, high-educated parents might encourage teenage mothers, which lack information regarding the value of preventive care, to visit the doctor more often. Second, high-educated parents might also be high-income parents, which are more likely to support their children financially, especially when their child is a teenage mother.
5.5 Nonlinear effects
Defining teenage childbearing as a dichotomous variable allows for nonlinear effects of age at first birth, which is implicitly suggested by policymakers’ emphasis of the teen birth rate (as opposed to average age at first birth, for example). Consequently, the analysis abstracts from variation in the effect of teenage childbearing within teenage mothers, such as differences between adolescent- and adult-teenage mothers. This section explores various measures of teenage childbearing and age at first birth to shed light on the functional-form relationship with the outcomes of interest.
First, I use age 19 rather than 20 as the cutoff age for teenage childbearing.Footnote 25 Reducing the cutoff age to 19 reduces the average age of teenage mothers from 18.2 to 17.4. If the effect of teenage childbearing is more acute for younger mothers then reducing the cutoff age should increase the magnitude of the effects of teenage childbearing. Second, I use age at first birth as a continuous-type variable. Because within-family estimations are employed, variation in age at first birth is generated differences in age at first birth between siblings and twins for teenage mothers and non-teenage mothers. Differences in age at first birth are decreasing in the age of first birth of the teenage mother and increasing in the age of first birth of the non-teenage mother. Thus, the estimate captures the effect of decreasing age at first birth of the teenage mother by one year (for a given age of first birth of the non-teenage mother).
Table 5 reports the results, where columns (1) and (2) use the baseline age cutoff (c.f., the within-family estimations in Table 3), columns (3) and (4) use age 19 as the cutoff for teenage childbearing, and columns (5) and (6) employ age at first birth as a linear independent variable. Defining teenage childbearing as having a child before the age of 19 reduces the number of teen mothers to 59 and 35 for siblings and twins, respectively, thereby reducing the precision of the coefficients. The results demonstrate that reducing the cutoff age does not result in significant differences in the effect of teenage childbearing, suggesting that teenage childbearing is not more acute for younger mothers. The only exception is the blood pressure test outcome, which is more acute for younger mothers, though the differences are not statistically significant. Using age at first birth as a linear independent variable results in coefficients that are consistent with the baseline results. For example, because age at first birth among teenage mothers is 5 years less (on average) than age at first birth among non-teenage mothers, the implied effect of teenage childbearing on blood pressure test using the twins sample is \(0.123/5=0.025\), which is slightly larger than the corresponding estimate of 0.019 (column 6).
To gain insight into the functional-form relationship with the outcomes of interest, this paper also employs a wider range of measures of teenage childbearing and age at first birth, which are reported in the online Appendix C. Specifically, a quadratic term is added to the age at first birth independent variable, the teenage mother dummy is used with the age at first birth independent variable, the teenage mother dummy is interacted with the age at first birth independent variable, and the teenage childbearing dummy is split into a dummy variable for adolescent-teenage mothers and a dummy variable for adult-teenage mothers.
The primary reason to employ the wider range of measures of teenage childbearing and age at first birth is to shed light on the interpretation of the findings. One interpretation of the adverse effects of teenage childbearing is due to the fact that, in general, older mothers (within a range) have better health and health behavior outcomes. A second interpretation is that older mothers have better health and health behavior outcomes, but the effect is less general and diminishes at older ages. A third interpretation, which is suggested by policymakers emphasis of teen birth rates, is that childbearing before a given age leads to adverse health outcomes. Mathematically, the first interpretation suggests that a linear function of age at first birth should fit the data best, while the second and third interpretations suggest that a nonlinear function of age at first birth (such as a quadratic expression or a dummy variable for teenage childbearing) should fit the data best. Finally, using two teenage childbearing dummies sheds light on whether the effect of teenage childbearing is particularly acute for adolescent-teenage mothers.
