
Abstract
Purpose
This study examines the EQ-5D-5L pain/discomfort dimension by drawing comparisons with five other pain and discomfort items (pain severity, discomfort severity, pain frequency, discomfort frequency and pain interference) collected in the Australian psychometric study for the EQ Health and Wellbeing instrument.
Methods
Participants, recruited via a market research company, completed an online survey. Methods of analyses included the assessment of descriptive statistics, variation in reporting patterns using chi-square tests and cross-tabulations, correlation analyses, ordered univariate logistic regression, and discriminatory power analyses (Shannon index (H′) and Shannon Evenness index (J′)).
Results
Survey data from 514 participants were used. Compared with EQ-5D-5L pain/discomfort, there was a higher proportion of respondents reporting some level of impairment on at least one of the pain severity and discomfort severity items (74% versus 81%). Correlation with EQ-5D-5L pain/discomfort was strongest for pain severity (r = 0.83) and weakest for discomfort frequency (r = 0.41); the same inferences were drawn for predictive ability. Adding any additional pain or discomfort items to the EQ-5D-5L increased the absolute informativity (H′) but not the relative informativity (J′). When replacing EQ-5D-5L pain/discomfort with separate pain and/or discomfort items – i.e., adding items to a modified ‘EQ-4D-5L’—absolute informativity increased, while relative informativity increased only when pain interference and frequency-related items (independently or in combination) were added.
Conclusion
The EQ-5D-5L pain/discomfort dimension captures aspects of pain more than aspects of discomfort. Potential reasons include the absence of descriptors or because pain is mentioned first in the composite item.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
Pain is a complex and subjective experience that is influenced by biological, psychological, and social factors [1]. Given its subjective nature, the measurement of pain poses a number of challenges, with no two individuals’ experiences being the same. Although pain most often has a physical cause, it is considered a psychological state and may be reported in the absence of tissue damage or any likely pathophysiological cause [2]. To capture the subjective experiences of pain, patient-reported outcome measures (PROMs) have been developed that typically measure several dimensions of pain, including intensity, frequency, interference with functioning, and effects on general quality of life [3]. Pain is also an ever-present domain in preference-based measures (PBMs) of health-related quality of life (HRQoL), which are often used in economic evaluation to guide resource allocation decisions in healthcare.
EQ-5D instruments are the most widely used and recommended PBMs by national health technology assessment agencies [4]. The three-level (EQ-5D-3L) and five-level (EQ-5D-5L) versions of the EQ-5D comprise five single-item dimensions: mobility, self-care, usual activities, pain/discomfort and anxiety/depression [5, 6]. The composite pain/discomfort dimension has three response choices (no, moderate, extreme) in the EQ-5D-3L and five response choices (no, slight, moderate, severe, and extreme) in the EQ-5D-5L. Early in the initial development of an EQ-5D instrument, items for pain and discomfort were merged to reduce the number of health states to be valued, although the developers acknowledged this may create ambiguity for respondents [7]. Three previous studies have explored the effects of splitting composite EQ-5D-5L dimensions (pain/discomfort and anxiety/depression) with respect to self-reported health [8,9,10], with two studies showing that the pain/discomfort dimension was mainly used by respondents to report pain.
Qualitative studies have shown that respondents consider pain and discomfort to be separate constructs and combining them into a single question has implications for how participants respond. For example, there is evidence that individuals who have experienced discomfort in relation to asthma rate their level of ‘pain or discomfort’ as low because they did not have pain [11]. Another study found that having discomfort was an inevitable consequence of pain but not the other way around, with participants reporting levels of discomfort (e.g., a sore waist or bloating) that did not necessarily cause pain [12]. Moreover, among people living in rural areas of China, pain has been shown to be associated with physical feeling, whereas the Chinese wording for discomfort includes emotions, such as being unhappy [12]. These findings reflect concerns raised by members of the EuroQol Group during the development phase of the EQ-5D, particularly in terms of whether discomfort only relates to physical disturbances [13]. While members of the EuroQol Group associated discomfort primarily with itching, aches, nausea, tiredness, dizziness, bloating, pins and needles and ringing in ears [13], such descriptors are not explicitly mentioned in existing versions of EQ-5D instruments.
