
Abstract
Background
Coronary artery disease (CAD) is known to impact on patients’ physical and mental health. The relationship between performance on treadmill exercise tolerance test (ETT) and health-related quality of life (HRQL)has never been specifically investigated in the setting of CAD.
Methods
Consecutive patients undergoing an ETT with the Bruce protocol during a diagnostic workup for CAD (n = 1,631, age 55 ± 12 years) were evaluated. Exercise-related indices were recorded. Detailed information on cardiovascular risk factors and past medical history were obtained. HRQLwas assessed with the use of the validated 36-Item Short Form Survey (SF-36) questionnaire.
Results
Increasing age and the presence of cardiovascular risk factors and comorbidities correlated with lower scores on the physical and mental health component of SF-36(all P < 0.05). Subjects with arrhythmias during exercise and slow recovery of systolic blood pressure had lower scores on the physical health indices or the Social Role Functioning component (P < 0.05). Achieved target heart rate and good exercise tolerance were independently associated with better scores of the physical and mental health domains of SF-36 and overall HRQLscores (β = 0.05 for target HR and PCS-36, β = 1.86 and β = 1.66 per increasing stage of exercise tolerance and PCS-36 and MCS-36, respectively, P < 0.001 for all associations). Ischemic ECG changes were associated with worse scores on Physical Functioning (β = − 3.2, P = 0.02) and Bodily Pain (β = − 4.55, P = 0.026).
Conclusion
ETT parameters are associated with HRQL indices in patients evaluated for possible CAD. Physical conditioning may increase patient well-being and could serve as a complementary target in conjunction with cardiovascular drug therapy.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
Mortality attributed to coronary artery disease (CAD) has declined over the last decades in the context of therapeutic advances and more effective primary and secondary prevention strategies. Still, CAD remains one of the leading causes of death in adults in developed countries [1]. Importantly, CAD has also a significant adverse impact on physical and mental wellbeing. Coronary heart disease presents with chest pain and shortness of breath mainly on exertion and symptoms can limit exercise capacity. Equally, CAD relates to significant anxiety about physical activity, as patients often fear that exercise may induce anginal symptoms or trigger life-threatening cardiac manifestations. The reluctance to exercise and the sedentary lifestyle can propagate a vicious circle of reduction in exercise tolerance and further detrimental effects on disease progression. Conversely, physical activity has been shown to correlate with improved quality of life (QoL) [2, 3] and to benefit mental health [4].
Health-related QoL (HRQL) measurements are patient-centred health outcomes that are useful for assessing both the impact of disease’s burden and the effectiveness of treatment interventions. Several studies have explored the negative consequences of CAD on the quality of life and mental health of patients [5,6,7]. Previous research has shown that patients with CAD have poorer HRQL than healthy controls [8]. Elucidating the factors that impair the QoL in CAD is crucial to gain insight into the global impact of the disease on patients’ life, and then to identify possible targets for intervention. To date, the relation of treadmill exercise tolerance test (ETT) parameters with physical and mental health has not been examined. Thus, the aim of this study was to evaluate the association between physical activity indices of patients with suspected or confirmed CAD and domains of physical and mental health. To this purpose, we used a well-characterized group of patients who underwent treadmill ETT and provided accurate estimates of physical ability.
Methods
Study sample
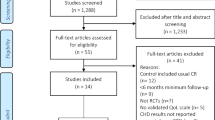
This cross-sectional study was conducted from January 2017 to June 2018 in a tertiary hospital setting. A total of 1,948 patients with known or suspected CAD [mean age 55 ± 12 years, 1270 (65%) males] were consecutively enrolled and underwent an ETT. The study was conducted in 1,631 subjects with complete data. The research protocol was approved by the local Ethics Committee (registration number: 2911-24022021) and all aspects of this research project were in compliance with the Declaration of Helsinki. All subjects gave informed consent prior to entering the study.
