
Abstract
Purpose
In patients with ischemic heart disease, the objectives were (1) to explore associations between patient-reported outcomes, sociodemographic, and clinical factors at discharge and 1-year all-cause mortality and (2) to investigate the discriminant predictive performance of the applied patient-reported outcome instruments on 1-year all-cause mortality.
Methods
Data from the Danish national DenHeart cohort study were used. Eligible patients (n = 13,476) were invited to complete a questionnaire-package, of which 7167 (53%) responded. Questionnaires included the 12-item Short form health survey (SF-12), Hospital anxiety and depression scale (HADS), EQ-5D, HeartQoL, Edmonton symptom assessment scale (ESAS), and ancillary questions on, e.g., social support. Clinical and demographic characteristics were obtained from registers, as were data on mortality. Comparative analyses were used to investigate differences in patient-reported outcomes. Mortality associations were explored using multifactorially adjusted Cox regression analyses. Predictive performance was analyzed using receiver operating characteristics (ROC).
Results
Patient-reported outcomes at discharge differed among those alive versus those deceased at one year, e.g., depression (HADS-Depression ≥ 8) 19% vs. 44% (p < 0.001). Associations with 1-year mortality included feeling unsafe about returning home from the hospital; hazard ratio (HR) 2.07 (95% CI 1.2–3.61); high comorbidity level, HR 3.6 (95% CI 2.7–4.8); and being unmarried, HR 1.60 (95% CI 1.33–1.93). Best predictive performance was observed for SF-12 physical component summary (Area under the curve (AUC) 0.706).
Conclusion
Patient-reported health, sociodemographic, and clinical factors are associated with 1-year mortality. We propose systematic screening with robust predictive tools to identify patients at risk and healthcare initiatives to explore and offer effective treatment to modify patient-reported health indicators.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Plain English summary
Ischemic heart disease is the most common heart disease and a leading cause of death globally. Patients’ own view of their physical and emotional health is known to be a reliable indicator of their risk of dying. Studies are still needed to identify which patient-rated health factors are the most important and which questionnaires, measuring these factors, are the strongest to predict mortality. In our study, roughly 7000 patients responded to questionnaires about their health-related quality of life, physical symptoms, and emotional distress. After one year, we collected information on mortality and combined the data. We found that some of the most important factors in predicting death within the first year were symptoms of depression, having other illnesses and feeling unsafe about returning home from the hospital. The results can be used to develop a questionnaire-package with the ability to identify those patients at risk of dying with high precision. Health care providers can not only use this information to allocate extra resources to these patients but also use the questionnaire data to address relevant physical and emotional problems that traditional health assessments do not reveal.
Introduction
Ischemic heart disease is a leading cause of death globally and in Europe alone responsible for roughly 20% of all deaths yearly [1, 2]. Even though incidence and mortality rates have decreased in middle- and high-income countries, mortality risk remains high for patients with a poor cardiac risk factor profile [1]. Compiling evidence has shown that patients’ self-reported physical and psycho-emotional health, in addition to more well-known clinical and health behavior risk factors, are important components in risk factor profile assessment [1, 3].
Evidence supporting the prognostic relevance of patient-reported outcomes have consistently demonstrated their association with serious adverse outcomes, including mortality [4,5,6,7,8,9,10,11]. Depression, in particular, has been strongly linked to mortality in patients with coronary artery disease, and a large meta-analysis found a 32% increased mortality risk for those with depressive symptoms, and a recent large study found a two-fold mortality risk for those diagnosed with depression [10, 11]. Health-related quality of life, anxiety, and symptom burden are other patient-reported outcomes that have been found to be associated with mortality, although the current evidence is not consistent [4,5,6,7,8,9]. In previous DenHeart research, we found a more than threefold risk of 1-year mortality for those with symptoms of depression and a 76% increased risk for those with anxiety symptoms among patients with ischemic heart disease [5].
Identifying poor physical and psycho-emotional health requires insight into the patients’ perceptions of their health, and high-quality patient-reported outcome measures can be used as tools to gain and quantify this insight [12]. The need for applying such measures in cardiovascular research, as well as in clinical practice, has been highlighted in European as well as American position papers [12,13,14]. Future work, however, is needed to solidify the prognostic value of patient-reported outcomes and to identify which patient-reported outcomes are the most predictive on mortality. Published literature investigating patient-reported health and mortality in patients with ischemic heart disease often report on small, selected patient populations, and studies exploring the predictive effect of various patient-reported outcome measures on mortality are lacking.
Objectives
The objectives of this study in patients with ischemic heart disease were (1) to investigate the associations between patient-reported outcomes including social support, disease management, and health behavior, as well as sociodemographic and clinical factors at discharge and 1-year all-cause mortality and (2) to investigate the predictive performance of the applied patient-reported outcome measures on mortality.
Methods
Study design
Data for this study were derived from the Danish national DenHeart study which is a cohort study including data from a questionnaire survey linked with complete baseline and follow-up register data. The published study protocol describes the design and methods in detail [15] and a brief overview is presented in the following.