Recently, a new quality of life measure has been developed for use in economic evaluation, the EQ Health and Wellbeing (EQ-HWB) instrument [14]. During the development of the EQ-HWB, six countries (Argentina, Australia, China, Germany, UK, and USA) were involved in the face validity and psychometric testing stages of the project [15, 16]. This work resulted in two experimental versions of the EQ-HWB: a 25-item long version and a 9-item short version. The short version is the classification system used for valuation. The long version contains pain severity and discomfort severity items, each with five levels of response (no, mild, moderate, severe, very severe), and pain frequency and discomfort frequency items, also with five levels of response (none of the time, only occasionally, sometimes, often, most or all of the time). The short version measures pain severity only. Compared with the EQ-5D-5L and EQ-5D-3L, other distinguishing features of the EQ-HWB include the explicit reference to physical pain and discomfort, and the use of contextual examples for physical discomfort (e.g., “e.g., feeling sick, breathless, itching (but not including pain)”).
It remains unclear what is captured by the single-item pain/discomfort dimension of the EQ-5D-5L and how it compares with other items that measure the frequency and severity of pain and discomfort. The collection of EQ-5D-5L data alongside other pain and discomfort items in the development phases of the EQ-HWB provides an opportunity to further explore the relationship between pain and discomfort. The aim of this study was to provide a detailed examination of the pain/discomfort dimension of the EQ-5D-5L (hereafter EQ-5D-5L P/D) by drawing comparisons with other pain and discomfort items. More specifically, our research questions were:
-
1.
Are there systematic differences in self-reported responses to the EQ-5D-5L P/D and other pain and discomfort items?
-
2.
To what extent is the information measured by other pain and discomfort items captured by the EQ-5D-5L P/D dimension?
-
3.
What is the discriminatory power of the EQ-5D-5L and a modified ‘EQ-4D-5L’ (where EQ-5D-5L P/D has been removed) with and without the addition of other pain and discomfort items?
Methods
Data source
Data from the EQ-HWB psychometric study in Australia were used [16]. Recruitment for the online survey was facilitated by a market research company (Accent). The recruitment strategy targeted individuals aged 18 years or over, for one of the following groups: people experiencing pain (including conditions such as back pain, arthritis, etc.); people experiencing a mental health problem; people using health care aids (e.g., wheelchair, cane, hearing aids); carers; and a ‘healthy’ sample (based on having an EQ VAS score greater than 80 and reporting no existing health conditions). The aim was to recruit at least 100 participants in each of these groups [16]. Survey completion provided implied consent, and participants were reimbursed based on their respective panel agreements. Median completion time of the survey was 17 min. Ethical approval for the study was granted by the University of Technology Sydney Human Research Ethics Committee (ref. ETH18-2507).
Survey data
The survey included demographic questions, 62 core items to be assessed for inclusion in the EQ-HWB, the EQ-5D-5L, the short Warwick-Edinburgh mental wellbeing Scale (SWEMWBS) [17], the adult social care outcomes toolkit (ASCOT) SCT4 [18], the assessment of quality of life 8-dimension questionnaire (AQoL-8D) [19], and additional items from the Australian arm of the EQ-HWB psychometric study that performed well in the Australian face validity study but were excluded by other international teams. Three versions of the online survey were created with block randomisation of the core items. While the EQ-5D-5L appeared in-between the core items, all other instruments and additional items appeared at the end. The six items related to pain and discomfort that were explored in this study are presented in Table 1. Since some EQ-HWB items underwent minor wording modifications prior to finalising the instrument (e.g., the response option ‘some of the time’ was changed to ‘sometimes’), we refer to pain and discomfort items collected as part of the EQ-HWB psychometric study rather than ‘EQ-HWB items’ throughout the manuscript.
Data analyses
Descriptive statistics were used to describe sample characteristics. The distributions of responses across the pain and discomfort items were tabulated and displayed using a stacked bar chart. Cross-tabulations was used to display the distributions of responses by EQ-5D-5L P/D levels. We hypothesised that the proportion of respondents reporting some level of impairment (levels 2–5) on EQ-5D-5L P/D will be lower than the proportion of respondents reporting impairment on at least one of the pain severity and discomfort severity items (chi-square test). This hypothesis was based on work that showed respondents under-report problems on the composite EQ-5D-5L P/D item [9].
The strength of relationships between the pain and discomfort items and all five dimensions of the EQ-5D-5L were assessed using Spearman’s rank correlation, with correlations interpreted as weak (> 0.0–0.4), moderate (> 0.4–0.7), or strong (> 0.7) [20]. For EQ-5D-5L P/D, correlations were expected to be stronger with the severity-related items compared with those for the frequency-related items and pain interference. We also expected the strongest correlations between pain interference and the EQ-5D-5L dimensions to be with usual activities and self-care, given that this item does not assess pain per se but interference with general function more broadly.