Demographic characteristics and risk factors
Detailed information was obtained for every participant with respect to smoking status, body mass index (BMI), hours of exercise per week, personal or family history of CAD, dyslipidemia, hypertension, diabetes mellitus and peripheral arterial disease, according to dedicated ESC (European Society of Cardiology) guideline definitions [9,10,11,12]. Current smokers were defined as those who were smoking at least one cigarette per day during the preceding month. Subjects with BMI > 30 kg/m2 were classified as obese, those between 25 and 30 kg/m2as overweight, those between 18.5 and 25 kg/m2as normal, and those < 18.5 kg/m2asunderweight. Family history of ischemic heart disease (IHD) was defined as having a first-degree male relative with CAD by age 55, or a first-degree female relative by age 65. The history of myocardial infarction was self-reported or according to hospital records, irrespective of the history of PCI (percutaneous coronary intervention), which was documented separately.
ETT
Participants underwent a treadmill ETT according to the standard Bruce protocol as previously described [13]. Briefly, we recorded blood pressure (BP) indices, heart rate (HR), and estimated work load in METs (metabolic equivalents, 1MET equals 3.5 ml of oxygen uptake per kg of body weight per minute) at the end of each of exercise stage, at peak exercise, and each minute after the cessation of exercise for a total of 3 min. Exercise capacity was quantified in METs and also in terms of total duration of exercise in mins. We used an ordinal scale to classify exercise tolerance in 6 categories (poor, modest, satisfactory, good, very good and excellent) given total exercise duration in mins and achieved workload in METs. The outcome of the treadmill ETT was adjudicated according to relevant ACC (American College of Cardiology)/AHA (American Heart Association) guidelines [14]. Target HR was calculated as 220-age (in years). HR recovery was defined as the reduction from the HR at peak exercise to the HR 2 min after the cessation of exercise. Slow HR recovery was defined as a change from peak exercise heart rate to heart rate measured 2 min later of less than or equal to 12 beats per minute [15].Exercise pulse pressure was calculated by the difference of systolic blood pressure (SBP) and diastolic blood pressure (DBP) at the end of each exercise stage. Delayed systolic blood pressure (SBP) recovery after exercise was defined as a value greater than 1 for SBP at 3 min of recovery divided by SBP at 1 min of recovery [16]. Positive (diagnostic) test results for CAD were defined using the ACC/AHA guidelines [14]. Arrhythmias during ETT were classified as supraventricular and ventricular as well as short- and wide-complex tachycardias according to 12-lead ECG appearance.
Assessment of HRQL
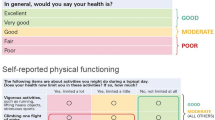
HRQL was assessed with the use of a self-administered questionnaire, the 36-Item Short Form Survey (SF-36) questionnaire (Greek standard version 1.0). The SF-36 is a generic measure of health status, which is not age or disease specific and consists of eight domains: physical functioning (PF); role physical (RP); bodily pain (BP); general health perception (GH); vitality (VT); social functioning (SF); role emotional (RE); and mental health (MH). Scores of physical component summary (PCS-36), mental component summary (MCS-36) and the eight domains were calculated from raw data, according to SF-36 manual. The domain scores ranged from 0 to 100, with higher scores indicating a better health status, and were transformed to have a mean of 50 and standard deviation of 10. Missing values were treated according to procedures suggested in the SF-36 manual [17].
Statistical analysis
Continuous variables are presented with mean and standard deviation (SD). Quantitative variables are presented with absolute and relative frequencies. Kolmogorov- Smirnov tests were used to access normality of the variables. Linear regression analyses were used to detect independently associated factors with HRQL dimensions. A prespecified set of confounders was used in regression analyses, including age, gender, BMI, cardiovascular risk factors (smoking, hypertension, hypercholesterolemia, family history of ischaemic heart disease, diabetes), features of CAD (previous infarction, previous revascularization) and PAD. Adjusted regression coefficients (β) with standard errors (SE) were reported from the results of the linear regression analyses. Multicollinearity was assessed via variance inflation factor (VIF) and it was found below 4 in all cases, indicating no presence of multicollinearity [18]. All P-values reported are 2-tailed. The significance level was set at 0.05. All analyses were conducted with the SPSS statistical package (Version 22.0).