Setting and participants
All patients discharged or transferred from a Danish heart center, between April 2013 and April 2014, were invited to participate in the survey. The questionnaire consisted of six standardized patient-reported outcome measures and 16 ancillary questions. The 80-item questionnaire took on average 20 min to complete. The patient’s assigned staff nurse assessed the patient’s eligibility for inclusion and either recruited the patient or noted the appropriate exclusion criteria. Patients were invited to either complete the questionnaire and return it before discharge or at home within three days following discharge. Patients transferred to another hospital were asked to complete the questionnaire at final discharge or within the following three days. Patients were excluded if they were younger than 18 years old, did not have a Danish civil registration number, or were considered incapable of reporting patient-reported outcomes (i.e., due to physical, cognitive, or linguistic impairment). The current study uses data only on patients with ischemic heart disease as an action diagnosis based on the International classification of diseases 10 (ICD-10) codes: I20–I25. The sample was divided into three subgroups: (1) IHD/AP subgroup: diagnoses reflecting chronic ischemic heart disease and stable angina (ICD-10: I20.1–I20.9, I24–I25); (2) non-STEMI/UAP subgroup: non-ST-elevation myocardial infarction and unstable angina (ICD-10: I20.0, I21.4–I21.9); and (3) STEMI subgroup: ST-elevation myocardial infarction (ICD-10: I21.0, I21.1, and I21.3). One-year follow-up data on all patients were collected retrospectively via national registers.
Variables, data sources, and measurements
Register data
Sociodemographic and clinical characteristics were obtained on all patients from the following national registers: the Danish national patient register [16], the Danish civil registration system [17], and the Danish Education Register [18]. Data included sex, age, marital status, length of hospital stay, educational level, and comorbidities. Comorbidities were collected 10 years back and were used for the calculation of the Tu comorbidity index score [19] excluding the DenHeart index admission. The score includes the following comorbidities: arrhythmia, cardiogenic shock, congestive heart failure, pulmonary edema, malignancy, diabetes, cerebrovascular diseases, chronic obstructive pulmonary disease, and acute and chronic renal failure. All diagnoses are weighed equally [19]. Education was categorized into three levels: (1) Basic (primary school); (2) medium (high school and vocational training); or (3) higher level (short-, medium-, and long-term higher education or research education). Comorbidity levels were divided into three categories using the Tu comorbidity index scores: (1) 0 for none; (2) 1–2 for moderate level; and (3) 3+ for high level.
Patient-reported outcome measures
In the current study, we used five of the standardized questionnaires and nine ancillary questions from the DenHeart survey. These were chosen to provide an overall reflection of the patient's physical and mental health, and all are outcomes that have been reported as influencing health outcomes. The standardized questionnaires are described briefly below.
The 12-item Short form health survey (SF-12) is a generic measure of self-rated health that can be amassed into a Physical component summary (PCS) and Mental component summary (MCS). Higher scores indicate better perceived health status [20]. Estimated minimal clinically important differences (MCIDs) of 3 and 2 points for the PCS and MCS, respectively, have been proposed [21].
The Hospital anxiety and depression scale (HADS) is a 14-item scale, offering two subscales measuring symptoms of anxiety (HADS-A) and symptoms of depression (HADS-D) [22]. Scores range from 0 to 21 and a score of eight or above indicates the possible presence of a mood disorder [22]. Proposed MCID is 1.7 points for both HADS subscales [23].
The EQ-5D-5L measures current health status [24]. It covers five dimensions including mobility, self-care, usual activities, pain/discomfort, and anxiety and depression rated on a five-point scale. A Visual analogue scale (VAS) is also included, ranging from 0 to 100 of self-perceived health with endpoints labeled as ‘best imaginable health state’ and ‘worst imaginable health state.’ Scores can be calculated into a summarized score for the five dimensions (EQ-5D index score) and a VAS score (EQ-5D VAS). Higher scores indicate better perceived health state [24]. For the EQ-5D index and VAS scores, suggested MCIDs are 0.051 and 6.9 points, respectively [25].
The HeartQoL is a heart disease-specific questionnaire developed in patients with ischemic heart disease measuring cardiac health-related quality of life [26]. The 14-item scale provides an overall global score (HeartQoL global), a 10-item physical subscale score (HeartQoL physical), and a 4-item emotional subscale score (HeartQoL emotional). Scores range from 0 to 3, with 3 indicating the best cardiac health-related quality of life [26]. A MCID estimate for the HeartQoL subscales is proposed as 0.35 point [27].
The Edmonton symptom assessment scale (ESAS) allows patients to rate their symptoms on a 10-point numeric rating scale [28]. The nine symptoms included are pain, fatigue, nausea, drowsiness, appetite, dyspnea, depression, anxiety, and well-being, and scores can be summarized into the ESAS distress score. Higher scores indicate the presence and intensity of symptoms [28]. We report the summary score and the individual symptoms fatigue and dyspnea in this study. For the ESAS, MCID estimates are suggested to be four points for the total score and one point for the individual symptom scores [29].
All instruments have been validated in patients with coronary artery disease [26, 30], except the ESAS [29]. All have been shown to be valid and reliable with internal consistency of scales/subscales exceeding an acceptable Cronbach’s alpha suggested as 0.70 [30, 31]. Additional information on the applied instruments including information on validity, reliability, and minimal important differences have been described elsewhere [15, 32]. Standardized patient-reported outcome measures were analyzed as continuous variables except the HADS which was dichotomized using the proposed cut-off score of ≥ 8.