The extent to which the pain and discomfort items were captured by EQ-5D-5L P/D were further investigated using univariate ordered logistic regression analyses, where the EQ-5D-5L P/D was included as the dependent variable. Model fit was examined using pseudo R-squared and the Likelihood Ratio (LR) Chi-Square test (H0 = all regression coefficients in the model are equal to zero). The coefficients produced are the ordered log-odds (logit) regression coefficients. Standard interpretation of the ordered logit coefficient is that for a one unit increase in the independent variable, the dependent variable level (EQ-5D-5L P/D) is expected to change by its respective regression coefficient in the ordered log-odds scale.
To determine the discriminatory power of the EQ-5D-5L with and without the addition of other pain and discomfort items, the Shannon index (H′) and the Shannon Evenness index (J′) were used. Shannon’s H′ (absolute informativity) is an expression of informational richness and reflects both informativity and evenness of the distribution of responses across all possible health states. Shannon’s J′ (relative informativity) adjusts for the theoretically possible number of health states of the descriptive system, capturing the evenness of a distribution only [21]. Both H′ and J′ need to be considered when interpreting informativity. The Shannon indices were calculated for each pain or discomfort item, separately, as well as for the EQ-5D-5L profiles with and without another pain and discomfort item. Based on the findings by Spronk and colleagues [22], we hypothesised that the addition of a pain or discomfort item (any of the five items) to the EQ-5D-5L would improve absolute informativity but not relative informativity. To assess whether any of the pain or discomfort items capture more informativity than the EQ-5D-5L P/D, we also calculated Shannon indices when replacing the EQ-5D-5L P/D item with a pain or discomfort item (i.e., adding items to a modified ‘EQ-4D-5L’), both frequency items, or both severity items.
Result
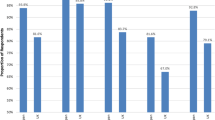
Five hundred forty-one participants were recruited and included in the analyses. Table 2 describes participant characteristics, as well as mean scores for the standardized instruments included in the survey. Figure 1 indicates a similar distribution of responses for EQ-5D-5L P/D, pain severity, and pain interference, although more respondents provided the lowest level of response (level 5, “most or all of the time”) for the pain interference item. Compared with the items measuring pain, a greater proportion of respondents reported level 1 (no problems/none of the time) on the discomfort items. Differences were also observed between the items referring to severity compared with those referring to frequency, where a higher proportion of respondents reported the lowest level (level 5) on the respective frequency item.

Distribution of responses across the six pain and discomfort items. Note: EQ-5D-5L P/D: Level 1 = no problems, Level 2 = slight problems, Level 3 = moderate problems, Level 4 = severe problems, Level 5 = extreme problems. Pain severity and discomfort severity: Level 1 = no, Level 2 = mild, Level 3 = moderate, Level 4 = severe, Level 5 = very severe. Pain frequency and discomfort frequency: Level 1 = none of the time, Level 2 = only occasionally, Level 3 = sometimes, Level 4 = often, Level 5 = most or all of the time
Table 3 shows the distribution of responses of the pain and discomfort items, by EQ-5D-5L P/D level. Among the 133 respondents who reported ‘no problems’ on EQ-5D-5L P/D, 76% and 72% reported no problems on ‘pain severity’ and ‘discomfort severity’, respectively; these proportions fell to 49% and 61% for the two frequency items (‘pain frequency’ and ‘discomfort frequency’, respectively). Similar observations (i.e., higher proportions in the severity items compared with the frequency items) are evident across all matched levels with EQ-5D-5L P/D (i.e., level 1 with level 1, level 2 with level 2, etc.) for levels 1 to 4. Caution is needed when interpreting patterns of responses for those reporting ‘extreme problems’ on EQ-5D-5L P/D due to the small sample size. The hypothesis that the proportion of respondents reporting some impairment on EQ-5D-5L P/D (74%) would be lower than the proportion of respondents reporting impairment on at least one of the pain severity and discomfort severity items was confirmed. The proportions of respondents reporting impairment on the pain severity and discomfort severity items were 78% and 66%, respectively; the proportion reporting impairment on at least one of these items was 81% (74% compared with 81%; χ2 (1028) = 6.44, p = 0.011).
Spearman correlations between the six pain and discomfort items and all EQ-5D-5L dimensions are presented in Table 4. Moderate to strong correlations were observed between EQ-5D-5L P/D and all pain and discomfort items. The hypothesis that stronger correlations would be observed between EQ-5D-5L P/D and the severity-related items (pain severity and discomfort severity) compared with frequency-related items (pain frequency and discomfort frequency) was not confirmed. Instead, correlations were stronger for the pain-related items compared with discomfort-related items. For discomfort frequency, the strongest correlations were with EQ-5D-5L anxiety/depression (r = 0.52) and EQ-5D-5L usual activities (r = 0.42). Our hypothesis for the pain interference item was not confirmed—the strongest correlations between pain interference and the EQ-5D-5L dimensions was for pain/discomfort (r = 0.73), usual activities (r = 0.60) and self-care (r = 0.46).