Results
Patient characteristics (n = 1,631) are presented in Table 1. The treadmill ETT was positive in 9.3% of the participants, while a slow recovery of HR and SBP was found in 32.6% and 57.2% of the participants, respectively. Table 2 shows the mean values of the SF-36 dimensions in the study population. The scales with the best and the poorest score values were the Physical Functioning and the Summary Mental Health Scale, respectively.
Multiple linear regression analyses for dimensions of SF-36 related to physical health (Table 3) showed that increasing age was associated with worse physical functioning, a greater perception of pain, and a worse global health status. Furthermore, participants with normal BMI had a lower perception of pain than obese individuals. Current smokers reported more pain, and subjects with hypercholesterolemia, previous CABG (coronary artery bypass surgery), peripheral arterial disease or diabetes had a worse general health status. As for ETT metrics, a longer exercise duration was associated with greater physical functioning (β = 0.64 per minute increase, P = 0.005), and achieved target HR (β = 0.15, P < 0.001 for physical functioning) and good exercise tolerance (β = 4.32 per increasing stage of exercise tolerance, P < 0.001 for bodily pain) were found to be associated with better scores on all dimensions related to physical health (Fig. 1a). Subjects with arrhythmias and those with slow recovery of SBP reported more body pain. Finally, ischaemic changes on the ECG were associated with worse physical functioning (β = − 3.2, P = 0.02) and more body pain (β = − 4.55, P = 0.026), while we did not find a significant association between positive ETT for CAD with exercise capacity (P = 0.179). All univariate associations between markers of exercise and indices of QoL were similar to multivariable associations. This minimised the risk of residual multi-collinearity or bias due to missing data for certain outcomes or exposure variables.

Physical (i.e. bodily pain) a and mental health b dimensions of quality of life are related to exercise tolerance in 1,631 subjects undergoing treadmill ETT. Coefficients and P-values are derived from multiple linear regression analysis after adjustment for major demographic characteristics, cardiovascular risk factors, presence of CAD and previous revascularization and PAD. β regression coefficient, ETT exercise tolerance test, CAD coronary artery disease, PAD peripheral arterial disease
More advanced age was associated with lower scores on all mental health scales (Table 4). Current smokers had worse scores on Vitality, Emotional Role Functioning and Mental Health. Additionally, achieved target HR (β = 0.07, P = 0.015 for mental health) and exercise tolerance (β = 2.69 per increasing stage of exercise tolerance, P < 0.001 for mental health) were found to be associated with better scores on all mental health dimensions (Fig. 1b), while subjects with a slow recovery of SBP had lower scores of social functioning (β = -2.62 per 1-unit increase in SBP at 3 min of recovery divided by SBP at 1 min post peak, P = 0.042).
Current smokers had lower scores of a mental component summary (MCS-36) scale, and subjects with diabetes had lower scores of a physical component summary (PCS-36) scale (Table 5).
With respect to potential differences in QoL indices between subjects with and without CAD, we tested a dedicated factor variable (i.e. presence of CAD as compared to absence of CAD) in all relevant regression models (Tables 3–5). Still, no significant associations with HRQoL were found.
Discussion
To our knowledge, this is the first study to demonstrate that treadmill exercise stress test parameters are associated with QoL indices. In brief, we found that specific risk factors for CAD (advanced age, obesity, hypercholesterolaemia, smoking, diabetes) and treadmill ETT parameters (inability to achieve the target HR, poor exercise tolerance, decreased exercise duration, positive stress test result, slow recovery of SBP, arrhythmias) are negatively associated with patients’ QoL and mental health. Among treadmill ETT parameters, the inability to achieve the target heart rate and the decreased exercise tolerance were the most significant ones, as they were found to be negatively associated with all 8 components of the HRQL indices.