Ancillary questions included the following: two questions reflecting social support (Does it ever happen that you are alone, even though you want to be with others?, and Do you have someone to talk to if you have problems or need support?); two questions reflecting disease management (Do you feel safe about returning home from the hospital?, and Do you know which symptoms should elicit contact to health care after your discharge?); and finally, four questions reflecting health behavior, height and weight, smoking, alcohol consumption, and physical activity. Questions reflecting social support and health behavior were derived from the Danish National Health Survey [33] and questions on disease management from the Danish national survey of patient experiences [34].
Data from the questionnaire were linked at the individual level with the relevant hospital discharge from the Danish National Patient Register and subsequently with data from other national registers.
Outcomes
One-year follow-up data on all-cause mortality were collected from the Danish civil registration system, which is a nationwide register with none lost to follow-up [17]. Data were collected at least one year following inclusion of the last participant.
Statistical methods
Continuous data are presented as mean and Standard deviation (SD) and categorical data as frequencies and percentages. Baseline characteristics, patient-reported outcomes, and mortality rates were analyzed using descriptive statistics. Differences in time to death among diagnostic subgroups and between survey responders and non-responders were analyzed using the log-rank test and visualized in Kaplan–Meier survival plots.
Associations with 1-year mortality were explored, by firstly analyzing differences in standardized patient-reported outcomes among those alive and those deceased at one year using Student’s t test for continuous variables and Pearson’s Chi-square test for categorical variables. Secondly, self-reported indicators of social support, disease management, and health behavior, as well as sociodemographic and clinical characteristics, and their associations with 1-year mortality were analyzed using Cox proportional hazards models with time to death as the underlying timescale and censoring on death. The assumptions on proportional hazards were assessed and verified. The standardized patient-reported outcomes were not explored in regression models as these have been reported in a prior DenHeart study [5]. The preselected indicator variables tested were chosen based on clinical relevance and prior research. Possible covariates were explored and significant differences among key variables were found between groups alive and deceased (Online resource 1). These were included as adjustment variables to reduce bias from confounding. The preselected indicator variables were tested individually and adjusted for sex, age, marital status, length of hospital stay, educational level, diagnostic subgroup, and the Tu comorbidity index score. Results are reported as hazard ratios (HRs) with 95% confidence intervals (CIs) and visualized in forest plots.
Receiver operating characteristic (ROC) curves with the Area under the curve (AUC) were generated to evaluate the crude discriminant predictive effect of the instruments and their subscales on 1-year mortality. This included the SF-12 PCS and MCS, the HADS-A and HADS-D, the EQ 5D index score and EQ-5D VAS plus the HeartQoL global and ESAS summary score. To allow for comparison, the HADS-A, HADS-D, and ESAS summary scores were reversed before analysis, as these scores indicate a poorer outcome with a high score as opposed to the remaining patient-reported outcomes. In general, an AUC of 0.5 suggests no predictive discrimination and 0.7 to 0.8 is considered acceptable [35].
A p-value of less than 0.05 was considered statistically significant. All analyses were done using IBM SPSS version 25.
Results
Participants
A total of 34,564 patients were discharged or transferred during the study period, 14,115 (41%) with ischemic heart disease. Eligible patients (n = 13,476) were invited to complete a questionnaire and 7167 responded (53%) (Fig. 1). The total sample consisted of 70% males, mean age was 66 years, SD 11, and 61% were married (Table 1). Looking into subgroups, more STEMI patients were male, younger and unmarried and had the lowest comorbidity of any group with 74% having no comorbidities compared with 57% in the non-STEMI/UAP group and 51% in the chronic IHD/AP group (Table 1). Baseline characteristics by responder group are presented as supplementary data (Online resource 2).

Patient flow-chart
Descriptive data
Table 2 presents the patient-reported outcomes in patients alive and patients deceased at 1-year follow-up. Missing data in summary scores were 19% for the SF-12 but did not exceed 5% for the remainder of the patient-reported outcome measures.
Scores for patients deceased at one year were significantly worse for all standardized patient-reported outcomes except the proportion of patients with a HADS-anxiety score ≥ 8. Lack of social support and poor disease management was significantly more prevalent in the deceased compared with alive patients at 1-year follow-up except for ‘not knowing whom to contact with questions about disease treatment.’ No associations were observed with the different indicators of health behavior, with the exception of poor physical fitness level (Table 2).
The overall 1-year mortality for the sample was 4% but varied among diagnostic subgroups with the lowest mortality rate of 3% in the chronic IHD/AP group and 6% in both the non-STEMI/UAP and the STEMI groups. The rates also varied between responders and non-responders with a mortality rate of 2% among responders and 7% among non-responders. Significant differences in time to death were identified both among diagnostic subgroups and responder groups (Fig. 2a and b).

Kaplan–Meier survival curves—a Diagnostic subgroups and b Survey responder groups (Total population, n = 13,476)
Outcome data
Figure 3a depicts associations with 1-year mortality among selected self-reported indicators of social support, disease management, and health behavior. Associations with 1-year mortality included poor physical fitness level, HR 2.23 (95% CI 1.56–3.17); feeling unsafe about returning home from the hospital, HR 2.07 (95% CI 1.18–3.61); and feeling alone occasionally or frequently, HR 1.63 (95% CI 1.12–2.37) (Fig. 3a). Among selected clinical and sociodemographic variables in the total population, depicted in Fig. 3b, associations were high comorbidity level score three and above, HR 3.6 (95% CI 2.7–4.8); STEMI group, HR 2.9 (95% CI 2.3–3.7); and being unmarried, HR 1.60 (95% CI 1.33–1.93) (Fig. 3b).