Table 5 shows the results from the univariate ordered logistic regression analyses. When regressing each item separately on EQ-5D-5L P/D, the pain severity item resulted in the best model fit. The coefficients in Table 5 are the ordered log-odds (logit) regression coefficients. For example, for ‘mild pain’ of the pain severity item, the ordered logit for being in a higher, more severe EQ-5D-5L P/D category is 3.47 higher than for ‘no pain’ (the reference category). The coefficients were higher for items related to pain compared with those related to discomfort or interference, meaning that pain severity had the strongest predictive ability of the EQ-5D-5L P/D.
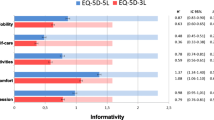
Table 6 presents the Shannon index (H′) and the Shannon Evenness index (J′) for all six pain and discomfort items. The highest absolute informativity and relative informativity was observed for pain frequency. This suggests that all five response levels of the pain frequency are almost equally used, and the item is most efficiently used in terms of informational richness compared to the other items, i.e., the level descriptors discriminate almost optimally between each other in this particular sample. The lowest discriminatory ability, meaning that less information is captured by the item, was observed for discomfort severity. Adding an additional pain or discomfort item to the EQ-5D-5L increased the absolute informativity but not the relative informativity, which confirms our hypothesis. This suggests that although adding another item increases the ability of the EQ-5D-5L to discriminate across individuals (as indicated by an increase in the Shannon Index H′), the addition of the extra item does not increase overall evenness (indicated by a decrease in the Shannon Evenness Index J′). Table 6 also shows the results when adding additional pain and discomfort items to a modified ‘EQ-4D-5L’. Replacing EQ-5D-5L P/D for pain frequency, discomfort frequency, or pain interference led to an improvement in both Shannon indices; only the Shannon H’ index was improved for pain severity and discomfort severity. When replacing EQ-5D-5L P/D with both severity items (pain severity and discomfort severity) or both frequency items (pain frequency and discomfort frequency), an improvement was observed in both Shannon indices for the frequency items only.
Discussion
Our findings show that there are systematic differences in self-reported responses to different types of pain and discomfort items, driven by the construct being measured (i.e., pain versus discomfort) as well as the framing of the response scale (i.e., severity versus frequency). Compared with the proportion of participants reporting problems (defined as ‘any impairment’) on at least one of the pain severity and discomfort severity items (81%), we found that significantly fewer participants reported problems on EQ-5D-5L P/D (74%). Findings also suggest that EQ-5D-5L P/D captures aspects of pain more than aspects of discomfort. Adding an additional pain or discomfort item to the EQ-5D-5L improved the absolute informativity of the EQ-5D-5L (i.e., more information was captured) but not the relative informativity (i.e., when correcting for the theoretically possible number of health profiles, the larger classification system was less efficient). Only when replacing EQ-5D-5L P/D for pain interference and frequency-related items (independently or in combination), both absolute and relative informativity increased.
The reporting of fewer problems on the composite EQ-5D-5L P/D compared with separate domains that measure pain and discomfort has been reported in three previous studies [8,9,10]. Our findings also align with results from a previous study that showed the composite EQ-5D-5L P/D is used mainly to report pain rather than discomfort [8]. A potential explanation for this observation could be the absence of contextual examples for discomfort, which, in contrast, are included in the EQ-HWB discomfort items. Current EQ-5D measures only have such descriptors for the usual activities dimension, referring to, “e.g., work, study, housework, family or leisure activities”. A recent study demonstrated the EQ-5D-5L usual activities dimension reflects the specific activities described to respondents, suggesting that respondents take the examples mentioned in the item description into account [23]. No descriptors are currently provided for pain or discomfort in EQ-5D instruments, where the understanding of the terms is subject to respondents’ own interpretations. Without explicit descriptors, respondents may interpret discomfort as a mild form of pain, as was shown in a study where 4% of respondents equated discomfort with ‘mild pain’ [9]. Although others have found ‘itching’ to be captured by the EQ-5D-5L [24], our findings indicate that respondents do not seem to associate aspects of discomfort that are included in the EQ-HWB discomfort items (such as feeling like throwing up, feeling breathless, itching or other physical discomfort) when responding to the EQ-5D-5L P/D. Our findings confirm previous studies where EQ-5D measures have been found to be unable to capture nausea in patients with acute leukemia [25] and respiratory symptoms (breathing problems) in patients with asthma and chronic obstructive pulmonary disease [26]. In fact, findings from a mixed-methods study showed that discomfort is an umbrella term for about a hundred different physical sensations, mental problems or feelings [9]. This broad interpretation of discomfort raises challenges for the identification of potential descriptors for the EQ-5D-5L P/D, should this be a line of research that is pursued.