Age is the strongest factor related to the development of CAD, as well as mortality, once coronary atherosclerosis manifests [19]. Age has been previously shown to influence adversely HRQL in patients with CAD [6]. There is, however, one study by Bosworth et al. [20], which produced slightly different results using the SF-36 questionnaire in patients with CAD. The researchers reported that while increased age was associated with decreased physical function and physical role function as expected, it was also associated with increased emotional role function, mental health and vitality. In our study, advanced age was found to have a significant negative impact on all eight domains assessed with the SF-36 questionnaire, addressing both physical and mental health.
Contrary to other studies [20,21,22,23,24,25], we did not identify a significant effect of gender on quality of life. However, smoking was shown to have a significant negative impact on bodily pain and three aspects of mental health (vitality, emotional role functioning and overall mental health). This is in keeping with previous evidence which suggests that smoking is associated with poor physical and mental health in patients with CAD. In a study by Stafford et al. [26], exposure to smoking at the time of the index cardiac event was found to be independently associated with an increased risk of major depressive disorder, minor depression or dysthymia.
Furthermore, hyperlipidaemia, diabetes and previous CABG had a negative impact on general health perceptions (part of physical health indices) in our study, but they did not seem to affect any of the mental health outcomes. The impact of hyperlipidaemia on quality of life has been assessed in the past, and the results have been conflicting. Farhat et al. reported that patients with hyperlipidaemia have lower quality of life when compared to controls [27],while Lalonde et al. [28] found that patients with hyperlipidaemia reported better physical health compared to those with normal lipid profile. HRQL has also been assessed extensively in patients with familial hypercholesterolaemia (FH). Some studies showed that FH has a negative impact on quality of life [29, 30], while others suggested that it does not affect it to a significant extent [31]. One study demonstrated that quality of life is affected only in FH patients who do not reach treatment targets [32], possibly offering an explanation for the conflicting results in literature. Evidence is more homogeneous for the deterioration of life quality in diabetes [33]. Accordingly, in our patients, diabetes had a significant negative impact on general health perceptions but not on the rest of the SF-36 categories.
Coronary revascularisation is linked with improvement in quality of life [34,35,36,37,38]. Of note, one study [39] that compared HRQL following revascularisation with either PCI or CABG, established a significant difference in favour of CABG when compared to the patients who had PCI, which arose from the better physical function in the former. Still, our results demonstrated negative association between CABG and general health perceptions category, while no significant association between PCI and any of the SF-36 outcomes was detected.
Importantly, our study provides initial evidence on treadmill stress test parameters which correlate with mental and physical health. Good exercise duration, achieved target HR, good exercise tolerance, diagnostic (positive) result for CAD and slow recovery of SBP were associated with quality outcomes. Among these parameters, the exercise tolerance and the achieved target HR stand out, as they appear to influence all eight SF-36 outcomes. To our knowledge, the correlation between treadmill stress test parameters and quality of life has not been examined before.
Achieving the target HR is challenging and suggests robust physical condition. Good exercise tolerance depends on similar factors and reflects optimal functional status. Based on the fact that good exercise capacity is known to be associated with improved quality of life [2, 3] and to benefit mental health [4], we expected these parameters to influence SF-36 positively. Interestingly, adequate exercise duration was only associated with better physical functioning, but not with any of the rest of physical or mental health outcomes.
These results corroborate previous studies which have demonstrated that cardiac rehabilitation can improve functional capacity, physical activity levels and quality of life after acute coronary syndromes [40,41,42]. Regular aerobic exercise is known to prevent cardiovascular disease. Once CAD has developed, exercise appears to attenuate disease progression, improve event-free survival [43, 44], and increase the threshold of angina-free activity levels. At the level of the endothelium, exercise induces higher expression and phosphorylation of the endothelial isoform of NO (nitric oxide) synthase, hence increasing the vascular production of NO. This decreases the generation of reactive oxygen species (free radicals), potentiates the CPC (circulating progenitor cells)-mediated rejuvenation of the endothelium and formation of new vessels, and enhances the myocardial expression of vascular growth factors which induce remodelling of capillaries and arterioles [45,46,47]. As a result, regular aerobic exercise has been shown to improve arterial stiffness, and its effects seem to be more significant in patients with greater arterial stiffness at baseline [48]. This is translated in prognostic benefit, as cardiac rehabilitation in patients with established coronary heart disease is associated with reduced all-cause mortality and cardiac mortality, and this effect on all-cause mortality seems to be independent of coronary heart disease diagnosis, type and dose of rehabilitation, or length of follow-up [43]. At the same time, cardiac rehabilitation has been shown to be cost-effective for this patient population [49].
