
Abstract
Background
Family Quality of Life (FQOL) is an important outcome for families of children with disabilities and is influenced by context and culture. Minimal research explores FQOL in African contexts.
Purpose
This scoping review identifies factors contributing to FQOL for families of children with disabilities in African contexts.
Method
We were guided by Arksey and O’Malley’s scoping review framework, searching for research papers from the following electronic databases: CINAHL, Embase, Medline, Global Health, and PsycINFO. Using pre-determined eligibility criteria, two authors independently reviewed articles for inclusion via Covidence, a reference manager that facilitates blind reviewing. Two other authors independently extracted data from studies using a data-charting form based on Zuna and colleagues’ FQOL framework. Reviewers met regularly for discussion to reach consensus.
Results
Fifty-three articles met the inclusion criteria, and findings demonstrated a broad variety of factors contributing to FQOL within the FQOL framework related to family unit factors, individual member factors, and external support factors. We found that poverty, stigma, and spirituality were particularly prominent factors affecting FQOL negatively and positively in African contexts.
Conclusion
Whilst there are universal factors that contribute to FQOL, recognising the influence of context-specific factors (i.e. poverty, stigma, spirituality) is important in order to provide effective, culturally relevant support that enhances FQOL for families of children with disabilities in African contexts.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Plain english summary
Family quality of life describes the ‘goodness’ of family life and considers the wellbeing of each individual family member and the family as a whole. Families of children with disabilities have some unique challenges, and it is important to understand what they need for a good family quality of life. Most of the research about family quality of life focuses on families in high-income, Western countries, and we need more research from low-income contexts, particularly African countries, to understand different perspectives. In this review, we looked at research from African countries about families of children with disabilities to find out what factors affect families’ quality of life. We found that there were things about individual family members (e.g. parents’ employment or children’s behaviour) as well as things about the whole family (e.g. family’s income or beliefs) that affected the family’s quality of life. Support from extended family, friends, health services, and government aid also helped families to have a better quality of life. We found that many African families of children with disabilities experienced poverty and discrimination which lowers their quality of life; however, they also relied on their strong spiritual beliefs to help them cope. Knowing what makes families’ lives more difficult and what makes their lives better can help to direct services that support families of children with disabilities in African countries and improve their quality of life.
Introduction
Family Quality of Life (FQOL) emerged from scholarship on individual Quality of Life (QOL) for people with disabilities and has developed into its own research field [1,2,3,4]. The definition of ‘family’ is dynamic and can vary depending on the setting and cultural values, but it is recognised as more than just blood relations and refers to a collective of individuals who identify or are recognised within the local community as family and who regularly interact and support one another [5,6,7,8]. In African contexts specifically, family is defined broadly and extended family members or even close friends are often strongly connected, responsible for, and considered integral to the family unit [9,10,11,12]. FQOL can be described as the “goodness of family life” [13] (p.29) and is an outcome of the complex interactions between family needs, strengths, characteristics as well as support and other contextual factors [4]. Zuna and colleagues [5] define FQOL as “a dynamic sense of well-being of the family, collectively and subjectively defined and informed by its members, in which individual and family-level needs interact” (p. 262).
Disability affects every family uniquely, but a supportive, loving family benefits a child’s wellbeing as well as the whole family [4, 14, 15]. Many families report high levels of FQOL despite some negative stereotypes of having children with a disability and undeniable challenges [4, 16]. Disability can affect family routines and self-efficacy and may accentuate parental stress, but families often show remarkable coping and resilience [17]. FQOL research originally focused on families of children with intellectual and developmental disabilities (IDD); however, the literature is expanding to explore FQOL with other forms of disability [18, 19]. Further research is needed to understand FQOL of families with various disabilities, family structures, and backgrounds.
There is limited FQOL research in low- and middle-income countries (LMICs) [20], with a noticeable gap in African countries [9, 21, 22]. Existing knowledge about FQOL is predominantly from and pertaining to high-income countries, despite the fact that the estimated prevalence of disability for African children is significantly higher (6.4% compared to 2.8% in high-income countries) [23]. Globally, the majority of children with disabilities (approximately 80%) live in LMICs [24]. Although disability affects families from every cultural background, the effect on FQOL can be more pronounced in African contexts, as disability-related support capacity can often be limited [20, 22]. Therefore, the FQOL literature does not represent a global perspective, and further research is required to better understand the universal, as well as unique, factors that contribute to the wellbeing of families of children with disabilities globally.
Despite the complexity of the FQOL construct and need for further research in African countries, available research findings indicate that support is an important factor contributing to FQOL [25,26,27,28]. Focusing specifically on LMICs, a scoping review of research findings demonstrated that families of children with disabilities rely mostly on informal support from extended family, friends, and the community, and that provision of support is associated with lower parental stress and care burden, increased knowledge/skills and life satisfaction, and greater social participation for children with disabilities [29]. Social support in the form of practical resources (e.g. money, childcare), emotional support or information, was found to be crucial for families of children with disabilities in African contexts with limited government/formal support and where extended families and communities comprise the central support networks [30, 31]. However, provision of informal social support can also be driven by obligation, reciprocity, and complex social expectations [12, 32]. Although there are gaps between the ideals and the lived reality, the sub-Saharan African philosophy of Ubuntu epitomises the crucial role of strong social connectedness and interdependence and is an important foundation to draw on for promoting dignity, reciprocity, and solidarity towards families of children with disabilities in various African communities [33, 34].
The purpose of this review is to systematically explore published literature to identify and discuss factors that contribute to FQOL for families of children with disabilities (hereafter referred to as ‘children’) in African contexts. Although Africa is a large and diverse continent, identifying common themes as well as unique differences between and within African countries can deepen our understanding of the needs of families and identify potential opportunities to provide support and enhance FQOL. Understanding contributing factors to FQOL for African families can help to inform culturally relevant service provision, addressing barriers that impede FQOL and supporting facilitators that enhance FQOL.
Method
We followed Arksey and O’Malley’s [35] methodological framework along with the PRISMA framework for scoping reviews [36]. First, we identified the research question: What factors contribute to FQOL for families of children with disabilities in African contexts? Based on Zuna and colleagues’ [5] FQOL framework, we focused on individual member, family unit, and support factors. We defined individual member factors as concepts about individual family members (e.g. demographics, characteristics, beliefs); family unit factors included concepts relating to the family as a whole, including characteristics (i.e. traits, descriptors) and dynamics (i.e. interactions/relationships, attitudes/values); support factors were defined as “less tangible resources provided to the individual or to the whole family which are expected to improve outcomes for the individual or family”. [5] (p. 265). We categorised support factors according to Kyzar and colleagues’ [25] classifications: emotional, physical, material/instrumental, and informational (see Table 1).
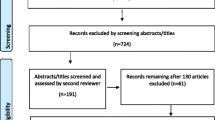
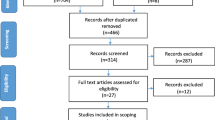
A health sciences librarian helped to structure the search strategy. Three authors discussed and confirmed inclusion/exclusion criteria iteratively (JVV, RPN, AN) (Table 2). We included full-text, original, peer-reviewed research in English that was conducted in African countries. Because minimal research has focused exclusively on FQOL in African contexts, our search strategy included related terms, such as QOL, wellbeing, family function, life satisfaction, coping, and resilience, based on definitions of FQOL and by exploring the indexing of key relevant articles and the scope of keywords in the databases. Hence, included articles did not always explicitly use the term ‘FQOL’, but all described some related family-reported outcome and various components of the FQOL framework from the perspective of family members of children with disabilities. The search included sources from 2000 onwards, as FQOL research became more established following the 2000 World Congress Conference of the International Association for the Scientific Study of Intellectual and Developmental Disability [1, 14]. We searched the following databases in May 2020: CINAHL, EMBASE, MEDLINE, PsycInfo, and Global Health (see Table 3 for specific search terms and Online Appendix I for sample database search strategy). Using Covidence software, JVV and AN independently screened titles and abstracts before meeting to discuss/resolve discrepancies. Both authors then independently conducted full-text reviews of selected papers before reaching consensus on the final included articles. We also hand-searched reference lists of the included articles, African Journal of Disability and all journals in the African Journals Online database. Figure 1 illustrates the selection process.