The word ‘or’ in the EQ-5D-5L P/D response levels could be another reason for under-reporting problems on the composite dimension. Although at face value, EQ-5D-5L P/D refers to pain or discomfort, respondents may feel that the item only asks either for pain or discomfort, but not both. Further research would be necessary to gain insight into this specific unknown. Additionally, the fact that pain is mentioned first in the composite item could also influence respondents to focus more on pain than discomfort.
Compared with EQ-5D-5L P/D, a further distinguishing feature of the pain or discomfort items included in this study relates to the explicit reference to physical pain or discomfort. This clarification was added in view of the face validity findings in the development of the EQ-HWB, where respondents queried whether pain and discomfort would also encompass distress and psychological pain or discomfort, including the feeling of embarrassment [15]. Following our observation that EQ-5D-5L P/D seems to measure pain more than discomfort, when comparing it to the pain severity item, which refers to physical pain, we observed a strong correlation, suggesting respondents associate EQ-5D-5L P/D more with physical pain. This observation also confirms findings from qualitative work, where respondents interpreted pain in terms of a physical feeling [12]. However, to avoid (or, more likely, reduce) ambiguity, there is scope for further research exploring contextual examples not only for discomfort but also for pain, such as ‘headache’ or ‘bodily pain’. We also found a moderate correlation between the discomfort items and EQ-5D-5L anxiety/depression. This may imply that the discomfort items capture mental/emotional discomfort in addition to physical discomfort, confirming findings where a large number of respondents gave psychological examples for discomfort [9].
Despite EQ-5D-5L P/D seeming to measure pain more than discomfort, adding another discomfort item to the EQ-5D-5L did not improve discriminatory power (Table 6). This is in line with findings by Spronk and colleagues, who showed that adding a pain or itching dimension to the EQ-5D-5L improved the informativity of the EQ-5D-5L but the gain in discriminatory power was negligible [22]. Only when replacing EQ-5D-5L P/D with the pain frequency item, and the two frequency items in combination, the discriminatory power increased (relative to EQ-5D-5L only). Given that the same was not observed when replacing EQ-5D-5L P/D with the severity-related items suggests that additional information is captured likely by the response scale referring to frequency rather than severity.
It has been argued that ‘frequency of pain’ should be considered in relation to severity, as mild pain that is chronic in nature may have an effect equivalent to that of acute pain that lasts only for a few days [27]. Especially in individuals experiencing fluctuations in pain or discomfort, frequency scales may provide additional information. Previous research has found that fluctuations of pain symptoms were associated with psychosocial factors, such as depression, anxiety and coping skills [28]. Therefore, the measurement of pain frequency may have provided additional information in terms of individuals’ sense of predictability and control over their pain symptoms as well as their coping skills (i.e., how well they are adjusting to pain) when appending the EQ-5D-5L with a frequency item. In this context, the role of the recall period needs to be considered, as frequency scales are only appropriate when respondents are prompted to recall their level of pain over a specified period a time. While the EQ-HWB pain or discomfort items refer to ‘the last 7 days’, the EQ-5D-5L refers to ‘your health TODAY’. A previous study found that the EQ-5D-5L’s reference point (‘today’) may underestimate the impact of persistent pain compared with a modified version referring to ‘the last month’ [29]. Whether differences between EQ-5D-5L P/D and the frequency items relate more to differences in the response scale (severity versus frequency) or to differences in the recall period is unclear.
In addition to queries about how individuals self-report their own health on the EQ-5D-5L P/D item, the fact that the EQ-5D-5L is accompanied by a value set raises questions as to what extent self-reported health corresponds with the interpretation of the composite EQ-5D-5L P/D dimension in health state valuation studies. Previous work looking at health state valuations has shown that EQ-5D-5L P/D was interpreted to mean pain, where the utility decrements for an altered ‘discomfort only’ subdimension were significantly smaller than for the composite EQ-5D-5L P/D at all levels [8]. Others have observed such a finding for level 5 only, suggesting that what respondents had in mind when valuing ‘extreme pain or discomfort’ was significantly worse than extreme discomfort on its own [10]. Collectively, these findings suggest that EQ-5D-5L P/D captures aspects of pain more than aspects of discomfort in the context of health state valuation, complementing our findings in the context of self-reported health.