The main strength of this study is the thorough investigation of the association of clinically relevant treadmill exercise test parameters with a validated questionnaire of assessment of physical as well as mental health. In addition, the large sample size provided adequate power to capture significant relationships when present. On the other hand, several limitations must be acknowledged. The cross-sectional design of the study did not allow to establish cause-effects relationships. Face-to-face interviews and self-reporting may introduce observer’s bias, as the subjects may opt to give socially desirable answers. Furthermore, exercise tolerance was evaluated in a semi-quantitative scale with arbitrary cut-offs. Finally, while we focussed on ETT-related variables, several psychological and social variables could have been usefully taken into account as independent variables to explain HRQL.
In conclusion, our study provides for the first-time valuable insights into the relationship between treadmill exercise test parameters and health-related quality of life, both physical and mental, in patients with CAD. It also helps to re-appraise the role of physical conditioning with respect to wellbeing in this population. Further research is warranted to highlight specific aspects of physical performance in terms of exercise tolerance or adaptation that could serve as targets of pharmacotherapy or non-drug related treatment in patients with CAD.
References
Sanchis-Gomar, F., Perez-Quilis, C., Leischik, R., & Lucia, A. (2016). Epidemiology of coronary heart disease and acute coronary syndrome. Annals of Translational Medicine. https://doi.org/10.1016/j.socscimed.2009.02.028.
Gillison, F. B., Skevington, S. M., Sato, A., Standage, M., & Evangelidou, S. (2009). The effects of exercise interventions on quality of life in clinical and healthy populations; a meta-analysis. Soc Sci Med. https://doi.org/10.1016/j.socscimed.2009.02.028.
Bize, R., Johnson, J. A., & Plotnikoff, R. C. (2007). Physical activity level and health-related quality of life in the general adult population: A systematic review. Preventive Medicine. https://doi.org/10.1016/j.ypmed.2007.07.017.
Sharma, A., Madaan, V., & Petty, F. D. (2006). Exercise for mental health. Primary Care Companion to the Journal of Clinical Psychiatry. https://doi.org/10.4088/PCC.v08n0208a.
Westin, L., Carlsson, R., Israelsson, B., Willenheimer, R., Cline, C., & McNeil, T. F. (1997). Quality of life in patients with ischaemic heart disease: A prospective controlled study. J Intern Med. https://doi.org/10.1046/j.1365-2796.1997.00203.x.
Sajobi, T. T., Wang, M., Awosoga, O., Santana, M., Southern, D., Liang, Z., et al. (2018). Trajectories of health-related quality of life in coronary artery disease. Circ Cardiovasc Qual Outcomes. https://doi.org/10.1161/CIRCOUTCOMES.117.003661.
Le, J., Dorstyn, D. S., Mpfou, E., Prior, E., & Tully, P. J. (2018). Health-related quality of life in coronary heart disease: a systematic review and meta-analysis mapped against the International Classification of Functioning, Disability and Health. Quality of Life Research. https://doi.org/10.1007/s11136-018-1885-5.
Unsar, S., Sut, N., & Durna, Z. (2007). Health-related quality of life in patients with coronary artery disease. J Cardiovasc Nurs. https://doi.org/10.1097/01.JCN.0000297382.91131.8d.
Catapano, A. L., Graham, I., De Backer, G., Wiklund, O., John Chapman, M., Drexel, H., et al. (2016). 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias. European Heart Journal. https://doi.org/10.5603/KP.2016.0157.