Appendix C exhibits four noteworthy patterns that are supported in most specifications. First, age at first birth squared is always the opposite sign of age at first birth and its inclusion significantly increases the goodness of fit of the model, thereby suggesting that the relationship is nonlinear. Second, the coefficient for the teenage childbearing dummy is similar when age at first birth is added to the model. Moreover, inclusion of the dummy for teenage childbearing results in insignificant effects of age at first birth, but an overall improvement in goodness of fit of the model, again suggesting that the relationship is nonlinear. Similarly, interacting the dummy for teenage childbearing with age at first birth results in insignificant effects of age at first birth, suggesting that age at first birth among non-teenage mothers is not a significant determinant of health and health behaviors. Finally, the dummy variable for adolescent-teenage childbearing is not significantly different from the dummy variable for adult-teenage childbearing, with the exception of the blood pressure test outcome.Footnote 26
To summarize, the results point to a nonlinear relationship between age at first birth and the outcomes of interest. The results suggest that there is not significant variation in the adverse effects within teenage mothers, and that age of first birth is not significant after controlling for teenage childbearing. However, estimating the precise turning point for age at first birth such that childbearing generates adverse health consequences is constrained by the small sample size and the low frequency of adolescent childbearing.
6 Sensitivity analysis
In this section, I address the various concerns in within-family estimations, which were discussed earlier. First, additional controls are introduced in the estimations for the sample of twins. Second, the effects are re-estimated for smaller samples of twins excluding arguably different twins.
Previous studies have shown that birth weight is an important factor for various long-run outcomes, such as education, income, physical growth, and behavioral development (Behrman and Rosenzweig 2004; Black et al. 2007; Gupta et al. 2013).Footnote 27 Birth weight is available for only twins in the MIDUS data, and sample means in Table 1 show that teen mothers have lower birth weight, except for twins in the within-family sample. Earlier age at menarche has been shown to be positively correlated with teenage childbearing (Klepinger et al. 1999; Chevalier and Viitanen 2003). Sample means in Table 1 show that teen mothers experience slightly earlier menarche compared to non-teen mothers. Controlling for birth weight and age at menarche does not substantially change the main results, and moreover, the effect of teenage childbearing on vigorous physical activity becomes more significant (column 1 of Table 6).
Following Webbink et al. (2008), I re-estimate the effects for a sample of twins excluding the pairs who differ at least 10 years in the timing of their first birth (10 pairs, of which 4 pairs are identical twins), which is expected to reduce heterogeneity within twins. The results shown in column (2) of Table 6 are again similar to the main results.
The identifying assumption that the mother’s twin provides a counterfactual is less likely to hold in cases where twins display marked differences prior to childbearing or are exposed to different environments, including families and peers. Therefore, I exclude twins who report separation before the age of 15 (7 pairs), report not dressing alike or having dissimilar playmates as children, or both. The results are reported in columns (3)–(6) of Table 6. The results are not significantly altered by the restrictions and, in particular, the estimates of “vigorous physical activity” and “blood pressure test” are robust (\(-1.426\) and \(-0.148\), respectively).
Measurement errors in the main explanatory variable (teenage child-bearing) could bias the estimates towards zero. Following Webbink et al. (2008), I address the problem of measurement error by using IV estimations, using teenage childbearing in the follow-up survey in 2004 as an instrument.Footnote 28 Because the main estimation results are biased towards zero, the IV estimates are generally larger, and statistical significance is similar (available upon request). Recall the main estimations exclude teenage mothers without siblings that are also mothers. However, childless siblings in the 1995/1996 survey might become mothers in the follow-up survey. The main estimations are robust to the inclusion of siblings and twins where childless females become mothers in the follow-up survey (available upon request).
7 Exploring the mechanisms
This section explores potential mechanisms through which teenage childbearing affects health. The mechanisms explored include education, number of children, marriage, child’s age, health insurance (Medicaid), living with adult child or grandchild, labor force participation, income, household income (sum of mother and spouse’s income), and various dimensions of spouse’s quality (education, labor force participation, and income).Footnote 29
Various approaches to uncover the mechanisms are used, including employing the mechanisms as outcome variables using within-family estimations for samples of siblings and twins, and using traditional mediation analysis.