Further research
Avenues for further work include exploring contextual examples for EQ-5D-5L P/D and the impact of such descriptors on health state valuations and self-reported health classifications. Methodological work could also examine the impact of reversing the order of the dimensions (i.e., discomfort preceding pain). The relationship between pain and discomfort items could also be investigated using other approaches, such as item response theory, as previously done for vision-related quality of life dimensions [30]. Repeating the study in a non-English-speaking population (where the wording for pain and discomfort may be interpreted differently [12]) could also provide further insights, although findings from a Hungarian study align with our work [9]. Similar analyses are likewise warranted for the other composite dimension of the EQ-5D-5L—the anxiety/depression dimension. While a previous study indicated that the composite anxiety/depression dimension is used as intended (i.e., to capture anxiety, depression, or both) [8], the same conclusion was not reached by other quantitative and qualitative studies [10, 31].
Strengths and limitations
The strengths of this study include the comparison of EQ-5D-5L P/D to different types of pain and discomfort items that differ in the construct being measured (i.e., pain versus discomfort) as well as the framing of the response scale (i.e., severity versus frequency). While previous studies assessed only the relationship between EQ-5D-5L P/D to pain and discomfort that were split into two subdimensions (i.e., pain and discomfort) [8,9,10], our study provides further insights into the extent to which EQ-5D-5L P/D captures pain interference as well as pain frequency and discomfort frequency, including examples for discomfort. We employed a range of statistical analyses that provided additional evidence as to what the EQ-5D-5L P/D is measuring and examined its discriminatory power with and without the addition of other pain and discomfort items, from which we formulated directions for further research. As with all studies, there are limitations. Our findings are specific to a single English-speaking country (Australia) and use data from a primary study where the sampling strategy purposively sampled people with specific characteristics [16]. Additionally, as this was a secondary analysis, all analyses relied on the pain and discomfort items collected in the EQ-HWB psychometric study. This means that comparisons with other studies that have used separate pain and discomfort items (with different wording) need to be made with caution. As noted earlier, there have also been slight wording modification to the EQ-HWB items since the psychometric study. Another limitation relates to the different recall periods for the EQ-5D-5L (‘TODAY’) and the pain and discomfort items (‘last seven days’); the extent to which this explains the differences in responses is unclear. Finally, the small number of respondents reporting ‘extreme’ pain/discomfort on the EQ-5D-5L limits the applicability of our findings to more severe samples. Although recruitment strategies in the Australian EQ-HWB psychometric study targeted people experiencing pain, the sampling approach was not informed by the study aims described in this paper (a common limitation of secondary analyses).
Conclusion
The pain/discomfort dimension of the EQ-5D-5L appears to capture aspects of pain more than aspects of discomfort. This creates challenges in the interpretation of responses to the composite item. While adding pain or discomfort items to the EQ-5D-5L does not improve discriminatory power, further studies are warranted to explore the addition of descriptors for pain and/or discomfort, presenting the dimensions separately, or the influence of reversing the order in the composite item.
Data availability
Data cannot be shared publicly. However interested researchers are invited to contact the corresponding author to discuss data access options.
References
Trachsel, L. & Cascella, M. (2020). Pain theory. StatPearls Publishing, from https://www.ncbi.nlm.nih.gov/books/NBK545194/
Raja, S. N., Carr, D. B., Cohen, M., Finnerup, N. B., Flor, H., Gibson, S., Keefe, F. J., Mogil, J. S., Ringkamp, M., Sluka, K. A., Song, X. J., Stevens, B., Sullivan, M. D., Tutelman, P. R., Ushida, T., & Vader, K. (2020). The revised international association for the study of pain definition of pain: Concepts, challenges, and compromises. Pain, 161(9), 1976–1982. https://doi.org/10.1097/j.pain.0000000000001939
Younger, J., McCue, R., & Mackey, S. (2009). Pain outcomes: A brief review of instruments and techniques. Current Pain and Headache Reports, 13(1), 39–43. https://doi.org/10.1007/s11916-009-0009-x
Kennedy-Martin, M., Slaap, B., Herdman, M., van Reenen, M., Kennedy-Martin, T., Greiner, W., Busschbach, J., & Boye, K. S. (2020). Which multi-attribute utility instruments are recommended for use in cost-utility analysis? A review of national health technology assessment (HTA) guidelines. The European Journal of Health Economics, 21(8), 1245–1257. https://doi.org/10.1007/s10198-020-01195-8
Szende, A., Oppe, M., & Devlin, N., (2007) EQ-5D Value sets: Inventory, comparative review and user guide. EuroQol Group Monographs, (vol. 2). Springer
Herdman, M., Gudex, C., Lloyd, A., Janssen, M., Kind, P., Parkin, D., Bonsel, G., & Badia, X. (2011). Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Quality of Life Research, 20(10), 1727–1736. https://doi.org/10.1007/s11136-011-9903-x
Gudex, C. (2005). The descriptive system of the EuroQol instrument. In P. Kind, R. Brooks, & R. Rabin (Eds.), EQ-5D concepts and methods: A developmental history (pp. 19–27). Springer.