Williams, B., Mancia, G., Spiering, W., Rosei, E. A., Azizi, M., Burnier, M., et al. (2018). 2018 ESC/ESH Guidelines for themanagement of arterial hypertension. European Heart Journal. https://doi.org/10.1093/eurheartj/ehy339.
Rydén, L., Grant, P. J., Anker, S. D., Berne, C., Cosentino, F., Danchin, N., et al. (2013). ESC guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J. https://doi.org/10.15829/1560-4071-2014-3-7-61.
Aboyans, V., Ricco, J. B., Bartelink, M. L. E. L., Björck, M., Brodmann, M., Cohnert, T., et al. (2018). 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS). European Heart Journal. https://doi.org/10.1093/eurheartj/ehx095.
Chrysohoou, C., Skoumas, J., Georgiopoulos, G., Liontou, C., Vogiatzi, G., Tsioufis, K., et al. (2017). Exercise capacity and haemodynamic response among 12,327 individuals with cardio-metabolic risk factors undergoing treadmill exercise. Eur J Prev Cardiol. https://doi.org/10.1177/2047487317726069.
Gibbons, R. J., Balady, G. J., Bricker, J. T., Chaitman, B. R., Fletcher, G. F., Froelicher, V. F., et al. (2002). ACC/AHA 2002 guideline update for exercise testing: Summary article. A report of the American College of Cardiology/American Heart Association task force on practice guidelines (committee to update the 1997 exercise testing guidelines). Circulation. https://doi.org/10.1016/s0735-1097(02)02164-2.
Cole, C. R., Blackstone, E. H., Pashkow, F. J., Snader, C. E., & Lauer, M. S. (1999). Heart-rate recovery immediately after exercise as a predictor of mortality. N Engl J Med. https://doi.org/10.1056/NEJM199910283411804.
McHam, S. A., Marwick, T. H., Pashkow, F. J., & Lauer, M. S. (1999). Delayed systolic blood pressure recovery after graded exercise: An independent correlate of angiographic coronary disease. J Am Coll Cardiol. https://doi.org/10.1016/S0735-1097(99)00269-7.
Ware, J. E., Snow, K. K., Kosinski, M., & Gandek, B. (1993). SF-36 Health Survey Manual and Interpretation Guide. . QualityMetric.
Hair, J. F., Black, W. C., Babin, B. J., & Anderson, R. E. (2010). Multivariate Data Analysis. (7th ed.). Pearson.
Goff, D. C., Lloyd-Jones, D. M., Bennett, G., Coady, S., D’Agostino, R. B., Gibbons, R., et al. (2014). 2013 ACC/AHA guideline on the assessment of cardiovascular risk: A report of the American college of cardiology/American heart association task force on practice guidelines. Circulation. https://doi.org/10.1161/01.cir.0000437741.48606.98.
Bosworth, H. B., Siegler, I. C., Olsen, M. K., Brummett, B. H., Barefoot, J. C., Williams, R. B., et al. (2000). Social support and quality of life in patients with coronary artery disease. Qual Life Res. https://doi.org/10.1023/a:1008960308011.
Brink, E., Grankvist, G., Karlson, B. W., & Hallberg, L. R. M. (2005). Health-related quality of life in women and men one year after acute myocardial infarction. Qual Life Res. https://doi.org/10.1007/s11136-004-0785-z.
Norris, C. M., Ghali, W. A., Galbraith, P. D., Graham, M. M., Jensen, L. A., & Knudtson, M. L. (2004). Women with coronary artery disease report worse health-related quality of life outcomes compared to men. Health Qual Life Outcomes. https://doi.org/10.1186/1477-7525-2-21.
Norris, C. M., Spertus, J. A., Jensen, L., Johnson, J., Hegadoren, K. M., & Ghali, W. A. (2008). Sex and gender discrepancies in health-related quality of life outcomes among patients with established coronary artery disease. Circ Cardiovasc Qual Outcomes. https://doi.org/10.1161/CIRCOUTCOMES.108.793448.