PRISMA flow diagram showing article selection process. AJOL African Journals Online, AJOD African Journal of Disability
Two authors (JVV, RPN) independently extracted data from each article to excel spreadsheets using qualitative content analysis where we familiarised ourselves with the articles and systematically searched for descriptions/concepts related to factors contributing to FQOL within the FQOL framework (deductively) and outside of the framework (inductively). The data extraction involved an iterative process where we met multiple times to discuss findings to capture relevant information and ensure consistency. Finally, we collated, summarised, and reported the results by systematically analysing the extracted data and describing the articles’ characteristics, before using qualitative thematic analysis [37] to identify codes and themes describing the factors contributing to FQOL.
Results
Fifty-three articles met the inclusion criteria, with the majority being qualitative studies (27/53) originating from South Africa (19/53), and focused on children with IDD (22/53). All studies included views of at least one parent (mostly mothers), but 24 also reported perspectives of other family members (i.e. grandparents, siblings, aunts), and 34 studies had mainly female participants (Table 4). The term ‘caregiver’ was used if this was the term primarily used by the study authors and referred to someone who had significant responsibility in raising the child with a disability. Studies covered 14 different African countries (South Africa, Kenya, Ghana, Nigeria, Uganda, Tanzania, Malawi, Ethiopia, Zimbabwe, Sudan, Egypt, Congo, Namibia, and Zambia) and included a range of disabilities such as IDD, cerebral palsy, hearing impairments, spina bifida, mental disabilities, and multiple disabilities. Only five studies used an existing FQOL measure: three used the Beach Centre FQOL Scale [38] and two used the FQOL Survey [39].
Individual member factors
Individual demographics
Research indicated that the child’s functional/care needs, comorbidities, and age influenced FQOL [9, 40,41,42,43,44,45,46,47,48,49,50,51,52,53,54]. Higher care needs and more comorbidities negatively affected FQOL. However, the type of disability did not appear to have a significant effect on FQOL. Authors reported mixed findings related to age, where some found improved FQOL with age (i.e. reduced care needs/parental responsibility) [55], whilst others found the opposite (i.e. less services for older children) [47, 56]. One Egyptian study found that having a male child influenced FQOL more negatively than a female child [46], but most studies found no significant correlation between the child’s gender and FQOL.
Several studies demonstrated how parental employment/occupation and education affected FQOL [9, 21, 22, 42, 46, 49, 53, 54, 56,57,58,59,60,61,62,63,64,65]. For example, parents with higher educational levels were more likely to have employment, leading to higher FQOL. Gender was also an associated factor, such that mothers/female caregivers often experienced greater care burden than fathers (with implications on their health) due to cultural expectations of women as primarily responsible for child raising [44, 45, 47, 49, 66,67,68,69,70,71,72,73]. However, other researchers found no significant associations between socio-demographic factors such as parental employment, education, age, gender, and FQOL [52, 59, 66, 74].
Individual characteristics
Individual characteristics relate to “more complex and multidimensional traits which might vary over time” [5] (p. 264). Children’s behaviour and communication impairments were negatively associated with FQOL [40, 44, 48, 56, 60, 67, 75,76,77,78,79,80]. Parents in various studies reported how their physical and psychological health affected FQOL, e.g. some parents (particularly mothers) experienced chronic pain, stress, and depression due to the heavy care burden of having a child with a disability [22, 44, 45, 48, 54, 59, 60, 62, 64, 65, 67, 68, 70,71,72,73, 75, 78, 79, 81,82,83].
Individual beliefs
Beliefs refer to a family member’s understanding, expectations, or meaning making related to their child [5]. Researchers described parents’ mixed emotions and beliefs towards their child [61, 64, 77, 80, 83]. Initially, they may have been devastated, but some caregivers progressed to greater acceptance of disability, recognising their responsibility and committing to protect, provide, and advocate for their child with patience and hope [42, 44, 48, 57, 60, 65, 70, 75, 80, 83,84,85]. Some caregivers saw their child as a ‘gift from God’ [40, 57] and “their child was one of their biggest sources of joy and pride” [70] (p. 110). Participants (particularly mothers) frequently described how their spiritual beliefs helped them cope [22, 44, 48, 62, 71, 80, 84, 86]. Researchers also found that acceptance, forgiveness, optimism, confidence, and proactiveness (i.e. learning new skills) contributed positively to FQOL [22, 40, 49, 51, 55, 56, 69, 71, 76, 80, 84]. Both problem- and emotion-focused strategies helped parents to cope [21, 84]; however, many parents continued to worry about their child’s future [48, 54, 62, 70, 77, 78, 84].
Family Unit factors
Family characteristics
Study findings indicated a connection between socio-economic status and FQOL [9, 10, 21, 40, 42,43,44, 49, 50, 52,53,54, 56, 58, 59, 61, 62, 70, 71, 75, 79]. Poverty was prevalent among families and financial needs had a significantly negative effect on FQOL [10, 22, 48, 63,64,65, 67, 68, 80, 81, 84]. Several studies demonstrated that the region where families lived influenced FQOL [58, 66]; for example, families in northern Uganda had lower FQOL than those in the south due to political instability and higher stigma [43], whilst Nigerian families of children with Down Syndrome in urban areas had higher FQOL than those in rural areas due to better service/resource access [56]. Four studies in this review showed that family composition influenced FQOL where two-parent families and/or married parents correlated with higher FQOL [9, 45, 50, 55]. Two studies indicated that having more children negatively influenced FQOL due to parents’ additional responsibilities [47, 50]. However, two other studies demonstrated that siblings could help family adaptation and positively affected FQOL due to their involvement in education/care of the child with a disability, reducing parental care burden [42, 55]. A number of studies identified family members other than parents as primary caregivers (mostly grandmothers) particularly if the mother had died, or if parents separated or rejected their child for various reasons; however, studies did not differentiate this as an isolated factor affecting FQOL, the relationships between family members were more important [53, 57, 67, 70, 83].
Family dynamics
Family relationships
There was strong evidence that family cohesion/cooperation and commitment positively contributed to FQOL [10, 40,41,42, 56, 57, 77]. Closely knit families with loving social/emotional relationships, mutual respect, and understanding adapted better and had more positive family outcomes [87]. Including children in family activities/chores and working together as a family also benefitted FQOL [57, 67]. Several authors discussed the importance of quality family time and maintaining routines [40,41,42, 56, 75, 87, 88]. However, disruptions to routines [81] and long working hours impeded FQOL [10, 56]. Families’ communication patterns also influenced FQOL where positive, affirming, and open communication led to better adaptation and wellbeing [40,41,42]. Conversely, miscommunication, particularly between parents and their child, hindered care and negatively affected FQOL [40, 77].
Authors described both positive and negative effects of spousal relationships on FQOL [55, 60, 61, 72, 81]. For example, Namibian mothers felt happy and socially integrated when their husbands were loving and accepting [48], and South African mothers reported improved communication and relationships with their spouses because of their child’s disability [44]. However, authors in various African countries, also described unsupportive, absent or abusive spouses, and marital strain (sometimes divorce) that resulted from having a child with a disability [48, 51, 65, 70, 71, 75, 78, 82]. Additionally, acceptance, care, and involvement of siblings with the child with a disability (particularly older siblings) positively influenced FQOL [55, 68, 75, 76].