Table 7 presents the effects of teenage childbearing on the mechanisms. The results demonstrate that teenage childbearing reduces education, income, household income, labor force participation, and the quality of the spouse (spouse’s income and education), and increases the number of children, while it does not affect the probability of being married or covered by Medicaid, living with adult child/grandchild, and the spouse’s labor force participation.Footnote 30 The within-family estimates using the sample of twins suggest that teenage childbearing reduces the probability of high school graduation, attending college, and labor force participation by 19, 11, and 13 percentage points, respectively. Similarly, teenage childbearing reduces the probability that the husband attends college by 14 percentage points. Teenage childbearing also reduces income, household income, and spouse’s income by about 3 income categories, which corresponds to an average increase of $3000. Finally, teenage childbearing leads to 0.3 more children.
While determining the extent that teenage childbearing bears on the mechanisms narrows down the set of mechanisms, establishing that these variables are mechanisms requires investigating if these mechanisms are also significant determinants of health and health behavior. To this end, I estimate the mediation (indirect) effect for all of the mechanisms using the Baron–Kenny approach (Baron and Kenny 1986). Specifically, the mediation effect is the product of the coefficient of teenage childbearing using the mechanisms as dependent variables and the coefficient of the mechanism using the health and health behavior outcomes as dependent variables (after controlling for teenage childbearing). That is, the mediation effect is the effect of teenage childbearing through various mechanisms.
Table 8 presents the coefficients of the mediation effects and their associated standard errors (calculated using the delta method) and p values. Table 8 also reports the ratio of the mediation (indirect) effect to the overall effect. This ratio can be interpretation as the mediation effect as a proportion of the overall effect of teenage childbearing on health and health behaviors, where the overall effect consists of both the direct and indirect effects.
Because there are many potential mechanisms, the mediation effect of each mechanism tends to be relatively small, and the probability of rejecting the null when it is not correct (statistical power) is therefore relatively low. Consequently, the coefficients of the mediation effects are not statistically significant. Nevertheless, the magnitude of the ratios of the indirect effect to the overall effect might provide some (limited) evidence regarding their importance. The results suggest that labor force participation, income, and matching outcomes (spouse’s education and labor force participation) are the primary potential channels. For example, the effect of teenage childbearing through income accounts for 25 % and 13 % of the overall effect of teenage childbearing on vigorous physical activity and health behavior index, respectively. Similarly, labor force participation, and spouse’s education and labor force participation accounts for 18 % (13 %), 14 % (11 %), and 11 % (6 %) of the overall effect on physical activity (health behavior index), respectively. On the other hand, the results provide less support that the effect of teenage childbearing is mediated through education, the number of children, marital status, health insurance, living with adult/grandchild, household income, and the spouse’s income.
This paper also employs the mechanisms as additional control variables in determining health behaviors and overall indices of health and health behaviors. If adding the mechanism reduces the effect of teenage childbearing then the mechanism is more likely to be important. On the other hand, if the effect does not change then it is less likely to be a potential mechanism. The results using the sample of twins are presented in an online appendix (Appendix D).Footnote 31 The results in Appendix D point to the same set of important mechanisms as the inclusion of labor force participation, income, and matching outcomes, tends to reduce the magnitude of the effect of teenage childbearing (i.e., the direct effect) on health and health behaviors.
8 Conclusion
This paper uses within-family estimations to explore the effects of teenage childbearing on health outcomes and behaviors of mothers in the US. While cross-sectional estimates suggest significant negative associations between teenage childbearing and health, the effects are mostly insignificant and small in magnitude after controlling for family fixed effects. Specifically, the results suggest no significant effects of teenage childbearing on self-reported health, chronic conditions, mental health, and doctor visit. There is, however, evidence that teenage mothers are less likely to have had a blood pressure check in the past 12 months, and engage in less vigorous exercise.