Associations with 1-year mortality—a Among self-reported indicators of social support, disease management, and health behavior (Responders, n = 7167) and b among selected clinical and sociodemographic variables (Total population, n = 13,476). Indicator variables were tested individually and adjusted for sex, age, marital status, length of hospital stay, educational level, diagnostic subgroup, and the Tu comorbidity index score
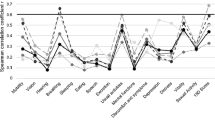
The best discriminant performance on 1-year mortality was observed for the SF-12 physical component summary (AUC 0.706), the EQ 5D VAS (AUC 0.666), and the HADS-D (AUC 0.653) (Fig. 4).

Receiver operating characteristic (ROC) curves of included patient-reported outcome measures (Responders, n = 7167)
Discussion
Key results
In this large unselected population of patients with ischemic heart disease, we found significant differences in patient-reported outcomes between those alive and those deceased at 1-year follow-up. Strong associations with 1-year mortality included feeling unsafe about returning home from hospital, high comorbidity level, and being unmarried. The best discriminant performance was observed for the self-rated physical health and symptoms of depression.
Interpretation
Patient-reported outcomes at discharge were not only statistically significantly different between patients alive and deceased at one year but also exceeded MCIDs for most scores. These included MCS and PCS (mental and physical health) of the SF-12; HADS-D (symptoms of depression); EQ-5D index and VAS scores (health status); HeartQoL global and physical subscales (disease-specific global and physical quality of life); and the ESAS total, fatigue, and dyspnea symptom scores. The HADS-A (symptoms of anxiety) and HeartQoL emotional (disease-specific emotional quality of life) did not exceed suggested MCIDs. Using MCIDs as a tool to interpret results might give an indication of the clinical relevance of a result. This is particularly relevant when working with patient-reported outcomes where a stastistically significant scale score difference may, in fact, make no real difference to the patients or clinicians. The validity of a MCID is thus important, and a review has highlighted that multiple methods are applied in estimating MCIDs leading to different results [36]. Researchers should take this into account and consider the method and context in which the estimates have been produced and how this relates to the conclusions of their own work.
Our findings are generally in line with previous research, adding to the compiling evidence of a strong link between poor patient-reported health indicators and mortality, particularly convincing for depression [4,5,6,7,8,9,10,11]. Nonetheless, mental health still seems to go unrecognized and undertreated in cardiac patients [37], and the recent cardiovascular disease statistics from the European Society of Cardiology state that although psychological and social factors are well established as cardiovascular risk factors, they are still not included in standardized assessment [1].
Self-reported indicators of lack of support and poor disease management were also, for the most part, significantly different among alive and deceased. Remarkably, self-reported indicators of health behavior covering more conventional cardiac risk factors such as obesity and smoking revealed no difference, except for poor physical fitness levels. Responses about health behavior at hospital discharge following a cardiac event may inaccurately reflect prior health behavior, and these factors are also known to be prone to social desirability bias [13], which may explain why the expected differences are not found. Even so, obesity, excessive alcohol use, and particularly smoking are well-established cardiac risk factors [3], although perhaps getting a disproportionate amount of attention compared with psychological and social factors that may warrant a much higher priority. In 2004, the large international INTERHEART study identified nine risk factors associated with incident myocardial infarction, and looking at the population attributable risks, they identified psychosocial factors as the third most attributable risk factor, only superseded by hypercholesterolemia and smoking and succeeded by more traditional risk factors, such as obesity, exercise, and alcohol intake [3] that are all factors traditionally intervened upon. Concordantly, previous DenHeart research found the three strongest population attributable risk factors of 1-year mortality, in a mixed population with cardiac disease, to be symptoms of depression, smoking, and anxiety [38]. The same study found that both anxiety and depression were associated with cardiac risk behavior including smoking, excessive eating, excessive alcohol consumption, and medication non-adherence, thus underpinning the close biobehavioral relationship between poor mental health and cardiac risk factors and, presumably, the causative mechanisms behind poor mental health and mortality risk [38]. Jointly, these findings bring into question whether it might be more appropriate to intervene upon psychological and social factors to not only alleviate the related distress and suffering for patients but also to reduce the increased risk of poor outcomes that are associated both directly and indirectly via the harmful health behavior choices these patients may make.
Looking at associations with 1-year mortality among clinical and sociodemographic variables, most results were in concordance with previous research [5], except for lower educational level not being associated with mortality, which is in contrast to other research in this area [39], however coincides with prior DenHeart findings [40]. Being unmarried was associated with 1-year mortality which was supported by our supplementary data, where 62% in the alive group were married compared to 46% in the deceased group (Online resource 1). Feeling lonely and feeling unsafe about returning home from the hospital were also associated with 1-year mortality, which are both presumably linked to living alone and having little or no social support. Living alone has consistently been found to be linked to the progression of cardiovascular disease as well as increased morbidity and mortality [41]. Interestingly, our prior DenHeart research found that feeling lonely was more predictive of poor outcomes than living alone and women who felt lonely had an almost three-fold mortality risk and men who felt lonely a two-fold mortality risk, whereas living alone only predicted 1-year mortality in men with a 34% increased risk [42].