Family values/attitudes
Across countries, African families’ religious/spiritual beliefs and values also influenced FQOL [10, 40,41,42, 54, 63, 87]. These beliefs helped families to accept and appreciate their child, thus, positively contributing to FQOL [41, 67, 78, 81]. Ajuwon [56] described how Nigerian families recognised that their child “brought a special joy and love to their entire family” (p. 39). Flexibility, willingness to learn and change, innovation, and creativity were also values that improved families’ adaption and FQOL [10, 40,41,42]. FQOL was influenced positively when families proactively taught their child life/social skills [68, 75, 77]. Maintaining traditional cultural values, community/social engagement, and fulfilling social expectations also strengthened family relationships and positively affected FQOL [56, 57]; however, some families withdrew from their communities due to stigmatising attitudes or care burdens [70, 73, 75, 82]. Additionally, many families persistently sought a cure and some maintained both biomedical and traditional views on disability [49, 64, 67, 73, 77, 86].
Support factors
Researchers described how some families received support and the positive contribution of support to FQOL; however, most authors highlighted families’ support needs and overall lack of support.
Instrumental support
Most studies highlighted families’ need for financial support as poverty negatively affected their FQOL. Some families received financial/material support from extended family, NGOs/charities, religious institutions, peer-support groups (through income-generation activities), and only occasionally from government grants, but overwhelmingly, research demonstrated the need for more support [43, 44, 48, 54, 56, 61,62,63,64, 66, 70, 77, 79, 84,85,86]. Researchers identified the importance of promoting school attendance and education, because as well as supporting the child’s development, it allowed parents to maintain employment, thus, reducing financial needs [40, 52, 53, 55, 64, 65, 67, 71, 78, 80, 86]. Several authors discussed the need for more public schooling, scholarships for children with disabilities, and special education [56, 68, 77, 87]. This tied to families’ need for respite/childcare to reduce care burden and allow parents to work [21, 42, 49, 64, 78, 79, 83]. Sometimes extended family, neighbours, or older siblings assisted with childcare, but families needed more support [55, 68, 80]. Families also needed better, affordable transportation to access health services which were often located in urban centres far from their homes [10, 54, 61, 68, 70, 71, 82].
Informational support
Researchers found that families needed more information related to their child’s disability, prognosis, and care [40, 64, 67, 71, 77, 79, 84, 86, 87]. Interestingly, in one study, Malawian parents with greater knowledge were more distressed [58], but typically, knowledge was reported as empowering and positively affecting FQOL [42, 46, 63]. Some parents acquired information from the internet [55, 68], through peer-support groups (including online forums) [55], parent training [51], and further education [56], all of which enhanced FQOL.
Physical support
Although access to medical and rehabilitation services benefitted FQOL [41, 42, 60, 76], many authors reported that health/rehabilitation services were inaccessible and unaffordable, had few specialists, and provided limited access to assistive devices [10, 21, 22, 43, 50, 53, 54, 56, 57, 65, 67, 68, 70, 73, 80, 82, 83, 86]. Even when families did access services, poor professional attitudes, neglect, and lack of family-professional partnerships negatively affected FQOL [56, 62, 64, 65, 70, 79, 82]. Conversely, one article noted that therapists’ encouragement could improve FQOL [47]. Schlebusch et al. [88] found that South African families were most satisfied with disability-related support, whereas Ajuwon [87] found that Nigerian families were least satisfied with disability services.
Emotional support
Families described immediate and extended family as their primary source of emotional support [40,41,42, 44, 47, 56, 60, 61, 63, 69, 71, 75, 77, 80, 86, 87]. However, many families required more emotional support and lacked supportive family members (e.g. unreliable/unsupportive fathers or in-laws) [48, 54, 64, 82]. Support from friends, neighbours, community, and religious groups (i.e. churches) appeared to positively affect FQOL by providing emotional/social support (primarily to mothers), highlighting the crucial role of informal social support [40,41,42,43,44,45, 48, 50, 56, 60,61,62, 67, 68, 80, 84]. Some families requested psychological support (e.g. counselling) to improve FQOL [58, 78]. Parents also indicated that they would welcome peer-support groups to share their experiences and emotions [50, 55, 64, 75, 78, 79].
Other factors contributing to FQOL
Several other factors contributing to FQOL were found through inductive analysis. Most studies mentioned the prevalence and negative influence of stigma against children with disabilities and their families [21, 22, 40, 43, 47,48,49, 54,55,56,57, 60,61,62,63,64,65, 67,68,69, 71, 75, 77,78,79,80, 86, 87]. In rare, extreme cases, caregivers were encouraged to kill their child [63, 65, 78]. Stigma was often perpetuated by cultural beliefs or ignorance around disability leading to exclusion of the family from their community. When the mother was blamed for the disability (often by spouses/ in-laws, but also self-blame [69]), the family unit could breakdown and mothers were left alone to provide and care for their family [49, 60, 82]. However, one South African study found that although mothers experienced marginalisation from outside their immediate community, “counter-narratives to disrupt the dominant narratives of taboo, stigma and tragedy are embedded in the mothers’ histories, religious beliefs and the philosophy or ethic of Ubuntu” [80] (p.377). Several authors also described reduced stigma over time with increasing advocacy and community awareness [60, 69, 87].
In addition, researchers reported the negative effect of environmental barriers on FQOL. For example, Ajuwon [56] described Nigerian families’ challenges with “galloping inflation, general insecurity in their communities, the widespread degradation of the environment occasioned by traffic congestion, toxic wastes, air pollution, frequent power outages, constant noise from generating plants, and incessant flooding of urban centres that lack poor drainage systems” (p. 40). Harsh environmental conditions, geographical challenges, and inaccessible built environments also negatively affected FQOL [61, 82]. For example, Zimbabwe’s political/economic instability and deplorable conditions [22], and violence, crime, and alcohol abuse in South Africa [70] negatively affected FQOL.
Discussion
This review demonstrated the broad range of factors contributing to FQOL for families of children with disabilities across 14 African countries. These included individual member factors such as parental employment, the child’s behavioural challenges, and parents’ spirituality and acceptance of disability, as well as family unit factors such as socio-economic status, relationships, and beliefs/values. Support factors also contributed significantly to FQOL, where families expressed a need for support at multiple levels: material/instrumental (e.g. financial, educational, respite, transport), informational (e.g. prognosis, care requirements), physical (e.g. health/rehabilitation services), and emotional (e.g. sharing experiences). Broader themes that we found through inductive analysis were not only the prevalence and negative influence of poverty and stigma, but also the positive contribution of spirituality to FQOL. Despite Africa’s cultural diversity, from our findings, we noted similarities in overall factors affecting FQOL across countries. However, understanding cultural differences within specific African contexts (i.e. language, particular spiritual values/customs or stigmatising beliefs) can foster more effective, appropriate support provision.
Poverty and FQOL
Regardless of country, we found the prevalence of poverty and its negative effect on FQOL. These findings only reinforce the complex, nuanced link between disability and poverty [89,90,91,92,93,94,95]. Families of children with disabilities in high-income contexts are also vulnerable to poverty and its negative effects on health, family interactions, education, social involvement, productivity, and future prospects [96, 97]. However, in African contexts, inadequate government support/social welfare, barriers to services (i.e. affordability, availability and accessibility), and dangerous/unhygienic environments can intensify these effects [92, 98]. The World Health Organisation’s (WHO) International Classification of Functioning, Disability, and Health (ICF) categorises environmental barriers as products and technology, natural environment and human-made changes to the environment, support and relationships, attitudes, and services, systems and policies [99]. Several researchers have used the ICF framework to investigate environmental barriers for people with disabilities (including children) in African contexts [100, 101]: financial burdens, inadequate transportation and infrastructure, and inaccessible natural environments can all hinder participation, and subsequently FQOL. Additionally, carers are often either unable to maintain employment due to high-care demands (reducing financial resources) or have limited quality family time due to the demands of low-paid jobs and lengthy commutes [54, 92, 93], both negatively affecting FQOL. Our findings did not clearly identify differences in FQOL when the family was headed by a grandparent or sibling; however, this is likely to affect a family’s ability to generate income and would be interesting to explore in future research. Poverty not only compounds the negative effects of disability (e.g. physical and psychological burdens), but can also affect families’ ability to cope with these added challenges [92]. Although many African families show remarkable resilience and FQOL is not solely dependent on external circumstances, recognising and addressing the pervasive effects of poverty can help direct contextually relevant and sustainable support services to enhance FQOL. For example, research has demonstrated the potential of community-based rehabilitation (CBR) programmes in low-income contexts as an approach to provide more affordable, accessible services and to empower families of children with disabilities (e.g. through income-generation activities); however, active engagement from families and the community is essential for sustainability and effectiveness [102,103,104,105,106]. Health/rehabilitation providers also need to consider the far-reaching effects of poverty on families, providing holistic support to the whole family, not just the child, and making appropriate recommendations (e.g. low cost, local). In terms of policy, governments need greater accountability to ensure effective implementation of social welfare policies that consider the entire family’s needs [95, 107]. Moreover, disability should be considered in mainstream development policies and programmes [92]. Further research is needed related to poverty and FQOL in low-income settings to direct future policy and practice [92].