This paper also demonstrates accounting for life-cycle effects results in several economically significant effects for women younger than 45, and especially women younger than 35, but very few effects for women over 45. The conclusion that teenage childbearing does not result in adverse impacts for the mother might be the consequence of not differentiating the effects over the lifecycle. This study adds support to policy makers concern regarding teenage childbearing, with the caveat that most adverse impacts diminish over time. This paper also demonstrates that minorities experience greater adverse effects of teenage childbearing on health outcomes. Similarly, teenage mothers with less educated parents tend to exercise less and are less likely to visit the doctor. As a result, reducing teenage pregnancy among minorities, and possibly other disadvantaged groups, might be particularly important.
Finally, this paper also uncovers the mechanisms through which teenage childbearing influences health behaviors and outcomes. Specifically, the effect may operate through reduced income and labor force participation, and matching with a lower “quality” spouse in terms of education and labor force participation. However, education, the number of children, marital status, health insurance, living with adult/grandchild, household income, and the spouse’s income do not appear to account for the effects of teenage childbearing.
Notes
In the US, the teen birth rate rose from 50 to 55 births per 1000 women between the ages of 15 and 19 in the late 1970s to around 60 in the early 1990s.
Birth rate before the age of 20 is a standard measure of teenage childbearing used by government agencies such as the Centers for Disease Control and Prevention. While the negative effects might be more acute for adolescent mothers, nearly three in four teen births occur between the ages of 18 and 19 in 2013 (Hamilton et al. 2015).
Inequalities in early life can be responsible for teenage pregancy, and investments in early stages of childhood might reduce disparities in later stages of life (Doyle et al. 2009).
Defining teenage childbearing as childbearing before the age of 20 is standard in the literature (Geronimus and Korenman 1992; Ribar 1994, 1999; Klepinger et al. 1999; Webbink et al. 2008, 2011; Fletcher 2012). The implications of this definition are discussed in Sect. 3, and I demonstrate that the results are similar excluding childbearing of aged 19.
For example, younger women are at a greater risk of pregnancy complications, such as anemia (Mirowsky and Ross 2002).
While there might be more stigma associated with adolescent fertility, many adult teenage pregnancies are out of wedlock, at least at the time of conception, which is often viewed disfavorably, especially among those with religious or traditional views of marriage.
Dropping out refers to not graduating high school or not attending and completing post-secondary education. While graduating college might not be essential in developing countries, a large fraction of the population in the United States attains an Associate or Bachelor’s degree, and studies document a large college-wage premium, especially among women (Katz and Murphy 1992; Card 1999; Dougherty 2005).
While the medical literature suggests that adult health outcomes between fraternal and identical twin pairs are not significantly different (Christensen et al. 1995; Duffy 1993), I also use a sample of identical twins. Because the number of identical-twin pairs is small (27 pairs), I focus on the results for the samples of twins, which, consistent with the medical literature, are similar to the results for identical twins (available upon request).
See Lundborg (2013) for an assessment of the representativeness of the MIDUS sample. Compared to the 1995 CPS data, the MIDUS sample contains more educated individuals than the general US population. Also, there are more whites in the siblings and twins samples (over 90 %), compared to the CPS sample (about 85 %).
Chronic conditions and diseases are the leading causes of death and disability, and are among the most costly health problems in the US (http://www.cdc.gov).
Because very few women reported fair and poor mental health (23 among twins sample), this paper does not use poor mental health as the main outcome. 20 % of the twins sample reported excellent mental health. Mental health disorders are the leading cause of disability in the US, are associated with increased prevalence of chronic diseases and lower participation in health-promoting behaviors, and are costly conditions (http://www.cdc.gov and http://www.ahrq.gov).
The estimates are reported in an online appendix (Appendix A).
Examples of vigorous physical activity in the survey are running or lifting heavy objects. An alternative measure of physical exercise, the number of times per month engaged in moderate physical activity (examples in the survey are bowling or using a vacuum cleaner) yield similar results.