In this study, we also explored the discriminant predictive effect of the instruments applied in order to provide insight into what measures might be most appropriate to include in the prognostic assessment in clinical practice. Physical health, measured by SF-12 PCS, was the only instrument with an acceptable AUC as a predictive tool, which seems apparent considering that poor self-rated physical health is a likely reflection of disease severity, which, in turn, is strongly linked to mortality [43]. Health measured by EQ-5D VAS and depression measured by the HADS-D had values just below the acceptable, however, in light of the substantial supportive evidence behind physical health and depression as linked to mortality [5,6,7, 9,10,11]; it seems reasonable that these instruments can offer a reliable predictive indication. Surprisingly, anxiety measured by HADS-A showed the lowest discriminant effect, indicating no discriminant predictive effect. Though several studies, including prior DenHeart research, have found associations between anxiety and mortality [4, 5, 8], the evidence is not consistent [4, 6, 9]. Anxiety is a more transient and variable state and presumably associations depend heavily on the time-point of data collection. DenHeart survey data were collected once at hospital discharge, and it is likely that a proportion of patients reporting symptoms of anxiety at discharge recover in the months following. Although an association can be demonstrated, the discriminant predictive effect may still be weak. This indicates that associations found in regression analysis may not be sufficient to conclude that an instrument will be able to predict an outcome. Further exploration within subgroups is also needed, as it is known that reporting varies substantially according to, for instance, sex and age. Thus, much more methodological work is needed to be able to include patient-reported outcomes in predictor models along with other relevant prognostic factors to accurately assess risk for each individual patient. Although the predictive performance of HADS-A was poor, it is important to acknowledge that anxiety as a permanent condition is agonizing for patients and has been linked to harmful health behavior and adverse outcomes [5, 36]. In a large study of patients with coronary heart disease, Moser and colleagues found that symptoms of anxiety measured at two time-points, and thus considered persistent, independently predicted morbidity and mortality, thus concluding that for anxiety to be a valid prognostic tool, it should be measured at multiple time-points [44]. More work is needed to explore when and how to screen for anxiety in order to detect those patients at risk who may benefit from treatment.
The health issues that patient-reported outcomes are indicative of are multiple and complex and require equally multifaceted and perhaps complex interventions. Cardiac rehabilitation has consistently been proven effective in improving particularly physical health and quality of life [45]. Though the term quality of life is commonly used in healthcare research, and is highlighted as an important patient outcome [1, 2], it has been argued for years that the term is being misused [46,47,48]. The claimed quality of life questionnaires usually measure the patients’ self-rated health, and although the term health-related quality of life is still very widely used in an attempt to more appropriately reflect the concept, more recent position papers use the term patient-reported outcome and patient-reported health status [13, 14]. For mental health concerns, the evidence is not robust, however, and approaches such as mindfulness and cognitive behavioral therapy have shown promising results and are safe and relatively inexpensive [49,50,51]. Lack of social support is arguably a societal problem in many high-income countries, where family structures have changed dramatically over the past century. Offering health care initiatives that can remedy loneliness and lack of support in a long-term and meaningful way for the individual is not feasible. Peer-support and additional attention to the needs and concerns of these patients following discharge are presumably the best we can offer as professionals.
Strengths and limitations
Our study included a large unselected sample of patients with ischemic heart disease. We used validated standardized patient-reported outcome measures, often used in cardiac populations, thus offering estimates that can be used for comparison and as benchmarks. We linked patient-reported data with high-quality register data with none lost to follow-up. These data allowed for the reduction of bias due to confounding factors in adjusted analysis, thus providing robust estimates. Although the DenHeart study aimed to include all patients and efforts were made to increase the response rate and secure complete data, the response rate in the overall study was 53%. Our data showed significant differences among responders and non-responders in baseline variables as well mortality rates, indicating that the most vulnerable patients were not included in this study. We expect that these non-responders would report worse patient-reported outcomes, thus possibly leading to underestimated results. Although we had access to information on several known confounding factors from registers and self-reported data, additional information about the burden of illness related to previous and current hospitalizations might have strengthened the study. Particularly the chronic IHD/AP group, included at various stages in their illness and with a large variation in the burden of disease, might have been too heterogeneous a group to assess as one. Adjustments in ROC analysis might have given insight into the predictive effect of the isolated instruments; however, we wanted to uncover the prognostic value as it would commonly be used in clinical practice, thus unadjusted. Repeated follow-up patient-reported outcome assessment could potentially have given insight into how these might evolve over time and have widened the perspective on the self-perceived illness trajectory. Not all patient-reported outcomes were validated in patients with ischemic heart disease, thus questioning the validity of results related to these. Also, not all MCID estimates were produced in cardiac patients; thus, interpretation should be considered indicative rather than conclusive. Multiple testing and mass-significance are potentially a problem in this study. The Bonferroni correction methods could have been applied to counteract this problem. Exploratory analysis, however, should always be interpreted with caution and be regarded as hypothesis-generating rather conclusive. Thus, the P values reported are uncorrected.
Conclusion
Patient-reported health status, symptoms of anxiety and depression, symptom burden, and disease-specific quality of life were expectedly and significantly different at discharge among patients alive versus patients deceased one year following. Strongest associations with 1-year all-cause mortality were high comorbidity, STEMI, poor physical fitness level, and feeling unsafe about returning home from the hospital. Predictive discriminant performance estimates of the patient-reported outcome instruments on mortality showed self-rated physical health (SF-12 PCS) to be a robust predictive tool, and probably also health status (EQ-5D VAS) and symptoms of depression (HADS-D) are acceptable.