Stigma and FQOL
Stigma was another factor mentioned in most of our included articles across countries and disability type. Despite stigma being a universal phenomenon for families of children with disabilities, it is experienced differently in different cultures [108, 109], and the consequences can be severe for African families (i.e. pressure to kill the child). Belonging and community engagement are particularly important in African contexts where the philosophy of Ubuntu highlights how individual identities are formed through community relationships [33, 34, 95]. Ngubane-Mokiwa [34] specifically emphasises the need to renegotiate the meaning of Ubuntu and correct misinterpretations/misapplications in light of the common exclusion and discrimination of people with disabilities that directly opposes Ubuntu values. In African contexts, stigma often emerges from ignorance or traditional/supernatural beliefs around disability (e.g. curse, God’s punishment), though sometimes in combination with biomedical knowledge [86, 95, 98, 110,111,112]. Additionally, stigma is more explicitly gendered where mothers/female caregivers are often blamed for the child’s disability and usually by immediate/extended family (e.g. in-laws, spouse) [69, 82, 95, 112,113,114]. Considering again the ICF’s Environmental Factors, Huus et al. [101] found that social barriers, including exclusion and discrimination of children with disabilities, were the most common environmental barrier for participation. Negative attitudes toward disability can also be more common in rural areas, perhaps due to lower education or awareness [115]. Anti-stigma interventions that promote acceptance and belonging for children and their families are, therefore, critical for enhancing FQOL. Smythe and colleagues [116] conducted a systematic review of interventions to reduce stigma for children with disabilities and their families in LMICs, and despite limited quality evidence, they found that education programmes reduced negative attitudes. Stigmatising attitudes/behaviours from health and education professionals were also evident in some of our articles; hence, further training and exposure to disability are needed. In fact, health/rehabilitation professionals should be actively engaged in advocacy and reducing stigma for children with disabilities and their families [117]. Several articles in our review described advocacy efforts (particularly of mothers) that sought to raise community awareness and advocacy for children’s rights [43, 44, 60]. Our findings also highlighted the benefits of establishing peer-support groups for countering stigma, by providing emotional support/solidarity, information, and opportunities for income generation [54, 118]. CBR programmes can support advocacy efforts of self-help and peer-support groups [102]. In addition, Ajuwon [56] emphasised “religious and cultural leaders as the key to this shift in knowledge and practice” (p.42) to dismantle stigmatising attitudes and behaviours. Approaches at individual, family, societal, and multiple levels are needed to address stigma and promote belonging regardless of country, but they must “strive to be culturally and contextually responsive by adapting to meet the needs of individuals, families and communities in a given context, time and place, rather than simply applying a broad ‘culturally specific’ brush for all” [109] (p. 168).
Spirituality and FQOL
Although some spiritual beliefs can perpetuate stigmatising attitudes/behaviours towards children and their families, our findings also demonstrated how crucial spirituality is for families’ coping, resilience, and FQOL across countries and disability type. Other international studies have shown religion/spirituality’s positive effect on FQOL, giving families meaning, hope, and acceptance despite the additional challenges [16, 119,120,121,122,123,124,125]; however, religious/spiritual coping appears more common in LMICs [54, 92, 108]. Religious institutions can provide a supportive inclusive community, emotionally and practically, yet at the same time may still perpetuate stigmatising attitudes [118, 126]. Health and education professionals need to understand and respect the significance of each families’ spiritual/religious beliefs and build on these as a strength to enhance FQOL, whilst providing evidence-based interventions in respectful partnership with families. Although spirituality is recognised as important for FQOL, further research is needed to explore the connection between spirituality and FQOL in African contexts.
Limitations
This review has several limitations that merit consideration. First, we only included original research published in English; thus, we may have missed important information in other languages or unpublished work. In addition, whilst we searched a broad range of databases and relevant journals, we did not have access to Africa-Wide Information which could have identified other relevant papers. Second, the majority of research (19/53 articles) originated from South Africa, giving a bias to this specific country rather than representing the African continent more broadly; however, we did include articles from 14 different countries and did not notice significant differences between countries regarding broad factors affecting FQOL. Finally, we found overlap within family unit and individual member factors (e.g. religion/spiritual beliefs), as well as disability type. However, the authors met frequently to discuss findings to ensure consistency.
Conclusion
FQOL is an important outcome for families of children with disabilities globally, and understanding its contributing factors can help to direct support provision. Understanding FQOL in African contexts is crucial to ensure that services are culturally appropriate and feasible, ultimately benefiting families. To the best of our knowledge, this is the first review that focuses on FQOL in African contexts. This scoping review demonstrates that universal factors contribute to FQOL (e.g. financial status, functional needs, family relationships, and values); however, poverty, stigma, and spirituality are particularly prevalent in African contexts and significantly contribute to FQOL. These factors are important to consider in international FQOL tools/measures to capture their influence on FQOL. Further research (qualitative and quantitative) is needed to explore FQOL in various African contexts, from the perspectives of support providers as well as families, to more fully direct intervention efforts.
References
Turnbull, A. P., Brown, I., & Turnbull, R. (2004). Families and People with Mental Retardation: International Perspectives (A. P. Turnbull, I. Brown, & R. Turnbull, Eds.). American Association on Mental Retardation.
Boelsma, F., Caubo-Damen, I., Schippers, A., Dane, M., & Abma, T. A. (2017). Rethinking FQoL: The dynamic interplay between individual and family quality of life. Journal of Policy and Practice in Intellectual Disabilities, 14(1), 31–38. https://doi.org/10.1111/jppi.12224
Samuel, P. S., Rillotta, F., & Brown, I. (2012). Review: The development of family quality of life concepts and measures. Journal of Intellectual Disability Research, 56(1), 1–16. https://doi.org/10.1111/j.1365-2788.2011.01486.x
Chiu, C., Kyzar, K., Zuna, N., Turnbull, A., Summers, J. A., & Gomez, V. A. (2013). Family quality of life. In M. W. Wehmeyer & . (Eds.), The Oxford handbook of positive psychology and disability (pp. 365–392). Oxford University Press.
Zuna, N., Summers, J. A., Turnbull, A. P., Hu, X., & Xu, S. (2011). Theorizing about family quality of life. In R. Kober (Ed.), Enhancing the quality of life of people with intellectual disabilities: From theory to practice (pp. 241–278). Springer. https://doi.org/10.1007/978-90-481-9650-0_15
Rillotta, F., Kirby, N., & Shearer, J. (2011). A comparison of two family quality of life measures: An Australian study. In R. Kober (Ed.), Enhancing the quality of life of people with intellectual disabilities: From theory to practice (pp. 305–348). Springer. https://doi.org/10.1007/978-90-481-9650-0_17
Rillotta, F., Kirby, N., Shearer, J., & Nettelbeck, T. (2012). Family quality of life of Australian families with a member with an intellectual/developmental disability. Journal of Intellectual Disability Research, 56(1), 71–86. https://doi.org/10.1111/j.1365-2788.2011.01462.x
Poston, D., Turnbull, A., Park, J., Mannan, H., Marquis, J., & Wang, M. (2003). Family quality of life: A qualitative inquiry. Mental retardation, 41(5), 313–328.