McDonald, R., Mullett, T. L., & Tsuchiya, A. (2020). Understanding the composite dimensions of the EQ-5D: An experimental approach. Social Science and Medicine, 265, 113323. https://doi.org/10.1016/j.socscimed.2020.113323
Rencz, F., & Janssen, M. F. (2022). Analyzing the pain/discomfort and anxiety/depression composite domains and the meaning of discomfort in the EQ-5D: A mixed-methods study. Value Health. https://doi.org/10.1016/j.jval.2022.06.012
Tsuchiya, A., Bansback, N., Hole, A. R., & Mulhern, B. (2019). Manipulating the 5 dimensions of the EuroQol instrument: The effects on self-reporting actual health and valuing hypothetical health states. Medical Decision Making, 39(4), 379–392. https://doi.org/10.1177/0272989X19851049
Whalley, D., Globe, G., Crawford, R., Doward, L., Tafesse, E., Brazier, J., & Price, D. (2018). Is the EQ-5D fit for purpose in asthma? Acceptability and content validity from the patient perspective. Health and Quality of Life Outcomes, 16(1), 160. https://doi.org/10.1186/s12955-018-0970-3
Yang, F., Jiang, S., He, X. N., Li, H. C., Wu, H. Y., Zhang, T. T., & Wu, J. (2020). Do rural residents in China understand EQ-5D-5L as intended? Evidence from a qualitative study. Pharmacoecon Open, 5(1), 101–109. https://doi.org/10.1007/s41669-020-00212-z
Fox-Rushby, J. (2005). First steps to assessing semantic equivalence of the EuroQol instrument: Results of a questionnaire survey to members of the EuroQol group. In P. Kind, R. Brooks, & R. Rabin (Eds.), EQ-5D concepts and methods: A developmental history (pp. 35–52). Springer.
Brazier, J., Peasgood, T., Mukuria, C., Marten, O., Kreimeier, S., Luo, N., Mulhern, B., Pickard, A. S., Augustovski, F., Greiner, W., Engel, L., Belizan, M., Yang, Z., Monteiro, A., Kuharic, M., Gibbons, L., Ludwig, K., Carlton, J., Connell, J., … Rejon-Parrilla, J. C. (2022). The EQ-HWB: Overview of the development of a measure of health and wellbeing and key results. Value Health, 25(4), 482–491. https://doi.org/10.1016/j.jval.2022.01.009
Carlton, J., Peasgood, T., Mukuria, C., Connell, J., Brazier, J., Ludwig, K., Marten, O., Kreimeier, S., Engel, L., Belizan, M., Yang, Z., Monteiro, A., Kuharic, M., Luo, N., Mulhern, B., Greiner, W., Pickard, S., & Augustovski, F. (2022). Generation, selection, and face validation of items for a new generic measure of quality of life: The EQ-HWB. Value Health, 25(4), 512–524. https://doi.org/10.1016/j.jval.2021.12.007
Peasgood, T., Mukuria, C., Brazier, J., Marten, O., Kreimeier, S., Luo, N., Mulhern, B., Greiner, W., Pickard, A. S., Augustovski, F., Engel, L., Gibbons, L., Yang, Z., Monteiro, A. L., Kuharic, M., Belizan, M., & Bjorner, J. (2022). Developing a new generic health and wellbeing measure: Psychometric survey results for the EQ-HWB. Value Health, 25(4), 525–533. https://doi.org/10.1016/j.jval.2021.11.1361
Stewart-Brown, S., Tennant, A., Tennant, R., Platt, S., Parkinson, J., & Weich, S. (2009). Internal construct validity of the Warwick-Edinburgh mental well-being scale (WEMWBS): A Rasch analysis using data from the Scottish health education population survey. Health and Quality of Life Outcomes, 7, 15. https://doi.org/10.1186/1477-7525-7-15
Netten, A., Burge, P., Malley, J., Potoglou, D., Towers, A. M., Brazier, J., Flynn, T., Forder, J., & Wall, B. (2012). Outcomes of social care for adults: Developing a preference-weighted measure. Health Technology Assessment, 16(16), 1–166. https://doi.org/10.3310/hta16160
Richardson, J., Sinha, K., Iezzi, A., & Khan, M. A. (2014). Modelling utility weights for the assessment of quality of life (AQoL)-8D. Quality of Life Research, 23(8), 2395–2404. https://doi.org/10.1007/s11136-014-0686-8
Akoglu, H. (2018). User’s guide to correlation coefficients. Turk J Emerg Med, 18(3), 91–93. https://doi.org/10.1016/j.tjem.2018.08.001
Janssen, B., Birnie, E., & Bonsel, G. J. (2007). Evaluating the discriminatory power of EQ-5D, HUI2 and HUI3 in a US general population survey using Shannon’s indices. Quality of Life Research, 16(5), 895–904. https://doi.org/10.1007/s11136-006-9160-6