Morys, J. M., Bellwon, J., Höfer, S., Rynkiewicz, A., & Gruchala, M. (2016). Quality of life in patients with coronary heart disease after myocardial infarction and with ischemic heart failure. Arch Med Sci. https://doi.org/10.5114/aoms.2014.47881.
Staniute, M., Brozaitiene, J., & Bunevicius, R. (2013). Effects of social support and stressful life events on health-related quality of life in coronary artery disease patients. J Cardiovasc Nurs. https://doi.org/10.1097/JCN.0b013e318233e69d.
Stafford, L., Berk, M., & Jackson, H. J. (2013). Tobacco smoking predicts depression and poorer quality of life in heart disease. BMC Cardiovasc Disord. https://doi.org/10.1186/1471-2261-13-35.
Farhat, A., Al-Hajje, A., Rachidi, S., Zein, S., Zeid, M. B., Salameh, P., et al. (2016). Risk factors and quality of life of dyslipidemic patients in Lebanon: A cross-sectional study. J Epidemiol Glob Health. https://doi.org/10.1016/j.jegh.2016.10.001.
Lalonde, L., O’Connor, A., Joseph, L., Grover, S. A., Cassidy, L. E., Green, L., et al. (2004). Health-related quality of life in cardiac patients with dyslipidemia and hypertension. Qual Life Res. https://doi.org/10.1023/B:QURE.0000021695.26201.a0.
Bruckert, E., Saheb, S., Bonté, J. R., & Coudray-Omnès, C. (2014). Daily life, experience and needs of persons suffering from homozygous familial hypercholesterolaemia: Insights from a patient survey. Atheroscler Suppl. https://doi.org/10.1016/j.atherosclerosissup.2014.07.006.
Hollman, G., Gullberg, M., Ek, A. C., Eriksson, M., & Olsson, A. G. (2002). Quality of life in patients with familial hypercholesterolaemia. J Intern Med. https://doi.org/10.1046/j.1365-2796.2002.00963.x.
Mata, N., Alonso, R., Banegas, J. R., Zambón, D., Brea, Á., & Mata, P. (2014). Quality of life in a cohort of familial hypercholesterolemia patients from the south of Europe. Eur J Public Health. https://doi.org/10.1093/eurpub/cks174.
Mortensen, G. L., Madsen, I. B., Kruse, C., & Bundgaard, H. (2016). Familial hypercholesterolaemia reduces the quality of life of patients not reaching treatment targets. Dan Med J., 63(5), A5224.
Jing, X., Chen, J., Dong, Y., Han, D., Zhao, H., Wang, X., et al. (2018). Related factors of quality of life of type 2 diabetes patients: a systematic review and meta-analysis. Health Qual Life Outcomes [Internet]., 16(1), 189. https://doi.org/10.1186/s12955-018-1021-9.
Lindsay, G. (2000). Assessment of changes in general health status using the short-form 36 questionnaire 1 year following coronary artery bypass grafting. Eur J Cardio-Thoracic Surg [Internet]., 18(5), 557–64. https://doi.org/10.1016/S1010-7940(00)00542-X.
Kiebzak, G. M., Pierson, L. M., Campbell, M., & Cook, J. W. (2002). Use of the SF36 general health status survey to document health-related quality of life in patients with coronary artery disease: Effect of disease and response to coronary artery bypass graft surgery. Hear Lung [Internet]., 31(3), 207–13.
Merkouris, A., Apostolakis, E., Pistolas, D., Papagiannaki, V., Diakomopoulou, E., & Patiraki, E. (2009). Quality of Life after Coronary Artery Bypass Graft Surgery in the Elderly. Eur J Cardiovasc Nurs [Internet], 8(1), 74–81. https://doi.org/10.1016/j.ejcnurse.2008.02.008.
Takousi, M. G., Schmeer, S., Manaras, I., Olympios, C. D., Makos, G., & Troop, N. A. (2016). Health-Related Quality of Life after Coronary Revascularization: A systematic review with meta-analysis. Hell J Cardiol [Internet]., 57(4), 223–37.