Schlebusch, L., Dada, S., & Samuels, A. (2017). Family quality of life of South African families raising children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 47(7), 1966–1977. https://doi.org/10.1007/s10803-017-3102-8
Aldersey, H. (2017). Family quality of life in the Democratic Republic of the Congo. Journal of Policy and Practice in Intellectual Disabilities, 14(1), 78–86. https://doi.org/10.1111/jppi.12189
Nidaw, B. (2018). The grace of a fulfilling life: Social inclusion in valued roles of women and children with disabilities in Ethiopia. Tilburg University.
Kassa, S. C. (2017). Drawing family boundaries: Children’s perspectives on family relationships in rural and urban Ethiopia. Children & Society, 31(3), 171–182. https://doi.org/10.1111/chso.12200
Brown, I., & Brown, R. (2004). Concepts for beginning study in family quality of life. In A. Turnbull, I. Brown, & H. R. Turnbull (Eds.), Families and people with mental retardation and quality of life: International perspectives (pp. 25–47). American Association on Mental Retardation.
Wang, M., & Brown, R. (2009). Family quality of life: A framework for policy and social service provisions to support families of children with disabilities. Journal of Family Social Work, 12(2), 144–167.
Brown, R. I., Hong, K., Shearer, J., Wang, M., & Wang, S.-y. (2011). Family quality of life in several countries: Results and discussion of satisfaction in families where there is a child with a disability. In R. Kober (Ed.), Enhancing the quality of life of people with intellectual disabilities: From theory to practice (pp. 377–398). Springer. https://doi.org/10.1007/978-90-481-9650-0_20
Boehm, T. L., & Carter, E. W. (2019). Family quality of life and its correlates among parents of children and adults with intellectual disability. American Journal on Intellectual and Developmental Disabilities, 124(2), 99–115. https://doi.org/10.1352/1944-7558-124.2.99
Kuhaneck, H. M., Madonna, S., Novak, A., & Pearson, E. (2015). Effectiveness of interventions for children with autism spectrum disorder and their parents: A systematic review of family outcomes. American Journal of Occupational Therapy. https://doi.org/10.5014/ajot.2015.017855
Jackson Carla, W., Wegner Jane, R., & Turnbull Ann, P. (2010). Family quality of life following early identification of deafness. Language, Speech, and Hearing Services in Schools, 41(2), 194–205. https://doi.org/10.1044/0161-1461(2009/07-0093
Kyzar, K. B., Brady, S. E., Summers, J. A., Haines, S. J., & Turnbull, A. P. (2016). Services and supports, partnership, and family quality of life: Focus on deaf-blindness. Exceptional Children, 83(1), 77–91. https://doi.org/10.1177/0014402916655432
International Association for the Scientific Study of Intellectual and Developmental Disabilities (IASSIDD). (2014). Families supporting a child with intellectual or developmental disabilities: The current state of knowledge. Journal of Applied Research in Intellectual Disabilities, 27(5), 420–430. https://doi.org/10.1111/jar.12078
Gona, J. K., Newton, C. R., Rimba, K. K., Mapenzi, R., Kihara, M., Vijver, F. V., & Abubakar, A. (2016). Challenges and coping strategies of parents of children with autism on the Kenyan coast. Rural and Remote Health, 16(2), 1–12.
van der Mark, E. J., & Verrest, H. (2014). Fighting the odds: Strategies of female caregivers of disabled children in Zimbabwe. Disability and Society, 29(9), 1412–1427. https://doi.org/10.1080/09687599.2014.934441
World Health Organisation (WHO) (2011). World report on disability. http://www.who.int/disabilities/world_report/2011/report.pdf
UNICEF. (2013). Children and young people with disabilities fact sheet. https://www.unicef.org/disabilities/files/Factsheet_A5__Web_REVISED.pdf
Kyzar, K. B., Turnbull, A. P., Summers, J. A., & Gomez, V. A. (2012). The relationship of family support to family outcomes: A synthesis of key findings from research on severe disability. Research and Practice for Persons with Severe Disabilities, 37(1), 31–44. https://doi.org/10.2511/027494812800903247
Friend, A., Summers, J., & Turnbull, A. (2009). Impacts of Family Support in Early Childhood Intervention Research. Education and Training in Developmental Disabilities, 44(4), 453–470. http://www.jstor.org/stable/24234255
Canary, H. E. (2008). Creating supportive connections: A decade of research on support for families of children with disabilities. Health Communication, 23(5), 413–426. https://doi.org/10.1080/10410230802342085
de Araujo, C. A. C., Paz-Lourido, B., & Gelabert, S. V. (2016). Types of support to families of children with disabilities and their influence on family quality of life. Ciencia and Saude Coletiva, 21(10), 3121–3130. https://doi.org/10.1590/1413-812320152110.18412016
Nuri, R. P., Batorowicz, B., & Aldersey, H. M. (2020). Family support and family and child-related outcomes among families impacted by disability in low- and middle-income countries: A scoping review. Journal of Child Health Care, 24(4), 637–654. https://doi.org/10.1177/1367493519883456
Lorenzo, T., McKinney, V., Bam, A., Sigenu, V., & Sompeta, S. (2019). Mapping participation of disabled youth in sport and other free-time activities to facilitate their livelihoods development. British Journal of Occupational Therapy, 82(2), 80–89. https://doi.org/10.1177/0308022618817281
McKenzie, J. A., McConkey, R., & Adnams, C. (2013). Intellectual disability in Africa: Implications for research and service development. Disability and Rehabilitation, 35(20), 1750–1755. https://doi.org/10.3109/09638288.2012.751461
Knight, L., Hosegood, V., & Timæus, I. M. (2016). Obligation to family during times of transition: Care, support and the response to HIV and AIDS in rural South Africa. AIDS Care, 28, 18–29. https://doi.org/10.1080/09540121.2016.1195486
Nolte, A., & Downing, C. (2019). Ubuntu – The essence of caring and being: A concept analysis. Holistic Nursing Practice, 33(1), 9–16. https://doi.org/10.1097/hnp.0000000000000302
Ngubane-Mokiwa, S. A. (2018). Ubuntu considered in light of exclusion of people with disabilities. African Journal of Disability, 7, 460–460. https://doi.org/10.4102/ajod.v7i0.460
Arksey, H., & O’Malley, L. (2005). Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology, 8(1), 19–32. https://doi.org/10.1080/1364557032000119616
Tricco, A. C., Lillie, E., Zarin, W., O’Brien, K. K., Colquhoun, H., Levac, D., Moher, D., Peters, M. D., Horsley, T., & Weeks, L. (2018). PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Annals of Internal Medicine, 169(7), 467–473. https://doi.org/10.7326/M18-0850
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. https://doi.org/10.1191/1478088706qp063oa
Hoffman, L., Marquis, J., Poston, D., Summers, J. A., & Turnbull, A. (2006). Assessing family outcomes: Psychometric evaluation of the Beach Center Family Quality of Life Scale. Journal of Marriage and Family, 68(4), 1069–1083. https://doi.org/10.1111/j.1741-3737.2006.00314.x
Brown, I., Brown, R. I., Baum, N. T., Isaacs, B. J., Myerscough, T., Neikrug, S., Roth, D., Shearer, J., & Wang, M. (2006). Family Quality of Life Survey: Main caregivers of people with intellectual or developmental disabilities. Toronto, ON, Canada: Surrey Place Centre.