Spronk, I., Bonsel, G. J., Polinder, S., van Baar, M. E., Janssen, M. F., & Haagsma, J. A. (2021). The added value of extending the EQ-5D-5L with an itching item for the assessment of health-related quality of life of burn patients: An explorative study. Burns, 47(4), 873–879. https://doi.org/10.1016/j.burns.2020.08.015
Gamst-Klaussen, T., & Lamu, A. N. (2020). Does the EQ-5D usual activities dimension measure what it intends to measure? The relative importance of work, study, housework, family or leisure activities. Quality of Life Research, 29(9), 2553–2562. https://doi.org/10.1007/s11136-020-02501-w
Spronk, I., Bonsel, G. J., Polinder, S., van Baar, M. E., Janssen, M. F., & Haagsma, J. A. (2020). Exploring the relation between the EQ-5D-5L pain/discomfort and pain and itching in a sample of burn patients. Health and Quality of Life Outcomes, 18(1), 144. https://doi.org/10.1186/s12955-020-01394-0
van Dongen-Leunis, A., Redekop, W. K., & Uyl-de Groot, C. A. (2016). Which questionnaire should be used to measure quality-of-life utilities in patients with acute leukemia? An evaluation of the validity and interpretability of the EQ-5D-5L and preference-based questionnaires derived from the EORTC QLQ-C30. Value Health, 19(6), 834–843. https://doi.org/10.1016/j.jval.2016.05.008
Hoogendoorn, M., Oppe, M., Boland, M. R. S., Goossens, L. M. A., Stolk, E. A., & Rutten-van Molken, M. (2019). Exploring the impact of adding a respiratory dimension to the EQ-5D-5L. Medical Decision Making, 39(4), 393–404. https://doi.org/10.1177/0272989X19847983
Bhardwaj, P., & Yadav, R. (2015). Measuring pain in clinical trials: Pain scales, endpoints, and challenges. Int J Clin Exp Physiol, 2(3), 151–156. https://doi.org/10.4103/2348-8093.169965
Schneider, S., Junghaenel, D. U., Keefe, F. J., Schwartz, J. E., Stone, A. A., & Broderick, J. E. (2012). Individual differences in the day-to-day variability of pain, fatigue, and well-being in patients with rheumatic disease: Associations with psychological variables. Pain, 153(4), 813–822. https://doi.org/10.1016/j.pain.2012.01.001
Durham, J., Steele, J. G., Breckons, M., Story, W., & Vale, L. (2015). DEEP study: Does EQ-5D-5L measure the impacts of persistent oro-facial pain? Journal of Oral Rehabilitation, 42(9), 643–650. https://doi.org/10.1111/joor.12296
Khadka, J., Gothwal, V. K., McAlinden, C., Lamoureux, E. L., & Pesudovs, K. (2012). The importance of rating scales in measuring patient-reported outcomes. Health and Quality of Life Outcomes, 10, 80. https://doi.org/10.1186/1477-7525-10-80
Bryan, S., Jowett, S., Hardyman, W., and Bentham, P., 2004 Does the EQ-5D ‘"nxiety/depression" item measure anxiety, depression, both or neither?. In 21st Scientific Plenary Meeting of the EuroQol Group. Chicago, US
Acknowledgements
We thank Professor Aki Tsuchiya for her discussion of an earlier draft of our paper at the 37th virtual EuroQol Plenary in 2020.
Funding
This study was funded by the EuroQol Research Foundation. Views expressed in this paper are not necessarily those of the EuroQol Research Foundation.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation and data collection were performed by LE and BM. Data analysis was performed by LE. The first draft of the manuscript was written by LE and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
All authors are members of the EuroQol Group Association.
Ethical approval
Ethical approval for the study was granted by the University of Technology Sydney Human Research Ethics Committee (ref. ETH18-2507). All participants provided implied consent by completing the online survey.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Engel, L., Whitehurst, D.G.T., Haagsma, J. et al. What is measured by the composite, single-item pain/discomfort dimension of the EQ-5D-5L? An exploratory analysis. Qual Life Res 32, 1175–1186 (2023). https://doi.org/10.1007/s11136-022-03312-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-022-03312-x