Mark, D. B., Knight, J. D., Velazquez, E. J., Wasilewski, J., Howlett, J. G., Smith, P. K., et al. (2014). Quality-of-Life Outcomes With Coronary Artery Bypass Graft Surgery in Ischemic Left Ventricular Dysfunction. Ann Intern Med [Internet]., 161(6), 392. https://doi.org/10.7326/M13-1380.
Szygula-Jurkiewicz, B., Zembala, M., Wilczek, K., Wojnicz, R., & Polonski, L. (2005). Health related quality of life after percutaneous coronary intervention versus coronary artery bypass graft surgery in patients with acute coronary syndromes without ST-segment elevation. 12-month follow up☆. Eur J Cardio-Thoracic Surg Internet., 27(5), 882–886. https://doi.org/10.1016/j.ejcts.2005.01.037.
Marchionni, N., Fattirolli, F., Fumagalli, S., Oldridge, N., Del Lungo, F., Morosi, L., et al. (2003). Improved exercise tolerance and quality of life with cardiac rehabilitation of older patients after myocardial infarction: Results of a randomized, controlled trial. Circulation. https://doi.org/10.1161/01.CIR.0000066322.21016.
Shepherd, C. W., & While, A. E. (2012). Cardiac rehabilitation and quality of life: A systematic review. International Journal of Nursing Studies. https://doi.org/10.1155/2020/1236968.
Prabhu, N. V., Maiya, A. G., & Prabhu, N. S. (2020). Impact of Cardiac Rehabilitation on Functional Capacity and Physical Activity after Coronary Revascularization: A Scientific Review. Cardiology Research and Practice. https://doi.org/10.1155/2020/1236968.
Taylor, R. S., Brown, A., Ebrahim, S., Jolliffe, J., Noorani, H., Rees, K., et al. (2004). Exercise-based rehabilitation for patients with coronary heart disease: systematic review and meta-analysis of randomized controlled trials. Am J Med [Internet]., 116(10), 682–92.
Anderson, L., Thompson, D. R., Oldridge, N., Zwisler, A.-D., Rees, K., Martin, N., et al. (2016). Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst Rev [Internet]. https://doi.org/10.1002/14651858.CD001800.pub3.
Linke, A. (2008). Effects of exercise training upon endothelial function in patients with cardiovascular disease. Front Biosci [Internet]., 13(13), 424.
Brown, M. D. (2003). Physiological Society Symposium - the Athlete’s Heart. Exp Physiol [Internet]., 88(5), 645–58. https://doi.org/10.1113/eph8802618.
Winzer, E. B., Woitek, F., & Linke, A. (2018). Physical Activity in the Prevention and Treatment of Coronary Artery Disease. J Am Heart Assoc [Internet]. https://doi.org/10.1161/JAHA.117.007725.
Ashor, A. W., Lara, J., Siervo, M., Celis-Morales, C., & Mathers, J. C. (2014). Effects of Exercise Modalities on Arterial Stiffness and Wave Reflection: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. PLoS One [Internet]., 9(10), e110034. https://doi.org/10.1371/journal.pone.0110034.
Takura, T., Ebata-Kogure, N., Goto, Y., Kohzuki, M., Nagayama, M., Oikawa, K., et al. (2019). Cost-Effectiveness of Cardiac Rehabilitation in Patients with Coronary Artery Disease: A Meta-Analysis. Cardiol Res Pract [Internet], 2019, 1–11.
Acknowledgements
Dr Georgios Georgiopoulos was supported by THE ONASSIS FOUNDATION UNDER THE SPECIAL GRANT & SUPPORT PROGRAM FOR SCHOLARS’ ASSOCIATION MEMBERS (GRANT No. R ZP 001/2019-2020).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Katsi, V., Georgiopoulos, G., Mitropoulou, P. et al. Exercise tolerance and quality of life in patients with known or suspected coronary artery disease. Qual Life Res 30, 2541–2550 (2021). https://doi.org/10.1007/s11136-021-02844-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-021-02844-y