Ahlert, I. A., & Greeff, A. P. (2012). Resilience factors associated with adaptation in families with deaf and hard of hearing children. American Annals of the Deaf, 157(4), 391–404. https://doi.org/10.1353/aad.2012.1629
Greeff, A. P., & Nolting, C. (2013). Resilience in families of children with developmental disabilities. Families, Systems and Health: The Journal of Collaborative Family HealthCare, 31(4), 396–405. https://doi.org/10.1037/a0035059
Greeff, A. P., & van der Walt, K.-J. (2010). Resilience in families with an autistic child. Education and Training in Autism and Developmental Disabilities, 45(3), 347–355.
Bannink, F., Idro, R., & van Hove, G. (2016). Parental stress and support of parents of children with spina bifida in Uganda. African Journal of Disability, 5(1), 225–225. https://doi.org/10.4102/ajod.v5i1.225
du Toit, C., Coetzee, Z., & Beeton, H. (2013). Mothers’ experiences of caring for a child with severe brain injury in a disadvantaged community in the Cape Flats. South African Journal of Occupational Therapy, 43(2), 17–22.
Minichil, W., Getinet, W., Derajew, H., & Seid, S. (2019). Depression and associated factors among primary caregivers of children and adolescents with mental illness in Addis Ababa, Ethiopia. BMC Psychiatry. https://doi.org/10.1186/s12888-019-2228-y
Awadalla, H. I., Kamel, E. G., Mahfouz, E. M., Mohamed, A. A., & El-Sherbeeny, A. M. (2010). Determinants of maternal adaptation to mentally disabled children in El Minia, Egypt. Eastern Mediterranean Health Journal, 16(7), 759–764.
Fatudimu, M. B., Hamzat, T. K., & Akinyinka, O. O. (2013). Comparative quality of life of Nigerian caregivers of children with cerebral palsy. International Journal of Therapy and Rehabilitation, 20(3), 131–135. https://doi.org/10.12968/ijtr.2013.20.3.131
Ntswane, A. M., & van Rhyn, L. (2007). The life-world of mothers who care for mentally retarded children: The Katutura township experience. Curationis, 30(1), 85–96. https://doi.org/10.4102/curationis.v30i1.1060
Marsh, V. M., Kamuya, D. M., & Molyneux, S. S. (2011). ‘All her children are born that way’: Gendered experiences of stigma in families affected by sickle cell disorder in rural Kenya. Ethnicity and health, 16(4–5), 343–359. https://doi.org/10.1080/13557858.2010.541903
Bannink, F., Idro, R., & Van Hove, G. (2018). Health related quality of life in children with spina bifida in Uganda. Disability and Health Journal, 11(4), 650–654. https://doi.org/10.1016/j.dhjo.2018.03.008
Zuurmond, M., O’Banion, D., Gladstone, M., Carsamar, S., Kerac, M., Baltussen, M., Tann, C. J., Gyamah Nyante, G., & Polack, S. (2018). Evaluating the impact of a community-based parent training programme for children with cerebral palsy in Ghana. PloS One. https://doi.org/10.1371/journal.pone.0202096
Alhazmi, A., Petersen, R., & Donald, K. A. (2018). Quality of life among parents of South African children with autism spectrum disorder. Acta neuropsychiatrica, 30(4), 226–231. https://doi.org/10.1017/neu.2018.5
Mohammed, F. M. S., Ali, S. M., & Mustafa, M. A. A. (2016). Quality of life of cerebral palsy patients and their caregivers: A cross sectional study in a rehabilitation center Khartoum-Sudan (2014–2015). Journal of Neurosciences in Rural Practice, 7(3), 355–361. https://doi.org/10.4103/0976-3147.182778
McNally, A., & Mannan, H. (2013). Perceptions of caring for children with disabilities: Experiences from Moshi, Tanzania. African Journal of Disability, 2(1), 1–10. https://doi.org/10.4102/ajod.v2i1.21
Pottas, A., & Pedro, A. (2016). Experiences of father carers of children with autism spectrum disorder: An exploratory study. Journal of Psychology in Africa, 26(6), 551–554. https://doi.org/10.1080/14330237.2016.1250426
Ajuwon, P. (2012). A study of Nigerian families who have children with and without down syndrome. Journal of Intellectual Disability Research, 56(7–8), 36–49. 25–27,29,32,41,45,46,48,54,56,60,62,65,71,73.
Barlindhaug, G., Umar, E., Wazakili, M., & Emaus, N. (2016). Living with disabled children in Malawi: Challenges and rewards. African Journal of Disability, 5(1), 254. https://doi.org/10.4102/ajod.v5i1.254
Masulani-Mwale, C., Kauye, F., Gladstone, M., & Mathanga, D. (2018). Prevalence of psychological distress among parents of children with intellectual disabilities in Malawi. BMC Psychiatry, 18(1), 146. https://doi.org/10.1186/s12888-018-1731-x
Dambi, J. M., Jelsma, J., & Mlambo, T. (2015). Caring for a child with cerebral palsy: The experience of Zimbabwean mothers. African Journal of Disability, 4(1), 1–10. https://doi.org/10.4102/ajod.v4i1.168
Cloete, L. G., & Obaigwa, E. O. (2019). Lived experiences of caregivers of children with autism spectrum disorder in Kenya. African Journal of Disability, 8, 1–9. https://doi.org/10.4102/ajod.v8i0.435
Pretorius, C., & Steadman, J. (2018). Barriers and facilitators to caring for a child with cerebral palsy in rural communities of the Western Cape, South Africa. Child Care in Practice, 24(4), 413–430. https://doi.org/10.1080/13575279.2017.1347146
Oti-Boadi, M. (2017). Exploring the lived experiences of mothers of children with intellectual disability in Ghana. SAGE Open. https://doi.org/10.1177/2158244017745578
Olawale, O. A., Deih, A. N., & Yaadar, R. K. K. (2013). Psychological impact of cerebral palsy on families: The African perspective. Journal of Neurosciences in Rural Practice, 4(2), 159–163. https://doi.org/10.4103/0976-3147.112752
Hemming, E., & Akhurst, J. (2009). Mothers’ life-worlds in a developing context when a child has special needs. Indo-Pacific Journal of Phenomenology, 9(1), 1–12. https://doi.org/10.1080/20797222.2009.11433988
Kyeremateng, J. D. A., Edusei, A., Dogbe, J. A., Opoku, M. P., Nketsia, W., Hammond, C., & Afriyie, S. A. (2019). Experiences of primary caregivers of children with cerebral palsy across the trajectory of diagnoses in Ghana. African Journal of Disability, 8, 1–11. https://doi.org/10.4102/ajod.v8i0.577
Gebeyehu, F., Sahile, A., & Ayalew, M. (2019). Burden, social support, and life satisfaction among caregivers of children with intellectual disability: The case of Felege Abay and Shembt primary schools, Bahir Dar, Ethiopia. International Quarterly of Community Health Education, 39(3), 147–153. https://doi.org/10.1177/0272684X18819974
Hartley, S., Ojwang, P., Baguwemu, A., Ddamulira, M., & Chavuta, A. (2005). How do carers of disabled children cope? The Ugandan perspective. Child: Care, Health and Development, 31(2), 167–180. https://doi.org/10.1111/j.1365-2214.2004.00464.x
Ambikile, J. S., & Outwater, A. (2012). Challenges of caring for children with mental disorders: Experiences and views of caregivers attending the outpatient clinic at Muhimbili National Hospital, Dar es Salaam - Tanzania. Child and Adolescent Psychiatry and Mental Health. https://doi.org/10.1186/1753-2000-6-16
Oti-Boadi, M., Dankyi, E., & Kwakye-Nuako, C. O. (2020). Stigma and forgiveness in Ghanaian mothers of children with autism spectrum disorders (ASD). Journal of Autism and Developmental Disorders, 50(4), 1391–1400. https://doi.org/10.1007/s10803-020-04366-x
van der Mark, E. J., Conradie, I., Dedding, C. W. M., & Broerse, J. E. W. (2019). ‘We create our own small world’: Daily realities of mothers of disabled children in a South African urban settlement. Disability and Society, 34(1), 95–120. https://doi.org/10.1080/09687599.2018.1511415
van der Mark, E. J., Conradie, I., Dedding, C. W. M., & Broerse, J. E. W. (2019). Exploring adaptation and agency of mothers caring for disabled children in an urban settlement in South Africa: A qualitative study. Women’s Studies International Forum. https://doi.org/10.1016/j.wsif.2019.102271
Shabo, F. H. (2011). Psychosocial impacts of mentally retarded children on parents in Sudan. Sudan Journal of Medical Sciences. https://doi.org/10.4314/sjms.v6i1.67270
Tigere, B., & Makhubele, J. C. (2019). The experiences of parents of children living with disabilities at Lehlaba protective workshop in Sekhukhune district of Limpopo province. African Journal of Disability. https://doi.org/10.4102/ajod.v8i0.528
Adegoke, B. O. A., Adenuga, O. O., Olaleye, O. A., & Akosile, C. O. (2014). Quality of life of mothers of children with cerebral palsy and their agematched controls. African Journal of Neurological Sciences, 33(1), 71–78.