Note that sample of siblings (twins) where at least one is a teenage mother is used in the analysis, and only siblings (twins) in the identifying samples identify the teenage childbearing coefficient (see Table 3 for observation numbers).
Teen mothers and non-teen mothers obviously have the same set of parents, thus, differences in parental education is due to a positive correlation between the number of “non-teen mothers” siblings and parental education.
In order to create the indices, each outcome is rescaled to map higher values to better health or health behaviors. Then, the z-score of each outcome is calculated by subtracting the mean of mothers who did not have teenage childbearing and dividing by the corresponding standard deviation.
PCA is a statistical technique of data reduction, which converts the correlated variables into an uncorrelated linear combinations of variables (principal components) that account for most of the variance. Following Kling et al. (2007), an equally weighted average of z-scores is also used to construct the indices; however, the results are consistent with using the PCA method (results are available upon request).
Following Lundborg (2013), education ranges from 1 to 4 based on the following categories: less than high school, GED or high school diploma, some college (no BA degree), and college degree or more. Following the approach of Ashenfelter and Krueger (1994), which is used by Lundborg (2013), the reports of siblings (twins) for parental education are averaged before obtaining a categorical parental education variable to address measurement error. In addition, the report of the sibling (twin) is used if there is only one report.
An alternative approach to explore life-cycle effects is to estimate the effect of teenage childbearing on health and health behaviors in the follow up survey (2004/2006) conditional on health and health behaviors in 1995/1996. The results (see online appendix–Appendix B) provide some evidence of convergence over the lifecycle; however, the results are imprecise due to potential attrition bias and small sample size.
In particular, Fletcher (2012) splits the sample into two using 45 as an age cutoff, while Webbink et al. (2008) restrict the sample to females older than 40. Both studies do not find significant differences using the various subsamples. I also re-estimate the life-cycle effects by splitting the sample (rather than using interactions) and find similar results as reported in Table 4 (available upon request).
Mullahy and Robert (2010) find that having kids ages 0–5 is associated with about 2 fewer minutes of exercise.
These results are imprecise as there are only 25 (12) and 18 (9) non-white mothers (families) in the samples for siblings and twins, respectively.
I did not set the threshold to age 18 because the number of teen mothers are significantly reduced (25 and 14 in the samples of siblings and twins).
The caveat applies that failing to find significant differences between adolescent-teenage childbearing and adult-teenage childbearing does not necessarily imply the effects are the same.
Conley et al. (2006) find that associations between birth weight and infant mortality for identical and fraternal twins vary by gestational age, which suggests that the role of genes or environment in birth weight-mortality associations vary across different situations. Therefore, within-twins estimations may not control completely for genetic endowments at conception. Moreover, Stenberg (2013) emphasizes the gene and environment interactions in interpreting the heritability estimates. It should be noted that the purpose of using twin data in this paper is to control for unobserved endowments.
The two measures are different for 5 observations in the sample of twins.
Education is measured as dummy variables indicating whether the respondent (at least) graduated from high school or attended college. Married and Medicaid indicate whether the respondent is currently married and covered by Medicaid. Child age is the age of the youngest child. Living with adult child/grandchild indicates whether the respondent lives with an adult child or grandchild at the time of the survey. Labor force participation indicates whether the respondent (spouse) is currently working for pay. Income is annual personal income of the respondent (spouse) in the past 12 months before taxes, excluding pensions, investments, or any other financial assistance/income, which ranges from 1 to 13 for different income levels (loss, 0/none, 1–1000, 1000–1999, 2000–2999,..., 100,000 or more).
These results are consistent with recent studies exploring the effects of labor market outcomes on mental health and the effects of childbearing on labor market decisions. For example, Mendolia (2014) shows that spouse’s job loss decreases individual and family mental health, which could be explained by the decrease in household income, and Herrarte et al. (2012) show that having a newborn has a negative effect on women’s labor market decisions.