The findings may guide clinicians and researchers in choosing appropriate patient-reported outcome measures. We propose systematic screening using robust predictive tools to identify patients at risk and healthcare initiatives to explore and offer effective treatment to modify poor patient-reported health indicators.
Generalizability
The study was carried out in Denmark. Differences among countries in health behavior, socioeconomic status, and healthcare provision are likely to impact public health and mortality in general, and generalizability of results may therefore be limited to similar cultural contexts. Generalizability of results is probably compromised by selection bias as our sample was not completely representative of the target population.
Data availability
The data underlying this article will be shared on reasonable request to the corresponding author.
References
Timmis, A., Townsend, N., Gale, C. P., et al. (2020). European society of cardiology: Cardiovascular disease statistics 2019. European Heart Journal, 41(1), 12–85. https://doi.org/10.1093/eurheartj/ehz859
Wilkins, E., Wilson, L., Wickramasinghe, K., et al. (2017) European cardiovascular disease statistics 2017. Brussels. Retrieved 19 Oct 2017 from http://www.ehnheart.org/images/CVD-statistics-report-August-2017.pdf
Yusuf, S., Hawken, S., Ounpuu, S., et al. (2004). Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet (London, England), 364(9438), 937–952. https://doi.org/10.1016/S0140-6736(04)17018-9
Celano, C. M., Millstein, R. A., Bedoya, C. A., Healy, B. C., Roest, A. M., & Huffman, J. C. (2015). Association between anxiety and mortality in patients with coronary artery disease: A meta-analysis. American Heart Journal, 170(6), 1105–1115. https://doi.org/10.1016/j.ahj.2015.09.013
Berg, S. K., Thorup, C. B., Borregaard, B., et al. (2019). Patient-reported outcomes are independent predictors of one-year mortality and cardiac events across cardiac diagnoses: Findings from the national DenHeart survey. European Journal of Preventive Cardiology, 26(6), 624–637. https://doi.org/10.1177/2047487318769766
Versteeg, H., Hoogwegt, M. T., Hansen, T. B., Pedersen, S. S., Zwisler, A. D., & Thygesen, L. C. (2013). Depression, not anxiety, is independently associated with 5-year hospitalizations and mortality in patients with ischemic heart disease. Journal of Psychosomatic Research, 75(6), 518–525.
Hansen, T. B., Thygesen, L. C., Zwisler, A. D., et al. (2014). Self-reported health-related quality of life predicts 5-year mortality and hospital readmissions in patients with ischaemic heart disease. European Journal of Preventive Cardiology. https://doi.org/10.1177/047487314535682
Wrenn, K. C., Mostofsky, E., Tofler, G. H., Muller, J. E., & Mittleman, M. A. (2013). Anxiety, anger, and mortality risk among survivors of myocardial infarction. American Journal of Medicine, 126(12), 1107–1113. https://doi.org/10.1016/j.amjmed.2013.07.022
Hosseini, S. H., Ghaemian, A., Mehdizadeh, E., & Ashraf, H. (2014). Levels of anxiety and depression as predictors of mortality following myocardial infarction: A 5-year follow-up. Cardiology Journal, 21(4), 370–377. https://doi.org/10.5603/CJ.a2014.0023
May, H. T., Horne, B. D., Knight, S., et al. (2017). The association of depression at any time to the risk of death following coronary artery disease diagnosis. European Heart Journal – Quality of Care and Clinical Outcomes, 3(4), 296–302. https://doi.org/10.1093/ehjqcco/qcx017
Meijer, A., Conradi, H. J., Bos, E. H., et al. (2013). Adjusted prognostic association of depression following myocardial infarction with mortality and cardiovascular events: Individual patient data meta-analysis. British Journal of Psychiatry, 203(2), 90–102. https://doi.org/10.1192/bjp.bp.112.111195
Norekval, T. M., Falun, N., & Fridlund, B. (2016). Patient-reported outcomes on the agenda in cardiovascular clinical practice. European Journal of Cardiovascular Nursing, 15(2), 108–111. https://doi.org/10.1177/1474515115614133
Anker, S. D., Agewall, S., Borggrefe, M., et al. (2014). The importance of patient-reported outcomes: A call for their comprehensive integration in cardiovascular clinical trials. European Heart Journal, 35(30), 2001–2009. https://doi.org/10.1093/eurheartj/ehu205
Rumsfeld, J. S., Alexander, K. P., Jr., Goff, D. C., et al. (2013). Cardiovascular health: The importance of measuring patient-reported health status: A scientific statement from the American heart association. Circulation, 127(22), 2233–2249. https://doi.org/10.1161/CIR.0b013e3182949a2e
Berg, S. K., Svanholm, J., Lauberg, A., et al. (2014). Patient-reported outcomes at hospital discharge from heart centres, a national cross-sectional survey with a register-based follow-up: The DenHeart study protocol. British Medical Journal Open, 4(5), e004709. https://doi.org/10.1136/bmjopen-2013-004709
Lynge, E., Sandegaard, J. L., & Rebolj, M. (2011). The danish national patient register. Scandinavian Journal of Public Health, 39(7 Suppl), 30–33. https://doi.org/10.1177/1403494811401482
Pedersen, C. B. (2011). The danish civil registration system. Scandinavian Journal of Public Health, 39(7 Suppl), 22–25. https://doi.org/10.1177/1403494810387965
Jensen, V. M., & Rasmussen, A. W. (2011). Danish education registers. Scandinavian Journal of Public Health, 39(7 Suppl), 91–94. https://doi.org/10.1177/1403494810394715
Tu, J. V., Austin, P. C., Walld, R., Roos, L., Agras, J., & McDonald, K. M. (2001). Development and validation of the Ontario acute myocardial infarction mortality prediction rules. Journal of the American College of Cardiology, 37(4), 992–997.