Olivier, M. A., & Ah Hing, A. D. (2009). Autistic spectrum disorder (ASD): Parental challenges and strategies. Vulnerable Children and Youth Studies, 4(1), 58–66. https://doi.org/10.1080/17450120802290572
Alli, A., Abdoola, S., & Mupawose, A. (2015). Parents’ journey into the world of autism. South African Journal of Child Health, 9(3), 81–84. https://doi.org/10.7196/SAJCH.7942
Mbwilo, G., Smide, B., & Aarts, C. (2010). Family perceptions in caring for children and adolescents with mental disabilities: A qualitative study from Tanzania. Tanzania Journal of Health Research, 12(2), 129–137. https://doi.org/10.4314/thrb.v12i2.56400
Masulani-Mwale, C., Mathanga, D., Silungwe, D., Kauye, F., & Gladstone, M. (2016). Parenting children with intellectual disabilities in Malawi: The impact that reaches beyond coping? Child: Care Health and Development, 42(6), 871–880. https://doi.org/10.1111/cch.12368
Sandy, P. T., Kgole, J. C., & Mavundla, T. R. (2013). Support needs of caregivers: Case studies in South Africa. International Nursing Review, 60(3), 344–350. https://doi.org/10.1111/inr.12022
Muthukrishna, N., & Ebrahim, H. (2014). Motherhood and the disabled child in contexts of early education and care. Childhood, 21(3), 369–384. https://doi.org/10.1177/0907568214524233
Schlebusch, L., & Dada, S. (2018). Positive and negative cognitive appraisal of the impact of children with autism spectrum disorder on the family. Research in Autism Spectrum Disorders, 51, 86–93. https://doi.org/10.1016/j.rasd.2018.04.005
Singogo, C., Mweshi, M., & Rhoda, A. (2015). Challenges experienced by mothers caring for children with cerebral palsy in Zambia. South African Journal of Physiotherapy, 71(1), 1–6. https://doi.org/10.4102/sajp.v71i1.274
Geere, J. L., Gona, J., Omondi, F. O., Kifalu, M. K., Newton, C. R., & Hartley, S. (2013). Caring for children with physical disability in Kenya: Potential links between caregiving and carers’ physical health. Child: Care, Health and Development, 39(3), 381–392. https://doi.org/10.1111/j.1365-2214.2012.01398.x
Gona, J. K., Mung’ala-Odera, V., Newton, C. R., & Hartley, S. (2011). Caring for children with disabilities in Kilifi, Kenya: What is the carer’s experience? Child: Care Health and Development, 37(2), 175–183. https://doi.org/10.1111/j.1365-2214.2010.01124.x
Barr, M. D., Govender, P., & Rencken, G. (2016). Raising a child with down’s syndrome: Perspectives from South African urban care-givers. African Health Sciences, 16(4), 929–935. https://doi.org/10.4314/ahs.v16i4.7
Tilahun, D., Hanlon, C., Fekadu, A., Tekola, B., Baheretibeb, Y., & Hoekstra, R. A. (2016). Stigma, explanatory models and unmet needs of caregivers of children with developmental disorders in a low-income African country: A cross-sectional facility-based survey. BMC Health Services Research, 16(1), 152. https://doi.org/10.1186/s12913-016-1383-9
Ajuwon, P. M., & Brown, I. (2012). Family quality of life in Nigeria. Journal of Intellectual Disability Research, 56(1), 61–70. https://doi.org/10.1111/j.1365-2788.2011.01487.x
Schlebusch, L., Samuels, A. E., & Dada, S. (2016). South African families raising children with autism spectrum disorders: Relationship between family routines, cognitive appraisal and family quality of life. Journal of Intellectual Disability Research, 60(5), 412–423. https://doi.org/10.1111/jir.12292
Banks, L. M., Kuper, H., & Polack, S. (2017). Poverty and disability in low- and middle-income countries: A systematic review. PloS One. https://doi.org/10.1371/journal.pone.0189996
Eide, A. H., & Ingstad, B. (2013). Disability and poverty - Reflections on research experiences in Africa and beyond. African Journal of Disability, 2(1), 31–31. https://doi.org/10.4102/ajod.v2i1.31
Groce, N., Kembhavi, G., Wirz, S., Lang, R., Trani, J.-F., & Kett, M. (2011). Poverty and disability – A critical review of the literature in low and middle-income countries. Leonard Cheshire Research Centre Working Paper. https://doi.org/10.2139/ssrn.3398431
van der Mark, E. J., Conradie, I., Dedding, C. W. M., & Broerse, J. E. W. (2017). How poverty shapes caring for a disabled child: A narrative literature review. Journal of International Development, 29(8), 1187–1206. https://doi.org/10.1002/jid.3308
Barratt, J., & Penn, C. (2009). Listening to the voices of disability: Experiences of caring for children with cerebral palsy in a Rural South African setting. In M. Maclachlan & L. Swartz (Eds.), Disability and International Development (pp. 191–212). Springer. https://doi.org/10.1007/978-0-387-93840-0_13
Mont, D. (2019). Childhood disability and poverty. Leonard Cheshire Disability and Inclusive Development Centre Working Paper. https://doi.org/10.2139/ssrn.3398210
Chataika, T., & McKenzie, J. Considerations of an African childhood disability studies. In T. Curran & K. Runswick-Cole (Eds.), Disabled Children’s Childhood Studies (pp. 152–163). Palgrave Macmillan. https://doi.org/10.1057/9781137008220_12
Dines, M. (2020). Protecting posterity: The effect of disability and poverty on children. http://hdl.handle.net/11558/5415
Park, J., Turnbull, A. P., & Turnbull, H. R. (2002). Impacts of poverty on quality of life in families of children with disabilities. Exceptional Children, 68(2), 151–170. https://doi.org/10.1177/001440290206800201
Adugna, M. B., Nabbouh, F., Shehata, S., & Ghahari, S. (2020). Barriers and facilitators to healthcare access for children with disabilities in low and middle income sub-Saharan African countries: A scoping review. BMC Health Services Research, 20(1), 1–11. https://doi.org/10.1186/s12913-019-4822-6
World Health Organisation (WHO) (2001). International Classification of Functioning, Disability and Health (ICF). World Health Organisation. https://www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health
Visagie, S., Eide, A. H., Dyrstad, K., Mannan, H., Swartz, L., Schneider, M., Gubela, M., Alister, M., Mustafa, K., Gert van, R., Karl-Gerhard, H., & Malcolm M. (2017) Factors related to environmental barriers experienced by persons with and without disabilities in diverse African settings. PloS one. https://doi.org/10.1371/journal.pone.0186342
Huus, K., Schlebusch, L., Ramaahlo, M., Samuels, A., Berglund, I. G., & Dada, S. (2021). Barriers and facilitators to participation for children and adolescents with disabilities in low-and middle-income countries – A scoping review. African Journal of Disability, 10, 771. https://doi.org/10.4102/ajod.v10i0.771
Wickenden, M., & Elphick, J. (2016). Don’t forget us, we are here too! Listening to disabled children and their families living in poverty. In S. Grech & K. Soldatic (Eds.), Disability in the Global South. International Perspectives on Social Policy, Administration, and Practice (pp. 167–185). Springer. https://doi.org/10.1007/978-3-319-42488-0_11
Mol, T. I., Van Brakel, W., & Schreurs, M. (2014). Children with disability in Nepal: New hope through CBR? Disability, CBR and Inclusive Development. https://doi.org/10.5463/DCID.v25i1.299