Note that introducing the mechanism as a control variable also reduces the sample size due to missing values. Therefore, direct comparison of Appendix D with the results reported in Table 3 has limitations.
References
Ashenfelter, O., & Krueger, A. (1994). Estimates of the economic return to schooling from a new sample of twins. American Economic Review, 84(5), 1157–73.
Ashenfelter, O., & Rouse, C. (1998). Income, schooling, and ability: Evidence from a new sample of identical twins. Quarterly Journal of Economics, 113(1), 253–84.
Baron, R. M., & Kenny, D. A. (1986). The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51, 1173–1182.
Behrman, J., & Rosenzweig, M. (2004). Returns to birthweight. Review of Economics and Statistics, 86(2), 586–601.
Black, S. E., Devereux, P. J., & Salvanes, K. G. (2007). From the cradle to the labor market? The effect of birth weight on adult outcomes. Quarterly Journal of Economics, 122(1), 409–439.
Bound, J., & Solon, G. (1999). Double trouble: On the value of twins-based estimation of the return to schooling. Economics of Education Review, 18(2), 169–182.
Bronars, S., & Grogger, J. (1993). The socioeconomic consequences of teenage childbearing: Results from a natural experiment. Family Planning Perspectives, 25(4), 156–161.
Card, D. (1999). The causal effect of education on earnings. In Handbook of Labor Economics. New York: Elsevier.
Chevalier, A., & Viitanen, T. (2003). The long-run labour market consequences of teenage motherhood in Britain. Journal of Population Economics, 16(2), 323–343.
Christensen, K., Vaupel, J. W., Holm, N. V., & Yashin, A. I. (1995). Mortality among twins after age 6: Fetal origins hypothesis versus twin method. British Medical Journal, 310, 432–436.
Conley, D., Strully, K. W., & Bennett, N. G. (2006). Twin differences in birth weight: The effects of genotype and prenatal environment on neonatal and post-neonatal mortality. Economics and Human Biology, 4, 151–183.
Cutler, D., & Lleras-Muney, A. (2010). Understanding differences in health behaviors by education. Journal of Health Economics, 29(1), 1–28.
Danaei, G., Ding, E. L., Mozaffarian, D., Taylor, B., Rehm, J., Murray, C. J., et al. (2009). The preventable causes of death in the United States: Comparative risk assessment of dietary, lifestyle, and metabolic risk factors. PLoS Med, 6(4), e1000058.
Dougherty, C. (2005). Why are returns to schooling higher for women than for men? Journal of Human Resources, 40, 969–988.
Doyle, O., Harmon, C. P., Heckman, J. J., & Tremblay, R. E. (2009). Investing in early human development: Timing and economic efficiency. Economics and Human Biology, 7, 1–6.
Duffy, D. L. (1993). Twin studies in medical research. Lancet, 341, 1418–1419.
Fletcher, J. M. (2012). The effects of teenage childbearing on the short- and long-term health behaviors of mothers. Journal of Population Economics, 25(1), 201–218.
Geronimus, A., & Korenman, S. (1992). The socioeconomic consequences of teen childbearing reconsidered. The Quarterly Journal of Economics, 107(4), 1187–1214.
Griliches, Z. (1979). Sibling models and data in economics: Beginnings of a survey. Journal of Political Economy, 87(5), 37–64.
Grossman, M. (2003). Household production and health. Review of Economics of the Household, 1(4), 331–342.
Grossman, M. (2006). Education and nonmarket outcomes. In Handbook of economics of education, volume 1 of handbook of economics of education (pp. 578–628). Amsterdam: Elsevier.
Gupta, D. N., Deding, M., & Lausten, M. (2013). The effect of low birth weight on height, weight and behavioral outcomes in the medium-run. Economics and Human Biology, 11, 42–55.
Hamilton, B., Martin, J., Osterman, M., Curtin, S. C. (2015). Births: Final data for 2013. Hyattsville, MD. Technical report, National Center for Health Statistics.