Ware, J. J., Kosinski, M., & Keller, S. D. (1996). A 12-item short-form health survey: Construction of scales and preliminary tests of reliability and validity. Medical Care, 34(3), 220–233.
Ware, J.J., Kosinski, M., Bjorner, J., Turner-Bowker, D., Gandek, B., Maruish. M. (2007) User’s manual for the SF 36v2® health survey (2nd ed.). Lincoln: Quality Metric Incorporated
Bjelland, I., Dahl, A. A., Haug, T. T., & Neckelmann, D. (2002). The validity of the hospital anxiety and depression scale. An updated literature review. Journal of Psychosomatic Research, 52(2), 69–77.
Lemay, K. R., Tulloch, H. E., Pipe, A. L., & Reed, J. L. (2019). Establishing the minimal clinically important difference for the hospital anxiety and depression scale in patients with cardiovascular disease. Journal of Cardiopulmonary Rehabilitation and Prevention, 39(6), E6–E11. https://doi.org/10.1097/HCR.0000000000000379
Rabin, R., & de Charro, F. (2001). EQ-5D: A measure of health status from the EuroQol group. Annals of Medicine, 33(5), 337–343.
Nolan, C. M., Longworth, L., & Lord, J. (2016). The EQ-5D-5L health status questionnaire in COPD: Validity, responsiveness and minimum important difference. Thorax, 71, 493–500. https://doi.org/10.1136/thoraxjnl-2015-207782
Oldridge, N., Hofer, S., McGee, H., et al. (2014). The HeartQoL: Part II. Validation of a new core health-related quality of life questionnaire for patients with ischemic heart disease. European Journal of Preventive Cardiology, 21(1), 98–106. https://doi.org/10.1177/2047487312450545
De Smedt, D., Clays, E., Hofer, S., et al. (2016). Validity and reliability of the HeartQoL questionnaire in a large sample of stable coronary patients: The EUROASPIRE IV study of the European society of cardiology. European Journal of Preventive Cardiology, 23(7), 714–721. https://doi.org/10.1177/2047487315604837
Chang, V. T., Hwang, S. S., & Feuerman, M. (2000). Validation of the edmonton symptom assessment scale. Cancer, 88(9), 2164–2171.
Hui, D., & Bruera, E. (2017). The Edmonton symptom assessment system 25 years later: Past, present, and future developments. Journal of Pain and Symptom Management, 53(3), 630–643. https://doi.org/10.1016/j.jpainsymman.2016.10.370
De, S. D., Clays, E., Doyle, F., et al. (2013). Validity and reliability of three commonly used quality of life measures in a large European population of coronary heart disease patients. International Journal of Cardiology, 167(5), 2294–2299. https://doi.org/10.1016/j.ijcard.2012.06.025
DeVellis, R. F. (2012). Scale development: Theory and applications (3rd ed.). Thousand Oaks: SAGE.
Rasmussen, T. B., Palm, P., Herning, M., et al. (2019). Subgroup differences and determinants of patient-reported mental and physical health in patients with ischemic heart disease: Results from the denheart study. Journal of Cardiovascular Nursing, 34(4), E11–E21. https://doi.org/10.1097/JCN.0000000000000583
Christensen, A. I., Ekholm, O., Glumer, C., et al. (2012). The danish national health survey study design and respondent characteristics. Scandivian Journal of Public Health, 40(4), 391–397. https://doi.org/10.1177/1403494812451412
The Danish National Survey of Patient Experiences [Om LUP | KOPA - Kompetencecenter for Patientoplevelser]. Retrieved 25 Sep 2020 from https://patientoplevelser.dk/lup/landsdaekkende-undersoegelse-patientoplevelser-lup/lup
Mandrekar, J. N. (2010). Receiver operating characteristic curve in diagnostic test assessment. Journal of Thoracic Oncology, 5(9), 1315–1316. https://doi.org/10.1097/JTO.0b013e3181ec173d
Mouelhi, Y., Jouve, E., Castelli, C., & Gentile, S. (2020). How is the minimal clinically important difference established in health-related quality of life instruments? Review of anchors and methods. Health and Quality of Life Outcomes. https://doi.org/10.1186/s12955-020-01344-w
Huffman, J. (2010). The relationship between depression, anxiety, and cardiovascular outcomes in patients with acute coronary syndromes. Neuropsychiatric Disease and Treatment, 6, 123. https://doi.org/10.2147/ndt.s6880
Berg, S. K., Rasmussen, T. B., Thrysoee, L., et al. (2018). Mental health is a risk factor for poor outcomes in cardiac patients: Findings from the national DenHeart survey. Journal of Psychosomatic Research, 112, 66–72. https://doi.org/10.1016/j.jpsychores.2018.07.002
Mackenbach, J. P., Bos, V., Andersen, O., et al. (2003). Widening socioeconomic inequalities in mortality in six Western European countries. International Journal of Epidemiology, 32(5), 830–837. https://doi.org/10.1093/ije/dyg209
Christensen, A. V., Juel, K., Ekholm, O., et al. (2020). Educational inequality in patient-reported outcomes but not mortality among cardiac patients: Results from the national DenHeart survey with register follow-up. Scandivian Journal of Public Health, 48(7), 781–790. https://doi.org/10.1177/1403494820901423