Bongo, P. P., Dziruni, G., & Muzenda-Mudavanhu, C. (2018). The effectiveness of community-based rehabilitation as a strategy for improving quality of life and disaster resilience for children with disability in rural Zimbabwe. Jamba: Journal of Disaster Risk Studies, 10(1), 442. https://doi.org/10.4102/jamba.v10i1.442
Njelesani, J., Couto, S., & Cameron, D. (2011). Disability and rehabilitation in Tanzania: A review of the literature. Disability and Rehabilitation, 33(23/24), 2196–2207. https://doi.org/10.3109/09638288.2011.563817
Ngubane, M., & Chetty, V. (2017). Caregiver satisfaction with a multidisciplinary community-based rehabilitation programme for children with cerebral palsy in South Africa. South African Family Practice, 59(1), 35–40. https://doi.org/10.1080/20786190.2016.1254929
Shumba, T. W., & Moodley, I. (2018). Implementation of disability policy framework in Namibia: A qualitative study. South African Journal of Physiotherapy. https://doi.org/10.4102/sajp.v74i1.400
Aldersey, H. M., Ahmed, A. N., Tesfamichael, H. N., & Lotoski, N. (2020). Needs of families of children with intellectual and developmental disabilities in Addis Ababa. African Journal of Disability, 9, 735. https://doi.org/10.4102/ajod.v9i0.735
Jansen-van Vuuren, J., & Aldersey, H. M. (2020). Stigma, acceptance and belonging for people with IDD across cultures. Current Developmental Disorders Reports, 7(3), 163–172. https://doi.org/10.1007/s40474-020-00206-w
Stone-MacDonald, A. (2012). Cultural beliefs about disability in practice: Experiences at a special school in Tanzania. International Journal of Disability, Development, and Education, 59(4), 393–407. https://doi.org/10.1080/1034912X.2012.723947
Bunning, K., Gona, J. K., Newton, C. R., & Hartley, S. (2017). The perception of disability by community groups: Stories of local understanding, beliefs and challenges in a rural part of Kenya. PLoS One. https://doi.org/10.1371/journal.pone.0182214
Taderera, C., & Hall, H. (2017). Challenges faced by parents of children with learning disabilities in Opuwo, Namibia. African Journal of Disability, 6, 1–10. https://doi.org/10.4102/ajod.v6i0.283
Aldersey, H., Kavira, S., Kiasimbua, J., Lokako, W., Miaka, P., & Monte, L. (2018). Stigma experienced by families with members with intellectual disabilities in Kinshasa. Democratic Republic of the Congo. Intervention, 16(2), 119–128. https://doi.org/10.4103/INTV.INTV_13_18
Hepperlen, R. A., Rabaey, P., Ament-Lemke, A., & Manley, H. (2021). Caring for a child with a disability in a Zambian community: A study using photo-elicitation. Child: Care, Health and Development. https://doi.org/10.1111/cch.12851
Maart, S., Eide, A. H., Jelsma, J., Loeb, M. E., & Ka Toni, M. (2007). Environmental barriers experienced by urban and rural disabled people in South Africa. Disability and Society, 22(4), 357–369. https://doi.org/10.1080/09687590701337678
Smythe, T., Adelson, J. D., & Polack, S. (2020). Systematic review of interventions for reducing stigma experienced by children with disabilities and their families in low- and middle-income countries: State of the evidence. Tropical Medicine and International Health, 25(5), 508–524. https://doi.org/10.1111/tmi.13388
Jansen-van Vuuren, J., Aldersey, H. M., & Lysaght, R. (2020). The role and scope of occupational therapy in Africa. Disability and Rehabilitation. https://doi.org/10.1080/09638288.2020.1743779
McKenzie, J. A., Kahonde, C., Mostert, K., & Aldersey, H. M. (2020). Community participation of families of children with profound intellectual and multiple disabilities in South Africa. Journal of Applied Research in Intellectual Disabilities, 34(2), 525–536. https://doi.org/10.1111/jar.12818
Boehm, T. L., & Carter, E. W. (2019). Facets of faith: Spirituality, religiosity, and parents of individuals with intellectual disability. Intellectual and Developmental Disabilities, 57(6), 512–526. https://doi.org/10.1352/1934-9556-57.6.512
Taub, T., & Werner, S. (2016). What support resources contribute to family quality of life among religious and secular Jewish families of children with developmental disability? Journal of Intellectual and Developmental Disability, 41(4), 348–359. https://doi.org/10.3109/13668250.2016.1228859
Karaca, A., & Konuk Şener, D. (2019). Spirituality as a coping method for mothers of children with developmental disabilities. International Journal of Developmental Disabilities. https://doi.org/10.1080/20473869.2019.1603730
Huang, Y. P., Chen, S. L., & Tsai, S. W. (2012). Father’s experiences of involvement in the daily care of their child with developmental disability in a Chinese context. Journal of Clinical Nursing, 21(21–22), 3287–3296. https://doi.org/10.1111/j.1365-2702.2012.04142.x
Norizan, A., & Shamsuddin, K. (2010). Predictors of parenting stress among Malaysian mothers of children with down syndrome. Journal of Intellectual Disability Research, 54(11), 992–1003. https://doi.org/10.1111/j.1365-2788.2010.01324.x
Kermanshahi, S. M., Vanaki, Z., Ahmadi, F., Kazemnejad, A., Mordoch, E., & Azadfalah, P. (2008). Iranian mothers’ perceptions of their lives with children with mental retardation: A preliminary phenomenological investigation. Journal of Developmental and Physical Disabilities, 20(4), 317–326. https://doi.org/10.1007/s10882-008-9099-3
Poston, D. J., & Turnbull, A. P. (2004). Role of spirituality and religion in family quality of life for families of children with disabilities. Education and Training in Developmental Disabilities, 39(2), 95–108.
Mugeere, A. B., Omona, J., State, A. E., & Shakespeare, T. (2020). “Oh God! Why did you let me have this disability?”: Religion, spirituality and disability in three African countries. Journal of Disability and Religion, 24(1), 64–81. https://doi.org/10.1080/23312521.2019.1698387
Acknowledgements
We would like to sincerely thank the Queen’s University Health Sciences librarian, Ms. Paola Durando for all of her time and support in assisting us with database searches for this review.
Funding
The first author receives funding for her Ph.D. from a Queen Elizabeth II Diamond Jubilee Scholarship program from Universities Canada, Rideau Hall Foundations, and Community Foundations Canada (2018–2021). However, the funders had no influence on the research process, writing, or publication.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to declare that are relevant to the content of this article.
Availability of data
Not applicable.
Code availability
Not applicable.
Ethical approval
This article does not contain any study with human participants conducted by any of the authors.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Jansen-van Vuuren, J., Nuri, R.P., Nega, A. et al. Family quality of life for families of children with disabilities in African contexts: a scoping review. Qual Life Res 31, 1289–1307 (2022). https://doi.org/10.1007/s11136-021-02994-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-021-02994-z