Herrarte, A., Moral-Carcedo, J., & Saez, F. (2012). The impact of childbirth on Spanish women’s decisions to leave the labor market. Review of Economics of the Household, 10(3), 441–468.
Hobcraft, J., & Kiernan, K. (2001). Childhood poverty, early motherhood and adult social exclusion. British Journal of Sociology, 52(3), 495–517.
Holmlund, H. (2005). Estimating long-term consequences of teenage childbearing an examination of the siblings approach. Journal of Human Resources, 40(3), 716–743.
Hotz, V., McElroy, S., & Sanders, S. (2005). Teenage childbearing and its life cycle consequences exploiting a natural experiment. Journal of Human Resources, 40(3), 683–715.
Idler, E., & Benyamini, Y. (1997). Self-rated health andmortality: A review of twenty-seven community studies. Journal of Health and Social Behavior, 38, 21–37.
Katz, L. F., & Murphy, K. M. (1992). Changes in relative wages, 1963–87: Supply and demand factors. Quarterly Journal of Economics, 107(February), 35–78.
Kearney, M. S., & Levine, P. B. (2012). Why is the teen birth rate in the United States so high and why does it matter? Journal of Economic Perspectives, 26(2), 141–63.
Klepinger, D., Lundberg, S., & Plotnick, R. (1999). How does adolescent fertility affect the human capital and wages of young women? Journal of Human Resources, 34(3), 421–448.
Kling, J. R., Liebman, J. B., & Katz, L. F. (2007). Experimental analysis of neighborhood effects. Econometrica, 75(1), 83–119.
Liao, T. (2003). Mental health, teenage motherhood, and age at first birth among British women in the 1990s. ISER Working Paper Series 2003–33. Institute for Social and Economic Research.
Lundborg, P. (2013). The health returns to schooling—What can we learn from twins? Journal of Population Economics, 26(2), 673–701.
Mendolia, S. (2014). The impact of husband’s job loss on partners’ mental health. Review of Economics of the Household, 12(2), 277–294.
Mirowsky, J., & Ross, C. E. (2002). Depression, parenthood, and age at first birth. Social Science and Medicine, 54(8), 1281–1298.
Mullahy, J., & Robert, S. A. (2010). No time to lose: Time constraints and physical activity in the production of health. Review of Economics of the Household, 8(4), 409–432.
Patel, P. H., & Sen, B. (2012). Teen motherhood and long-term health consequences. Maternal Child Health Journal, 16(5), 1063–1071.
Ribar, D. (1994). Teenage fertility and high school completion. Review of Economics and Statistics, 76(3), 413–424.
Ribar, D. (1999). The socioeconomic consequences of young women’s childbearing: Reconciling disparate evidence. Journal of Population Economics, 12(4), 547–564.
Rosenzweig, M., & Wolpin, K. (1988). Heterogeneity, intrafamily distribution, and child health. Journal of Human Resources, 23(4), 437–461.
Stenberg, A. (2013). Interpreting estimates of heritability-a note on the twin decomposition. Economics and Human Biology, 11, 201–205.
Webbink, D., Martin, N., & Visscher, P. (2008). Does teenage childbearing increase smoking, drinking and body size? Journal of Health Economics, 27(4), 888–903.
Webbink, D., Martin, N., & Visscher, P. (2011). Does teenage childbearing reduce investment in human capital? Journal of Population Economics, 24, 701–730.
WHO. (2009). Global health risks: Mortality and burden of disease attributable to selected major risks. Geneva: World Health Organization Press.
Acknowledgments
The author would like to thank Melissa S. Kearney, Laura M. Argys, Jere Behrman, Kenneth L. Leonard, Vikesh Amin, Dana C. Andersen, and participants at the 2014 PAA conference for many valuable comments. This paper has been significantly improved from the insightful comments of two anonymous referees.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Güneş, P.M. The effects of teenage childbearing on long-term health in the US: a twin-fixed-effects approach. Rev Econ Household 14, 891–920 (2016). https://doi.org/10.1007/s11150-016-9326-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11150-016-9326-0