Jensen, M. T., Marott, J. L., Holtermann, A., & Gyntelberg, F. (2019). Living alone is associated with all-cause and cardiovascular mortality: 32 years of follow-up in the Copenhagen male study. European Heart Journal – Quality of Care Clinical Outcomes, 5(3), 208–217. https://doi.org/10.1093/ehjqcco/qcz004
Christensen, A. V., Juel, K., Ekholm, O., et al. (2020). Significantly increased risk of all-cause mortality among cardiac patients feeling lonely. Heart, 106(2), 140–146. https://doi.org/10.1136/heartjnl-2019-315460
Knuuti, J., Wijns, W., Achenbach, S., et al. (2020). 2019 ESC guidelines for the diagnosis and management of chronic coronary syndromes. European Heart Journal, 41(3), 407–477. https://doi.org/10.1093/eurheartj/ehz425
Moser, D. K., McKinley, S., Riegel, B., et al. (2011). Relationship of persistent symptoms of anxiety to morbidity and mortality outcomes in patients with coronary heart disease. Psychosomatic Medicine, 73(9), 803–809. https://doi.org/10.1097/PSY.0b013e3182364992
Anderson, L. J., & Taylor, R. S. (2014). Cardiac rehabilitation for people with heart disease: An overview of Cochrane systematic reviews. International Journal of Cardiology, 177(2), 348–361.
Dijkers, M. (2007). “What’s in a name?” The indiscriminate use of the “Quality of life” label, and the need to bring about clarity in conceptualizations. International Journal of Nursing Studies, 44(1), 153–155. https://doi.org/10.1016/j.ijnurstu.2006.07.016
Moons, P. (2004). Why call it health-related quality of life when you mean perceived health status? European Journal of Cardiovascular Nursing, 3(4), 275–277. https://doi.org/10.1016/j.ejcnurse.2004.09.004
Moons, P., Budts, W., & De, G. S. (2006). Critique on the conceptualisation of quality of life: A review and evaluation of different conceptual approaches. International Journal of Nursing Studies, 43(7), 891–901. https://doi.org/10.1016/j.ijnurstu.2006.03.015
Richards, S. H., Anderson, L., Jenkinson, C. E., et al. (2018). Psychological interventions for coronary heart disease: Cochrane systematic review and meta-analysis. European Journal of Preventive Cardiology. https://doi.org/10.1177/2047487317739978
Rutledge, T., Redwine, L. S., Linke, S. E., & Mills, P. J. (2013). A meta-analysis of mental health treatments and cardiac rehabilitation for improving clinical outcomes and depression among patients with coronary heart disease. Psychosomatic Medicine. https://doi.org/10.1097/PSY.0b013e318291d798
Abbott, R. A., Whear, R., Rodgers, L. R., et al. (2014). Effectiveness of mindfulness-based stress reduction and mindfulness based cognitive therapy in vascular disease: A systematic review and meta-analysis of randomised controlled trials. Journal of Psychosomatic Research, 76(5), 341–351. https://doi.org/10.1016/j.jpsychores.2014.02.012
Acknowledgements
Our gratitude to all the patients who took the time at a difficult stage in their life to fill out our questionnaire and to the healthcare staff who assisted us in the data collection. Thank you to Novo Nordisk Foundation and the participating heart centers for funding the DenHeart survey and to Herlev and Gentofte University Hospital, department of cardiology, for funding the current study. Finally, a special thank you to Phil Helfter for proof-reading the manuscript.
Funding
The study was funded by the five participating Heart centers and the Novo Nordisk Foundation (NNF130C0007229). The Heart centers participated in the collection of patient-reported outcomes, but neither they nor the Novo Nordisk Foundation influenced any part of study design or data interpretation.
Author information
Authors and Affiliations
Contributions
SKB conceived the idea for the DenHeart survey and TBR for the current sub-study. TBR and BB performed the statistical analyses. TBR drafted the manuscript. All co-authors revised the manuscript critically.
Corresponding author
Ethics declarations
Conflict of interest
Authors have no competing interests.
Ethical approval
The study was approved by the national data protection agency (reg. 2007-58-0015/30-0937). The Danish National Board of Health approved the use of register data (FSEID-01131). The study fully complies with the declaration of Helsinki and was registered at ClinicalTrials.gov (NCT 019-6145) and approved by the institutional boards of the participating heart centers. Surveys are not required by Danish legislation to be approved by humans’ ethics committee.
Consent to participate
All included patients signed informed consent.
Consent for publication
With their informed consent, participants agreed to the publication of results.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Rasmussen, T.B., Borregaard, B., Palm, P. et al. Patient-reported outcomes, sociodemographic and clinical factors are associated with 1-year mortality in patients with ischemic heart disease—findings from the DenHeart cohort study. Qual Life Res 31, 389–402 (2022). https://doi.org/10.1007/s11136-021-02956-5
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-021-02956-5